Embed Size (px)
Citation preview

Pulmonary Complication Of Sickle
Cell DiseaseSaleh Alharbi MD FAAP FCCP
ABP SBPAssistant Professor of Pediatrics
Omm Al-Qura University

Outlines
ACS PHT Plastic Bronchitis Preoperative Management Pulmonary Rehabilitation

Acute Chest Syndrome
Inclusion: all children and adolescents with sickle cell diseases
Definition: a new infiltrate on CXR, excluding atelectasis, plus one or more of the following :
tachypnea fever > 38.5 chest pain cough wheezing hypoxemia (room air SaO2 3-5% points less than baseline)

Acute Chest Syndrome Pulmonary infiltrates
sometimes with effusion with one or more of the following:
Chest pain 40% also have abdominal pain
Fever Impaired oxygenationMay also have chills
Often preceded by vaso-occlusive crisis• high phospholipase A-2 levels

Acute Chest Syndrome
intravascular clogging fat embolism atelectasis infection thromboembolism

Infectious Causes
Staph aureus Strep pneumoniae Hemophilus influenzae Klebsiella pneumoniae Chlamydia Mycoplasma Viral
most common

Causes of Acute Chest Syndrome

Pathogenesis
Gladwin et al. Lancet 2000;355:1477

Vicious Cycle
Sickling worsens with hypoxemia, acidosis Atelectasis causes vasoconstriction
sluggish flow and more occlusion Chest pain causes splinting
under aeration and atelectasis Narcotics for pain may decrease ventilation
increased atelectasis increased PaCO2 increases acidosis

Co-morbidities
asthma marked anemia thrombocytopenia pulmonary hypertension cor pulmonale

One thing leads to another
Acute chest syndrome often recurs Gradual scarring Restrictive lung disease Pulmonary hypertension
even without overt acute chest episodes Cor pulmonale 20% of patients with ACS develop neurologic
complications (often beginning with confusion)

Acute Chest Syndrome: Outcome
Complete recovery 91% Weaned of supplemental O2 3.1±1.9 days Hospital discharge 5.4±2.3 days
Chronic respiratory disease 3%
Death 6% Blood: 2004

Therapy of Acute Chest Syndrome
Oxygen avoid excess which reduces erythropoiesis
Careful rehydration maintain euvolemia judicious use of furosemide often helpful
Pain control narcotics ketorolac acetaminophen

Antibiotics
For the first 72 hours of admission, the patient should receive a third-generation cephalosporin (IV cefotaxime, 200mg/kg/day, divided q6–8h, max. 10g/day starting 24hr after the initial admission dose of ceftriaxone).

Beyond 72h, some may be switched to cefuroxime (75 -150mg/kg/day IV, divided q8h, max. 6g/day), as follows: Mild pneumonia & stable Cefotaxime for
72h, then cefuroxime Moderately severe pneumonia Continue
cefotaxime Severe pneumonia or unstable Cefotaxime +
vancomycin 60mg/kg/day, divided q6h; max. 4g/day

Children ≥ 5 years of age should be suspected of having mycoplasma pneumonia; add Clarithromycin 15mg/kg/day po divided q12h (max.
1g/day) or Erythromycin (40mg/kg/day, IV, divided q6h; max. 4g/day or po as estolate, divided q6-12h, max. 2g/day).
Use IV Clarithromycin in patients younger than 5 only if there is suspicion of mycoplasma.
Patients with a significant beta-lactam antibiotic allergy can be treated with clindamycin (40mg/kg/day, IV, divided q6-8h; max.
3.6g/day); or 30mg/kg/day po (q6-8h max. 1.8g/day).

For children older than 4 years, consult a respiratory therapist for incentive spirometry: 10 breaths q1–2h when awake, or 5 breaths every 15 minutes

Therapy of Acute Chest Syndrome
Improve oxygen delivery reduce % hemoglobin S
packed red cell transfusion – early on! exchange transfusion if still worsening (rarely needed if
transfused early) bronchodilators
albuterol regardless of presence or absence of wheezing non-invasive ventilation endotracheal intubation
adequate PEEP incentive spirometry

Therapy of Acute Chest Syndrome
Dexamethasone may shorten course However, use of steroids associated with:
1/3 of patients are readmitted Increased risk of avascular necrosis Pancreatitis

Therapy of Acute Chest Syndrome
Unproven therapies, but “seem to work” Dornase alfa- inhaled Nitric oxide ECMO

Newer therapies
Dexamethasone 0.3mg/kg IV q12h x 4 doses – Inhibition of inflammation, inhibit cytokine induction of adhesive
molecules Nitric oxide (NO) – Decrease pulmonary vascular resistance, improve pulmonary
blood flow Polaxamer 188 – Reduce blood viscosity, inhibit RBC adhesion to endothelium

Purified Poloxamer 188 for Treatment of Acute Vaso-occlusive Crisis of SCD
Randomized Controlled Trial
Purified poloxamer 188 may increase tissue oxygenation and thereby reduce inflammation, pain, and the overall duration of such painful episodes in patients with SCD
Conclusions A decrease in the duration of painful episodes and an increase in the proportion of patients who achieved resolution of the symptoms were observed when the purified poloxamer 188–treated
patients were compared with the patients receiving placebo.
JAMA. 2001;286:2099-2106

Options for Respiratory Failure 1. Exchange transfusion 2. Respiratory support
Conventional mechanical ventilation High-frequency oscillatory ventilation
For ventilated patients repeated daily bronchoscopy with lavage and aggressive suctioning of bronchial casts
Nitric Oxide (NO) via mask or endotrachial tube Extra Corporeal Membrane Oxygenation (ECMO) has been
reported

Summary ( ACS) Oxygen to correct hypoxia • Respiratory therapy including use of incentive
spirometry • Antibiotic coverage (including community acquired
organisms) • Maintain euvolemia • Pain management – avoid chest splinting and over
sedation • Bronchodilator therapy trial • PRBC Tx if respiratory compromise

Pulmonary Hypertension in Sickle Cell Disease
Many Factors Contribute to Development of PAH in SC Disease
¨ Repeated Episodes of Regional Pulmonary Hypoxia¨ Infection¨ Bronchoreactive lung disease¨ Chronic thromboembolism + fat embolism¨ Pulmonary fibrosis¨ Intravascular hemolysis with release of Hgb and
arginine

Regional Pulmonary Hypoxia
Sickling, Vascular adhesion, production of vasoactive substances
Reoxygenation followed by reperfusion injury
Progressive tissue damage with altered pulmonary vascular tone, vascular
proliferation in the muscle wall and hypercoagulable state causing pulmonary thrombosis and progressive loss of the vascular bed
Obliterative Pulmonary Vasculopathy with pulmonary hypertension

Role of NO (Nitric oxide)
Produced by endothelial cells (blood vessels)
Has vasodilative and cytoprotective effects that counter the processes induced by hypoxia
However, in sickle cell disease, levels of both arginine (the substrate for NO) and NO are low, diminishing the benefits of NO
Why is NO low in Sickle Cell Disease? Intravascular hemolysis

Depletion of NO in sickle cell anemia
Sildenifil:Increase effect of NO on cellular function

Plastic Bronchitis In Acute Chest Syndrome
Plastic bronchitis is a rare disorder characterised by the formation of branching mucoid bronchial casts
Recently a high prevalence (72%) of plastic bronchitis, a condition associated with widespread mucous plugging of the tracheobronchial tree, has been reported in patients with ACS following flexible bronchoscopy

It is usually associated with underlying pulmonary diseases like bronchial asthma, allergic bronchopulmonary aspergillosis, cystic fibrosis, bronchiectasis and at times other system diseases like congenital heart defects and sickle cell disease
Plastic bronchitis presenting as acute respiratory distress with wheezing, breathlessness, and cough, mimicking foreign body aspiration had been reported

Treatment of plastic bronchitis in acute chest syndrome of sickle cell disease with intratracheal rhDNase S S Manna, J Shaw, S M Tibby, A Durward Arch
Dis Child 2003;88:626–627

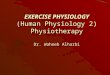
Plastic Bronchitis and the Role of Bronchoscopy in the Acute Chest Syndrome of Sickle Cell Disease Chuanpit Moser, Eliezer Nussbaum and Dan M. Cooper
Chest 2001;120;608-613

Chest radiographs of an 11-year-old boy with SCD obtained during an episode of ACS. Top: Before bronchoscopy, left lower lobe consolidation was evidenced by loss of cardiac and diaphragmatic silhouettes (small arrows). Bottom: After bronchoscopy, marked improvement was shown by reappearance of the aortic and left diaphragmatic borders (large arrows).

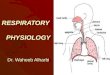
Chronic Pulmonary Disorders in Sickle Cell
Disease: Findings at Thin-Section CT’
The main finding of our study is that significant pulmonary interstitial disease is present on thin-section CT scans of the lower lungs in 41% of these selected patients with SC disease.
Pulmonary interstitial disease was manifested by a patchy and predominantly basal distribution of interlobular septal thickening, panenchymalbands, pleural tags, dilated secondary pulmonary lobules, traction bronchiectasis, and architectural distortion.
Radiology 890 Volume 193 Number 3 2004

Future directions
Sildenafil reduces pulmonary hypertension improves exercise endurance
Gardos channel blockers (not yet available) improve intraRBC dehydration improve markers of hemolysis
Arginine + hydroxyurea improves available nitric oxide, and may help vasculopathy

Preoperative Management
Preoperative transfusion improves morbidity
Highest risk of acute chest syndrome in first 48 hours after surgery
Outpatient surgery may be ill-advised Better outcomes with laparoscopy

Incentive spirometry is indicated for older children with chest or back pain: 10 breaths q1–2h while awake, or 5 breaths every 15 minutes .
The hospital’s Child Life representative may also assist younger children with deep-breathing and blowing bubbles

Pulmonary Rehabilitation
The goals of pulmonary rehabilitation are to reduce symptoms, decrease the degree of disability, increase the patient's participation in physical and social activities and improve the patient's quality of life.
In addition to exercise training, pulmonary rehabilitation encompasses patient education, psychosocial and behavioral intervention and outcome assessment.
American Thoracic Society Updates Statement 2007

Benefits of Pulmonary Rehabilitation
According to the report, studies have shown that pulmonary rehabilitation increases the level of exercise a patient can perform and decreases the degree of dyspnea for a given level of exercise.
According to the report, controlled trials have also shown that pulmonary rehabilitation is associated with a trend toward a decrease in the use of health care resources, including a reduction in the number and duration of hospitalizations.

Essential Components of Pulmonary Rehabilitation
1.Exercise training. The report indicates that studies have shown a high level of exercise training
(i.e., 60 percent of the maximal work rate, above the anaerobic threshold) produces greater improvement in maximal and submaximal exercise responses in patients with chronic obstructive pulmonary disease than does a low level of exercise training.
In patients who cannot train at 60 percent of their maximal work load for a prolonged period, interval training in the form of two to three minutes of high-intensity (60 to 80 percent of maximal exercise capacity) exercise is recommended.

Endurance training of the upper extremities is recommended in addition to endurance training of the lower extremities.
Most pulmonary rehabilitation programs use, alone or in combination, a stationary cycle or walking for building endurance in the legs.

2.Patient education. According to the ATS statement, patient education is an integral
component of a pulmonary rehabilitation program. Important subject areas include breathing retraining (such as pursed-lip breathing
and diaphragmatic breathing), techniques for energy conservation and the proper use of medications.
3.Psychosocial and behavioral intervention.
Problems such as anxiety, depression and difficulties coping with chronic pulmonary disease can be addressed during pulmonary rehabilitation.