Embed Size (px)
Citation preview

SAE Form Completion
Guidance Notes for Completing the SAE reporting form (v 9)

Causality – Importance for Completion
• Failure to provide a causality assessment will result in …
– A submission to regulatory authorities as if the SAE were drug-related.
• Failure to provide a causality assessment could result in
– unnecessary queries back to site
– SUSARs resulting from missing data
– Unblinding of patients
Provide your medical opinion on what most likely caused
the event

ReminderResolved with Sequelae
• “Resolved with Sequelae”
– If the sequelae is serious it must be reported as a separate SAE..
If completed, confirm if additional SAE

Coding of events – Additional Event Terms
• Event terms and unrelated sign and symptoms that are not serious
– note Not Serious by writing (NS) beside each term
• Event terms that are unrelated to the SAE being reported and are serious
– Report on a separate SAE form
• Recorded event terms or signs/symptoms that do not fit with the reported event, will be queried by Roche Drug Safety.
– Respond with 24 hours • If no response, event will be reported as serious and drug
related
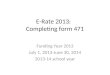
In this example it is clear to see what the Investigator has assessed as Non-Serious.

Examples
• The following slides show examples that were highlighted by Regulatory Authorities. All events were recorded in the narrative but only one event per case was reported as an actual SAE.

Example 1
On 11th January 2007 the patient started treatment with subcutaneous Peg-Interferon Alfa 2a 180mcg per week, and oral Ribavirin 100mg daily. Some time later, the patient developed severe depression. On 01 March 2007, the patient started treatment with Escitalopram (Cipralex) 10mg daily. Seven days later, the event of depression resolved. The patient developed diabetes mellitus which was considered Life Threatening and required hospitalisation. The patient was anti-Islet cell antibody positive. Approximately 11th March 2007, the patient developed a severe worsening of her condition and received emergency treatment. The following day, she received an infusion due to severe dehydration, confusion and temporal and spatial disorientation. The patient was hospitalised. Treatment with Peg-Interferon Alfa 2a and Ribavirin was stopped. The same day, the patient developed Kussmaul respiration and had a glucose value higher than 900mg/dl. In hospital she received intensive care and was diagnosed with manifest diabetes mellitus with ketoacidotic coma and pre-renal renal insufficenciency. A blood gas analysis showed severe Ketoacidosis, and positive antibodies against Islet Cells and GADA antibodies were seen. The patient was treated with Insulin.
– Separate SAE forms would be required for: • Diabetes Mellitus• Ketoacidotic Coma• Pre-Renal Insufficiency
– They would all be reported to authorities within a single case.

Example 2
In May 2007 the patient was diagnosed with a Carcinoma of the Colon Sigmoideum. Subsequently, on 11th May surgery was performed for a right Hemicolectomy, resection of the colon sigmoideum and partial resection of the Urinary Bladder. On 20th July 2007, the patient commenced oral Capecitabine 2000mg twice daily. On an Unspecified date he commenced intravenous Bevacizumab 200mg once every 3 weeks. On 17th August 2007 the dose of Bevacizumab was reduced (patient had received 2 cycles). On 25th August 2007, the dose of Capecitabine was reduced (patient had received 2 cycles). The same day, he experienced severe mucositis (CTCAE Grade 3). On an unspecified date the patient was hospitalised and Creatinine was 3mg/dl (normal range 0.7-1.2mg/dl). On 10th September 2007, the event resolved. It was reported that the patient did not drink enough and had loss of fluid because of diarrhoea. It was further reported that because of dehydration, pre-renal failure appeared and there was an accumulation of Capecitabine.
– Separate SAE forms for: • Grade 3 Mucositis• Pre-Renal Failure
– Would be reported to authorities in a single case.