Embed Size (px)
Citation preview

Received: 29 May 2001Accepted: 29 April 2002Published online: 15 June 2002© Springer-Verlag 2002
Abstract Objective: To assess thesafety of long-distance ground inter-hospital transport of critically ill pa-tients with the most severe unstablerespiratory failure after establishmentof a dedicated transport system.Design and setting: Cohort study,retrospective chart review in 13 hos-pitals and intensive care units (ICU)in Finland, and a tertiary referralcenter and ICU of a university hospi-tal. Patients: 66 consecutive critical-ly ill patients who were transferredto our ICU from 13 different ICUs inFinland because of severe, progres-sive respiratory failure, 52 (79%)with acute respiratory distress syn-drome. Measurements and results:Major complications during transferand patients’ oxygenation. The me-dian transfer distance was 161 km(range 120–460 km). Drugs for car-diovascular support were infused in59 patients (89%) during transfer.
Fourteen patients (21%) were trans-ferred in prone position because oflife-threatening hypoxemia. The ra-tio of arterial blood PaO2 and thefraction of oxygen in the ventilatorwas 8.5±2.7 kPa (64±20 mmHg) be-fore transfer and 9.7±3.6 kPa(73±27 mmHg) after transfer. Therewere no major complications duringthe transfer. ICU mortality was 30%.Conclusions: Long-distance inter-hospital ground transfer of even crit-ically ill patients with severe unsta-ble respiratory and circulatory fail-ure is safe if a dedicated transportteam and a specially equipped trans-port vehicle are used.
Keywords Critical care · Respiratory failure · Mechanicalventilation · Transportation of patients · Acute respiratorydistress syndrome
Intensive Care Med (2002) 28:1122–1125DOI 10.1007/s00134-002-1348-9 O R I G I N A L
Ari UusaroIlkka ParviainenJukka TakalaEsko Ruokonen
Safe long-distance interhospital ground transferof critically ill patients with acute severeunstable respiratory and circulatory failure
Introduction
Transport of acutely ill patients between hospitals andalso within a hospital may increase morbidity and evenmortality [1, 2]. The transport of intensive care unit(ICU) patients is a particular challenge due to the severi-ty of illness and the need for continuous complex thera-pies during the transport. Intensive care patients aretransferred from a hospital to another for several reasons,for example, due to lack of beds.
Data are scarce on the risks of interhospital transportof the most severely ill patients. The aim of our studywas to assess the safety of long-distance interhospital
ground transport of patients with acute severe unstablerespiratory failure (most of whom had acute respiratorydistress syndrome, ARDS) after we designed and estab-lished a dedicated transport system.
Patients and methods
This study was approved by the institutional review board of ourhospital. The review board waived the need for informed consent.We included all patients (n=66) with severe respiratory failurewho were transported to our ICU from ICUs elsewhere in Finlandduring the first 6 years (1993–1999) after establishing a center foradvanced care for ARDS. All patients were transported because ofsevere, progressive respiratory failure. We had no uniform criteria
A. Uusaro (✉ ) · I. Parviainen · E. RuokonenKuopio University Hospital, Critical Care Research Program, Department of Anesthesiology and Intensive Care, Division of Critical Care, PO Box 1777,70211, Kuopio, Finlande-mail: [email protected].: +358-17-173311Fax: +358-17-173443
J. TakalaDepartment of Intensive Care Medicine,University Hospital of Bern (Inselspital),Bern, Switzerland
1123
for transfers. In each case the physician of the referring ICUjudged that she/he could no longer take care of the patient due toprogression of the disease. A decision to transfer was made by oursenior intensivist based primarily on the severity of gas exchangeabnormalities. Also other organ failures and comorbidity wereevaluated. ARDS, according to common consensus conferencecriteria, was the most common (79%) diagnosis for the transportedpatients (Table 1).
After the primary ICU physician consulted us and a decision totransfer was made, a dedicated transport team was alarmed. Thisteam included one intensivist, one nurse, and two paramedics. Weused a customized ambulance for transport. The ambulance wasequipped with an intensive care ventilator (Servo 900 C, Siemens,Solna, Sweden) with additional supply of oxygen and air and ourroutine monitoring devices and drugs. We had triple supply forelectricity. The ambulance was equipped with a diesel-poweredgenerator and a backup inverter. We also had a separate battery forthe ventilator.
When the team arrived at the referring ICU, 1–3 h were neededto complete patient monitoring, if necessary, and to stabilize thepatient. Most often we adjusted ventilatory settings and some-times, in cases of extreme hypoxemia, tested the effect of proneposition on gas exchange.
We used a regular hospital bed for transports. Patients were notdisconnected from the ventilator at any time during the transport.Vital signs, hemodynamics, and gas exchange were recorded every15 min. We defined major complication as any further immediate-ly life-threatening deterioration in the clinical status of the patient(such as progressive hypoxemia, hypotension, or cardiac failurenot responding to vasoactive drugs, new pneumothorax, accidentalremoval of tubes or catheters). Minor complications were not de-fined.
We used descriptive statistics and the t test. p values less than0.05 were taken as indicating statistically significant differences.
Results
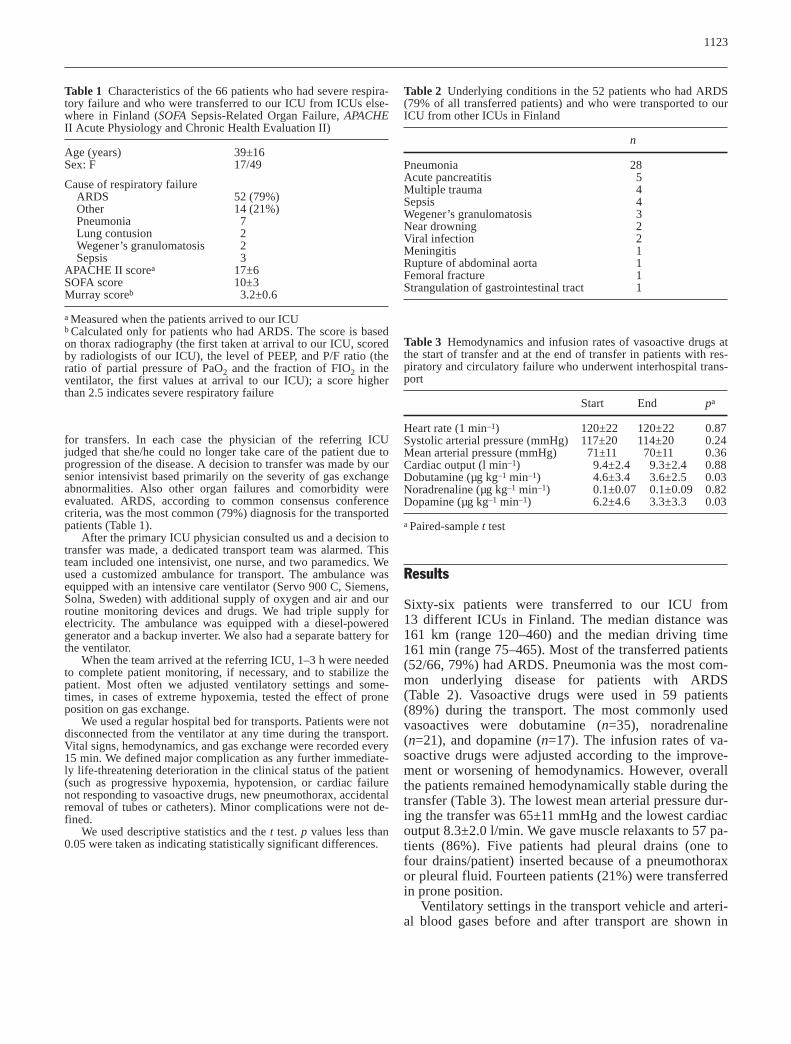
Sixty-six patients were transferred to our ICU from 13 different ICUs in Finland. The median distance was161 km (range 120–460) and the median driving time161 min (range 75–465). Most of the transferred patients(52/66, 79%) had ARDS. Pneumonia was the most com-mon underlying disease for patients with ARDS(Table 2). Vasoactive drugs were used in 59 patients(89%) during the transport. The most commonly usedvasoactives were dobutamine (n=35), noradrenaline(n=21), and dopamine (n=17). The infusion rates of va-soactive drugs were adjusted according to the improve-ment or worsening of hemodynamics. However, overallthe patients remained hemodynamically stable during thetransfer (Table 3). The lowest mean arterial pressure dur-ing the transfer was 65±11 mmHg and the lowest cardiacoutput 8.3±2.0 l/min. We gave muscle relaxants to 57 pa-tients (86%). Five patients had pleural drains (one tofour drains/patient) inserted because of a pneumothoraxor pleural fluid. Fourteen patients (21%) were transferredin prone position.
Ventilatory settings in the transport vehicle and arteri-al blood gases before and after transport are shown in
Table 1 Characteristics of the 66 patients who had severe respira-tory failure and who were transferred to our ICU from ICUs else-where in Finland (SOFA Sepsis-Related Organ Failure, APACHEII Acute Physiology and Chronic Health Evaluation II)
Age (years) 39±16Sex: F 17/49
Cause of respiratory failureARDS 52 (79%)Other 14 (21%)Pneumonia 7Lung contusion 2Wegener’s granulomatosis 2Sepsis 3
APACHE II scorea 17±6SOFA score 10±3Murray scoreb 3.2±0.6
a Measured when the patients arrived to our ICUb Calculated only for patients who had ARDS. The score is basedon thorax radiography (the first taken at arrival to our ICU, scoredby radiologists of our ICU), the level of PEEP, and P/F ratio (theratio of partial pressure of PaO2 and the fraction of FIO2 in theventilator, the first values at arrival to our ICU); a score higherthan 2.5 indicates severe respiratory failure
Table 2 Underlying conditions in the 52 patients who had ARDS(79% of all transferred patients) and who were transported to ourICU from other ICUs in Finland
n
Pneumonia 28Acute pancreatitis 5Multiple trauma 4Sepsis 4Wegener’s granulomatosis 3Near drowning 2Viral infection 2Meningitis 1Rupture of abdominal aorta 1Femoral fracture 1Strangulation of gastrointestinal tract 1
Table 3 Hemodynamics and infusion rates of vasoactive drugs atthe start of transfer and at the end of transfer in patients with res-piratory and circulatory failure who underwent interhospital trans-port
Start End pa
Heart rate (1 min–1) 120±22 120±22 0.87Systolic arterial pressure (mmHg) 117±20 114±20 0.24Mean arterial pressure (mmHg) 71±11 70±11 0.36Cardiac output (l min–1) 9.4±2.4 9.3±2.4 0.88Dobutamine (µg kg–1 min–1) 4.6±3.4 3.6±2.5 0.03Noradrenaline (µg kg–1 min–1) 0.1±0.07 0.1±0.09 0.82Dopamine (µg kg–1 min–1) 6.2±4.6 3.3±3.3 0.03
a Paired-sample t test

1124
Table 4. Arterial PCO2 increased and pH decreasedslightly. We calculated the ratio of partial pressure ofPaO2 and the fraction of FIO2 in the ventilator (P/F ratio)before and after transport. The P/F ratio before transportwas 8.5±2.7 kPa (range 4.7–18.4; 64±20 mmHg, range35–138) and that after transport 9.7±3.6 kPa (range4.4–22.3; 73±27 mmHg, range 33–167) after the trans-port (95% confidence interval of the difference –2 to–0.5 kPa, –15 to –4 mmHg, p=0.001).
There were no major medical or technical complica-tions during the transfer. The ICU length of stay for thetransported patients at our department was 15±9 days.ICU mortality was 30% overall and 31% in patients whohad ARDS. Nonsurviving patients died after12.5±10.1 days of intensive care. No deaths were relatedto the transfer.
Discussion
Our results demonstrate that long-distance interhospitalground transfers of even the most critically ill patientswith unstable severe respiratory and circulatory failureare safe. There were no major complications during thetransfers, despite the fact that 79% of our patients hadARDS, all had severe hypoxemia, and 89% required car-diovascular support. This is an important result whenone considers risks associated with transfers and the po-tential patient benefits of the transfer. ARDS is an exam-ple of severe disease in which regionalization may offeran outcome benefit [3]. Despite our findings it is impor-tant carefully to evaluate risks of transfers particularly inpatients with ARDS, since worsening hypoxemia is com-mon even in patients with less severe respiratory failure[4, 5]. Also, due to the retrospective nature of our studywe are not able to discuss minor complications.
Several studies suggest that even intrahospital trans-fers of critically ill patients are associated with compli-cations [1] The most common complications are hypox-emia and hypotension. Severe gas exchange abnormali-ties before transfer, as indicated by the need for positiveend-expiratory pressure and high (>0.5) FIO2 require-
ment, were predictors of deterioration in respiratoryfunction during intrahospital transfer of critically ill pa-tients [4, 5]. The mean FIO2 of our patients was 0.96, themean level of positive end-expiratory pressure12 cmH2O, and the median length of transfer in our se-ries was 161 km. However, we found that P/F ratio ofour patients was slightly higher on arrival to our ICUthan it was before the transfer. Before the transfer we didnot have a uniform protocol for patient stabilization. Weadjusted ventilator settings based on mechanical proper-ties of the lung, arterial, and mixed venous blood gasmeasurements and the interaction between ventilationand cardiac performance.
Some other studies also show that intra- and interhos-pital patient transfers may be safe especially if adequatepreparations are carried out by a dedicated team beforetransfer [6]. A specialized pediatric transport escort re-duced the incidence of adverse insults from 72% to 8%during interhospital transfer of pediatric emergencies [7].A recent study reviewed the outcome of 39 patients withrespiratory failure who were transferred via ground [8].The mean length of transfer was shorter than in our se-ries, and the severity of gas exchange (P/F ratio) wascomparable to our data. Only 72% of the patients by Ge-bremichael et al. [8] had an arterial line, 67% pulmonaryartery catheter, 56% of the patients needed vasoactivedrugs, and not all patients were on mechanical ventila-tion. In this series one patient died during transfer butgas exchange after transport was not reported.
Another group of investigators reported a series ofeight patients who underwent interhospital ground trans-fer because of severe ARDS [9]. All patients had severehypoxemia, defined as a P/F ratio lower than 6.7 kPa(50 mmHg), before transfer. Rossaint and colleagues [9]reported that gas exchange in their patients improvedduring the transfer. However, all of their patients wereput on mobile extracorporeal membrane oxygenation be-fore transfer because the authors felt that patients wouldnot survive conventional transport without this. In ourstudy 13 of the 66 patients (20%) had a P/F ratio lowerthan 6.7 kPa (50 mmHg), but our patients were trans-ferred safely using conventional mechanical ventilation.
Table 4 Initial ventilatory set-tings, lowest arterial and mixedvenous oxygen saturations dur-ing transfer and arterial bloodgases before (last values at thereferring ICU) and after (thefirst values immediately afterarrival to our ICU) transfer inpatients with severe respiratoryfailure (FIO2 fraction of oxy-gen in the inspiratory gas,PEEP positive end-expiratorypressure, SpO2 arterial oxygensaturation, SvO2 mixed venousoxygen saturation)
Before After p
FIO2 (fraction) 0.96±0.1 – – –PEEP (cmH2O) 12±3 – – –Minute volume (l) 13±3 – – –Ventilatory frequency (1/min) 23±6 – – –Tidal volume (l) 0.7±0.2 – – –Lowest SpO2 during transfer (%) 84 (61–96) – – –Lowest SvO2 during transfer (%) 61 (35–82) – – –pH – 7.32±0.08 7.30±0.11 0.043PaO2 (kPa) – 8.02±2.02 8.48±2.05 0.088PaCO2 (kPa) – 7.08±2.17 8.14±3.03 0.002Base excess (mmol/l) – 0.5±6.1 1.1±6.4 0.108

1125
Helicopters or fixed-wing aircrafts are recommendedfor transfers of critically ill patients over distances of80–240 km [10]. Before we established our center, wefirst considered air transfers but then gave up this idea.In our view, air transports would not be possible for ourpatients because of the severity of respiratory and circu-latory failure, and hence the ventilator and monitoringrequirements and extensive patient care during transfer.In addition, ground transports are likely to be cheaperthan air transports.
In conclusion, we found that patients with severe un-stable respiratory and concomitant circulatory failure canbe transferred without major complications. We suggestthat with a dedicated transport team, proper patient stabi-lization before transport, and a transport vehicle with in-tensive care facilities, interhospital ground transfers ofcritically ill patients over long distances are safe.
References
1. Braman SS, Dunn SM, Amico CA,Millman RP (1987) Complications dur-ing intrahospital transport in criticallyill patients. Ann Intern Med 107:469–473
2. Schiff RL, Ansell DA, Schlosser JE,Idris AH, Morrison A, Whitman S(1986) Transfer to a public hospital. A prospective study of 467 patients. N Engl J Med 314:552–557
3. Maerki SC, Luft HS, Hunt SS (1986)Selecting categories of patients for re-gionalization. Implications of the rela-tionship between volume and outcome.Med Care 24:148–158
4. Waydhas C, Schneck G, Duswald KH(1995) Deterioration of respiratoryfunction after intra-hospital transportof critically ill surgical patients. Inten-sive Care Med 21:784–789
5. Marx G, Vangerow B, Hecker H, Leuwer M, Jankowski M, PiepenbrockS, et al (1998) Predictors of respiratoryfunction deterioration after transfer ofcritically ill patients. Intensive CareMed 24:1157–1162
6. Edge WE, Kanter RK, Weigle CGM,Walsh RF (1994) Reduction of morbid-ity in interhospital transport by special-ized pediatric staff. Crit Care Med 22:1186–1191
7. Macnab AJ (1991) Optimal escort forinterhospital transport of pediatricemergencies. J Trauma 31:205–209
8. Gebremichael M, Borg U, HabashiNM, Cottingham C, Cunsolo L,McCunn M, et al (2000) Interhospitaltransport of the extremely ill patient:the mobile intensive care unit. CritCare Med 28:79–85
9. Rossaint R, Pappert D, Gerlach H,Lewandowski K, Keh D, Falke K(1997) Extracorporeal membrane oxy-genation for transport of hypoxemicpatients with severe ARDS. Br J Anae-sth 78:241–246
10. Wallace PGM, Ridley SA (1999)Transport of critically ill patients. BMJ319:368–371