Embed Size (px)
Citation preview

Postgraduate Medical Journal (1986) 62, 205-207
Sarcoidosis - a cause of steroid responsive total alopecia
S.R. Smith, M.J. Kendall, and 'G.M. Kondratowicz
Department ofTherapeutics and Clinical Pharmacology, and 'Department ofPathology, University ofBirmingham, Birmingham B15 2TJ, UK.
Summary: We present a case of sarcoidosis complicated by total alopecia and a myopathy occurringin a young West Indian woman. There was a very satisfactory response to oral steroids.
Introduction
Although cutaneous involvement in sarcoidosis isrelatively common, alopecia is rare. There are a fewreported cases ofcicatricial alopecia due to sarcoidosiswhich predominantly affects black women withevidence of intrathoracic sarcoidosis and cutaneousinvolvement at other sites (Golitz et al., 1973). Treat-ment including intra-lesional and systemic steroids hasgenerally been disappointing (Golitz et al., 1973;Rudolph et al., 1975). We have recently observedsignificant regrowth of hair after systemic steroidtherapy in a patient who presented with total alopeciadue to cutaneous sarcoidosis together with in-volvement of lung, liver and muscle.
Case report
A 23 year old West Indian woman presented with a 3month history of increasingly severe exertional dysp-noea, pain and swelling in her lower legs and anorexia.Four years earlier she had developed total alopeciaover a period ofa few weeks which had persisted apartfrom one brief episode of scanty re-growth of headhair 18 months earlier which only lasted for about onemonth. On examination there was total absence ofhead and body hair with no evidence of scarring(Figure 1). There were small oval dusky red nodulesover her wrists and ankles but no involvement of thescalp. The calf muscles were very tender to palpationand there was overlying pitting oedema. Chest expan-sion was symmetrically reduced but there were noadded sounds. There was no hepatomegaly and therest of the examination was normal.
Investigations showed deranged liver function tests,an elevated serum creatine phosphokinase and amyopathic picture on electromyography. The chest X-ray showed patchy shadowing in both lung fields but
:.
Figure 1 The patient showing alopecia.
no hilar adenopathy, and pulmonary function testsrevealed a restrictive defect with marked impairmentof gas transfer. Mantoux testing at 1 in 1,000 wasnegative despite BCG inoculation in her teens. Biopsyof liver and calf muscle with overlying skin showednumerous non-caseating granulomata. The scalp was
A) The Fellowship of Postgraduate Medicine, 1986
Correspondence: S.R. Smith, B.Sc., M.D., M.R.C.P.Accepted: 31 July 1985
copyright. on 25 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.62.725.205 on 1 M
arch 1986. Dow
nloaded from

206 CLINICAL REPORTS
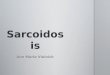
also biopsied which showed fibrosis and chronicinflammatory infiltrate around many hair follicles andsebaceous glands. In places this infiltrate was gran-ulomatous and included Langhans type giant cells(Figure 2).
Because of deteriorating liver function (serumbilirubin rising from 23 Lmol/I to 45 jimol/l and alk-aline phosphatase rising from 753 U/1 to 1,020 U/1,upper limits of the normal range being 20 Imol/l and350 U/l respectively) and increasing dyspnoea she wascommenced on prednisolone 50 mg on alternate days.During the subsequent 9 months there was completeresolution of her dyspnoea, muscle pain and legoedema, anorexia and skin nodules. The disap-pearance of the leg oedema presumably reflects con-trol of the active granulomatous inflammation in theskin and underlying muscle. In addition there has beendefinite and continuing re-growth of hair (Figure 3). Itis now about 2 cm long over most of the head andaxillary and pubic hair has also returned. Repeatbiopsy of the scalp 6 months after starting treatmentno longer showed the inflammatory reaction that was
..
.~~~~~ i::~~~~~~..~~~~~~~~~~~L~~~~~~~~~~~~~~~~~~~~~~J :,:S..'
.~~~~~~~~~~~~~~~~~~~. ~~~~~~~~~~~~~~~~~~~~~~~~~~~ ~~~~~~~~~~. ..
Figure 2 Scalp biopsy showing a granulomatous infiltratearound hair follicles and including a small well definedsarcoid granuloma and a multinucleate giant cell.
- - :::.:.. -~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......~~~~~~~~~~~~~~~~~~sl..
Djibouti:::~~~ ~ ~ ~ ~ ~ ~ ~ ~ 0i::
Figure 3 The patient showing regrowth of scalp hair and eyebrows.
copyright. on 25 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.62.725.205 on 1 M
arch 1986. Dow
nloaded from

CLINICAL REPORTS 207
present around almost all of the follicles in the pre-treatment biopsy. The liver function tests and creatinephosphokinase have returned to normal and remainedso and the pulmonary function tests have markedlyimproved. She is now taking only 7 mg ofprednisolonedaily.
Discussion
Both alopecia (Golitz et al., 1973; Rudolph et al.,1975) and myopathy (Callen, 1979) are rare manifesta-
tions of sarcoidosis. We can find no previous report oftotal alopecia occurring in sarcoidosis, nor of such aconvincing response to treatment with steroids. Hairgrowth has been progressive during the 9 months sincestarting treatment, whereas there had been no sig-nificant regrowth during the previous 4 years. Thealopecia antedated the other manifestations of sar-coidosis by several years and we suggest that cutan-eous sarcoidosis is worth considering in patients,especially coloured women, presenting with totalalopecia.
References
CALLEN, J.P. (1979). Sarcoidosis appearing initially aspolymyositis. Archives of Dermatology, 115, 1336.
GOLITZ, L.E., SHAPIRO, L., HURWITZ, E. & STRITZLER, R.(1973). Cicatricial alopecia of sarcoidosis. Archives ofDermatology, 107, 758.
RUDOLPH, R.I., HOLZWANGER, J.M. & HEATON, C.L.(1975). Diffuse cicatricial alopecia of the scalp caused bysarcoidosis. Cutis, 15, 524.
copyright. on 25 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.62.725.205 on 1 M
arch 1986. Dow
nloaded from