Embed Size (px)
Citation preview

november/december 2014
Safetyconnectofficial Safety Publication of air methodS corPoration
what you should know about ebola pg. 4
Patti Corbett reCeives safety award pg. 7
winter safety: heaters, Cords & automated weather pg. 8
a refueler's bad day pg. 11
aLSo
eBoLaPg. 2
a medicaL crewmemBer’S firSthand encounter with the eBoLa viruS
air methodS corporation / 7211 S. peoria St. / engLewood, co 80112
[ contentS ]
1 message from the ceo
6 get your flu shot!
7 Know your SmS
12 event review committee
13 occ update
“though we celebrate each opportunity to extend and enhance a patient’s life, our greatest celebration is the daily, safe return of each member of our team to their loved ones—this is our highest priority. at times, this may require the courage to stop or not accept a mission due to factors in the moment that exceed what we believe, and have been taught, are unacceptable risks for our team.”
air methods is committed to the creation of an environment designed to facilitate a culture founded on the principles of continuous improvement through managing the everyday risk and being vigilant and accountable to one another.
as defenders of tomorrow, air methods is committed to:
• the growth, maturation and continuous improvement of our safety and risk management systems.
• creating and nurturing a Just culture that empowers all employees to report openly on any and all safety risks free from the risk of retaliation.
• developing effective safety, environment and health management policies within the framework of a Safety management System.
• Promoting and supporting safety training and safety awareness programs.• facilitating a culture that includes a focus on safety assurance by educating all levels of management and all frontline
employees as frontline risk managers educated in the art of risked-base decision-making.• the certification of functional area’s declaration of compliance with company policy and procedures, federal, state and
local laws and regulations through the use of internal and external audits and evaluations. • Sharing best practice methods, risk-based data and lessons learned with our employees, customers and industry as well
as monitoring industry activity to ensure best safety and risk mitigation practices are incorporated at air methods.• demonstrating to customers and stakeholders a clear commitment and unwavering dedication to transparency, quality
and continuous improvement.• Providing the necessary resources in all areas to support this policy.
air methods maintains a zero tolerance towards injury, illness or death of our employees, customers, partners, patients or vendors. risks inherent in all operations must be managed to a level as low as reasonably practical. all employees are expected to protect themselves and each other by adhering to the principles outlined in this policy statement and all relevant safety, health and environmental policies and regulations, working in a manner that safeguard themselves, co-workers and other persons consistent with air methods dna.
meSSage from the ceo
aaron toddair methodS ceo
featureS
2 a BruSh with eBoLa
a medical crewmember’s firsthand encounter with the ebola virus
newS & noteS
chriStina BrodSLy / director of corporate communicationS [email protected]
november/december 2014
Safetyconnect
november/december 2014 / Safety connect 1
airmethodS.com
air methodS defenderS of tomorrow Safety Policy
4 what you ShouLd know aBout eBoLa
7 patti corBett receiveS Safety award
8 heating hangarS SafeLy
9 check thoSe cordS!
10 know your automated weather
11 a refueLer’S Bad day
cover Story

november/december 2014 / Safety connect 32 Safety connect / november/december 2014
i’ve been flying for Phoenix air as a flight medic (and more recently as a flight nurse) for over a decade. We transport people from overseas after they have been injured or become sick. circumnavigating the globe over the course of 24 to 48 hours is a logistical feat for an operator, and moving patients out of non-english-speaking countries presents many communication challenges. recently Phoenix air was contacted by Samaritan’s Purse, founded by the rev. billy graham, to extract one of their physicians who had contracted the ebola virus.
over the past two years, Phoenix air engineers, in collaboration with the centers for disease control and Prevention (cdc) and the department of defense, developed the aeromedical biologic containment System (abcS). this containment system was designed to repatriate americans infected with airborne diseases, such as SarS, merS, bird flu, swine flu, etc. When ebola began raging out of control in africa, the abcS was activated quickly. the theory and the physical science
Prior to coming in contact with the patient, the team is completely gowned up and the abcS environment on board the plane is prepared. contact with the patient and their escorts are accomplished on the tarmac at the airport instead of at the hospital. the patient is escorted up the stairway by one crew member and into the highly-modified gulfstream iii jet. the handrails and stairs are then wiped down with clorox by another crewmember in isolation gear. the patient is given clean tyvek booties to complement their full-body isolation gear at the time of initial contact.
the patient is escorted through the plastic-draped interior to the back of the aircraft where the abcS is secured by a specially-designed metallic exoskeleton. the negative-pressure system inside the abcS is activated prior to the patient entering. the patient then goes through the ante-chamber into the patient compartment, which is about the size of a galley kitchen normally found on a jet this size and has a height of nearly six feet at the center. leads, wires and tubes from monitoring equipment outside the abcS are fed through tight plastic sleeves in preparation to receive the patient.
on the right-hand side of the patient compartment inside the aircraft, a stretcher is secured by a locking mechanism to the metal frame of the system. it is prepped with padding, sheets and blankets for the patient's comfort and warmth, since airplane cabins can get quite cold at 40,000 feet. this is important because fevers range from 100.2 to 107f with ebola, depending on the evolution of the infection. the medical team member who has direct contact with the patient applies the monitoring leads, supplemental o2 and blood pressure cuff and if not already done, initiates iv access for fluids and medications to be administered from outside the abcS.
at this stage, the goal is to have as little contact with the infected person as possible during transport. a standard chemical camping toilet treated with sterilizing chemicals is in close proximity, and the patient is shown the easiest way to disconnect themselves and access the toilet when needed. as most patients are medical professionals themselves, they are able to reapply the monitoring equipment when finished. due to the nature of the disease, the patients are often dehydrated from fever, diaphoresis, diarrhea and vomiting.
magazines are left in the patient compartment at arm’s reach for those patients able to pass the time reading, and they have access to their computers if they desire. Snacks and bottled water are at the bedside for patients who aren’t vomiting. additional overhead lights inside the abcS can be shut off, allowing the patients to rest, which seems to be the most common request. after medicating the first physician i ever escorted, he reported that the flight itself had been the first time he had rested in days. disposable thermometers and air-sickness bags are placed at the bedside for self-monitoring, and a two-way dedicated
walkie-talkie is available, allowing the patient to easily contact the medical crew outside the abcS. the second of two negative-pressure failure alarms is activated during transport.
medications for pain, fever, nausea and antihistamines are prepped for patient arrival in the abcS and administered right away so that departure is accomplished as quickly as possible. during completion of this phase, the primary negative-pressure failure alarm is activated. initiating the recording of vital signs and activation of the iv pumps is
a medicaL crewmemBer’S firSthand encounter with the eBoLa viruS
a BruSh with
iral hemorrhagic fevers that cause high temperatures and bleeding disorders have been around for a long time, but not in our part of the globe. in august of this year, Phoenix air was called to transport
a physician home to america to be treated for the ebola virus disease in the only aircraft in the world capable of making that trip safely—especially from an infectious disease perspective.
eBoLaBy Mike APPLeGATe, Air Life GeorGA the firSt
PhySician i ever eScorted rePorted that
the flight itSelf had been the
firSt time he had reSted in dayS.
has worked even better than imagined and successfully brought the Samaritan’s Purse physician home—literally saving his life. at the time of this writing, there have been approximately 11 ebola-positive or exposed patients transported in the abcS successfully.
i have personally transported two ebola patients from Sierra leone—one to america and one to Paris. one transport out of africa required 13 hours of total flight time, with one stop for fuel, where we were not permitted to even open the door of the aircraft. many of these transports require overnight stops in other countries.
We usually fly with a three-person medical crew—two actively monitor the patient, while the other is staged as a safety officer in close proximity. all of us are well-trained in donning and doffing the isolation gear and moving into and out of the abcS environment. our mindset is conditioned as, “go slow to go fast!”—simple but valuable advice that i received from working at air methods for air life georgia.
the demands of the learning curve regarding getting into and out of the total isolation gear are considerable; however, we complied strictly with the guidelines set forth by the cdc and our own consulting emergency and critical care physicians. after one of our training sessions, i remember asking the flight team’s medical director if we were “swatting a fly with a sledge hammer.” his answer was an immediate and emphatic, “yes!” rehearsal of over-caution was essential, and the choreography of getting the patient on board the jet was discussed at great length during the flight over the atlantic.
L to r: the aBcS unit sitting outside phoenix air’s gulfstream iii jet; the aBcS unit onboard the jet; ebola patient boarding the phoenix air jet.
cont’d page 6
november/december 2014 / Safety connect 54 Safety connect / november/december 2014
eBoLawhat you ShouLd K n o W a b o u t
overview• ebola virus disease (evd), formerly known as ebola
hemorrhagic fever, is a severe, often fatal illness in humans.
• the virus is transmitted to people from wild animals and spreads in the human population through human-to-human transmission.
• the most common symptoms are fever, vomiting and diarrhea. Some patients have a rash and unexplained bleeding.
• the incubation period for the ebola virus is 21 days; typically, the onset of symptoms is eight to 10 days.
the ebola virus disease (evd), first identified in 1976, was named after the ebola river located in the remote villages of central africa, near tropical rainforests. the most recent outbreak in West africa has involved major urban as well as rural areas.
in late September, when the first u.S. case was identified in dallas, texas, air methods quickly began disseminating information to its employees. the following information is from the most recent updates from the centers for disease control and Prevention (cdc) and World health organization (Who) as of november 12, 2014.
treatment & prevention• treatment is geared toward symptoms. early
supportive care with rehydration and symptomatic treatment improves survival. there is as yet no licensed treatment proven to neutralize the virus, but a range of blood, immunological and drug therapies are under development.
• there are currently no licensed ebola vaccines, but potential candidates are undergoing evaluation.
• health officials are scrambling to begin human testing of a handful of experimental drugs for ebola, but the effort has sparked an ethical debate over randomizing versus giving the medications to all participants in the study.
• researchers have developed a single-dose; needle-free ebola vaccine that protects monkeys against
infection for more than four months. the vaccine is administered through the nose, protecting the primates via the respiratory tract.
•one key advantage, according to researcher maria croyle of the university of texas at austin, is that the vaccine could potentially prevent transmission of the virus from unintentional needle sticks through the unsafe handling of medical waste. news of the vaccine is reported in molecular Pharmaceuticals, a journal of the american chemical Society. the inhaled vaccine uses a harmless adenovirus (which causes the common cold) to deliver the vaccine. in a study involving macaque monkeys, none of the three primates that received the vaccine
become infected when exposed to the ebola virus at least 21 weeks later.
• the investigators say more work is needed on the formula. an under-the-tongue formulation of the vaccine is also in development. at least two other candidate vaccines against ebola are in clinical trials in the united States and africa.
air medicaL impLicationSin october 2014, conference calls in the format of a town hall meeting were held to discuss the latest information regarding the ebola virus disease and to give staff an opportunity to ask questions.
at the present time, air methods will not knowingly transport a patient that has been diagnosed with the ebola virus. as per the cdc recommendations, we are not equipped with the proper isolation equipment. the cdc will dispatch a highly-specialized team with the training and resources to properly transport these patients (see previous article). air methods will continue to screen patients for exposure and potential risk via a three-point process that includes aircom, med crews and aviation using the ebola virus disease (evd) Screening for emS, provided by the cdc.
We cannot stress enough the importance of assuring the required PPe is onboard your aircraft. this includes masks (n95 and regular disposable masks), gloves, face shield/goggles, gowns.
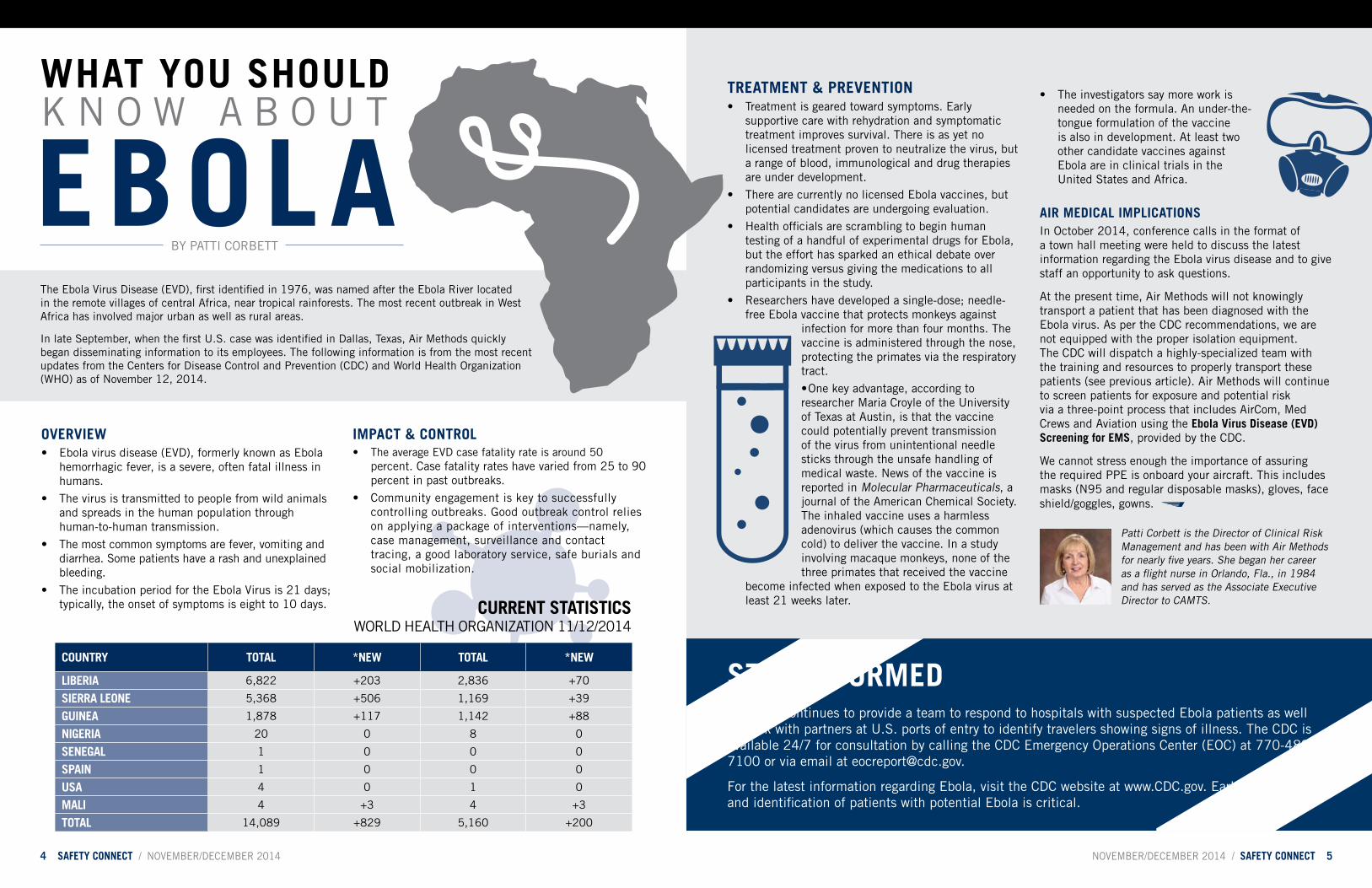
country totaL *new totaL *new
LiBeria 6,822 +203 2,836 +70
Sierra Leone 5,368 +506 1,169 +39
guinea 1,878 +117 1,142 +88
nigeria 20 0 8 0
SenegaL 1 0 0 0
Spain 1 0 0 0
uSa 4 0 1 0
maLi 4 +3 4 +3
totaL 14,089 +829 5,160 +200
Patti corbett is the director of clinical risk management and has been with air methods for nearly five years. She began her career as a flight nurse in orlando, fla., in 1984 and has served as the associate executive director to camtS.
by Patti corbett
impact & controL• the average evd case fatality rate is around 50
percent. case fatality rates have varied from 25 to 90 percent in past outbreaks.
• community engagement is key to successfully controlling outbreaks. good outbreak control relies on applying a package of interventions—namely, case management, surveillance and contact tracing, a good laboratory service, safe burials and social mobilization.
Stay informedthe cdc continues to provide a team to respond to hospitals with suspected ebola patients as well as work with partners at u.S. ports of entry to identify travelers showing signs of illness. the cdc is available 24/7 for consultation by calling the cdc emergency operations center (eoc) at 770-488-7100 or via email at [email protected].
for the latest information regarding ebola, visit the cdc website at www.cdc.gov. early recognition and identification of patients with potential ebola is critical.
current StatiSticS World health organization 11/12/2014

november/december 2014 / Safety connect 76 Safety connect / november/december 2014
on September 23, 2014, air methods director of clinical risk management Patti corbett was awarded the lynn Stevens excellence in Safety award by the air & Surface transport nurses association. this award is presented for excellence in safety to an individual who has made significant contributions to safety initiatives that have impacted the safety and culture of a specific program or the transport community as a whole. criteria included individual steps above and beyond industry norms that distinguish the individual by implementation of an innovation, policy or practice centered on safety excellence.
Please join us in congratulating Patti corbett for her years of service and commitment to excellence in safety in receiving this prestigious award. We applaud you, Patti!
•rePort your Safety concernS
•management evaluateS the riSK
• change iS imPlemented
• effectiveneSS of the change iS meaSured
KnoW your SmS
KEEP UP THE GREAT WOR
K!
patti corBett receiveS Lynn StevenS exceLLence in Safety award
Safety management SyStemalthough ebola has caught the attention of people worldwide, don’t forget about the flu. With the season upon us, getting a flu shot should be a priority. influenza is a serious illness occurring globally with an annual attack rate estimated at 5–10 percent in adults, and 20–30 percent in children. in 2013, the cdc reported that flu vaccinations prevented an estimated 6.6 million flu-related illnesses and 79,260 hospitalizations.
you may be able to pass on flu to others before you have symptoms. most healthy adults may be able to infect others one day before symptoms occur, and up to seven days after becoming sick. flu vaccinations are covered by most insurance providers when administered by a primary-care physician or at most national pharmacy chains utilizing an fSa/hSa account card. We cannot stress enough the importance of getting a flu vaccination.
accomplished by the outside crew member, with the other crewmember remaining inside with the patient to ensure equipment is working properly before exiting the abcS. once the patient is briefed and secured for takeoff, the medical crewmember in direct contact exits the patient compartment into the antechamber, seals the door and hits the start button on the five-minute timer to begin doffing the isolation gear.
during the interim, the “clean” medical crewmember (still gowned in isolation gear) places the plastic drapery into red bio-hazard bags for eventual disposal. the plastic is still considered “clean” because the booties remained clean, and the patient is instructed to lean only on the med crew escort if movement support is needed. the plastic also serves to isolate the cockpit for the benefit of the pilots when boarding. the clean crew member observes the crew coming from the patient compartment to assist them in doffing their gear. the extra set of eyes is essential, since during the doffing process is when most contamination
occurs. once this phase is complete, the primary negative-pressure failure alarm is activated.
once back on the ground in the u.S., the whole process is required to happen in reverse. the job of the designated safety officer is to stay a safe distance from the patient and without the encumbrance of any isolation gear to ensure that the handoff is executed as safely as possible. to date, no crew members have been infected. the isolation procedures of the medical crews, the abcS and the reverse-engineered ventilation system for the aircraft have all performed as designed, and the health of everyone involved in the evacuations has remained uncompromised.
mike applegate is a senior flight nurse and clinical base educator for air life georgia at the Kennesaw base. When he’s not at the base or with his wife, Stacey, and their six children, mike is circling the globe with Phoenix air.
a BruSh with eBoLa cont’d
get your fLu Shot!

november/december 2014 / Safety connect 98 Safety connect / november/december 2014
winter weather Safety winter weather Safety
it’s that time of year again when questions begin flowing in about how to keep our maintenance technicians warm in the winter. Some may have the latest and greatest state-of-the-art heating systems like radiant heat or infrared heating, while others rely on torpedo heaters and/or other heating devices.
the torpedo heater has been around for as long as i can remember and has been in many garages and worksites. though torpedo heaters are a great source of heat during the winter months, they don’t come without issues and concerns associated with operating them in a confined work space or enclosed hangar. the question has always been, “can we use torpedo heaters in the hangar?”
the biggest issue with torpedo heaters is that they operate by burning various types of fuel, such as kerosene, propane, gasoline or diesel fuel, which all emit carbon monoxide and could lead to carbon monoxide poisoning. according to the u.S. national library of medicine, carbon monoxide (co) is an odorless and colorless gas that causes thousands of deaths each year in north america and is the leading cause of poisoning death in the united States. because co has no warning properties, you should be aware of the symptoms,
heating hangarS SafeLyprecautionS and conSiderationS when uSing torpedo heaterS
which are flu-like in nature and include dizziness, fatigue, headache, nausea and irregular breathing. you should seek medical attention if you experience any of these symptoms while working around an appliance that emits carbon monoxide. you must ask yourself, “do i want to use a torpedo heater in the hangar while performing maintenance on my aircraft?”
another concern with torpedo heaters is the fact that they produce an open flame when operating, which creates an even bigger problem when it comes to employees’ health and safety in the workplace. though some may say the torpedo heater doesn’t really have an open flame because they can’t see it, the flame is still there, and some units get hot enough to cause the metal shields to glow. in addition, an open flame is never a good idea if you’re performing any type of fuel-cell maintenance; new company guidance will soon state as much.
currently, our published guidance in the SmS Policies & Procedures manual, section 11.13.9 heating, states we cannot use hydrocarbon-fueled heating appliances (torpedo heaters) inside buildings. however, we are aware oSha regulation 1926.154 temporary heating devices states flammable liquid heaters may be used indoors as long as sufficient quantities of fresh air are supplied to maintain the health and safety of the worker.
our director of maintenance is in the process of conducting a risk assessment with the safety department to identify ways to mitigate potential negative risks and exposures from operating torpedo heaters in the hangars while maintaining our employees’ health and safety in the workplace. if we can keep mitigating controls in place at all times, we should be able to use the heaters in the hangars—especially given the new technology and safety features in the market today. a couple of examples of risk mitigation would be (1) to have the hangar door(s) partially opened to ensure adequate ventilation, (2) to use carbon monoxide testers near the employees while the torpedo heater is in operation, (3) to maintain adequate clearance from all combustibles and (4) to never point torpedo heaters directly toward aircraft.
We are reaching out to our employees to get their input on ways and ideas to safely operate torpedo heaters and/or other heating devices in the hangar. if you have ideas you think would be helpful, please send them to michael Koenes in the safety department at [email protected].
the holiday season is a joyous time for get-togethers with family and friends, but it is also a time when fires can be started when too many electrical cords from holiday lights are all plugged into the same outlet or when electrical heaters are plugged into worn-out, outside extension cords in order to warm hangars and aircraft.
the hazards with electrical power and electrically-powered equipment and appliances are not generally considered until a personal injury or property damage occurs. very little, if any, thought is given to where this source of energy
comes from or just how dangerous it can be. in fact, since november of last year, there have been at least three reported events involving electrical power—one of which resulted in significant damage to the interior of one of our aircraft, another that involved damage to an aircraft start cart, and the third involving a shore power line.
fortunately, there were no personal injuries associated with these events, but the results were expensive. all three incidents involved the use of extension cords (or, more accurately put, the improper use of extension cords), and all three events ultimately resulted
in fires. in order to prevent similar occurrences, some basic electrical safety considerations must be utilized.
Prior to using extension cords, a simple assessment should be made to determine the type and size of the extension cord to be used. this is dependent on the amount of electrical power required by a given piece of equipment or appliance. length and gauge should be considered. an ordinary household extension cord used to power lamps and small appliances are 16 gauge or smaller, while large-gauged extension cords are rated at 16 gauge for light duty, 14 gauge for medium duty, 12 gauge for heavy duty and 10 gauge for extra heavy duty.
the length of the cord should also be taken into consideration. extension cords should not be connected together in a series (“daisy chaining”). rather, a single longer cord should be substituted for two or more shorter cords. industrial-use extension cords are available in various lengths (commonly 25, 50 and 100 feet).
When routing extension cords, special care should be taken to avoid “kinking” or “pinching,” as this increases the amount of resistance in the cord and will result in the cord overheating. extension cords should not be routed through confined spaces or under stationary equipment.
When extension cords are not in use, they should be completely disconnected from the power source and properly
stowed. if extension cords remain connected to an electrical source but are not connected to an appliance or equipment, they will still draw electrical power from the source and, if coiled (even loosely), will generate heat, thus posing a fire hazard.
When a cord on an appliance or equipment shows signs of wear or when the outer insulation is damaged, that cord should be taken out of service. While a cord at first glance may not show outward signs of damage, there may be some separation of the interior insulation. this is identified by unusual lumps or flat spots in the cord. also, extension cords used exclusively outdoors will deteriorate faster due to the effects of ultraviolet rays and other weathering considerations. When a damaged or worn cord is found, it should be replaced. under no circumstances should cords smaller than 14 gauge be repaired by splicing. in cases involving extension cords of 14 gauge or larger, they may be spliced/ repaired, but this must be done only by qualified personnel.
Whether it’s the holiday season or any other time of the year, a recommended best practice for extension cords is to inspect them regularly. and for those outdoor cords, set a pre-determined service life and then throw them away when they reach their due date. it is better to replace an extension cord than a hangar or aircraft, or even more importantly, a human life. Please enjoy the holidays. and use your extension cords safely!
by michael KoeneS
check thoSe cordS!‘tiS the SeaSon for fire hazardS
by Jonathan Primm
Jonathan Primm has been a regional safety director for air methods since august 2012 and was previously the eastern regional Safety director at omniflight helicopters. he has extensive industrial and environmental safety knowledge gained over eleven years while working for a helicopter company in the gulf of mexico, mr. Primm and his wife, Susana, reside in newnan, ga.
the biggeSt iSSue With torPedo heaterS iS that they oPerate by burning fuel, Which emitS carbon monoxide.

november/december 2014 / Safety connect 1110 Safety connect / november/december 2014
as winter sets in for most of the u.S., changes in temperature and weather will start to alter operations, specifically, the limitations found in automated weather reporting.
as an example, let’s suppose you have looked at the weather most of the afternoon and have a pretty good idea about what’s going on—at least meteorologically. currently it’s ok, not great, and the outlook for the next four hours is similar. after that, the forecast calls for deteriorating conditions. With that summary stashed in your memory, you have one last look at the airport metar nearest the destination hospital:
Kamc 112053z auto 30007Kt 8Sm bKn018 ovc033 m03/m06 a3005 rmK a02 SlP194
When you arrive at the hospital things start getting weird. you call the aSoS at the nearby airport and hear:
SPeci Kamc 112120z auto 32009Kt 8Sm bKn013 ovc018 m03/m05 a3005 rmK a02
that doesn’t seem too bad, except as you stand outside the aircraft you observe (un-forecast) freezing drizzle beginning to speckle the windscreen and the surface of the pad. So, let’s assume the nearby airport has the same weather as the pad. the reason cases like this can occur is due to limitations in automated weather reporting. Some readers, i’m sure, have experienced such scenarios.
here are some things to keep in mind when looking at automated metar reports:
• relative to the scenario above, aSoS stations do not report some types of drizzle (yes, there are multiple types) unless they are augmented by an actual human observer. Particles smaller than 1mm in diameter will go unreported. likewise, precipitation may be absent unless the rate meets a certain criteria. in the above scenario (which is based on a true story), the freezing drizzle goes undetected.
• aSoS systems do have freezing rain detectors, although certain rates of accumulation must be met before freezing rain will be reported. occasionally, conditions can prompt a report of “light snow.” however, the actual conditions are light freezing rain.
• Sensors are reporting averages over a 10-minute (or longer) time period. conditions that are reported may not be entirely accurate when a rapidly-moving front or convective activity is changing field conditions.
KnoW your automated weather
• on the flip side, calm conditions can also provide misleading reports. When a hole in the clouds happens to be residing directly above the station, the ceiling can be reported as clear. or if a cloud layer is stationary over an otherwise clear area, the sky coverage will be misleading.
• during conditions of fog or precipitation, sky coverage may be reported as lower than actual conditions. this is due to some interference with the laser used to measure cloud bases.
• hazy daylight conditions may lead to reports with much higher visibilities than what you will actually see.
• though out-of-season, automated systems cannot detect convective activity, funnel clouds or tornadoes.
despite the quirks of automated systems, overall they are incredibly reliable and provide a backbone of weather information that allows us to operate in a safe and weather-educated manner. Just remember, in certain conditions, you should cross-reference metar data with radar or any other weather data you can access. as an additional resource, the occ is available 24/7 to assist in gaining weather information and weather decision-making.
in august of this year, a fixed-wing air ambulance operating in new mexico suffered a fatal crash. the national transportation Safety board's preliminary report (ntSb identification: cen14fa462) indicates that the aircraft was refueled with the wrong fuel type, which led directly to the loss of the aircraft, all crew and their patient. We will need to wait for the final report in order to fully understand all of the events that led to this fatal error. What could have distracted this refueler and the pilot from ensuring that the appropriate fuel type was delivered?
recently, i had the opportunity to observe a transport aboard one of our company aircraft. our final destination was an airport, and while the medical crew took the patient over to the hospital, i waited with our pilot. We would need some fuel for the flight home. the fixed-base operator (fbo) ramp worker/refueler who met us was a pleasant gentleman and was on a first-name basis with our pilot. it was nice to see the
amicable relationship. the pilot ordered up his fuel and then headed into the fbo to wait for his crew's return. he clearly trusted that this refueler was going to choose the correct fuel truck, appropriately ground the aircraft and deliver the amount of fuel as requested. despite how well he knew the refueler and despite how many times this gentleman had refueled this aircraft, this was a risky gamble. What kind of day was this refueler having? Was today the day he might be so distracted that his actions lead to a fatal error?
after completing the refueling and while i was sitting in the fbo, i overheard an interesting conversation as the refueler made a phone call. he was, in fact, having a bad day. his relief had not shown up to work, so he was forced to stay until other coverage could be found. Was he going to miss an important family event or another appointment because he was stuck at work? What was he actually thinking about when our fuel load was ordered and he went to get the fuel truck? Was
a refueLer’S Bad day
he so distracted that he had made an error? no, fortunately he had chosen the appropriate truck, drove within a safe distance of the aircraft, correctly grounded the aircraft to the truck and delivered the appropriate volume of fuel. but when our pilot walked away, he had no idea what the outcome might be or what kind of a day this refueler was having.
our relationships with coworkers and support personnel are at the core of creating a pleasant work environment. unfortunately, those relationships can lead to complacency as we are certain that our friend or colleague would never make an error. but the fact remains we each will make non-intentional errors as we all succumb to different distractions. So, while we can trust, that trust must never be unconditional—especially when the task has potentially fatal consequences if not executed properly.
Several months ago, failure to monitor aircraft refueling of
one of our company fixed-wing aircraft led to a chain of events that resulted in substantial wheel and brake damage to the aircraft as the pilot attempted to burn off excess fuel. he had not monitored the fueling of his aircraft and too much fuel was pumped on board—a costly event for our company, but fortunately not a fatal one. taking the time to monitor refueling is not only a good idea; it's a requirement of our general operations manual (gom). Why is it a requirement in our gom? because it's a critically good idea with potentially fatal consequences when a distraction occurs!
Jeff currin is air methods’ new foQa manager. he has a great deal of experience in psychology/human factors research, having completed a m.S. in psychology and served as a contract researcher for naSa ames. additionally, Jeff is a commercial fixed-wing pilot and has previously worked flying skydivers and flying oregon’s backcountry.
by Jeff currin
Jonathan gryniuk is a regional safety director and began his helicopter emS career in 1992 with hartford life Star. he holds a degree in respiratory care and has been both a flight respiratory therapist and flight paramedic. Jonathan currently serves as board secretary to camtS. he and his family reside in castle rock, colo.
our reLationShipS with coworkerS and Support perSonneL are at the core of creating a pLeaSant work environment. unfortunateLy, thoSe reLationShipS can Lead to compLacency aS we are certain that our friend or coLLeague wouLd never make an error.
by Jonathan gryniuK
winter weather Safety

november/december 2014 / Safety connect 1312 Safety connect / november/december 2014
reporting timely and accurate information to others is a key part of effective communication. as a Pic, you are responsible for maintaining two-way communication with your communications center, which includes keeping them up-to-date with the status of your flight. When you encounter an unplanned event or deviation, it is important to relay that fact back to the communication specialist so they are able to update your required electronic flight plan.
one of the operational control center’s (occ) responsibilities is to monitor both pilots and communication centers to ensure that they remain safe and compliant with internal policies and procedures as well as external regulations. the ability to accomplish this is reduced when seemingly trivial details are left out of reports or anytime a message is inadvertently changed as it is passed from person to person. a recent example of this was a report the occ received that a pilot had “cut off his finger and went to the emergency room” without any additional information. When the full story was revealed some time later, the injury turned out to be a minor cut while preparing a meal and did not result in the base being out of service.
When an event occurs and it is relayed through your communication center, it is helpful to follow up with the occ once time permits to ensure accuracy and answer
operationaL controL center (occ) update
a meSSage from your occ
any additional questions that may arise. there is a misconception that when pilots get a message to contact the occ, it indicates they are in trouble or did something wrong. often, it just means operational control center analysts are simply seeking more information to determine how to handle a situation. it is in everyone’s best interest to ensure the original report is as complete and accurate as possible to avoid the potential for an inappropriate response to the situation.
remember: a very effective way to communicate routine and non-urgent information to the occ staff is through the use of its email account. if you send an email to [email protected], it will go to all ten of the occ analysts. once they are able to help, someone will respond. of course, don’t hesitate to call the occ at (866) 676-3442 in the event you need immediate assistance with operations-related issues.
michael benton is the aviation compliance manager and occ supervisor for air methods. his experience includes check airman, training manager and line pilot. he is a 15-year uS army combat veteran who served in both bosnia and iraq. michael enjoys life in colorado with his wife, linda, and their four children.
the imPortance of timely & accurate communicationby michael benton
event review committee (erc)
there have recently been a number of inspection overflights reported in aSaP and mSaP reports. Some of these are the result of system error (and the company is correcting the cause), but others are simply the result of pilot and/or mechanic error: Pilots did not scroll down far enough on the flight release to see items due, or they flew too close to the due time and received an unexpected scene call to an unusually-far distance. in other cases, the pilots simply did not understand the tolerance policy. because air methods has an approved aircraft inspection Program (aaiP), many inspections allow for an exceedance that would otherwise be in violation under fars. be aware that not all inspections have a tolerance.
inspection tolerances in the aaiP are controlled by the manufacturer’s requirements. if the manufacturer has no tolerance allowed for an inspection item, the inspection
a reminder from your aSap & mSap ercs
item will be found in a no tolerance (nt) inspection or placed in a convenient lower frequency inspection. if the manufacturer has a tolerance for an inspection item and the tolerance is less than 10 percent, the inspection item will be found in a restricted tolerance (rt) inspection or placed in a convenient lower frequency inspection. if the tolerance is at least 10 percent, the inspection will be placed in an inspection without designators. a statement of “no tolerance allowed” or “tolerance is restricted to xx hours and/or xx days,” as required, shall be placed in the note section of the header on the aaiP inspection form.
use of an inspection tolerance is considered non-routine. it is a margin to protect both you and the company, and is not standard operating procedure. you should plan to never use it.
overfLightS & inSpection toLeranceS






























