Upload
deliapatrisa
View
214
Download
0
Embed Size (px)
Citation preview
7/26/2019 Sanitation Problem Health Sector
1/44
The sanitation problem:What can and should the health sector do?
Report
7/26/2019 Sanitation Problem Health Sector
2/44
Report
Half of the people living in developingcountries do not have access to even abasic toilet.1This presents a major riskto public health. Diseases attributableto poor sanitation currently kill morechildren globally than AIDS, malaria andmeasles put together, and diarrhoeais the single biggest killer of children
in Africa.2
Safe sanitation is widelyacknowledged to be an essentialfoundation for better health, welfareand economic productivity, but progress
in reducing the burden of sanitation-related diseases borne by poor peoplein developing countries remains slowand is holding back progress on allother development outcomes.
The wider problem of political andfinancial neglect of sanitation issues
has already been well documented3
and the 2008 International Year ofSanitation signalled a concertedeffort to try and address the sanitation
Summary
Summary recommendations:1. Global health institutions should acknowledge and address the impact
of sanitation on the global disease burden, the contribution of improvedsanitation to reducing that disease burden and the potential benefits forpublic health outcomes.
2. International donors should prioritise support for programmes in countrieswith low sanitation coverage and high burden of sanitation-related diseaseand invest in research and evaluation to understand the relative healthimpacts and additive effects of different types of sanitation intervention.
3. Developing country governments should ensure that sanitation isaddressed within all relevant health policies, regulations, guidelinesand procedures and establish targets and indicators for monitoring
improvements in sanitation related diseases.4. Developing country governments should strengthen public health legal
and regulatory frameworks to improve inter-sectoral coordination betweenministries and agencies responsible for sanitation at different levels andenhance accountability for results.
5. National and sub-national health programme priorities should takeaccount of sanitation-related disease burden and ensure that sanitationand hygiene are fully integrated within disease specific and nationalhealth programmes.
7/26/2019 Sanitation Problem Health Sector
3/44
Report
problem. But WaterAids experienceon the ground in Africa and Asia hasshown that the enduring challenge is
not just how to provide infrastructure,but also how to promote uptakeand use of facilities. Infrastructureis necessary but not sufficient forbetter health. There is a critical need todevelop better integrated approachesin order to maximise the health gainsassociated with sanitation interventionsin support of the ongoing drive toacheive Sanitation and Water for All.4
The health sector has an importantrole to play in promoting sanitation.Creating demand and changingbehaviours are both areas wherethe health sector has a strong trackrecord and recognised comparativeadvantage. However, there is a lack ofconsensus regarding institutional rolesand responsibilities for sanitation in
developing countries, and the degree ofhealth sector involvement in promotingsafe sanitation varies significantly. Thisreport draws upon recent WaterAid-funded research into the differentroles played by the health sectorin developing countries and makesrecommendations for acceleratingprogress on sanitation and securingrelated health outcomes.
The report reviews recent trends inhealth sector policy and programmesin developing countries, confirms theinadequate nature of existing institutionalresponses to the sanitation problemin these countries, and highlights theabsence of strong political leadershipand lack of clearly-defined institutionalroles and responsibilities. It furthernotes that health sector planning andfunding allocations frequently do notreflect the burden of disease attributableto sanitation in developing countriesand that contemporary health systems
are primarily focused on treatmentand patient-based interventions whilepreventive and public health aspects tend
to receive less attention.5
In developingcountries the majority of investment insanitation is currently channelled throughinfrastructure ministries where it is mainlyfocused on providing new facilities.Meanwhile, budget allocations tohealth ministries for sanitation tend tobe less clearly defined and allocationof health system resources for relatedactivities is often diffuse, making it
difficult to monitor results.
There is relatively little research onappropriate health sector roles andresponsibilities in promoting sanitationbut after reviewing existing theory andpractice the study focuses on four keyfunctional deficits that characteriseexisting institutional responses tosanitation and health:
1. norms and regulations2. inter-sectoral policy and coordination3. delivery of scaleable
sanitation programmes4. collection and use of data
This report explores the role of thehealth sector in addressing each of thefunctional deficits identified, drawing
on examples from the four countrycase studies.
The study concludes that improvedcollaboration between WASH and healthsectors is key to improving sanitation-related health outcomes. It shows thathealth systems have a critical role toplay in promoting sanitation but thatexisting health sector involvement isfrequently sub-optimal. It makes a seriesof recommendations for health sectorstakeholders interested in acceleratingprogress on sanitation and securing relatedhealth gains in developing countries.
7/26/2019 Sanitation Problem Health Sector
4/44
Report
A WaterAid report, May 2011. Written by Yael Velleman and Tom Slaymaker.
Acknowledgements:This policy report draws upon the findings ofWaterAid-funded research conducted in collaboration with the Water Institute(WI) at the Gillings School of Public Health, University of North Carolina,during 2010. The views expressed here are those of WaterAid and do notnecessarily reflect those of the Water Institute.
With particular thanks to WaterAid country programme staff in Malawi,Nepal and Uganda for their support and contributions to this report.
This paper should be cited as WaterAid (2011) The sanitation problem:What can and should the health sector do?
A soft copy of this and all other WaterAid papers can be found atwww.wateraid.org/publications.
Front cover image of children in Malawi:WaterAid/Layton Thompson
7/26/2019 Sanitation Problem Health Sector
5/44
Report
1
1. Introduction 2
2. The critical role of sanitation in health 4
3. The inadequacy of existing institutional responses 9
4. The role of the health sector in addressing existing deficits 12
4.1. Core functional deficits in securing progress on sanitation
and related health gains 12
4.1.a Functional deficit 1: Norms and regulations 13
4.1.b Functional deficit 2: Inter-sectoral policy and coordination 15
4.1.c Functional deficit 3: Delivery of scalable sanitation programmes 20
4.1.d Functional deficit 4: Collection and use of data 26
5. Facilitators and barriers for implementation of health sector functions 28
5.1.a Leadership 285.1.b Community participation 29
5.1.c Human resources 29
5.1.d Financing 30
6. Recommendations for health sector stakeholders 31
6.1. International health policy and donor policy 31
6.2. National development policy and resource allocation 32
6.3. National health policy and sanitation programme design 32
6.4. Other stakeholders 34
Table of contents
7/26/2019 Sanitation Problem Health Sector
6/442
Report
WaterAids vision is of a world where everyone has access to safe waterand sanitation. This vision can only be achieved by working in collaborationwith others. This report is part of an ongoing programme of work whichseeks to reach out beyond the water, sanitation and hygiene (WASH)
sector to engage with actors and agencies from other sectors, particularlyhealth and education, as part of a concerted joint effort to address the lackof access to WASH and the profound impact it has on health, welfare andeconomic growth in the worlds poorest countries and communities.
1. Introduction
Box 1: Health sector or health system?The terms health sector and health system are often used interchangeablyand are rarely defined. For the purposes of this paper the term health sector
is used to refer to the various different actors and agencies that play a rolein improving health (whether political, financial, technical or administrative),whereas the term health system is used to refer to the system for delivery ofhealthcare services (mostly understood as curative or palliative services).According to the World Health Organization (WHO):
A well functioning health system responds in a balanced way to apopulations needs and expectations by: Improving the health status of individuals, families and communities. Defending the population against what threatens its health. Protecting people against the financial consequences of ill-health. Providing equitable access to people-centred care. Making it possible for people to participate in decisions affecting their
health and health system.6
7/26/2019 Sanitation Problem Health Sector
7/44
Report
3
The report argues that the scale ofthe financial and human costs of theneglect of sanitation cannot be ignored;
and that joint, cross-sector efforts thatmake better use of existing resourcesare critical to building on the gainsachieved so far in improving globalhealth. Progress on global health, inparticular on child health, will requirehealth and sanitation professionals towork together to tackle poor sanitation.This report attempts to provide somepractical recommendations on how tofacilitate this joint effort.
The report draws on research conductedduring 2010 in collaboration with theWater Institute at the Gillings Schoolof Global Public Health, Universityof North Carolina, USA. The researchteam investigated the characteristics ofhealth sector involvement in sanitationin developing countries, includinggovernance structures, health sector
roles and responsibilities, and currentinitiatives to link sanitation and health.Four developing countries with differinginstitutional arrangements for sanitationand varying degrees of sanitation
coverage provided the context for moredetailed case studies: Malawi, Nepal,Sri Lanka and Uganda.7Extensive in-
country support was provided by localWaterAid staff and partners.
A triangulation approach wasused to gain a fuller picture of theinteraction of the health sector withsanitation policies, programmes, andimplementation. Data were collectedusing a range of methods including:a review of academic literature andcountry policies and programmes;expert consultation via in-person fieldinterviews with representatives fromthe health and WASH sectors (includingstaff from national governmentagencies, non-governmentalorganisations and external supportagencies); and development of aninteractive online survey using a wikiapproach8to elicit responses fromstakeholders in a larger number of
countries. The full report prepared bythe Water Institute, on which thisreport draws, is available separatelyas a background paper.
7/26/2019 Sanitation Problem Health Sector
8/444
Report
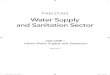
The F-diagram (figure 1) summarises theestablished means by which sanitationand associated hygiene practicesprevent infection.
1.1 billion people practise indiscriminateor open defecation.14This situationrepresents a significant and constantbarrier to human and economicdevelopment, through direct impact onhealth, as well as broader impacts onwellbeing and poverty. Although morethan 800 million people globally lack
access to safe drinking water, this paperwill focus specifically on sanitation;this focus is driven by the neglect ofthe sanitation issue, as well as theparticular role of the health sector insanitation promotion.
The impact of inadequate globalsanitation coverage on health isparticularly significant: the World
Health Organization (WHO) estimatesthat 7% of the worlds deaths and
More than one third of the worlds population does not have accessto improved9sanitation a sanitation facility that ensures hygienicseparation of human excreta from immediate human contact,10therebypreventing infection caused by the ingestion or contact with human
faeces (the faecal-oral route of transmission). At current rates,the sanitation MDG target will not be met globally until 2049; insub-Saharan Africa, it will not be met until the 23rd century.11
2. The critical role of sanitation in health
What is sanitation?Sanitation is the collection, transport, treatment and disposal or reuseof human excreta, domestic wastewater and solid waste, and associatedhygiene promotion.12
Fluids
Fields
Flies
Fingers
HumanFaeces
FoodsNew
Human Host
The effective separation of faeces from humancontact through improved disposal of excreta
Good hygienic practices such as hand-washingwith soap after going to the toilet
Figure 1: The F-diagram sanitation as a primarybarrier between excreta andhuman contact13
7/26/2019 Sanitation Problem Health Sector
9/44
Report
5
8% of the global disease burdenare caused by diseases related tounsafe sanitation.15Unsafe sanitation
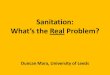
is a major risk factor for diarrhoealdisease,16the biggest cause of deathin children under the age of five insub-Saharan Africa17and the secondleading contributor to the globaldisease burden (see figure 2). Further,poor hygiene practices are a major riskfactor for respiratory infections, theleading contributor to the global burdenof disease.18Lack of access to WASH
is strongly associated with furtherdiseases and infections, includingintestinal nematode infections,lymphatic filariasis, trachoma andschistosomiasis, among others.19Asshown in figure 2, diarrhoea causesmore deaths in children under fiveyears old than HIV/AIDS, malaria,and measles combined.20
The impacts of WASH on the worldsdisease burden were critically reviewedby Ustin et al in 2008.22The reviewnoted that poor WASH causes anestimated 88% of cases of diarrhoeaworldwide, and although annualchild mortality has decreased since
the report was released in 2008,Ustin and colleagues showed that28% of child deaths were due to
unsafe WASH. Further, an estimated50% of childhood malnutrition wasassociated with repeated diarrhoeaor intestinal nematode-relateddiseases. Children in developingcountries suffer disproportionately,with models indicating that over 20%of global mortality and disease burdenof children 0-14 years old are due tounsafe WASH.23
In a recent review of survey datafrom 172 countries, results showeda robust association between accessto sanitation technologies andreduced child mortality and morbidity.Sanitation access lowered the oddsof children suffering from diarrhoeaby 7-17%, and reduced mortalityfor children under five by 5-20%.
Figure 3 shows cross-tabulation ofdiarrhoea and child mortality rateswith sanitation technology level. Itdemonstrates that child morbidityand mortality are substantially lowerfor children with access to advancedsanitation technologies.24
Pneumonia
Preterm BirthComplications, 12%
Birth Asphyxia, 9%
Sepsis, 6%
Other, 5%
Congenital Abnormalities, 3%Tetanus, 1%
Diarrhoea
Measles, 1%Injury, 3%
Malaria, 8%
AIDS, 2%Pertussis, 2%
Meningitis, 2%
Other Infections, 9%
Other Non-Communicable Diseases, 4%*
Neonataldeaths, 41%
14%
14% 4%
Figure 2: Global causes of child deaths21
1%
7/26/2019 Sanitation Problem Health Sector
10/446
Report
This situation is reflected in the burdenof disease in the case study countries:table 1 provides an overview of theestimated prevalence of sanitation-related infections in the case studycountries. In 2004 (the latest year forwhich comparative data are available),
diarrhoeal disease caused an estimated69% of the deaths and 68% of thedisease burden in three of the fourcountries studied: Malawi, Nepal and
Uganda. In contrast, diarrhoea causedless than 1% of the deaths and diseaseburden in Sri Lanka. Other diseasesrelated to unsafe sanitation suchas intestinal nematode infections,malnutrition, trachoma, schistosomiasisand lymphatic filariasis, were estimated
to have caused several thousanddeaths and significant disease burdeneach year in the case study countries.Malnutrition was estimated to have
0.20
0.18
0.160.14
0.12
0.10
0.08
0.06
0.04
0.02
0.00
Open
Latrine
Flush
DIARRHOEA CHILD MORTALITY
Open
Latrine
Flush
Figure 3: Correlation of sanitation access with diarrhoea and child mortality25
Table 1: Summary statistics on deaths and disability from WASH-related diseases in 200426
Malawi Nepal Sri Lanka Uganda World
Population 12,895,000 26,554,000 19,040,000 28,028,000 6,436,826,000
Deaths DALYsa Deaths DALYsb Deaths DALYsb Deaths DALYs Deaths DALYsb
Diarrhoeal diseases (% oftotal deaths or DALYs)
20,700(9%)
674,000(8%)
15,800(6%)
523,000(6%)
900(
7/26/2019 Sanitation Problem Health Sector
11/44
Report
7
caused up to 23% (Malawi) of theWASH-related disease burden. Thetotal estimated WASH-related disease
burden differs significantly betweenMalawi (12%), Nepal (11%) and Uganda(11%) on the one hand, and Sri Lanka(2%) on the other. Further, the totaldeath rate from WASH-related diseasesalso differs significantly betweenMalawi (11%), Nepal (7%), Uganda(8%), and Sri Lanka (
7/26/2019 Sanitation Problem Health Sector
12/448
Report
The tremendous impact of sanitationon health results in significanteconomic returns on investment in
sanitation, for individuals as well asnational economies. Evans et al34determine that such returns includedirect healthcare savings by both healthagencies and individuals, aswell as indirect benefits such as
productive days gained per year (forpersons 15-59 years of age); increasedschool attendance for children; timesavings (working days gained) resulting
from more convenient access toservices; and a high value of deathsaverted (based on future earnings). Thestudy further showed that achievingthe water and sanitation MillenniumDevelopment Goal (MDG)35could yieldsubstantial economic benefits, rangingfrom US$3-34 per US$1 invested,depending on the region.
There are also significant benefitsfor health systems and budgetaryresources; according to UNDP, at anygiven time half of the hospital beds indeveloping countries are occupied bypatients suffering from sanitation- andwater-related diseases,36representinga tremendous burden for alreadyoverstretched health systems. It alsoestimates that universal access
to even the most basic water andsanitation facilities would reduce thefinancial burden on health systems indeveloping countries by about US$1.6billion annuallyand US$610 millionin Sub-Saharan Africa, whichrepresents about 7% of the regionshealth budget.37
In 2008, the World Banks Water andSanitation Program (WSP) conductedan economic impact analysis of
sanitation in five south-east Asiancountries: Cambodia, Indonesia, theLao Peoples Democratic Republic,Vietnam, and the Philippines. Theresearch estimated that these countrieslose an estimated US$9 billion (2005dollars) a year 2% of their combinedGDP because of poor sanitation.38A similar study in India showedthat inadequate sanitation cost the
economy US$53.8 billion annually inlost productivity, healthcare provisionand other losses - equivalent to 6.4%of GDP in 2006.39
The data above provides compellingevidence on the benefits of sanitationinvestment and the scale of thefinancial and above all human costsof not investing cannot be ignored
by any sector. In a time of financialcrises and shrinking domestic andaid financial flows, joint efforts thatmake better use of existing resourcesare not only sensible but critical tobuilding on the gains achieved so farin improving global health. Clearly,if real improvement is to be madein population health in developingcountries, especially on child mortality
where performance has beenparticularly poor, then health andsanitation professionals need to workin concert to tackle poor sanitation asa major cause of ill health.
7/26/2019 Sanitation Problem Health Sector
13/44
Report
9
3. The inadequacy of existinginstitutional responses
While health professionals frequentlyacknowledge sanitation as a vitalprecondition for acceptable standardsof public health,40interviews conductedwith senior health professionals forthis and other studies41show that theyrarely consider sanitation to be withintheir own scope of responsibility;rather, it is someone elses business.42
This is reinforced by the fact thatsanitation is generally weaklyintegrated within increasingly curativeand palliative health systems, at theexpense of preventive approaches;in some cases, sanitation is not evenconsidered to be part of the healthsectors policy mandate. On the otherhand, interviews with frontline healthprofessionals show that although
promoting safe sanitation is rarely acore component of health programmesby design, the scale and severity of thesanitation problem on the ground issuch that they are often compelled tointervene in an ad hoc manner usingavailable and limited resources.
Despite the fundamental importanceof sanitation to human health and other
development outcomes, sanitationis often a low priority in nationaldevelopment agendas, obscured bythe more politically attractive focus
on safe drinking water. For example,sanitation was initially omitted from theinitial list of MDG Targets, only addedin 2002. Recently, the 63rdWorld HealthAssemblys report on the monitoring ofthe MDGs, and the resulting resolution,failed to acknowledge that the sanitationaspect of MDG Target 7c will not bemet thereby failing to acknowledge
its importance for the achievement ofthe health MDGs.43This lack of globalprioritisation is mirrored in nationalpolicies and priorities, with the bulkof WASH financing allocated to waterinfrastructure, and environmental healthprogrammes suffering from lack offunding and prioritisation the 2009World Bank Africa Infrastructure CountryDiagnostic Report found average annualpublic spending on sanitation to be nomore than 0.22% of GDP, of which 0.2%was recurrent expenditure and only0.02% represented new investment.As noted earlier, progress on access tosanitation remains painfully slow. Giventhe compelling evidence provided aboveon the links between sanitation andhealth, it is unsurprising that progresson critical health aspects, in particularchild health, has been equally slow.44
The effect of slow progress oninfrastructure coverage is exacerbatedby the design and delivery of sanitation
The need for joining health and engineering expertise is self-evident,and has led to the introduction of public health acts and urbansewerage systems in rich countries. This potential remains largelyunrealised in developing countries.
7/26/2019 Sanitation Problem Health Sector
14/4410
Report
programmes; in addition to low levelsof funding, sanitation programmesare also characterised by short-term
project cycles that lead to a focus onconstruction of new infrastructurewithout due consideration ofinfrastructure sustainability and use.45Inadequate attention to creatingdemand for sanitation and changingbehaviour means that potentialhealth gains are not realised. Decisionmaking on sanitation policy tends tobe conducted at a central governmentlevel, while WASH departmentsat lower levels of government arefrequently understaffed and under-resourced without the necessarycommunity-level reach on a regular andconsistent basis outside the projectcycle. Such community-level reachis essential for enabling demand forsanitation, adoption of sound hygienepractices, and generating capacities forconstructing and maintaining sanitation
facilities. This community-level reachand ability to drive up demand forservices and related behaviour changeis one crucial area where the healthsector can help deliver progress onsanitation and associated healthbenefits. This difference in reachbetween the health and WASH sectorsis depicted in figure 5.
Curative patient treatment is just oneaspect of health systems, although itis the most publicly visible one, andis therefore prioritised both politicallyand financially. But another key role isthe promotion of changes in behaviourand lifestyle to improve health andprevent disease. Such behaviourchange can include the generation ofdemand or take-up for specific services(eg. vaccination) and products (eg. bednets). The fact that the health sectorhas engaged in such activities forcenturies, and has developed tried and
tested approaches for doing so, placesit in a unique position of expertise.With health professionals (doctors,nurses, health promoters) located evenat remote rural locations, the sectoralso has incomparable reach intoand influence over the population itserves. Health professionals, especiallydoctors, wield considerable authority,and command respect in many societiesworldwide. As one interviewee inNepal put it, people listen to doctorsmore than they listen to engineers.
The leadership of health professionalshas been demonstrated globally inlarge-scale efforts and programmesfor prevention and control of HIV/AIDSand non-communicable diseases, bothassociated with lifestyle choices andrequiring strategies that emphasisebehaviour change. The expertise forchanging behaviour and promotinguptake of services and products, as
well as service scope and reach arelacking in the institutional structureof the WASH sector, which remainsproject-driven and heavily focused
Central Government
District Authorities
Community
Household
WASHHealth
Health SurveillanceAssistants/
Health Promoters
CommunityHealth Workers
ProjectCycle
Figure 5: Comparative reach of healthand WASH sectors
Local Government
7/26/2019 Sanitation Problem Health Sector
15/44
Report
11
on engineering and infrastructureaspects46. The behavioural (software)aspects of sanitation must be
addressed systematically if increasesin sanitation coverage are to take placeand result in better health outcomes.Box 3 provides a discussion onsanitation and hygiene promotion.
All health sector stakeholdersinterviewed agreed that the existinginstitutional responses to sanitation
are inadequate given the burden ofdisease attributable to poor sanitationexperienced in developing countries.But what precisely can and shouldthe health sector do about thesanitation problem?
Box 3: Sanitation and hygiene education or promotion?The terms education and promotion are often used interchangeably, butare in fact two very different approaches. According to Curtis,47the need fora promotion approach is rooted in the fact that getting people to changethe habits of a lifetime is difficult, takes time and requires resources andskill. With regards the promotion of hand-washing with soap, while pastapproaches utilised hygiene education (teaching why hygiene practices suchas hand-washing are necessary, and how to practice them) to affect behaviourchange, it is now understood that knowledge about germs is insufficient tochange behaviour, due to time or financial costs as well as social attitudes tohand-washing. Unlike hygiene education, hygiene promotion builds on theunderstanding of community attitudes, knowledge, practices and desires.
Its reliance on participation and appropriateness provides better chancesfor sustained behaviour change, as well as reduced reliance on large-scaleeducation campaigns. Similar lessons have been learnt regarding sanitationpromotion; Jenkins and Caircross have documented the reasons leading toconstruction and use of latrines at the household level, noting that householdadoption of sanitation practices is often associated with comfort, prestigeand safety as much as with health considerations.48Successful sanitationpromotion approaches must consider these motivations in order to ensuresustainable impact.
7/26/2019 Sanitation Problem Health Sector
16/4412
Report
4.1 Core functional deficits insecuring progress on sanitationand related health gains
Little research has been undertaken onthe involvement of the health sectorin decreasing the disease burdencaused by poor sanitation.49Rehfuess,Bruce, and Bartram50assert six specifichealth sector functions in relation toenvironmental health issues such aspoor sanitation.
Drawing on this and other literature,the WaterAid research presented in this
paper focused on four broad functionaldeficits which typically constrain efforts
to accelerate progress on sanitationand secure related health gains:1. Norms and regulations.2. Inter-sectoral policy
and coordination.3. Delivery of scaleable sanitation
programmes.4. Collection and use of data.
These four functional deficits are usedhere as a framework for examiningexisting institutional arrangements forsanitation in developing countries andidentifying potential roles for the healthsector, both within its own purview andin partnership with other sectors,52intackling these deficits.
4. Functional deficits and the role ofthe health sector in addressing them
Table 2: Health sector functions and roles51
Health sector roles
Function 1.Norms and regulations
Develop health-protecting standards and regulations appropriate to the countryssocial, economic and environmental circumstances.
Monitor implementation and contribution to population health.
Function 2:Inter-sectoral policyand coordination
Build and maintain expertise to track and influence major policies that impact health. Employ formal mechanisms for health impact assessments. Establish effective multi-disciplinary collaboration.
Function 3:Health facilities
Set standards for healthcare facilities. Budget for structural improvements and capacity-building to encourage staff
behavioural changes. Enforce compliance through an independent oversight function.
Function 4:Disease-specific andintegrated programmes
Integrate environmental determinants (eg. safe sanitation) into health professionaltraining curricula.
Incorporate environmental health actions into health programmes. Work with partners to raise awareness.
Function 5:Outbreaks
Maintain expertise to advise on and conduct outbreak investigations. Test, implement and revise procedures in cooperation with other actors. Update regulations and policies accordingly.
Function 6:Impacts, threats,
and opportunities
Seek evidence for causal associations between environmental factors(eg. absence of sanitation) and health.
Assess potential values and harms of technology innovation and policy development.
7/26/2019 Sanitation Problem Health Sector
17/44
Report
13
4.1.a Functional deficit 1:
Norms and regulations
Policy and supporting legislation is
essential to provide a clear visionand to establish basic principlesand objectives to guide sanitaryimprovements. In several of thecountries reviewed there exists somesort of historic public health legislationthat considers health risks associatedwith poor sanitation. For example,Sri Lanka developed the first publichealth-orientated legislation in the
19th century when the Public Healthand Ordinance and Small TownsSanitary Ordinance of 1892 provideda legal basis to enact local sanitationrequirements. Uganda and Malawicreated public health legislation aroundthe time they gained independencefrom Britain. Ugandas Public Health act,enacted in 1964 and updated in 2002,requires sanitation in all households.
Malawi enacted a Public Health Act in1948 which regulates sewerage andinfectious disease prevention but itsupdated National Health Act and Policy2010 awaits approval. Nepal is the onlycountry of the four case studies thatdoes not have a public health act. Veryfew countries have an explicit nationalsanitation policy, although some havedrafted policies which have not been
officially agreed and launched, andare therefore yet to be translated intoaction. However where such policiesdo exist, they often lack traction atprogramme level, and do not usehealth outcomes as success indicators.Health policies on the other hand tendto focus on service delivery aspects,with less emphasis, and consequentlyless human and financial resources
dedicated to preventive measures,including sanitation.
Health sector roles in promotingsanitation include supporting the
development of norms and regulationsthat will improve health and encouragethe definition and adoption of safesanitation practices, and establishingmechanisms to enable periodicreview and updating in response toemerging challenges. While sanitationtechnology is still being developed,the input of the health sector is crucialto ensure that adopted technology
meets the required health standards.In Sri Lanka, for example, the healthsector was actively involved in thedevelopment of guidelines for latrineconstruction and safe disposal ofexcreta, which has contributed tosignificant improvements in the generalstandard of sanitation facilities inrecent years. Development of normsand regulations is also closely linked
to education and awareness-raising,which are critical factors in promotingbehaviour change and in generatingdemand for sanitation services andinfrastructure. Public informationcampaigns run by the health ministryin Sri Lanka are considered to haveplayed a key role in stimulating demandamong communities for improvedsanitation facilities.
An obvious opportunity for thehealth sector to promote behaviourchange (and ultimately better policyand programming) starts with safesanitation within healthcare facilities.Clean and well-maintained facilitiesprovide a model to users of healthypractices that can be implemented inhomes, schools, and other settings as
well as reducing the risk of infectionwithin healthcare facilities. However
7/26/2019 Sanitation Problem Health Sector
18/4414
Report
facilities observed in the case studycountries suffer from extremelypoor maintenance and, too often,
a complete absence of sanitationfacilities. The availability of functioningsanitation in Nepals health facilities isseverely inadequate. Hospital wastemanagement and general attention tothe physical functioning of governmenthospitals and clinics is slowly improvingas part of the attention given to theseaspects in the health sector-wideapproach (SWAp) and the technical
assistance provided by WHO (with theassistance of the Global Alliance forVaccines and Immunisations (GAVI)).In Uganda, information obtained fromstudies, interviews and visits to healthfacilities indicates poor sanitationconditions in many healthcare facilities.In Sri Lanka, the government has notissued specific guidelines for hospitalplanning, including sewage system
design, and there are concerns thatestablished government and Ministryof Health (MoH) guidelines have notbeen closely followed by contractorsinvolved in recently-constructed newhospital buildings.
With appropriate regulations officiallyin place, health decision makerscan ensure that health facilities are
adequately equipped with functioningsanitation facilities. They can alsorequire safe sanitation practices by staffand ensure compliance through regularinstruction and monitoring. Health
sector professionals are well-placed tolead by example and to demonstrateappropriate practices for the thousands
of patients they treat annually, as wellas opportunistic promotion of hygienemessages through posters, talkswith patients in waiting rooms, andindividual conversations with patients(either during routine visits such as forchild vaccination or for acute visits dueto WASH-related infections).
Monitoring and enforcement remains a
key challenge in the countries studied.Sri Lanka has been more successfulthan most in managing to retainan active network of public healthinspectors that traditionally combinedpromotion and inspection activitiesto generate better sanitation-relatedbehaviour in the population. There areexamples, such as in Uganda, of theenforcement of sanitation practices
through other means, including thepenalisation for non-compliancewith sanitation standards throughfines or prison sentences, but thereare concerns that such approachesmay be less effective in generatingbehaviour change that translatesinto health gains. While regulationsare crucial for resolving conflicts, forexample between tenants and their
non-complying landlords, the actualhygienic and effective use of sanitationfacilities is better addressed throughcommunity-level outreach a specialityof the health sector.
7/26/2019 Sanitation Problem Health Sector
19/44
Report
15
4.1.b Functional deficit 2: Inter-sectoral
policy and coordination
Securing progress on sanitation andassociated health gains requires
concerted action across a diverse rangeof actors. A number of sectors, includinghealth, education, environment,industry, transport and infrastructure,address or impact on various aspectsof sanitation on a regular basis. Cross-sectoral action provides a financiallyprudent and more sustainable meansto improve population health andincrease investment by other sectors.
This requires leadership, includingcommitment from top officials andengagement at all levels. Such
leadership relies on health ministriesmoving beyond the mere managementof health systems to assuming astewardship role for promoting and
safeguarding acceptable standardsof public health, and asserting theauthority associated with this roleover the activities of other sectors.
One way of breaking down theinstitutional silos that hamperinter-sectoral cooperation is theestablishment of joint financingarrangements. In the past few years,
there has been a shift in the wayin which external donor support isdelivered. While SWAps have, over
Findings: Clear policy, legislation and minimum standards are an important
foundation for securing potential health gains from WASH. Some countrieshave public health legislation in place but very few have explicit policiesand strategies for addressing sanitation.
Ministries of Health and health authorities often play a minimal role insanitation policy setting and programming, whether led by or includedwithin the Ministry of Healths environmental health division.
Where sanitation policies exist they are generally approached from anengineering (supply-side) perspective, which does not recognise thepublic health implications of sanitation (and consequently, does not usebehaviour change or health outcomes as indicators of a well-functioning
sanitation infrastructure). Many developing countries lack commonly agreed minimum standards
for sanitation (eg. in schools and clinics). Concepts and definitions ofwhat constitutes safe or improved sanitation are still evolving (eg. thesanitation ladder), and require significant inputs from public healthprofessionals (beyond technology).
When sanitation enforcement mechanisms are in place, such as housingregulations and bylaws, they are often constrained due to minimal fundingand inadequate human resources. Formal sanctions alone are unlikelyto result in health gains unless coupled with efforts to promote safe
sanitation and improved hygiene practices. No examples were found for the purpose of this study of regulations or
guidelines for patient safety and infection control measures, which relateto safe sanitation.
7/26/2019 Sanitation Problem Health Sector
20/4416
Report
the years, been accompanied byfinancing arrangements such asbasket funds (jointly managed by
SWAp partner institutions), there hasbeen a recent growth in earmarkingfunds through budget support. Suchfinancing arrangements can improveharmonisation between actors andalignment with government financialmanagement systems, as well asencourage adoption of commonlyagreed sector performance indicators.However, they can also reinforce sector
silos by increasing the competitionfor resources (for example, healthministries may be reluctant to sharebudget resources with institutionsoutside the sector, or to spend oninterventions deemed to be outsidethe sectors remit).
Certain efforts have been made in thecase study countries to break down
silos, such as involvement of water andsanitation officials in health planningand budgeting processes in Nepal,and similar efforts in Malawi butthese remain largely ad hoc and havenot been effectively institutionalised.In Uganda, a separate sanitationbudget line has been established inorder to address the financial neglectof sanitation as well as to enable
monitoring of sanitation spending;however, at the time of writing of thisreport, the budget line has not yetbeen furnished with funds, nor hasthere been an agreement between thethree responsible ministries (Ministryof Water and Environment Environment(MoWE), Ministry of Health (MoH)and Ministry of Education and Sports(MoES)) on how these funds will be
managed. While there has been anincrease in the number of programmes
requiring inputs across a number ofdifferent sectors (eg. nutrition, childand maternal health), no examples were
found of joint reporting by water andhealth ministries on sanitation-relatedhealth outcomes.
Examples of mechanisms for inter-sectoral policy and coordination onsanitation were identified in all thecountries studied at both nationaland district levels. These can takethe shape of a SWAp led by the water
or health ministry, as well as that ofworking groups set up to addressspecific issues such as sanitation.However, with the exception of Malawi,health sector participation in inter-sectoral mechanisms led by the waterand sanitation infrastructure sectortends to be sporadic or crisis-driven(for example, following a diseaseoutbreak). In addition, participation is
usually undertaken at the junior stafflevel and does not match the levelof seniority of water and sanitationinstitution attendees. At a district level,coordination structures may sufferfrom lack of financing, under-staffingand low capacity, lack of decision-making autonomy and poor links withnational level institutions and inter-sectoral mechanisms.
In Uganda, at the national level,the National Sanitation WorkingGroup (NSWG) has the mandateof operationalising the sanitationMemorandum of Understandingsigned by the MoH, MoWE and MoES,integrating sanitation and hygienepromotion in sector operations, andimproving cross-sectoral coordination.
The NWSG is chaired by the World BankWSP, and comprises of government
7/26/2019 Sanitation Problem Health Sector
21/44
Report
17
ministries (MoWE Directorate for WaterDevelopment, MoH EnvironmentalHealth Division, MoES), development
partners (UNICEF, GIZ (Gesellschaftfur Internationale Zusammenarbeit))and NGOs (WaterAid in Uganda, PlanInternational, UWASNET, AMREF,Netwas and Water for People). Atthe district level, coordination isundertaken through the DistrictWater and Sanitation CoordinationCommittees (DWSCCs), who bringtogether administrative and political
leaders, technical officers, and NGOand community-based organisaitonrepresentatives to oversee theimplementation of water supply andsanitation programmes and strengthencollaboration and coordination withother sectors and actors at the districtlevel. The DWSCCs have real potentialfor local-level collaboration but theireffectiveness may be hampered by the
substantial increase in the numberof districts in the country, which isyet to be matched by adequate localgovernment capacity. The ImprovedSanitation and Hygiene (ISH)promotion 10-year financing strategyfor Uganda, which defines the pillarsfor improved sanitation and hygiene(generate demand, supply sanitation,and develop an enabling framework
to support and facilitate acceleratedscaling up), has yet to receive officialgovernmental support and fundingremains fragmented, resulting in small-scale, uncoordinated implementation.
Within the health sector, the Division ofHealth Promotion and Education (HPE)at the MoH leads the implementation ofHPE programmes and works with other
agencies to review relevant standardsand regulations. At the district level, the
District Director of Household Servicescoordinates planning, managing, andmonitoring of information, education
and communication activities andworks with all agencies including thedistrict information office. At healthcentres, HPE activities are carriedout by available health professionalsand village health teams, basedon need and prevalent healthproblems. However, coordination andcollaboration between HPE and theDWSCCs and NWSG in responding to
sanitation-related health problemscurrently remains limited.
Nepal does not have a Public Health Actto allocate sanitation and environmentalhealth tasks to specific actors. This isconsidered an important obstacle toengaging the district-based health staffin integrating their activities with otherstakeholders in environmental health,
exacerbated by lack of clarity regardingthe responsibilities of the DistrictPublic Health Officers and the PublicHealth Officer. Health and sanitationstakeholders interviewed indicatedlack of interaction across sectors andprogrammes, and a narrow sectoralapproach applied by professionals inboth sectors, and within sectors, withvertical approaches (see box 4 overleaf)
leaving little scope for interactionbetween subprograms, let alonewith other sectors. One professionalinterviewed noted that without officialguidance to ensure collaboration, ittends to be an exception rather thanthe rule. The recent Nepal Health SectorSupport Programme (NHSSP-II) maypresent an opportunity to developa public health act and/or a WASH
strategy with firm and formalised linkswith health institutions.
7/26/2019 Sanitation Problem Health Sector
22/4418
Report
In Malawi, as a result of the developmentof the National Sanitation Policy (NSP)in 2008, the Ministry of Irrigationand Water Development (MoIWD)established a Sanitation and HygieneDepartment in 2009 to lead the nationalsanitation initiatives. At the local level,the District Assemblies are responsiblefor ensuring that the policy is reflected
in strategies for implementationthrough the Development Strategyand Improvement Programmes (DSIP).It is most likely that, while the WaterDepartment will take the lead inwater and possibly some subsidisedimplementation of sanitation activities,sanitation promotion and monitoringwill be led by the Health Department.Although the NSP was adopted by the
government in 2008, its official launchhas been delayed several times and is
not expected until 2011. The NSP willbe supported by development partnersunder a SWAp for sanitation, bringingtogether government institutions andother relevant stakeholders. The SWApis anticipated to improve coordinationand participation in the formulationand implementation of sector policies,planning, and investment. Oversight will
be provided by the National Sanitationand Hygiene Coordination Unit (NSHCU),chaired by the director of PreventiveHealth Services (PHS) of the MoH andwith the director of MoIWD acting as theexecutive secretary.
Successive governments in Sri Lankahave prioritised investment in healthand education which has led, inter
alia, to significant improvementsin public health. Sanitation has
Box 4: Water, sanitation and hygiene within the secondNepal Health Sector Support Programme (NHSSP II)
Efforts are ongoing to ensure that WASH issues are firmly embedded withinthe NHSSP II: The Ministry of Health and Population (MoHP) has assigned a focal point
to coordinate with the WASH sector In 2010, Global Handwashing Day was celebrated nationally, bringing
together the MoHP and the Ministries of Physical Planning and Works,of Education, of Local Development, WaterAid and UNICEF.
MoHP has formed a Water Quality Surveillance Thematic Group to workon capacity assessment and developing a Water Quality SurveillanceGuideline to Nepal.
An Environmental Health and Hygiene technical committee has beenformed under MHP/ National Health Education, Information andCommunication Center to work on WASH-related health issues and providetechnical inputs on broader environmental health issues including WASH.
The Primary Health Care Revitalization Division (a newly developed divisionat MoHP/Department of Health Services) has one environmental healthsection which is also responsible for WASH issues in urban areas.
WASH has been discussed at the Health Joint Sector Review in February2011. The subsequent aide memoire also included WASH aspects.
7/26/2019 Sanitation Problem Health Sector
23/44
Report
19
been incorporated into centralgovernment health policies sincethe 19th century, and institutional
roles and responsibilities have beenclearly articulated historically throughlegislation as far back as 1865.An integrated health system thatincorporates curative and preventivefunctions has been in place since 1925,including a Health Unit system withresponsibilities including: generalhealth surveys; collection and studyof vital statistics; health education;
investigation and control of infectiousdiseases; maternal and child health;school health work; rural and urbansanitation. Sri Lanka s current HealthMaster Plan 2007-201553 places a strong
emphasis on inter-sectoral action,noting that it is a major process indeveloping healthcare programmes
and that the contributions made byother sectors such as related other [sic]government ministries, private sector,Non Governmental Organizations,international and UN agencies andCommunity Based Organizations cannotbe under-estimated. As shown in table 3,the plan also lists relevant agenciesfor each programme that addressessanitation targets. The plan also notes
that the MoH is working to develop formalinter-sectoral coordination mechanisms,with the objective of bringing togetheractors across different levels in a jointeffort to improve health.
Table 3: Inter-sectoral policy and coordination
National-level sanitationcoordination body
National sanitationpolicy/plan Stakeholders Other notes
Nepal
Steering Committeefor NationalSanitation Action
National Hygiene andSanitation Master Plandraft 2010 (awaitingfinal approval)
Ministry of Physical Planning and Works
MoPPW, DWSS, MoHP, MoES, MoLD,donors and NGOs (40 members).
Health representationusually does not includeministerial leadership,except during crises
Malawi
National Sanitation andHygiene CoordinationUnit (NSHCU)
National SanitationPolicy (NSP) 2008(has not beenformally launchedby government)
NSP states that, with the Directorof Ministry of Irrigation and WaterDevelopment (MoIWD) acting as theexecutive secretary.
Director of Public HealthServices of the Ministryof Health will chair theNSHCU MoIWD added aSanitation and HygieneDepartment in 2009
Sri Lanka
National SanitationTask Force
National SanitationPolicy 2006
National SanitationAction Plan 2008
Government, donor agencies, andinternational and local NGOs.
Uganda
National SanitationWorking Group
No official sanitationpolicy exists; ISHstrategy existsbut has not beenoperationalised
Government (MoWE, MoH, MoES,Ministry of Finance, Planning andEconomic Development, Ministry of LocalGovernment, Ministry of Gender, Labourand Social Development), donor agencies,National Water and Sewerage Corporation(NWSC), and international and local NGOs.
Governmentparticipation in thegroup is technicallevel only
7/26/2019 Sanitation Problem Health Sector
24/4420
Report
4.1.c Functional deficit 3: Delivery of
scalable sanitation programmes
The strong track record of the health
sector in creating demand for serviceuse and in generating behaviour changehas been described above; this expertisegives health professionals a pivotal rolein ensuring that safe sanitation practicesare included within the menu ofdesired health behaviours. Several keyareas of opportunity include disease-specific and integrated programmes,community health clubs, and school
sanitation initiatives.
Disease-specific programmes in Nepalare reported to be strongly influencedby donor priorities without necessarilyconsidering national health priorities,leading to, among other things, anunhealthy competition between thevarious programmes, fragmentation andpoor coordination and resource sharing
(thus neglecting to maximise efficiencyas well as exacerbating barriers to inter-sectoral collaboration), and an increasedburden on health professionals and
administrators. Several respondentsin the field interviews suggested thatprogramme priorities should be driven
by existing disease burden (and considerchildren as a separate category) ratherthan by donor-led priorities. This,along with the absence of clear linesof responsibility for sanitation withinthe Ministry of Health and Population,has implications for the ability toeffectively incorporate sanitation intohealth programming. Malawi has severaldisease-specific programmes that could
potentially be linked with sanitation, butcurrently there exists little horizontalinteraction between these programmes.
Health professionals in all programmesplay an important role in educatingpatients and encouraging behaviourchange. Integration of sanitationconcepts and practices, such as theimportance of proper toilet installation
and maintenance, into existing disease-specific and primary healthcareprogrammes, would significantly increasecurrent outreach. Health promotion and
Findings: Lack of effective inter-sectoral collaboration is a major factor causing slow
progress on sanitation. Ministries of Health and health authorities often play a minimal role in
sanitation policy setting and programming, whether led by or includedwithin the Ministry of Healths environmental health division.
Improving access and changing behaviours requires coordination betweenmultiple agencies. Most countries have a coordinating body of some sortwith a mandate on sanitation but responsibilities, accountabilities andfinancing arrangements tend to be poorly defined.
SWAps have the potential to improve coordination of financing forsanitation but can also reinforce silos and present obstacles to
inter-sectoral collaboration District level coordination is crucial for effective programme implementation,
but district structures often lack the autonomy needed to respond flexibly tosanitation-related health problems and tend to suffer from under-resourcingin human and financial terms
7/26/2019 Sanitation Problem Health Sector
25/44
Report
21
Box 5: Disease-specific and integrated programmes.Much debate has taken place in the past few years on the advantages and
disadvantages of vertical versus integrated health programmes.Verticalapproachestarget a particular disease or issue and are considered by someas more viable due to their perceived immediate and quantifiable results.Horizontal approachesplace greater emphasis on long-term sustainabilitythrough a broader view of health.54In the late 1980s and early 1990s manycountries applied primary healthcare or integrated approaches (such asthe Integrated Management of Childhood Diseases approach, which used apackage of key child health interventions). However, due to lack of quantifiablesuccesses, among other things, leading international organisations andagencies began focusing on disease-specific initiatives, crowding out
integrated childhood management programmes (eg. in Nepal). To date, billionsof dollars have been spent on these global health initiatives, which areoften backed by strong political support and disease-specific internationalcampaigns. As initiatives develop and lessons learnt are fed back into thedesign of global health approaches, the picture has become more complex. Arecent literature review55states that there arefew instances where there isfull integration of a health intervention or where an intervention is completelynon-integrated. Instead, there exists a highly heterogeneous picture bothfor the nature and also for the extent of integration. Health systems combineboth non-integrated and integrated interventions, but the balance of these
interventions varies considerably.
communication must underlie all publichealth programmes, and provides a keyopportunity for outreach and scalableprogrammes. Safe sanitation can beincorporated into programme deliveryas a fundamental practice in most, if notall, programmeswhether vertical or
horizontal. For example, sanitation andhygiene promotion can be integratedinto HIV/AIDS programmes in order toreduce the risk of infection in patientswith compromised immune systemsand reduce the possible adverse impactof strategies for prevention of mother-to-child transmission.56
Examples of integration in
disease-specific programmes:While few instances of incorporatingsafe sanitation recommendationswithin disease-specific programmes
were identified during interviews,some very successful examples wereobtained from the literature reviewed.For example, research in Uganda showsthat providing latrines to people livingwith HIV/AIDS decreased the risk ofdiarrhoea by 31%.57Sri Lanka provides
one of the few examples wherereduction in diseases related to unsafesanitation is included as a measurablehealth programme outcome. Its HealthMaster Plan, as shown in table 4overleaf, provides a model exampleby including sanitation targets withinseveral disease-specific programmessuch as HIV/AIDS, hepatitis, diarrhoea,and water-borne disease control. In
addition, the plans targets includemeasurable outcomes such as diseasereduction as measured by hospitalrecords and mortality reduction.
7/26/2019 Sanitation Problem Health Sector
26/4422
Report
Box 6: Lessons from EthiopiaIn Northern Ethiopia, the Amhara Regional Health Bureau and the CarterCenter work in tandem to deliver health education to nearly 3,500communities. As part of the trachoma prevention programme, materialsthat include a focus on improving sanitation by promoting household latrineconstruction and use were developed, and model latrines were constructedin public gathering places, using local materials. Since 2002, more thanone million household latrines have been constructed using only minimalresources to train local leaders and health extension workers. By fostering
political support, government policy, and community education, access tolatrines rose from 6% to just over 50% of households in just one year. Follow-up research indicates that participation in health education activities was asignificant predictor of latrine ownership. In addition, political commitmentof the local government and intensive community mobilisation were twofundamental reasons for the substantial increase in latrine coverage.58By making latrine ownership a local government objective, leaders wereempowered to penalize households refusing to install latrines if necessary.Although no known use of sanctions occurred, the mere possibility of penaltyadded an element of urgency and legality to the programme. Follow-upresearch shows that high prevalence of latrines and latrine use still existedmore than three years later, demonstrating the positive impact of integratingsanitation into a disease-specific programme by definition.59
Table 4: Sanitation-related programmes within the Sri Lanka Health Master Plan 2007-2016
Health services delivery programme title Focal points Relevant agencies
1.4 Disease control programme
1.4.2.b Communicable Diseases Control:STD/AIDS Control
1.4.2.d .4 Communicable Diseases Control:Immunisable Diseases Control: ViralHepatitis Prevention and Control
1.4.2.f Communicable Disease Control:Food and Water-Borne Diseases:Control/Prevention and Control ofDiarrhoeal Diseases
1.4.2.g Communicable Diseases Control:Water-Borne Diseases Control - 2
Simple interventions like improving thehousehold level hygiene and sanitation as wellas creating awareness of these issues - of whatthey are and how they work, and access toinformation on water, hygiene and sanitationissues can bring down the burden of disease andmisery especially among the underserved andthe poor.
Ministry of Health,Provincial HealthAuthorities, NationalWater Supply andDrainage Board, LocalAuthorities, Ministryof Plantation andInfrastructure.
1.5 Programme for vulnerable populations
1.5.7 Health of People in Urban Slums Health status of a population is dependenton the living condition and water supplyand sanitation.We have to have a multi-sectoral approach inhealth prevention and promotion strategies andit should be through appropriate technology indelivering the services. Most of the activitieswe have to work with the water board, and theMunicipal council or urban councils. Also wehave to use the existing systems and mechanismto implement the programmes.
Ministry of Health,Provincial HealthAuthorities, NationalWater Supply andDrainage Board, LocalAuthorities, Ministryof Plantation andInfrastructure.
1.5.8 School Health Conduct a School Sanitation Survey annuallyand data provided to the Ministry of Educationand other relevant Ministries and Departments.Availability of sanitation and water supply.Percentage of Officers of Health providing datato the Medical Officer/Maternal and Child Health.
Ministry of EducationProvincial EducationAuthorities.
7/26/2019 Sanitation Problem Health Sector
27/44
Report
23
In Uganda, the MoWE developed astrategy to provide guidelines on howto mainstream approaches to include
persons living with HIV/AIDS in waterand sanitation service provision. Thestrategy does not propose stand-aloneactivities but instead builds on andincorporates HIV/AIDS-related activitiesinto existing sector workplans over themedium and long term.
Integrated programmes
Each of the case study countries
examined employs volunteers or paidstaff to deliver health and sanitationpromotion at the household level;however, with the possible exceptionof Malawis and Sri Lankas healthworkers, safe sanitation is not includedwithin primary healthcare approaches,which tend to be limited to curativeinterventions. In addition, countriesallocate minimal resources for field
visits, as shown in Uganda and SriLanka. Rather than conducting visitsto villages and households, healthworkers mostly operate out of clinicsand community health facilities.Currently, disease-specific programmesfocus primarily on curative measures,
whereas factors that exacerbatedisease, such as poor sanitation,often are not addressed. For example,
most of Nepals and Ugandas healthprogrammes do not include safesanitation. The proposed NepalHealth Sector Support ProgrammeII (NHSSP-II) 2010-2015, however,includes both sanitation and waterquality surveillance aspects. Actionsunder NHSSP-II include: a) promotinghygiene and sanitation through theexisting institutional infrastructure;
b) promoting hygiene and sanitationin conjunction with other essentialhealthcare services to mainstreamhygiene and sanitation promotion;and c) in partnership with relatedagencies, establishing a water qualitysurveillance system and promoting useof safe water. Under the programme,the Ministry of Health has added severalservices to the existing Essential Health
Care Services (EHCS) package, includinghygiene and sanitation promotion inpartnership with other agencies.
In Malawi, Health SurveillanceAssistants, who work directly withcommunities and interface with village
Box 7: Lessons from Pakistan
Pakistans Lady Health Workers (LHWs) programme, established in the early1990s, provides an example of integrated programming identified in theliterature. Today, over 100,000 LHWs provide the backbone of the countrysprimary healthcare approach. In at least two follow-up evaluations of theprogramme, diarrhoea incidence was reduced compared with populationsnot receiving LHW visits.60The LHW programme has been able to buck theinternational trend by providing a service with tangible health impacts,through reduction in childhood diarrhoea. However, a review of Pakistanssanitation coverage shows that only 45% of the population currently hasimproved sanitation coverage,61highlighting the complexity of the link
between increased sanitation coverage and reduction in diarrhoea (ie. theexistence of a latrine does not mean that it is being used or hygienicallymaintained in a way that ensures separation between humans and faeces).
7/26/2019 Sanitation Problem Health Sector
28/4424
Report
health committees, address sanitationwithin the EHCS package, but staffingshortages present a major constraint. In
contrast to the other three countries, SriLanka promotes sanitation throughoutdisease-specific and primary healthagendas, as well as the Health Ministry-led public information campaignsmentioned above. Another exampleof integration is provided by Uganda,where the MoWE has developed astrategy to provide guidelines on
mainstreaming HIV/AIDS issues intowater and sanitation provision. Thestrategy does not propose stand-alone
activities but instead builds on andincorporates HIV/AIDS-related activitiesinto existing sector work plans in themedium and long term.
Community Health Clubs
The community development approachemphasises bottom-up capacitybuilding to address the determinants
Box 8: Community-based approaches tohealth promotion examples from Africa:
The benefits of community-based approaches have been investigated inseveral African countries. Using information gathered over 15 yearsof creation and tracking of pilot projects in several African countries,
Juliet Waterkeyn63has shown that the community health club (CHC) approachis a cost-effective model that creates a strong demand for sanitation anda culture of healthy behaviour. Waterkeyn and her colleagues used hygienepromotion (in coordination with health agencies) to raise demand for
sanitation. Data from Zimbabwe, Uganda, and South Africa showed highlevels of community response through CHCs. Health workers provided sixmonths of weekly low-cost hygiene promotion sessions resulting in latrinecoverage rising to 43%, contrasted with 2% in the control area. Faced withscarcity of latrine hardware options and financial constraints to hardwarepurchase, the remaining 57% adopted faecal burial, a method previouslyunknown to community members which, although not ideal, signifiesan understanding of the need to remove excreta from the immediateenvironment. In rural areas, the concept of zero open defecation hasbeen enthusiastically endorsed by CHCs.
Despite the success of the CHCs, Waterkeyn notes that the health sectorsinvolvement in Ugandas CHCs from 2003 to 2005 was minimal due to the lackof staffing availability and transportation. At the district level, health workersattended workshops and then withdrew from their commitment to conductcommunity training if per diems were not provided. However, at the nationallevel the Environmental Health Department recently initiated efforts toaddress unsafe sanitation by developing a standard toolkit for participatoryhygiene and sanitation transformation (PHAST) training with a team thatis conducting training sessions in one district. Although the integration of
health and sanitation promotion through CHCs in Uganda was less successful,results elsewhere merit further exploration.
7/26/2019 Sanitation Problem Health Sector
29/44
Report
25
of health, such as safe sanitation. InUganda, village health teams (VHTs),comprised of volunteer community
members, have been used since 2003to improve the health status of villagemembers through facilitating processesof community mobilisation andparticipation in delivering, managing,and improving health practices at thehousehold level. Within the minimumhealthcare package, VHTs provideservices within a range of primaryhealthcare aspects, including diarrhoea
control and home-based managementpractices for safe sanitation. VHTsare not formally remunerated, butlocal leaders and NGOs supportthem through training opportunitiesand provision of bicycles and somecompensation. While VHTs have notbeen introduced everywhere (they havebeen established in approximately77.5%62of districts but interviewees
reported that only about one thirdof the districts have trained VHTs inall villages), experience shows thatwhere they are active, improvement insanitation practices is noted.
In Malawi, sanitation and hygienepromoters are employed to provideinformation, education, andcommunication using methods such as
drama and music. The promoters reportto Health Surveillance Assistants (HSA),and could potentially be incorporatedinto the HSA cadre. Promoters holdregular progress meetings and promoteWASH practices, including the properinstallation and maintenance oflatrines. Since 1997, Malawi has had aprogramme for early child development,later developed into an Integrated
Management of Childhood
Illnesses (ICMI) programme covering11 of Malawis poorest districts. Inthis process, community groups came
together to analyse health, nutrition,and development problems and decideon actions to address them. Thegroups tackled hygiene, sanitation,breastfeeding, and complementaryfeeding and established community-based childcare centres run bytrained community volunteers. By2000, the programme reached 1,179villages in the 11 districts. In 2004, an
assessment found significant changesin breastfeeding practices, age atintroduction of complementary feeding,disposal of faeces, and use of iodisedsalt. Conversely, no differences werefound in handwashing practices or theuse of antenatal care services.
In Nepal, approximately 47,000Female Community Health Volunteers
deployed by the health sector arebecoming increasingly pivotal forhealth improvements. This approachcan be used at a local level to providecapacity building support for sanitationpromotion, as volunteers are alreadyengaged in managing diarrhoealcases under the IMCI programme.Cross-sectoral coordination andunderstanding between the health
and WASH sectors is crucial for thesuccess of this approach. There is alsosignificant potential for synergies withNGO projects that use community-led total sanitation (CLTS) techniquesto try and raise awareness amongcommunities about the dangers ofopen defecation and to encouragebehaviour change and create demandfor improved sanitation.
7/26/2019 Sanitation Problem Health Sector
30/4426
Report
4.1.d Functional deficit 4:Collection and use of data
Collection of data is critically importantfor health workers, planners andpolicymakers for tracking trends and
monitoring the effectiveness of healthprogrammes. The quality of reportingdepends on the quality of nationalhealth-information systems, whichtend to be weak in many developingcountries.64For example, diarrhoealmortality rates may be under-reportedwhen it is the underlying rather thanthe immediate cause of death (ie. theimmediate cause of death may be
AIDS or malaria).65
Further, not alldiarrhoea cases are treated in healthfacilities, meaning that not all diarrhoealdeaths occur in these facilities anotherpotential reason for under-reporting ofboth diarrhoeal mortality and morbidity.The role of the health sector in this regardincludes participating in data collectionand information-sharing mechanisms toshift health programming from a reactive
to preventive orientation.The degree to which this occurs in thestudy countries varies significantly.Nepal has a robust Health Management
Information System (HMIS) that producesa range of detailed information forservice-delivery, supplemented by regularhousehold and facility surveys that yielddata harder to collect through routine
reporting. The surveys also shed lighton inequalities in health service use andcollect opinions on the quality of servicesprovided. Household and service deliverydata are used to validate HMIS data.
In Uganda, the Health Sector StrategicPlan (HSSP II) indicates the need forimproving the usage of the HMIS, inorder to facilitate the collection ofaccurate and reliable data in a timelymanner. It is hoped that such datawill improve planning processes atall levels. Improving the systemssensitivity to gender- and disease-specific information will allow a betterunderstanding of health inequalities andthe necessary changes in managementand planning of health facilities andservices. A multi-sectoral epidemicpreparedness and response committeehas been formed in all districts, and hasproved useful in managing epidemics.Certain challenges remain, such as theshortage of staff with the requisite skills
Findings: Promoting uptake and use of sanitation is an enduring challenge and its
absence is a barrier to progress in sanitation coverage, but it is rarely anexplicit component in health programme design.
District and local health worker practices and programmes are typicallydisease-focused and rarely consider or integrate sanitation as a strategyto reduce the disease burden (diarrhoeal and others).
Sanitation is rarely included in primary healthcare programmes andservices or meaningfully integrated into disease-specific (eg. HIV/AIDS) orintegrated programmes (eg. IMCI), but there are examples where this hasbeen successfully done (eg. the Sri Lanka Health Master Plan).
Local implementation of sanitation policies and programmes providesgood synchronicity with public health objectives as well as potentialfor improved health outcomes. There is evidence to suggest a positiverelationship between health promotion at community and householdlevel and latrine ownership and use.
7/26/2019 Sanitation Problem Health Sector
31/44
Report
27
to manage epidemics effectively, lack ofresources, and lack of prioritisation ofsuch activities at the district level.
Malawi has a HMIS, managed by thePlanning Department of the MoH, whichacts as the primary source of data for thehealth sectors monitoring and evaluationsystem. An equivalent system is used bythe education sector (EMIS). The NationalStatistics Office (NSO) also provides datafor many key indicators through reportscompiling the results of national surveys,such as the Demographic and Health
Survey and the Multiple Indicator ClusterSurvey. The water supply and sanitationSWAp calls for a Water and SanitationManagement Information System(WSMIS) to provide effective analysisand planning through access to validand timely information, and specifiesthe need for coordinating multiple datasets and systems already in place; butin practice there has been only limited
linkage between ongoing developmentof the HMIS, EMIS and WSMIS systems.
Health workers in Nepal, Uganda andMalawi rarely utilise their HMISs tomonitor sanitation-related diseases
trends and to target sanitationinterventions accordingly. Rather,HMISs are mostly used in times of
crisis. Examples of events that couldhave been mitigated through moreeffective surveillance include choleraoutbreaks in Nepals Jajarkot regionand along the shores of Lake Malawi,and a hepatitis E outbreak in northernUganda. While data are often reportedon a regular basis, they are notroutinely analysed, resulting in lostopportunities to reduce the frequencyand/or severity of disease outbreaks.
In comparison, Sri Lanka undertakesongoing data collection and monitoringby employing regional epidemiologiststo track disease patterns, includingWASH-related diseases. Because one oftheir primary responsibilities is districtmonitoring, these epidemiologistshave the authority and resourcesto follow up when needed. Their
responsibilities are also directly linkedwith monitoring for reductions in WASH-related diseases. This is a rare exampleof a health programme that includesspecific outcome targets on reduction indiseases related to unsafe sanitation.
Findings: Data and analyses are not routinely shared between sectors, especially at
district levels, resulting in lost opportunities to identify and target vulnerablepopulations (eg. low income areas, unplanned urban settlements, or areasprone to disease outbreaks).
Significant weaknesses exist within respective sector informationmanagement systems (including a lack of sanitation-related information inHMIS, as well as a lack of health information in WASH MIS).
With the exception of Sri Lanka, existing data on sanitation-related infectionsand diseases is often weakly integrated within the design, implementationand monitoring of sanitation programmes.
Critical information for tracking national, district, and local budget allocations
and expenditure for sanitation is often lacking. Furthermore information onimpact/cost-effectiveness of sanitation interventions is often inadequate foreffective results-based programme management and resource allocation.
7/26/2019 Sanitation Problem Health Sector
32/4428
Report
5.1.a LeadershipThe support of health sector leadershipis crucial for long-term sustainableimplementation of policy andprogramme changes. Leaders withinthe health sector must first determinethat sanitation is relevant to theachievement of the sectors goals and
improved health outcomes, as well asrepresenting a potential saving on thesectors resources.
In the countries studied, few solidexamples have been identified ofhealth sector leadership that activelysupports and facilitates safe sanitation.Sri Lankas President has expressedhis personal interest in ensuring thatsanitation coverage continues toincrease, using all possible governmentand other resources. In contrast,the current state of political affairsin Nepal has stalled progress onsanitation policy and programming.Health leaders in Malawi and Ugandaare overwhelmed with institutionalconstraints and the challenges ofimplementing numerous global healthinitiatives, and while in Uganda aMemorandum of Understandinghas been signed between the three
ministries responsible for sanitation,progress is constrained by lack of clearpolicy, financial resources and district-level capacity.
A positive example of leadership-drivensanitation progress is provided byKenyas Ministry of Public Health and
Sanitation, which is driving the push toreduce health disparities in her countrycaused by a myriad of issues that includeunsafe sanitation.66In March 2010, theMinister released the Policy guidelineson control and management of
diarrhoeal diseases in children under
five years, which include sanitationprovision as a cost-effective preventiveintervention to be incorporated intodiarrhoea-control activities.67
Nepals participation in the biennialSouth Asian Conference on Sanitation(SACOSAN) is a prime impetus formeeting Nepals national goal ofachieving universal sanitation coverageby 2017. Nepals delegation to pastSACOSAN conferences included uppermanagement from the Ministry ofHealth. Nepal will host SACOSAN V,currently scheduled for 2012.
5. Facilitators and barriers to healthsector addressing functional deficits
Several common facilitators and barriers that contribute to or hinderimplementation of the health sector functions described abovehave been identified over the course of this research. These includeaspects relating to leadership, financing, human resources, and
community participation.
7/26/2019 Sanitation Problem Health Sector
33/44
Report
29
5.1.b Community participation
Community participation andmobilisation is critical for long term
programme sustainability. Whenprogrammes are designed with localinput, they are more likely to achievelasting results. Sri Lanka has longembraced community participation inlocal water and sanitation projects;68a recent example is the post-tsunamirecovery project in the district of Galle.Villagers are learning about safe WASHpractices from local health workers
while also monitoring construction ofsanitation infrastructure and facilities.The latrine promotion programme inEthiopias Amhara region mentionedearlier is another relevant example.
5.1.c Human resources
A well-organised, trained, supportedand supervised workforce is neededto maximise sustainable health
outcomes.69The issue of incentivesis also crucial, not only for generalworkforce motivation but also crucially
for improved health programmeintegration, as discussed in box 9overleaf. Developing countries are
particularly susceptible to healthworker shortages, as many workersleave to obtain higher paying jobs inricher countries, and well-trained andexperienced staff, if they remain in theirown country, tend to be concentratedin urban centres or affluent areas,creating inequality between regionsand exacerbating the challenges ofdecentralisation. Human resources
issues were identified in each ofthe countries studied. Uganda andMalawi have extremely high healthcareworker shortages up to 50% in somedistricts. In addition to these shortages,training and education is also lacking.A recent review of the informationneeds of healthcare workers indeveloping countries identifies theissue of information poverty, which
leaves workers without access to theinformation they need to perform theirjobs well.70
7/26/2019 Sanitation Problem Health Sector
34/4430
Report
5.1.d Financing
The size, predictability and timing offinancial resources is a critical elementfor effective and well-functioning healthand sanitation programmes. Whereascompetition for limited financialresources can inhibit cooperation whileeach institution jealously guards its own
limited budget, if approached correctlyit can encourage health professionalsto seek creative solutions for moreeffective use of resources. Inter-sectoralpartnerships can achieve multiple goalswith limited funds. Conducting outreachwithout exploring potential financingpartnerships can result in missedopportunities to reach additionalaudiences with the same funds.
In addition to the health datachallenges described, collection offinancial data to include sanitationbudget allocations and spendingis needed. Within the case studycountries, coordinated mechanisms totrack national, district and local budgetallocations and expenses do not exist.
Further, obtaining total in-countryexpenditures related to sanitation isnearly impossible due to the myriaddifferent government and non-government funding sources.
Box 9: The role of incentivesHealth professionals can influence the use of safe sanitation practices via
their daily responsibilities. Policymakers at the ministerial and other executivelevels can legislate or mandate that sanitation be included as a priority inthe work programmes of health services. Healthcare workers and healthpromoters can guide patients and the public on safe sanitation practicesand their benefits. Information specialists can work to track health trendsinfluenced by sanitation so that policymakers and educators can respondaccordingly. But such action requires the right incentives. The performanceof health professional such as doctors, nurses and administrators is rarelyassessed against delivery of health promotion activities. Even when suchactivities are included in performance assessment, the focus is on tangible
outputs rather than outcomes such as reduction in sanitation-relatedinfections. If busy and understaffed healthcare facilities are expected todeliver such action, this expectation must be accompanied by sufficienthuman, technical and financial resources, and factored into performanceassessments. Concurrently, environmental health aspects such as sanitationand hygiene must be included in medical and nursing training curricula if theyare to be prioritised by healthcare professionals, rather than perceived asthe responsibility of volunteers or promoters. Such an approach takes intoconsideration the strong influence that healthcare professionals, particularlydoctors, have over public perceptions of what constitutes healthy behaviour.
7/26/2019 Sanitation Problem Health Sector
35/44
Report
31
This will require that sanitation isrecognised as part and parcel ofa well-functioning health system,defined as consisting of all the
organizations, institutions, resourcesand people whose primary purposeis to improve health (see box X). Werecommend that health actors aspireto deliver the following actions at threelevels international, national, andprogramme delivery.
6.1. International health policyand donor policy
At the international level, funding andprogramme priorities do not mirrorgreatest disease burden or lowestsanitation coverage. Global healthinstitutions, donors and academics canencourage health systems to targetthe greatest causes of ill-health. Whenthose causes, such as sanitation, lieoutside the health sectors traditionaldomain, development partners can help
facilitate inter-sectoral collaboration.Further, development partners should
coordinated amongst themselves tomaximise efficient use of resources andincrease results.
Recommendations for global healthinstitutions, donors, academics, andother external support agencies:
Global health institutions tochampion the recent shift away fromdisease-specific curative approachesto integrated approaches to healthpromotion and disease prevention,geared towards and assessed againstthe achievement of health outcomes.
Global health policy initiatives toacknowledge and give a higherprofile to the impact of sanitationon the global burden of disease, thepotential contribution of sanitationto reducing that burden of disease,and the potential benefits for publichealth outcomes.
Development partners to prioritiseprogramme interventions and
impact evaluations in countries withlow sanitation coverage and highsanitation-related disease burden.
6. Recommendations forhealth sector stakeholders
Sanitation infrastructure is necessary but not sufficient for betterhealth. The failure of health sector stakeholders to work jointlywith WASH sector counterparts to address key functional deficitsis constraining progress on sanitation and related health outcomes.
Various actions can be taken by international, national and local healthsector actors that could help accelerate progress on sanitation andleverage gains in health, most notably by reducing the impact of themain causes of child mortality such as diarrhoea and under-nutrition.
7/26/2019 Sanitation Problem Health Sector
36/4432
Report
Development partners to encouragehealth agencies and professionals tointegrate sanitation within existing
and future health sector policies. Development partners to promote
and support the development ofnational health plans and strategiesto target sanitation-related diseaseburden, at a level proportionateto impact.
Development partners to encouragehealth agencies and professionals tointegrate use of safe sanitation within
existing and future disease-specificand integrated health progra