Embed Size (px)
Citation preview

CLINICAL CANCER RESEARCH | RESEARCH BRIEFS: CLINICAL TRIAL BRIEF REPORT
Safety andFeasibility of PARP1/2 Imagingwith 18F-PARPiin Patients with Head and Neck Cancer A C
Heiko Sch€oder1,2, Paula Dem�etrio De Souza Franca1,3, Reiko Nakajima1, Eva Burnazi4, Sheryl Roberts1,Christian Brand1, Milan Grkovski5, Audrey Mauguen6, Mark P. Dunphy1,2, Ronald A. Ghossein7,Serge K. Lyashchenko1,2,4, Jason S. Lewis1,2,4,8, Joseph A. O'Donoghue5, Ian Ganly9, Snehal G. Patel9,Nancy Y. Lee10, and Thomas Reiner1,2,11
ABSTRACT◥
Purpose: We performed a first-in-human clinical trial. The aimof this study was to determine safety and feasibility of PET imagingwith 18F-PARPi in patients with head and neck cancer.
Patients and Methods: Eleven patients with newly diagnosedor recurrent oral and oropharyngeal cancer were injected with18F-PARPi (331 � 42 MBq), and dynamic PET/CT imaging wasperformed between 0 and 25 minutes postinjection. Static PET/CTscans were obtained at 30, 60, and 120 minutes postinjection. Bloodsamples for tracer concentration and metabolite analysis were collect-ed. Blood pressure, ECG, oxygen levels, clinical chemistry, and com-plete blood countwere obtainedbefore and after tracer administration.
Results: 18F-PARPi was well-tolerated by all patients without anysafety concerns. Of the 11 patients included in the analysis, 18F-PARPi
had focal uptake in all primary lesions (n¼ 10, SUVmax¼ 2.8� 1.2)and all 18F-FDG–positive lymph nodes (n ¼ 34). 18F-PARPi uptakewas seen in 18F-FDG–negative lymphnodes of 3patients (n¼ 6). Focaluptake of tracer in primary andmetastatic lesions was corroborated byCT alone or in combination with 18F-FDG. The overall effective dosewith 18F-PARPi PET was 3.9 mSv – 5.2 mSv, contrast was high[SUVmax(lesion)/SUVmax(trapezius muscle) ¼ 4.5] and less variablethan 18F-FDG when compared with the genioglossus muscle (1.3 vs.6.0, P ¼ 0.001).
Conclusions: Imaging of head and neck cancer with 18F-PARPi isfeasible and safe. 18F-PARPi detects primary and metastaticlesions, and retention in tumors is longer than in healthytissues.
IntroductionDiagnosis and treatment of many malignant tumors have dramat-
ically improved in recent decades, and oral and oropharyngeal squa-mous cell carcinoma are no exception to this trend. However, mostpatients with oral and oropharyngeal squamous cell carcinoma stillpresent with advanced disease and regional or distantmetastases at thetime of diagnosis.
Presence of pathologic regional lymph nodes is the most powerfuland consistent predictor of outcome for oral cancers (1), and the abilityto accurately assign the exact extent of metastatic spread within theneck lymphatic system is therefore of great significance (1, 2). Com-plete surgical removal of metastatic disease in the neck has a clearimpact on prognosis, but it often remains unclear until histopathologicanalysis is complete, if a lymph node was metastatic or not (3, 4).
Clinical palpation of the neck is inadequate, as are the availableradiologic investigative tools. This is because many patients presentwith enlarged lymph nodes due to inflammation around the tumorsite. These inflamed lymph nodes may mimic neck metastases on CTscans and are often 18F-FDG PET avid (5). On the other hand, somemetastatic neck nodes may not be enlarged and show no abnormal18F-FDG uptake. For these reasons, elective neck dissection or irra-diation are often recommended in patients with head and neck cancerfor prophylactic treatment of occultmetastases. Ideally; however, theseprocedures, which can lead to increased comorbidities and reducedquality of life due to overtreatment (6, 7), would be avoided if thepresence of occult metastases could be definitively ruled out.
PARP PET imaging could potentially provide a solution for thisunmet clinical need. Because of its importance for cell survival, PARPis overexpressed in many malignancies, including oral and oropha-ryngeal squamous cell carcinoma (8, 9). Several radiolabeled PARPinhibitors were tested in preclinical studies, showing correlation ofuptakewith PARP1 expression, and suggesting that imaging is possiblewith little unspecific uptake in healthy head and neck tissue (10, 11).
The purpose of this study was to clinically translate 18F-PARPi, aPARP inhibitor derived from the core scaffold of olaparib (12), and toprovide a first step toward validating the tracer as a clinical tool. OtherPARP inhibitor–based imaging agents, based on different core scaf-folds, were translated earlier (13, 14). In this first-in-human phase Iclinical trial in patients with oral and oropharyngeal cancer, we
1Department of Radiology, Memorial Sloan Kettering Cancer Center, New York,New York. 2Department of Radiology, Weill Cornell Medical College, New York,New York. 3Department of Otorhinolaryngology and Head and Neck Surgery,Federal University of S~ao Paulo, S~ao Paulo, Brazil. 4Radiochemistry and Molec-ular Imaging Probes Core, Memorial Sloan Kettering Cancer Center, New York,New York. 5Department of Medical Physics, Memorial Sloan Kettering CancerCenter, New York, New York. 6Department of Epidemiology & Biostatistics,Memorial Sloan Kettering Cancer Center, New York, New York. 7Department ofPathology, Memorial Sloan Kettering Cancer Center, New York, New York.8Molecular Pharmacology Program, Memorial Sloan Kettering Cancer Center,New York, NewYork. 9Department of Surgery, Memorial Sloan Kettering CancerCenter, New York, New York. 10Department of Radiation Oncology, MemorialSloan Kettering Cancer Center, New York, New York. 11Chemical Biology Pro-gram, Memorial Sloan Kettering Cancer Center, New York, New York.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Authors: Thomas Reiner, Memorial Sloan Kettering CancerCenter, 1275 York Avenue, New York, NY 10065. Phone: 646-888-3461; Fax:646-422-0408; E-mail: [email protected]; and Heiko Sch€oder,[email protected]
Clin Cancer Res 2020;26:3110–6
doi: 10.1158/1078-0432.CCR-19-3484
�2020 American Association for Cancer Research.
AACRJournals.org | 3110
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

determined the safety and feasibility of 18F-PARPi imaging. We alsocorrelated 18F-PARPi uptake in tumors and normal tissue to standardof care 18F-FDG imaging.
Patients and MethodsFurther description of the experimental procedures and methods,
including radiopharmaceutical preparation, tracer formulation andquality control can be found in the Supplementary Materials.
Study designThis exploratory, phase I, single-center, open-label, prospective
Health Insurance Portability and Accountability Act (HIPAA) com-pliant study was approved by theMemorial Sloan Kettering (MSKCC)Institutional Review Board and conducted in accordance with theDeclaration of Helsinki (Clinicaltrials.gov NCT03631017). Writteninformed consent was obtained from all patients. The primary objec-tives of this phase I trial were to evaluate the safety and feasibility of18F-PARPi. We report the biodistribution and radiation dosimetry,and describe the tumor uptake of 18F-PARPi compared with 18F-FDG.Patients were accrued between January 2019 and September 2019 andreferred to the MSK Molecular Imaging and Therapy Service for theirnewly diagnosed or recurrent oral or oropharyngeal cancer. Twelvepatients were enrolled on this study protocol. Of these, 11 patientscompleted the study (8 patients with oropharyngeal squamous cellcarcinoma and 3 patients with oral cavity squamous cell carcinoma).One patient withdrew consent before administration of 18F-PARPi. Nopatients were excluded from the analysis. Inclusion and exclusioncriteria are summarized in Supplementary Table S1.
ProceduresAll patients underwent clinical examination, baseline vital signs,
pulse oximetry, ECG, and blood tests (<2 weeks prior to imaging). Nofasting was required prior to 18F-PARPi imaging. On the day ofimaging, two intravenous catheters were placed in each forearm, onefor injection of 18F-PARPi and one for drawing of IV blood samples.18F-PARPi was administered to patients at an average activity of 333�44 MBq (9.0� 1.2 mCi) by intravenous bolus injection. For the first 6patients, a dynamic PET scan (with the field of view including the
heart, lungs, liver, and kidneys) was acquired to study the biodistribu-tion and clearance of the tracer. For the subsequent 5 patients, thedynamic PET scan was centered on the head and neck region. In allinstances, the CT component of the dynamic PET/CT was acquiredwith a tube current of 40 mA. Immediately after the dynamic study, astatic PET/CT scan (extending from skull vertex to upper thighs in 6patients, and over the head and neck region in 5 patients) was obtained(30minutes postinjection; CT tube current: 80mA). Two further staticPET/CT scans were taken at approximately 60 and 120 minutespostinjection (CT tube current: 10 mA).
A total of 5 blood samples (at approximately 1, 5, 30, 90, and 150minutes postinjection) were drawn to quantify blood pool activity andto study 18F-PARPi metabolites. After imaging, vital signs wereobtained and an ECG performed, and blood samples were collectedfor hematology and blood chemistry analysis. A follow-up phoneinterview (1–3 days after the imaging study) was conducted todocument any side effects occurring after completion of the imagingstudy.
IHCParaffin-embedded slides from surgical specimen or core biopsies of
the primary tumor were obtained from consented patients and pro-cessed at the molecular cytology core facility at MSKCC (New York,NY). PARP1 IHC was performed using the Discovery XT processor(Ventana Medical Systems). The anti-PARP1 rabbit mAb (46D11,Cell Signaling Technology) specifically bound both human PARP1(0.4mg/mL). Paraffin-embedded formalin fixed 3-mm sections weredeparaffinized with EZPrep buffer, antigen retrieval was performedwith CC1 buffer (both Ventana Medical Systems), and sections wereblocked for 30minutes with Background Buster solution (Innovex).Anti-PARP1 antibodywas incubated for 5 hours, followed by 1 hour ofincubation with biotinylated goat anti-rabbit IgG (PK6106, VectorLaboratories) at a 1:200 dilution. For IHC detection, a DAB detectionkit (Ventana Medical Systems) was used according to the manufac-turer's instructions, sections were counterstained with hematoxylinand cover-slipped with Permount (Thermo Fisher Scientific). Incu-bating with a rabbit IgG instead of the primary antibody controlled fornonspecific binding of the secondary antibody. Slides were scanned(Mirax, 3DHISTECH) to allow for digital histologic correlation.Hematoxylin and eosin (H&E)-stained slides were used to determineareas of tumor and areas of normal muscle. Those exact same areaswere used for PARP1 quantification using a consecutive slide.
Blood clearance and metabolite analysisBlood clearance measurements were performed as previously
reported (15). Briefly, multiple venous blood samples were obtainedbetween 1 and 150 minutes after intravenous injection of 18F-PARPi.Activity in whole blood and plasma was measured in duplicate using acalibrated NaI (Tl) Wallac Wizard 2480 automatic g-counter (PerkinElmer, Inc.). The measured activity concentrations were converted topercentage injected activity per kilogram (%ID/kg). Metabolite anal-ysis of activity in plasma was performed by reverse-phase HPLC within-line radiation (Posi-RAM model 4, LabLogic) detection using aKinetex Biphenyl column (Phenomenex, 150� 4.6 mm; 5 mmparticlesize) and amobile phase gradient of 10%–75% acetonitrile (0.1% TFA)in water (0.1% TFA) over 20 minutes. Intact 18F-PARPi elutes at 16minutes and a number of metabolites elute from 7–8 minutes.
DosimetryAbsorbed radiation doses to normal tissues were estimated for the
first 6 patients of the study, based on dynamic and static PET/CT
Translational Relevance
Preclinically, labeled PARP1-targeted olaparib derivatives havebeen used to visualize several malignancies with high contrast,including head and neck cancer. These results suggest that PARP1-targeted imaging agents could potentially be used as a quantitativewhole-body imaging test for primary and metastatic lesions,improving diagnostic sensitivity and specificity compared withthe standard of care. This first-in-human study of 18F-PARP1 inpatients with head and neck cancer established that imaging withthe olaparib-based PARP1 imaging agent18F-PARPi is feasible andsafe, and that contrast ratios in the head and neck region arecomparable with 18F-FDG. Retention in tumors and metastaticnodes is longer than in physiologic tissues, including the salivaryglands. The number of PET avid lymph nodes is higher for18F-PARPi than for 18F-FDG, and a subset of 18F-PARPi–positive and 18F-FDG–negative lymph nodes resolved after che-moradiation. Further study of 18F-PARPi in head and neck canceris being pursued.
PARP1/2 Imaging with 18F-PARPi in Head and Neck Cancer
AACRJournals.org Clin Cancer Res; 26(13) July 1, 2020 3111
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

images. Activity concentration–time curves were generated by analysisof VOIs generated for liver, kidney, spleen, cardiac blood pool, bone,lung, gallbladder and urinary bladder. Red marrow activity concen-trationwas assumed equal to that of blood.Whole-body time–activity–time curves, generated using the 4 points defined by the administeredactivity (time zero) and the total activities in the three whole-body PETscans, were used to calculate monoexponential clearance half-times.The area under activity concentration–time curves (AUC) were esti-mated by trapezoidal integration with a terminal contribution calcu-lated by extrapolation from the lastmeasured value using the shorter ofapparent terminal clearance rate or physical decay. Whole-organAUCs were obtained by multiplying the activity concentration AUCby organmass. Baseline values of organmass were taken from the OakRidge National Laboratory (ORNL) phantoms of OLINDA/EXM 2.0(Hermes Medical Solutions) representing standard human. Organmasses were rescaled if body mass differed by more than 15% fromthe standard value (73.7 kg for males; 56.9 kg for females). Organresidence times were derived by dividing organ AUC values byadministered activity. For urinary bladder contents, residence timeswere estimated by theOLINDA/EXM2.0 voiding bladdermodel basedon the fraction of activity clearing via urinary bladder, the mono-exponential whole-body biological half-time, and an assumed voidinginterval of 1 hour. Residence times for the remainder of body werederived by subtracting all the individually estimated residence timesfrom the whole-body residence time. Absorbed radiation doses to thewhole body and various organs were calculated using OLINDA/EXM
2.0 with effective doses based on the tissue weighting factors of ICRPReport 103 (16).
PET/CT imaging and analysisAll PET/CT images were obtained on a Discovery 710 PET/CT
scanner (GE Healthcare), using low dose CT settings (10–80 mA,120 kV) for CT images that were used for attenuation correctionand anatomic correlation. All studies were reviewed using theHybrid Viewer display and analysis application (Hermes MedicalSolutions). 18F-PARPi PET/CT and 18F-FDG PET/CT studies wereinterpreted by two nuclear medicine physicians with at least 10 yearsof PET/CT experience. Three-dimensional threshold-based volu-metric regions of interest (VOI) were placed in reference regions[bilateral submandibular gland, parotid gland, blood pool of neck,contralateral posterior neck muscles (trapezius and semispinalis),genioglossus muscle, bone marrow, mediastinal blood pool, myo-cardium, normal liver, renal cortex, and spleen] and over all sites ofabnormal uptake in lymph nodes, or soft-tissue lesions with refer-ence to the PET/CT images. Abnormal 18F-PARPi and 18F-FDGuptake was defined as outside physiologic sites (such as palatinetonsils or skeletal muscle) and of intensity greater than regionalbackground. Uptake of 18F-PARPi in the soft-tissue lesions andlymph nodes was assessed by measuring the maximum standardizeduptake values (SUVmax).
Statistical analysisUptake values are presented as mean � SE, unless otherwise
specified. Distribution of uptake with 18F-PARPi and 18F-FDG (onlesions where both were available) were compared using a WilcoxonSigned Rank test for paired data, while their variances were comparedusing a Levene test. R version 3.6.0 was used for analysis.
ResultsPatient population
A total of 11 patients with cytologically or histologically confirmedsquamous cell carcinoma of the oral cavity or oropharynx completedthe study protocol. Supplementary Table S2 lists the patient demo-graphics and key diagnostic parameters, including stage and lymphnode status, and Fig. 1 shows a schematic overview of the studyworkflow. There were 10 males and one female, with a mean age of64 years. At the time of imaging, 8 patients had newly diagnoseddisease (all with the primary lesion in the oropharynx). The 3 patientsthat had recurrent disease at the time of imaging had previously beendiagnosed with oral cavity squamous cell carcinoma. One patient hadtheir primary lesion surgically removed before imaging. Nodalinvolvement (anatomically abnormal lymph nodes) was present in9 of the 11 patients, and disease stage ranged from I to IVb (8th edition,AJCC). Lymph nodes were considered to be abnormal when at leastone of following criteria was met: central necrosis or inhomogeneousenhancement (contrast-enhanced CT and /or MRI), shortest axialdiameter greater than 11 mm in cervical regions and change in shapeand/or ill-defined irregular margins in a lymph node. Twenty-sevenpercent of patients (n ¼ 3) were HPV-negative (all oral cavitysquamous cell carcinoma) and 73% were HPV-positive (all oropha-ryngeal cases).
Radiotracer characteristicsThe radiochemical synthesis of 18F-PARPi was performed using a
synthetic route similar to what we have reported before (Supplemen-tary Fig. S1; ref. 12).Wefirst synthesized para-[18F]fluoro-benzoic acid
Figure 1.
Schematic overview and flow chart of the 18F-PARPi phase I clinical trial.
Sch€oder et al.
Clin Cancer Res; 26(13) July 1, 2020 CLINICAL CANCER RESEARCH3112
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

as a radiolabeled synthon before conjugation with the 1(2H)phthala-zinone targeting group. On average, patients were therefore injectedwith 290 pmol of 18F-PARPi, 6.7 orders of magnitude lower than thetwice daily administered dose of olaparib (2 � 300 mg) and thereforeunlikely to elicit a pharmacodynamic response.
Adverse events and metabolismAll patients tolerated the injection of 18F-PARPi well, and no
adverse events were recorded related to the 18F-PARPi injection. Onepatient died within a 2-week window after completing the study, andone patient experienced grade 1 mucositis over the tumor site, whichresolved the following day. The death was considered unrelated to theadministered drug. The mucositis was considered possible related tothe administered drug. For all patients, clinical chemistry and hema-tology were determined and an electrocardiogram was performedbefore and after the administration of 18F-PARPi (SupplementaryTable S3). While some patients presented with abnormal findingsbefore imaging, no clinically relevant changes were observed afterradiotracer injection or at follow-up.
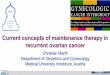
Biodistribution and dosimetryMaximum intensity projection PET images of a representative
patient injected with 18F-PARPi (images obtained at 30, 60, and 120minutes postinjection) are shown in Fig. 2A. At 120 minutes,uptake in the primary tumor had an SUVmax of 4.1, whereas themetastatic lymph node had an SUVmax of 3.6 (radiologic lymphnode level 2). Across the entire patient population, the averageprimary tumor SUVmax was 2.8 � 1.1 at 120 minutes. The primaryroutes of excretion were renal and hepatobiliary with most of thetracer excreted renally. Activity in the renal cortex diminished overtime (SUVmax ¼ 16 � 8 at 30 minutes, 9 � 4 at 60 minutes, and 7 �5 at 120 minutes) with commensurate accumulation in the urinarybladder. The maximal observed activity in the urinary bladdercorresponded to 20%–38% of the total administered, typically atthe 30–60 minute scan times.
Absorbed radiation doses to normal tissues from 18F-PARPi wereestimated on the basis of the tracer biodistribution of the first sixpatients. Key dosimetry data are plotted in Fig. 2B, and the entiredataset can be found in Supplementary Table S4. The effective dose of
Figure 2.
Biodistribution, histology, anddosimetry of 18F-PARPi.A,Maximum intensity projections at 30, 60, and 120minutes post 18F-PARPi injection in a67-year-oldmenwithoropharyngeal squamous cell carcinoma. Green arrow, primary tumor; red arrow, metastatic lymph node. B, Dosimetry of select organs, whole body, and effectivedose in patients (n ¼ 6) injected with 18F-PARP (see Supplementary Table S4 for the comprehensive dataset). C, PARP1 IHC and corresponding H&E images of theprimary lesion of a 49-year-old man with carcinoma in the right palatine tonsil and corresponding H&E images. D, PARP1 IHC and corresponding H&E images of theprimary lesion of a 51-year-old man with oral tongue carcinoma.
PARP1/2 Imaging with 18F-PARPi in Head and Neck Cancer
AACRJournals.org Clin Cancer Res; 26(13) July 1, 2020 3113
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

18F-PARPiwas 0.014� 0.002mSv/MBq, calculatedwith ICRP103. In atypical diagnostic setting, the effective radiation dose is projected to be3.9 mSv–5.2 mSv.
PARP1 was highly expressed in both oral and oropharyngealsquamous cell carcinoma in our patient population (Fig. 2C and D;Supplementary Fig. S2), corroborating earlier work (8, 9).
MetabolismResearch blood draws were obtained for 10 patients at five time-
points after tracer injection, activity counted, andmetabolites analyzed(Supplementary Fig. S3A). Using a two-phase decay curve, we deter-mined the weighted blood half-life to be 4.2 minutes (whole blood,Supplementary Fig. S3B). Only small quantities of metabolites weredetected at 1 and 5 minutes (99.2% � 1.5% and 89.9% � 11.4%18F-PARPi, respectively, Supplementary Fig. S3C). At 30 minutes, andwith decreasing blood pool concentration of the injected tracer, wedetected a radiometabolitewith a retention time of 7–8minutes (50.9%� 11.5%; Supplementary Fig. S4).
Organ residence timeInvestigating the specificity of 18F-PARPi, we looked at the resi-
dence times of the tracer in tumors, metastatic nodes, and healthytissues (Fig. 3). In spleen and liver, which both express large phys-iologic amounts of PARP1 and PARP2 (17), initial uptake was high,followed by rapid clearance over the 2-hour imaging period[SUVmax(spleen, 30 minutes) ¼ 6.1 � 1.3 and SUVmax(spleen,120min)¼ 2.2� 0.6, representing a 64% drop]. Similarly, the SUVmax
in bone marrow was high in the 30-minute PET/CT scan, but valuesdeclined by 53% between 30 and 120 minutes. Comparably, fastclearance was found for physiologic structures within the head andneck region. Uptake in the submandibular and parotid glandsdecreased by 57% and 56%, respectively. In contrast, tracer retentionin tumor and metastatic nodes was significantly longer, with SUVmax
values declining by just 13% for both primary and PET-avid lymphnodes [SUVmax(tumor, 30 minutes) ¼ 3.4 � 0.8 and SUVmax(tumor,120 minutes) ¼ 3.0 � 1.1; SUVmax(lymph node, 30 minutes) ¼ 3.3 �1.3 and SUVmax (lymph node, 120 minutes) ¼ 2.9 � 1.1].
18F-FDG and 18F-PARPi in primary tumor and normal necktissues
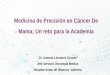
To determinewhether 18F-PARPi could be a relevant imaging tracerfor the head and neck region, we compared its retention with that ofstandard-of-care 18F-FDG (Fig. 4). For both imaging agents, uptakewas corroborated with tumor outlines defined by standard-of-careT1-weighted Gd-MRI imaging (Fig. 4C). Across the patient popula-tion, 18F-FDG had higher average tumor SUVmax values than18F-PARPi, but SUVmax values for
18F-FDG decreased for level 2 andlevel 3 lymph nodes. A smaller decrease in SUVmax values was foundfor 18F-PARPi (66% and 15% for 18F-PARPi and 18F-FDG, respec-tively, when grouping primary/level 1 lymph nodes and level 2/level 3lymph nodes; Fig. 4D). Uptake ratios [SUVmax(lesion)/SUVmax(tra-pezius muscle)] for 18F-FDG were higher than for 18F-PARPi (median¼ 10.4 vs. 4.5, P < 0.0001, Fig. 4E). Interestingly, when comparinguptake ratios [SUVmax(lesion)/SUVmax(genioglossus muscle)], wefound similar median values for 18F-FDG and 18F-PARPi (median¼ 3.0 vs. 3.3, P ¼ 0.23), although the variance was less for 18F-PARPithan for 18F-FDG (1.3 vs. 6.0, P ¼ 0.001, Fig. 4F). This could be ofpotential relevance in patients with recurrent oral cancers or in theposttreatment setting, leading to asymmetric uptake in the oral cavityor higher uptake in the genioglossus muscle secondary to partialglossectomy, tongue movement, or hypoglossal palsy (18–20).
18F-FDG and 18F-PARPi uptake matched with respect to the pres-ence and location of the primary lesion. However, the two tracers haddivergent uptake patterns in the lymphatic system (SupplementaryFig. S5). For 18F-FDG, 34 lymph nodes were PET-avid. For18F-PARPi, we observed 40 18F-PARPi avid lymph nodes. These 40lymph nodes included all of the lymph nodes that were detected using18F-FDG. No evidence of additional FDG-avid and PARPi-avid
Figure 3.18F-PARPi pharmacokinetics in physiologic tissue, 18F-PARPi avid lymph nodes,and primary tumor. A, 18F-PARPi tracer accumulation in a 67-year-old man withoropharyngeal squamous cell carcinoma is initially high in the submandibulargland (white triangles) and subsequently decreasing. In comparison, the primarytumor in the base of the tongue (black arrow) andmetastatic lymph node (blacktriangles) exhibit more sustained retention of the radiotracer. Top row, PETimage only; bottom row, PET/CT. B, Time–activity curves of a 67-year-old manpatient, derived from the area with highest 18F-PARPi uptake (SUVmax, primarytumor, and metastatic lymph node) or from the whole structure (SUVmean,parotid gland, submandibular gland, and suboccipitalmuscle).C, SUVmax uptakevalues for normal structures (left) and primary tumor/metastatic lesions (right,each n ¼ 6 patients with whole-body PET scans).
Sch€oder et al.
Clin Cancer Res; 26(13) July 1, 2020 CLINICAL CANCER RESEARCH3114
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

adenopathy or distant metastatic disease was seen. Because of protocolregulations, no biopsy material was available for the additional 6 lymphnodes; however, a subset of them resolved after chemoradiation (which,however, does not provemalignancy, Supplementary Fig. S5A and S5B).
DiscussionRecently, PARP-targeted agents have received considerable atten-
tion as imaging agents (10, 21) based on the ubiquitous expression ofPARP in many types of cancers, with the promise to serve as anaccurate sensor of malignancy where standard-of-care methods cur-rently fail.
Radiation doses associated with 18F-PARPi PET imaging wererelatively low. The overall equivalent dose was 3.9 mSv–5.2mSv, lowerthan that reported for 18F-FDG (8.1 � 1.2 mSv; ref. 22). This was, inpart, due to the selective uptake of the tracer, paired with a short bloodhalf-life and fast clearance. 18F-PARPi rapidly cleared from thecirculatory system and accumulated in the urinary bladder andgallbladder following respective transit through the kidneys and liver.
PARP1 is located in the nuclei of cells. Consequently, the cellmembrane and nuclear membrane permeability of 18F-PARPi has tobe high, allowing both fast uptake of radiotracer and clearance ofunbound material for image contrast generation. This was seen inthe submandibular glands, where the SUVmax at 20–30 minutes washigher than in the primary tumor for 80% (n ¼ 10 evaluablepatients) of all patients (Fig. 3). Subsequently, the delivered activityin these healthy tissues cleared quickly, whereas the activity per-sisted longer in tumor and metastatic nodes (Fig. 3B). At 120minutes postinjection the situation had inverted, and none of thesubmandibular glands showed activity higher than the primarytumor. Similar rapid clearance of radiotracer was noted in otherhealthy organs, including the spleen, genioglossus muscles, parotidglands, and bone marrow. For future studies, imaging with PARPinhibitors after longer time intervals postinjection might yieldfurther improved contrast ratios.
Because this is a phase I study, we were unable to collect unstainedhistologic slides (for primary and metastatic lesions) from a statisti-cally meaningful number of patients. Consequently, the focus of an
Figure 4.
Comparison of standard-of-care 18F-FDG and 18F-PARPi in a 52-year-old man with cancer in the base of the tongue. A, 18F-PARPi PET at the level of the epiglottis(black triangles) showed an 18F-PARPi avid primary lesion in the base of tongue (white arrows) andmetastatic lymph node (right level 2, black arrow) at 120minutesafter 18F-PARPi administration.B, 18F-FDG PET at the same level showed 18F-FDG avid lesion in the base of tongue (white arrows) andmetastatic lymph nodes (blackarrow). C, Postcontrast T1-weighted axial MRI image (epiglottis level) showed a large expansile multicompartmental heterogeneously, ill-defined enhancing lesioncentered in the base of tongue with effacement of the bilateral valleculae and extension along the median and lateral glossoepiglottic folds into the epiglottis.D, Comparison of SUVmax values obtained for 18F-PARPi versus 18F-FDG in tumors and lymph nodes across the patient population. E, SUVmax-based uptake ratios(lesion and trapezius muscle) for 18F-PARPi and 18F-FDG without separation of primary lesion and lymph nodes. F, SUVmax-based uptake ratios (lesion andgenioglossus muscle) for 18F-PARPi and 18F-FDG without separation of primary lesion and lymph nodes.
PARP1/2 Imaging with 18F-PARPi in Head and Neck Cancer
AACRJournals.org Clin Cancer Res; 26(13) July 1, 2020 3115
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

upcoming phase II study will be to determine the sensitivity andspecificity of 18F-PARPi in head and neck cancer.
In conclusion, we performed the first-in-human translation of18F-PARPi, a PARP-targeted 1(2H)phthalazinone, and the first imag-ing of PARP in head and neck cancer. Administration of 18F-PARPiwas safe, and aside from a grade 1 mucositis, which was possiblyrelated, no adverse events were attributed to the tracer injection.18F-PARPi is a promising new agent for the imaging of head andneck squamous cell carcinoma.
Disclosure of Potential Conflicts of InterestJ.A. O'Donoghue is an employee/paid consultant for Janssen Research &
Development, LLC. S.G. Patel is an advisory board member/unpaid consultantfor Summit Biomedical Imaging LLC. T. Reiner is an employee/paid consultantfor and reports receiving commercial research grants from Theragnostics, othercommercial research support from Pfizer, Immunogen, and Summit BiomedicalImaging, and holds ownership interest (including patents) in and reportsreceiving other remuneration from Summit Biomedical Imaging. N.Y. Lee is anadvisory board member at Merck, Merck Serono, Pfizer, and Eli Lilly and receivescommercial research support from Astra-Zeneca and Pfizer. No potential conflictsof interest were disclosed by the other authors.
Authors’ ContributionsConception and design: H.M. Sch€oder, S.K. Lyashchenko, N.Y. Lee, T. ReinerDevelopment ofmethodology: E.M. Burnazi, C. Brand, S.K. Lyashchenko, J.S. Lewis,J.A. O'Donoghue, S.G. Patel, T. ReinerAcquisition of data (provided animals, acquired and managed patients, providedfacilities, etc.): H.M. Sch€oder, P.D.D.S. Franca, E.M. Burnazi, S. Roberts, C. Brand,M. Grkovski, J.A. O'Donoghue, I. Ganly, S.G. Patel, N.Y. Lee
Analysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): H.M. Sch€oder, P.D.D.S. Franca, R. Nakajima,E.M. Burnazi, M. Grkovski, A. Mauguen, R. Ghossein, J.A. O'Donoghue, T. ReinerWriting, review, and/or revision of themanuscript:H.M. Sch€oder, P.D.D.S. Franca,R. Nakajima, E.M. Burnazi, M. Grkovski, A. Mauguen, M.P.S. Dunphy, R. Ghossein,S.K. Lyashchenko, J.S. Lewis, J.A. O'Donoghue, I. Ganly, S.G. Patel, N.Y. Lee, T. ReinerAdministrative, technical, or material support (i.e., reporting or organizing data,constructing databases): H.M. Sch€oder, P.D.D.S. Franca, J.S. Lewis, S.G. Patel,T. ReinerStudy supervision: H.M. Sch€oder, N.Y. Lee, T. Reiner
AcknowledgmentsThis work was supported in part by NIH grants R01 CA204441, R35 CA232130,
and P30 CA008748, the Tow Foundation, the MSK Center for Molecular Imaging &Nanotechnology, the MSK Imaging and Radiation Sciences Program, and the MSKMolecularly Targeted Intraoperative Imaging Fund. We acknowledge and thankStephen Carlin and Kevin Staton for help with clinical radiochemistry; Aisha Shicklerand Yorann Roux for blood and metabolite analysis; Ryan Min for patient coordi-nation; Christopher Riedl, MD, PhD, for help with the clinical workflow; and SusanneKossatz, PhD and Wolfgang A. Weber, MD for helpful discussions and help withpreparing the clinical trial.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received October 23, 2019; revised January 15, 2020; accepted March 30, 2020;published first April 3, 2020.
References1. Zanoni DK,Montero PH,Migliacci JC, Shah JP,Wong RJ, Ganly I, et al. Survival
outcomes after treatment of cancer of the oral cavity (1985-2015). Oral Oncol2019;90:115–21.
2. Ho AS, Kim S, Tighiouart M, Gudino C, Mita A, Scher KS, et al. Metastaticlymph node burden and survival in oral cavity cancer. J Clin Oncol 2017;35:3601–9.
3. Gupta P, Migliacci JC, Montero PH, Zanoni DK, Shah JP, Patel SG, et al. Do weneed a different staging system for tongue and gingivobuccal complex squamouscell cancers? Oral Oncol 2018;78:64–71.
4. Zanoni DK,Migliacci JC, Xu B, Katabi N,Montero PH, Ganly I, et al. A proposalto redefine close surgical margins in squamous cell carcinoma of the oral tongue.JAMA Otolaryngol Head Neck Surg 2017;143:555–60.
5. Kim SJ, Pak K, Kim K. Diagnostic accuracy of F-18 FDG PET or PET/CT fordetection of lymph nodemetastasis in clinically node negative head and neck cancerpatients: a systematic review andmeta-analysis. Am JOtolaryngol 2019;40:297–305.
6. D'Cruz AK, Vaish R, Kapre N, Dandekar M, Gupta S, Hawaldar R, et al. Electiveversus therapeutic neck dissection in node-negative oral cancer. N Engl J Med2015;373:521–9.
7. Mehanna H, Wong WL, McConkey CC, Rahman JK, Robinson M, Hartley AG,et al. PET-CT surveillance versus neck dissection in advanced head and neckcancer. N Engl J Med 2016;374:1444–54.
8. Kossatz S, Brand C, Gutiontov S, Liu JT, Lee NY, Gonen M, et al. Detection anddelineation of oral cancer with a PARP1 targeted optical imaging agent. Sci Rep2016;6:21371.
9. Kossatz S, Pirovano G, Franca PDDS, Strome AL, Sunny SP, Zanoni DK, et al.PARP1 as a biomarker for early detection and intraoperative tumor delineationin epithelial cancers – first-in-human results. Nat Biomed Eng 2020;4:272–85.
10. Carney B, Kossatz S, Reiner T. Molecular imaging of PARP. J Nucl Med 2017;58:1025–30.
11. Wilson TC, Xavier MA, Knight J, Verhoog S, Torres JB, Mosley M, et al. PETimaging of PARP expression using (18)F-Olaparib. J Nucl Med 2019;60:504–10.
12. Carney B, Carlucci G, Salinas B, Di Gialleonardo V, Kossatz S, Vansteene A, et al.Non-invasive PET imaging of PARP1 expression in glioblastoma models.Mol Imaging Biol 2016;18:386–92.
13. Michel LS, Dyroff S, Brooks FJ, Spayd KJ, Lim S, Engle JT, et al. PET of poly(ADP-Ribose) polymerase activity in cancer: preclinical assessment and first in-human studies. Radiology 2017;282:453–63.
14. Makvandi M, Pantel A, Schwartz L, Schubert E, Xu K, Hsieh CJ, et al. A PETimaging agent for evaluating PARP-1 expression in ovarian cancer. J Clin Invest2018;128:2116–26.
15. Dunphy MPS, Harding JJ, Venneti S, Zhang H, Burnazi EM, Bromberg J, et al.In vivo PET assay of tumor glutamine flux and metabolism: in-human trial of(18)F-(2S,4R)-4-fluoroglutamine. Radiology 2018;287:667–75.
16. The 2007 recommendations of the International Commission on RadiologicalProtection. ICRP publication 103. Ann ICRP 2007;37:1–332.
17. Uhlen M, Fagerberg L, Hallstrom BM, Lindskog C, Oksvold P, Mardinoglu A,et al. Proteomics. Tissue-based map of the human proteome. Science 2015;347:1260419.
18. ChowZ,McIvor J,McDonnell O, Khaleel Z. False-positive uptake of 18F-FDG inhypoglossal nerve palsy following chemoradiotherapy for tongue base cancer.ANZ J Surg 2016;86:313–4.
19. Meerwein CM, Queiroz M, Kollias S, Hullner M, Veit-Haibach P, Huber GF.Post-treatment surveillance of head and neck cancer: pitfalls in the interpretationof FDG PET-CT/MRI. Swiss medical weekly 2015;145:w14116.
20. Metser U,Miller E, LermanH, Even-Sapir E. Benign nonphysiologic lesions withincreased 18F-FDG uptake on PET/CT: characterization and incidence. AJRAmJ Roentgenol 2007;189:1203–10.
21. Knight JC, Koustoulidou S, Cornelissen B. Imaging the DNA damage responsewith PET and SPECT. Eur J Nucl Med Mol Imaging 2017;44:1065–78.
22. Quinn B, Dauer Z, Pandit-Taskar N, Schoder H, Dauer LT. Radiation dosimetryof 18F-FDG PET/CT: incorporating exam-specific parameters in dose estimates.BMC Med Imaging 2016;16:41.
Clin Cancer Res; 26(13) July 1, 2020 CLINICAL CANCER RESEARCH3116
Sch€oder et al.
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484

2020;26:3110-3116. Published OnlineFirst April 3, 2020.Clin Cancer Res Heiko Schöder, Paula Demétrio De Souza França, Reiko Nakajima, et al. Patients with Head and Neck Cancer
F-PARPi in18Safety and Feasibility of PARP1/2 Imaging with
Updated version
10.1158/1078-0432.CCR-19-3484doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2020/04/03/1078-0432.CCR-19-3484.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/26/13/3110.full#ref-list-1
This article cites 22 articles, 3 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/26/13/3110.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/26/13/3110To request permission to re-use all or part of this article, use this link
on July 28, 2021. © 2020 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 3, 2020; DOI: 10.1158/1078-0432.CCR-19-3484