Embed Size (px)
Citation preview

Jon Evans, MA, President & CEO
Mandy Fauble, PhD, LCSW, Vice President of Clinical Operations
Lee Penman, RN, Clinic Coordinator
Safe Harbor Behavioral Health
Early Onset Schizophrenia: Outcomes from
the National Council Community of Practice
• 1% of the population develops schizophrenia
• Less than 1% develops schizoaffective disorder
• This translates to 100,000 people between 15-25 who are
developing symptoms each year
http://practiceinnovations.org/ConsumersandFamilies/ViewAllC
ontent/RAISE_WhenMySonBecameIll/tabid/238/Default.asp
x
Psychosis
2

• 1/3 of people with schizophrenia attempt suicide in their
lifetime and 1 in 10 die by suicide
• Co-morbid medical care is great
• Unemployment and disability is a challenge, as is lack of
meaningful work opportunities
• The illness is most costly in the first years, especially upon
onset
• http://www.cdc.gov/mentalhealth/basics/burden.htm
Burden of Disease
3

• “The overall U.S. 2002 cost of schizophrenia was estimated
to be $62.7 billion, with $22.7 billion excess direct health
care cost ($7.0 billion outpatient, $5.0 billion drugs, $2.8
billion inpatient, $8.0 billion long-term care). The total direct
non-health care excess costs, including living cost offsets,
were estimated to be $7.6 billion. The total indirect excess
costs were estimated to be $32.4 billion.”
• “Schizophrenia is a debilitating illness resulting in significant
costs. The indirect excess cost due to unemployment is
the largest component of overall schizophrenia excess
annual costs.”• Wu, Eq, Birnbaum, H.G, Shi, L., Ball, D.E, Kessler, R.C., Moulis, M. & Aggarwal, J. (2002. The
economic burden of schizophrenia in the United States in 2002. Journal of Clinical Psychiatry, 66(9),
1122-1129. .
4

• National Council Opportunity
– Application Process for No-Charge program
– 10 Agencies Selected
• Webinars
• Office Hours
• Training track at National Council
• Staff activities and Instruments
Early Onset of the Project
5

• Prodrome stage
– Missing history, time and the unfolding story at this stage
– Difficulty prospectively
• More than 8% of healthy kids report some type of hallucination-
like event during development McGee, R., Williams, S., Poulton, R., (2000).
Hallucinations in nonpsychotic children. Journal of American Academy of Child & Adolescent Psychiatry, 39,
12-13. Cited in White, T., Anjum, A., & Schulz, S.C. (2006). The schizophrenia prodrome. The American
Journal of Psychiatry, 163(3), 376-380.
• “Early Onset”
– No treatment history
– First two-three years of onset - Up to five years? Age range varies
• In common
– Idea that duration of untreated psychosis really matters
– Specialized care can make a huge difference
What Does Early Onset Mean?
6
• Family and client confusion
• Frequent inexperience with
the healthcare system
• Grief and loss
– Denial
– Anger
– Sadness
– Isolation
• Substance use
• Peer group primacy
• Emerging self in the context
of medications
– Sexual, intellectual, emotional,
spiritual, physiological
• Risk for police interactions
• Environmental risks
• Finding a ‘voice’ and power
• Risk of poverty
– Caused by illness
– Exacerbating illness
• Variable insurance coverage
• Not well represented
politically
• Not well ‘matched’ by staff
and peer opportunities
• Loss of independence
• Social disconnect of
symptoms
Developmental Factors
7

Medications Profiles are Better…But
8

Social Effects of Illness in Treatment?
9

Evaluation Tool: SW
10
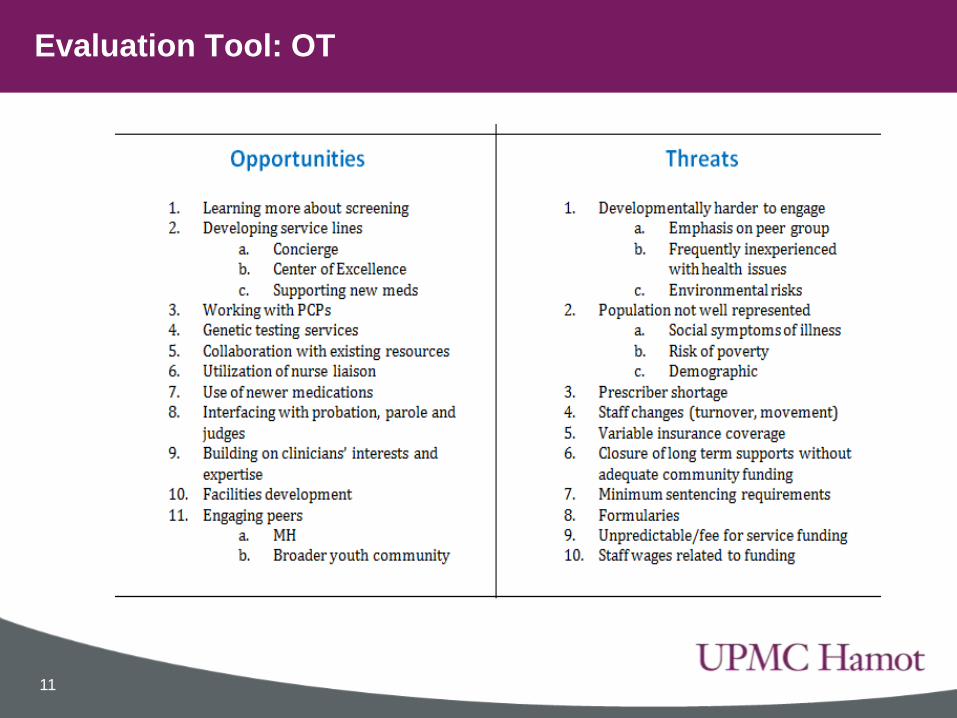
Evaluation Tool: OT
11

• Core roles for 30-35 clients
– Team Leader
– Therapist(s)
– Case Manager(s)
– Supportive Employment and Education Worker
– Prescription Services
– Think ACT or CTT prior to chronicity
Programming: Coordinated Specialty Care
12

• Outreach
• Engagement
• Manualized interventions for therapy
• Family work and Multifamily group work
• Case Management
• Vocational activities
• Peers and Inspiration
• Other needs: housing, substance use, trauma, crisis
intervention etc.
• Manuals & Fidelity
Coordinated Specialty Care Activities
13

• CBT-P is a recommended model
• https://www.youtube.com/watch?v=DkI1FudZrAs
• http://practiceinnovations.org/ConsumersandFamilies/Sympt
omManagement/RAISE_DealingWithParanoia/tabid/221/Def
ault.aspx
• Have a look at some studies and tools:
• http://www.isps.org/index.php/learning-resources/learning-tools/cbt-for-
psychosis-cbtp
• https://www.youtube.com/watch?v=4O-eomW0hzw
Dealing Directly with Psychotic Symptoms
14

• Scale of competence 0-6– Incompetent, Novice, Advanced Beginner, Competent, Proficient, Expert
• 12 Items
– Agenda Setting and Adherence
– Feedback
– Collaboration
– Pacing and Efficient Use of Time
– Interpersonal Effectiveness
– Eliciting Appropriate Emotional Expression
– Eliciting Key Cognitions
– Eliciting Behaviors
– Guided Discovery
– Conceptual Integration
– Application of Change Methods
– Homework Setting
• James, Blackburn & Reichelt, 2001
Evaluation Tool: Revised Cognitive Therapy Scale
15

• Provides excel worksheets to think about costing
• Live online at
http://practiceinnovations.org/OnTrackUSA/tabid/253/Defaul
t.aspx
• These tools can help in a variety of programs
Evaluation of Financial Data Tools: OnTrack USA
16

17
Flexible Tool to Estimate Number of Teams Needed for People with First Episode Psychosis (FEP) and Associated Costs
User Can Input Different Numbers and Assumptions in Green Rows (5, 6, 9, 11, 13, 14, 19, 20, 22)
Note: Generic Tool for Estimating Number of Teams and Associated Costs (September, 2014). New York State example in separate tab.
Low Estimate Medium Estimate #1 Medium Estimate #2 High Estimate
Total population size (V) 1,000,000 1,000,000 1,000,000 1,000,000
Number of new individuals with FEP per 100,000 population/year1 (V) 15 16.7 20 30
Rate of new cases of FEP per year (# new individuals/100,000) 0.00015 0.000167 0.0002 0.0003
Number of incident cases of FEP per year (Population size*Rate of new cases of FEP per year) 150 167 200 300
Fraction of incident cases approached (V) 0.2 0.333 0.25 0.5
Number of incident cases approached (Cases*Fraction approached) 30 56 50 150
Fraction of those approached agreeing to enter services (V) 0.5 0.5 0.6 0.75
Number of total new active individuals receiving services per year (Cases approached * Fraction agreeing to
enter services)
15 28 30 113
Maximum # active individuals served per team (V) 30 35 30 35
Average # months in treatment (V) 18 18 22 24
Number of new individuals each team can take/month (active cases per team/months in treatment) 1.667 1.944 1.364 1.458
Number of new individuals each team can take/year (new individuals per month*12) 20 23 16 18
Number of teams needed for population (# new active individuals per year/new individuals per team
per year)
0.75 1.19 1.83 6.43
Population size to support 1 team (population size/# of teams) 1,333,333 839,163 545,455 155,556
Personnel costs per team: Salary and fringe (as calculated on Personnel Costs worksheet) (V) 419,998 419,998 419,998 419,998
Non-personnel costs per team (as calculated on NPS Costs worksheet) (V) 49,711 49,711 49,711 49,711
Total direct costs per team (personnel + non-personnel costs) 469,709 469,709 469,709 469,709
Percentage of indirect costs per team (V) 15% 15% 15% 15%
Total indirect costs per team 70,456 70,456 70,456 70,456
Total costs per team per year (direct and indirect costs) 540,165 540,165 540,165 540,165
Cost per client (Total costs/clients served per team) 18,006 15,433 18,006 15,433
Total cost per year for population (# teams*total cost per team) $405,124 $643,696 $990,303 $3,472,491
Note: Tool illustrates costs and teams needed under low, medium, and high estimates of the number of persons served, which corresponds to various estimates of incidence, percentage of persons approached, and percentage agreeing to services, number of clients served per team, and average months in treatment.
Note: Users can see how the number of estimated teams needed and associated costs per year change under varying assumptions.
1Incidence of all psychoses are estimated at 27.1/100,000 (Kirkbride et al, 2009) and 31.6/100,000 (Baldwin et al, 2005). Incidence of non-affective psychoses (ICD 10 codes F20-F29 including schizophrenia, schizotypal disorder, delusional disorders, brief psychotic disorder, shared psychotic disorder, schizoaffective disorders, other psychotic disorder not due to a
substance or known physiological condition, and unspecified psychosis not due to a substance or known physiological condition) are estimated at 16.7/100,000 (Kirkbride). Affective psychoses are estimated at 6.8/100,000 (Kirkbride) and 11.6/100,000 (Baldwin). Incidence of schizophrenia alone is estimated at 8.9/100,000 (Kirkbride) and 7.0/100,000 (Baldwin).

Financial Evaluation: Start Up Costs
18
Annual cost of each team
Role % Time Annual Salary Rate Cost1
FEP Team Leader 100% 84,000 $84,000
2IPS Specialist 100% 56,400 $56,400
3Recovery Coach (MSW) 100% 70,974 $70,974
4Psychiatrist 30% 157,735 $47,321
5RN 10% 78,710 $7,871
6Total salary for team $266,566
7Fringe 36%
8Total + Fringe $362,529
9Indirect 15%
10Total Cost $416,908
11Cost per Client (30 client team) 13,897
12Cost per client (35 client team) $11,912
13
Cost per initial year (based on estimate of 30 total active clients per team and 4 new clients per month in start-up)14 Month #new clients per month Cumulative clients Annual cost of new clients
151 4 4 $55,588
162 4 8 $50,955
173 4 12 $46,323
184 4 16 $41,691
195 4 20 $37,059
206 4 24 $32,426
217 4 28 $27,794
228 2 30 $11,581
239 0 30 $0
2410 0 30 $0
2511 0 30 $0
2612 0 30 $0
27Total cost of initial year $303,417
28 Cost per initial year (based on estimate of 35 total active clients per team and 4 new clients per month in start-up)
29 Month #new clients per month Cumulative clients Annual cost of new clients
301 4 4 $47,647
312 4 8 $43,676
323 4 12 $39,706
334 4 16 $35,735
345 4 20 $31,764
356 4 24 $27,794
367 4 28 $23,823
378 4 32 $19,853
389 3 35 $11,912
3910 0 35 $0
4011 0 35 $0
4112 0 35 $0
42Total cost of initial year $281,910
Note: Monthly enrollment figures differ from Line 14 in the Generic Tool. This table describes estimates of enrollment at start-up, when teams are first trying to fill up. Line 14 of the Generic Tool describes the number of new enrollees a team can take at steady-state capacity, which is a function of the number of enrollees per team and the number of months clients tend to stay in treatment.
• Staffing. Teams hire and maintain the required staff.
– 1.0 FTE Team Leader who is a licensed clinician
– 1.0 FTE IPS Specialist
– 0.5 FTE Skills Trainer who is a licensed clinician
– 0.2 FTE Psychiatrist
• Vacancies are filled within 30 days
• Caseload size under 30. Teams maintain a caseload that is
small enough to allow for intensive and highly individualized
services while, at the same time, serving as many clients as
possible within these service demands.
• Full team meets at least weekly.These meetings are for
strategic clinical thinking and reviewing the status and “next
steps toward goals” for each person on the team’s caseload.
Performance Standards
19

• Intake occurs promptly.
– Intake occurs within 1 week of referral.
• At least one member of the team is available 24/7. Team
has on-call system for after-hours availability and service
logs show that any given month includes services on nights
and weekends.
• Outreach. Teams see clients in the field as needed. At least
10% of participants have at least one visit in the community.
Performance Standards
20

• Safety assessment. All clients assessed for suicide risk and
safety plans are formulated and implemented for those
determined to be at risk.
– The HASS Demo or equivalent screening tool is completed with
every participant at intake and whenever concerns about possible
suicide are raised.
• For those who meet or exceed the specified threshold
indicating a risk of suicide, a safety plan developed the
same day of the screening is included in the chart. Is this
given to the individual and the family so they will be able to
act according to the plan?
Performance Standards
21

• Discharge.
– The team provides a critical time intervention rather than a source of
services for people well along in their recovery. Clients transition
from the team to routine services as soon as clinically appropriate.
– The team follows up with discharged clients to help assure a smooth
transition to routine community services.
– Median and average length of stay with Connection Team of all
participants to be calculated at the end of each quarter.
– Mean length of stay for discharged clients will not exceed 30 months.
– Individual length of stay will not exceed 36 months.
– At least 90% of participants plan for discharge with Team (as
opposed to leaving precipitously).
– Discharge planning begins at start of treatment
– At least 90% percent of discharged participants attend their first
appointment within 30 days of discharge.
Performance Standards
22

• There are many standards in each domain. These can be
found at:
• http://www.nimh.nih.gov/health/topics/schizophrenia/raise/C
SC-for-FEP-Manual-II-Implementation-Manual_147093.pdf
Performance Standards
23

Lessons Learned
24