Embed Size (px)
Citation preview

Morales et al. Journal for ImmunoTherapy of Cancer (2015) 3:22 DOI 10.1186/s40425-015-0066-0 J Im
munother C
CASE REPORT Open Accessancer: first published as 10.1
Safety and efficacy of ipilimumab to treatadvanced melanoma in the setting of livertransplantationRita E Morales1, Alexander N Shoushtari2, Michelle M Walsh3, Priya Grewal4, Evan J Lipson5 and Richard D Carvajal3*
186/s
40425-015-0066-0 on 16 June 20Abstract
Ipilimumab is a first-in-class immunological checkpoint blockade agent and monoclonal antibody against CytotoxicT-Lymphocyte Antigen 4 (CTLA-4) that has demonstrated survival benefit and durable responses in patients withmetastatic melanoma. To date, solid organ transplant recipients have been excluded from clinical trials with cancerimmunotherapies on the basis of their concurrent treatment with immunosuppressive agents. We present the firstcase to our knowledge of a patient with advanced cutaneous melanoma receiving ipilimumab status post orthotopicliver transplantation with a partial response. Transaminitis was observed 4 months after administration of ipilimumabthat resolved with close observation. No evidence of graft rejection has been observed to date. This case advocates forfurther investigation of the safety and efficacy of cancer immunotherapies in solid organ transplant recipients.
on April 30, 2021 by gues
http://jitc.bmj.com
/15. D
ownloaded from
BackgroundPatients presenting with melanoma after solid organtransplantation present unique challenges to oncologists.There are several important considerations in this set-ting, including the risk of injury to the allograft withthe administration of anticancer therapy and the scar-city of published data regarding the clinical manage-ment of advanced melanoma in organ transplantrecipients. This is especially relevant given the recentdevelopment of immunomodulatory therapies for thetreatment of metastatic melanoma. Ipilimumab is afirst-in-class immunological checkpoint blockade agentapproved by the United States Food and Drug Adminis-tration (FDA) in 2011 for the treatment of unresectableor metastatic melanoma. Two phase III studies havedemonstrated improved overall survival rates withipilimumab as compared to dacarbazine or a peptidevaccine control [1,2], Long-term disease control hasbeen documented in approximately 20% of individualstreated [3]. Given the success of ipilimumab in ad-vanced melanoma, it is important to consider the safetyand efficacy of this agent in solid organ transplant
* Correspondence: [email protected] Herbert Irving Comprehensive Cancer Center, Columbia UniversityMedical Center, 177 Fort Washington Avenue, Suite 6-435 Garden North,New York, NY 10032, USAFull list of author information is available at the end of the article
© 2015 Morales et al.; licensee BioMed CentraCommons Attribution License (http://creativecreproduction in any medium, provided the orDedication waiver (http://creativecommons.orunless otherwise stated.
recipients. The only published experience administer-ing drug to a solid organ transplant recipient is by Lipsonand colleagues [4], who reported two cases of successfuladministration of ipilimumab to patients with kidneytransplants. Here, we present the first case describing theuse of ipilimumab in a patient with a liver transplant.
t. Protec
Case presentationA 67-year-old man with a history of hepatitis C virus(HCV) and hepatocellular carcinoma (HCC) underwentorthotopic liver transplantation in 2006. He presentedwith decompensated liver disease marked by ascites andhepato-renal syndrome leading to renal failure. He wason hemodialysis prior to transplant and had a Model forEnd-Stage Liver Disease (MELD) score of 35 at time oftransplant. His donor was a 49-year-old man with nohistory of malignancy. Explant pathology revealed estab-lished cirrhosis with a 2.5 cm moderately differentiatedHCC with evidence of microvascular invasion. Aftertransplantation, he maintained stable liver function onan immunosuppressive regimen of tacrolimus and myco-phenolate mofetil. He underwent two post-transplantliver biopsies, which revealed HCV recurrence: Grade 1,Stage 1 in 2008 and Grade 1, Stage 2 in 2010. His liver
l. This is an Open Access article distributed under the terms of the Creativeommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andiginal work is properly credited. The Creative Commons Public Domaing/publicdomain/zero/1.0/) applies to the data made available in this article,
ted by copyright.

Morales et al. Journal for ImmunoTherapy of Cancer (2015) 3:22 Page 2 of 4
on April 30, 2021 by guest. P
rotected by copyrighhttp://jitc.bm
j.com/
J Imm
unother Cancer: first published as 10.1186/s40425-015-0066-0 on 16 June 2015. D
ownloaded from
enzymes remained in the normal range at this time. Heunderwent HCC surveillance at 6 monthly intervals forthe first 2 years after transplant and yearly thereafter forthe next 3 years.In 2007, a small pigmented skin lesion above his left
eyebrow grew larger and became ulcerated. A biopsy inSeptember 2009 revealed an ulcerated melanoma at least0.7 mm in Breslow thickness. Wide local excision withsentinel lymph node biopsy performed in November 2009demonstrated residual ulcerated melanoma, 2.51 mmthick, Clark Level IV, with a mitotic index of 11/mm2 andno lymphovascular or perineural invasion. Two sentinelnodes were negative for disease. Initial clinical staging byAmerican Joint Committee on Cancer (AJCC) 7th editionwas T3bN0, Stage IIB. In 2010, HCC surveillance imagingrevealed a 5 cm right adrenal mass that was subsequentlyresected. The pathology revealed metastatic HCC. At thispoint his immunosuppression was switched from tacroli-mus to rapamycin 3 mg daily and he was continued onmycophenolate mofetil 500 mg twice daily.The patient underwent active surveillance with clinical
exams and imaging studies until October 2013, when henoticed a swollen mass in the left parotid region. A nee-dle biopsy revealed melanoma wild-type for BRAF andcKIT. A positron emission tomography/computerizedtomography (PET/CT) scan performed in November2013 demonstrated prominent focal hypermetabolicactivity in bilateral lung nodules, bony foci and a parotidlesion, consistent with M1c disease. Magnetic resonanceimaging (MRI) of the brain showed no evidence ofmetastases. A repeat scan in January 2014 showed in-creasing nodal and bony disease and new hepatic metas-tases in the allograft. At that point, he was initiated ontherapy with paclitaxel. His rapamycin was reduced from3 mg to 1 mg daily and mycophenolate mofetil was dis-continued, given prior clinical reports documentingtumor regression with reduction of immunosuppression[5,6]. He completed 5 cycles of chemotherapy as well as14 of 20 planned fractions of palliative radiotherapy tothe hip before experiencing multifocal disease progres-sion in April 2014, with increasing disease burden in thelungs, mediastinal lymph nodes, liver and spleen.After a multidisciplinary team-based discussion in-
cluding both medical oncology and transplant medicine,the decision was made to begin therapy on ipilimumabwhile maintaining rapamycin at 1 mg daily. Given theincreased risk of graft rejection, the treatment planincluded weekly monitoring of liver function tests. Thepatient received his four induction doses of ipilimumab3 mg/kg between April 2014 and July 2014. The patientexperienced a mild non-pruritic rash on his torso afterthe second infusion, which lasted one week and re-solved with topical steroids. The aspartate aminotrans-ferase (AST), alanine aminotransferase (ALT) and alkaline
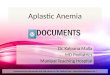
phosphatase were mildly elevated at baseline (CommonTerminology Criteria for Adverse Events [CTCAE] v4.0Grade 1) and remained stable throughout the course oftreatment. Total bilirubin was within normal limits atbaseline and remained normal throughout the course oftreatment. The fourth and final dose of ipilimumab wasadministered at week 10, on 7/1/2014. On week 12, aGrade 2 transaminitis and alkaline phosphatase eleva-tion developed, with no associated hyperbilirubinemia.The patient was managed conservatively with frequentlaboratory tests. AST and ALT levels peaked at a Grade3 on week 16 with stabilization or improvement thefollowing week without intervention (Figure 1). Becausethe patient remained asymptomatic and compliant withweekly laboratory testing, it was decided to maintainhim on close monitoring and defer initiation of cortico-steroids. Alkaline phosphatase levels peaked at week 17,but remained Grade 1 throughout the course of treat-ment. At last monitoring in February 2015, this valuehad returned to within normal limits. Total bilirubinhas remained within normal limits since the inductionof treatment. By week 20, all lab values resolved toGrade 1, and conservative management was continued.The patient declined a recommended liver biopsy. Thepatient remains stable 10 months following induction oftreatment.Repeat CT scans conducted in July 2014, after his
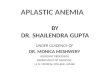
fourth infusion of ipilimumab, showed dramatic tumorregression in the lungs (Figure 2a) as well as the liver(Figure 2b). Clinically, the patient continues to feel welland is undergoing continued close monitoring for bothhis liver function and disease status.
ConclusionsCompared to the general population, organ transplantrecipients (OTRs) have an estimated 2.4 fold increasedrisk of developing melanoma [7]. Prognosis for thesepatients is also estimated to be worse than those withnon-transplant associated melanomas. Brewer and col-leagues [8] performed the largest retrospective review ofpatients with melanoma arising post-transplant to date,which demonstrated decreased overall survival for OTRswith localized melanomas with Breslow thickness >1.5 mmor Clark Levels III and IV, compared to immunocompetentcontrols. They also found that the degree of immunosup-pression was negatively correlated with survival.Given the increased risk for melanoma in solid organ
transplant patients as well as poor outcomes, the devel-opment of treatment strategies for this population isnecessary. Two previously published case reports havedescribed complete responses of metastatic melanomaafter withdrawal of immunosuppressive medications inaplastic anemia and myasthenia gravis, without signifi-cant adverse effects related to immune reconstitution
t.

0
50
100
150
200
250
Un
its/
L
ALT Values
AST/ALT ULN
AST Values
AST/ALT Grade 2
AST/ALT Grade 3
1 62 3 4 5 7 8 9 10
Months
0
50
100
150
200
250
Un
its/
L
ALT Values
AST/ALT ULN
AST Values
AST/ALT Grade 2
AST/ALT Grade 3
1 62 3 4 5 7 8 9 10
Months
Figure 1 Demonstration of changes in AST/ALT values over time with administration of ipilimumab; AST and ALT levels were measured weeklyduring the administration of ipilimumab. Sixteen weeks following initial induction, AST and ALT levels peaked at Grade 3. Resolution to Grade 1was seen at Week 20, and monthly monitoring of liver function tests has been performed since, with continued evidence of stability. Arrowsdenote the times of administration of ipilimumab.
Morales et al. Journal for ImmunoTherapy of Cancer (2015) 3:22 Page 3 of 4
hJ Im
munother C
ancer: first published as 10.1186/s40425-015-0066-0 on 16 June 2015. Dow
nloaded from
[5,6]. However, withdrawal of immunosuppression may notbe feasible in the setting of solid organ transplantation.Therefore, therapeutic options for the advanced melanomamust include consideration of agents such as ipilimumab.There are at least two barriers to the use of immune
checkpoint inhibitors such as ipilimumab in OTRs. Firstly,because ipilimumab ostensibly requires a competent T-
Baselinea)
b)
Figure 2 Demonstration of radiographic response to ipilimumab; CT scansdemonstrate regression of lung and liver metastases (arrows).
cell population to carry out its antitumor function, the co-administration of immunosuppressive agents such as rapa-mycin to prevent graft rejection may impact the efficacy ofipilimumab in this population. In this case, the patient wasmaintained on low-dose immunosuppression with rapa-mycin throughout his course of treatment with ipilimu-mab. However, given his marked radiographic response
Week 12
performed prior to and 12 weeks after initiation of therapy
on April 30, 2021 by guest. P
rotected by copyright.ttp://jitc.bm
j.com/

Morales et al. Journal for ImmunoTherapy of Cancer (2015) 3:22 Page 4 of 4
on April 30, 2021 by guest. P
rotected by copyrighhttp://jitc.bm
j.com/
J Imm
unother Cancer: first published as 10.1186/s40425-015-0066-0 on 16 June 2015. D
ownloaded from
to treatment, it appears that the efficacy of the ipilimu-mab was not significantly affected by his concurrentimmunosuppression.A second barrier to treatment in cases such as this
stems from the ability of drugs such as ipilimumab toactivate T cells that may be specific for non-self antigensexpressed by the allograft, precipitating organ rejection.In our patient, there was initial concern for an adverseimmune reaction to treatment, especially given the risein liver function tests that was seen after 12 weeks oftreatment. However, with no further ipilimumab admin-istration and expectant observation, the patient’s transa-minitis resolved to near baseline levels within 8 weeks.Given these challenges, it is important to identify which
patients may tolerate a reduction of immunosuppressionas well as the use of immunomodulatory agents. Althoughno definitive prognostic markers have been identified, sev-eral studies have identified increased length of time sincetransplantation as a predictive factor for tolerance ofimmunosuppression withdrawal [9,10]. In addition,compared with other organs such as the heart and lung,liver grafts are considered to be the least immunogenicorgans for transplant and thus can sustain less aggres-sive immunosuppressive regimens [11]. The patient de-scribed above received his liver transplant 8 yearsbefore induction with ipilimumab, and was thus able totolerate reductions to his immunosuppressive regimenbefore induction with ipilimumab. This, along withclose monitoring of liver function and immunosuppres-sive drug levels, may have contributed to our success intreating him both safely and effectively with this drug.Although further study in a large patient cohort is
warranted, this case has demonstrated the feasibility andefficacy in administering ipilimumab to a liver transplantrecipient, and may suggest that liver transplant recipientsseveral years post-transplant may be appropriate candi-dates for trials with immunomodulatory treatments. Oursmall sample size underscores the importance of reportingsafety and efficacy data for ipilimumab in the solid tumororgan transplant population. Furthermore, the promisingdata from trials of programmed cell death-1 (PD-1) andprogrammed death-ligand 1 (PD-L1) antibodies in meta-static melanoma make it especially important to study thepotential effects of immune checkpoint inhibitors in im-munocompromised patients. The risks surrounding graftrejection in the setting of immune activation with theseagents must be strongly considered when making treat-ment decisions in this population.
ConsentWritten informed consent was obtained from the patientfor publication of this case report and any accompanyingimages. A copy of the written consent is available forreview by the Editor-in-Chief of this journal.
AbbreviationsHCV: Hepatitis C Virus; HCC: Hepatocellular carcinoma; CTCAE: CommonTerminology Criteria for Adverse Events; AST: Aspartate aminotransferase;ALT: Alanine aminotransferase; OTR: Organ transplant recipient.
Competing interestsANS will receive travel support from Bristol-Meyers Squibb. EJL serves as aconsultant for Amgen and Castle Biosciences. REM, MMW, PG and RDC haveno competing interests to disclose.
Authors’ contributionsREM and RDC conceived of this case report concept. RDC, MMW, ANS andPG participated in the care of this patient. All authors participated in thedevelopment and approval of this manuscript.
Author details1Columbia University College of Physicians and Surgeons, 630 W. 168thStreet, New York, NY 10032, USA. 2Melanoma and ImmunotherapeuticsOncology Service, Memorial Sloan Kettering Cancer Center, 300 East 66thStreet, New York 10065NY, USA. 3The Herbert Irving Comprehensive CancerCenter, Columbia University Medical Center, 177 Fort Washington Avenue,Suite 6-435 Garden North, New York, NY 10032, USA. 4Division of LiverDiseases, Mount Sinai School of Medicine, One Gustave L. Levy Place, Box1104, New York, NY 10029, USA. 5Johns Hopkins University School ofMedicine, Sidney Kimmel Comprehensive Cancer Center, 400 N. Broadway,Baltimore, MD 21231, USA.
Received: 16 March 2015 Accepted: 28 April 2015
References1. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al.
Improved survival with ipilimumab in patients with metastatic melanoma. NEngl J Med. 2010;363(8):711–23. doi:10.1056/NEJMoa1003466.
2. Robert C, Thomas L, Bondarenko I, O’Day S, Weber J, Garbe C, et al.Ipilimumab plus dacarbazine for previously untreated metastatic melanoma.N Engl J Med. 2011;364(26):2517–26. doi:10.1056/NEJMoa1104621.
3. Schadendorf D, Hodi FS, Robert C, Weber JS, Margolin K, Hamid O et al.Pooled Analysis of Long-Term Survival Data From Phase II and Phase IIITrials of Ipilimumab in Unresectable or Metastatic Melanoma. J Clin Oncol2015. doi:10.1200/JCO.2014.56.2736.
4. Lipson EJ, Bodell MA, Kraus ES, Sharfman WH. Successful administration ofipilimumab to two kidney transplantation patients with metastaticmelanoma. J Clin Oncol. 2014;32(19):e69–71. doi:10.1200/JCO.2013.49.2314.
5. Dillon P, Thomas N, Sharpless N, Collichio F. Regression of advancedmelanoma upon withdrawal of immunosuppression: case series and literaturereview. Med Oncol. 2010;27(4):1127–32. doi:10.1007/s12032-009-9348-z.
6. Hodi FS, Granter S, Antin J. Withdrawal of immunosuppression contributingto the remission of malignant melanoma: a case report. Cancer Immun.2005;5:7.
7. Dahlke E, Murray CA, Kitchen J, Chan AW. Systematic review of melanomaincidence and prognosis in solid organ transplant recipients. Transplant Res.2014;3:10. doi:10.1186/2047-1440-3-10.
8. Brewer JD, Christenson LJ, Weaver AL, Dapprich DC, Weenig RH, Lim KK,et al. Malignant melanoma in solid transplant recipients: collection ofdatabase cases and comparison with surveillance, epidemiology, and endresults data for outcome analysis. Arch Dermatol. 2011;147(7):790–6.doi:10.1001/archdermatol.2011.159.
9. Benitez C, Londono MC, Miquel R, Manzia TM, Abraldes JG, Lozano JJ, et al.Prospective multicenter clinical trial of immunosuppressive drug withdrawalin stable adult liver transplant recipients. Hepatology. 2013;58(5):1824–35.doi:10.1002/hep.26426.
10. de la Garza RG, Sarobe P, Merino J, Lasarte JJ, D’Avola D, Belsue V, et al. Trialof complete weaning from immunosuppression for liver transplantrecipients: factors predictive of tolerance. Liver Transpl. 2013;19(9):937–44.doi:10.1002/lt.23686.
11. Sanchez-Fueyo A, Strom TB. Immunologic basis of graft rejection andtolerance following transplantation of liver or other solid organs.Gastroenterology. 2011;140(1):51–64. doi:10.1053/j.gastro.2010.10.059.
t.