Embed Size (px)
Citation preview

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.
Special Needs
Plan (SNP) Model
of Care Training May 30, 2019

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.2
Lisa Roth, VP Care Coordination
Janelle Howe , Director Clinical Care
Maureen Mello, Senior Project Manager
Lisa Desai, Manager Care Coordination
Henry Argueta, Personal Assistance Line Specialist
Adalinda Gutierrez RN, BSN, PHN, Network Compliance Mgr – Clinical
Kim Kochan RN, VP Care Management – AppleCare
Gabriela Segovia, Director Ambulatory Care Management – Epic/
Beaver
Presenters

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.3
Accreditation Statement
RN: SCAN Health Plan (SCAN) is a provider approved by the
California Board of Registered Nursing (Provider #CEP-13453).
This activity has been approved for up to 1.5 contact hour(s).
BBS: Course meets the qualifications for 1.5 hours of continuing
education credit for LMFTs, LCSWs, LPCCs, and/or LEPs as
required by the California Board of Behavioral Sciences. SCAN
Health Plan is a CAMFT-approved continuing education provider.
Provider No. 127226

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.4
Questions from the Audience

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.5
First 60 min of the presentation : • SCAN’s Special Needs Plan (SNP) Model of Care (MOC)Training
– This applies to all Medical Groups delegated to provide care for
below SNP types:
Chronic Special Needs Plan (C-SNP) – Balance, heart First,
VillageHealth
Dual Special Needs Plan (D-SNP) - Connections, Connections
at Home
Institutional Special Needs Plan (I-SNP) – Healthy at Home
Second 30 min of the presentation :• SCAN’s Initial Health Assessment (IHA)/ Staying Healthy
Assessment (SHA) Training
– This applies to all Medical Groups delegated to provide care for the
below SNP type:
D-SNP – Connections, Connections at home
Important Note
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.6
Learning Objectives
Objective 1
Objective 2
Objective
3
Identify the 4
elements of model
of care
Demonstrate Audit &
oversight preparedness
Explain your
requirements as a
SNP provider

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.7
The 4 elements of SNP model of care
SNP Population
Care Coordination
Provider Network
Quality Measurement
& Performance
Special Needs Plans:
- Chronic SNP (C-SNP)
- Fully Integrated Dual
Eligible SNP (FIDE –SNP)
- Institutional SNP (I-SNP)
Care Coordination:
- Health Risk Assessment (HRA)
- Individualized Care Plan (ICP)
- Interdisciplinary Care Team (ICT)
- Care Transitions (CT)
Staff/providers deliver
care to SNP
members must
complete SNP MOC
training annually
- Measures are evaluated on
an annual basis
- SNP model of care program
evaluation process
- Quality Improvement Plan
Note : Please refer to appendix for more information on each of these elements.
Appendix slides I -VIII

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.8
Journey of a Special Needs Plan Member
Member becomes a
SNP member
SCAN Care Coordinator onboard
the memberConducts the HRA and ICP
• HRA - Health Risk
Assessment
• ICP – Individualized Care
Plan
Documents placed on SNP
sftp• Copy of the Health Risk
Assessment (HRA)
• Copy of the Individualized Care
Plan (ICP)
• Trigger Report with identified
triggers from HRA responses
Case Management
activities for triggered
SNP members begin
/and or Care Transitions
activities (Based on the
delegation status)
Note : Please refer to appendix for more information on each of these elements.
Appendix slides V-VIII

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.9
Journey Continues….(SCAN)
Member becomes a
SNP member
SCAN Care Coordinator onboard
the member
Conducts the Health
Risk Assessment, Care
Plan
Documents placed on SNP sftp
• Copy of the Health Risk
Assessment (HRA)
• Copy of the Individualized Care
Plan (ICP)
• Trigger Report with identified
triggers from HRA responses
Note : Please refer to appendix for more information on each of these elements.
Appendix slides V-VIII
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.10
Journey Continues….(SCAN Medical Group)
Note : Please refer to appendix for more information on each of these elements.
Appendix slides V-VIII
Pick up documents
placed on SNP sftp
Case Management
activities for triggered
SNP members begin /and
or Care Transitions
activities (Based on the
delegation status)
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.11
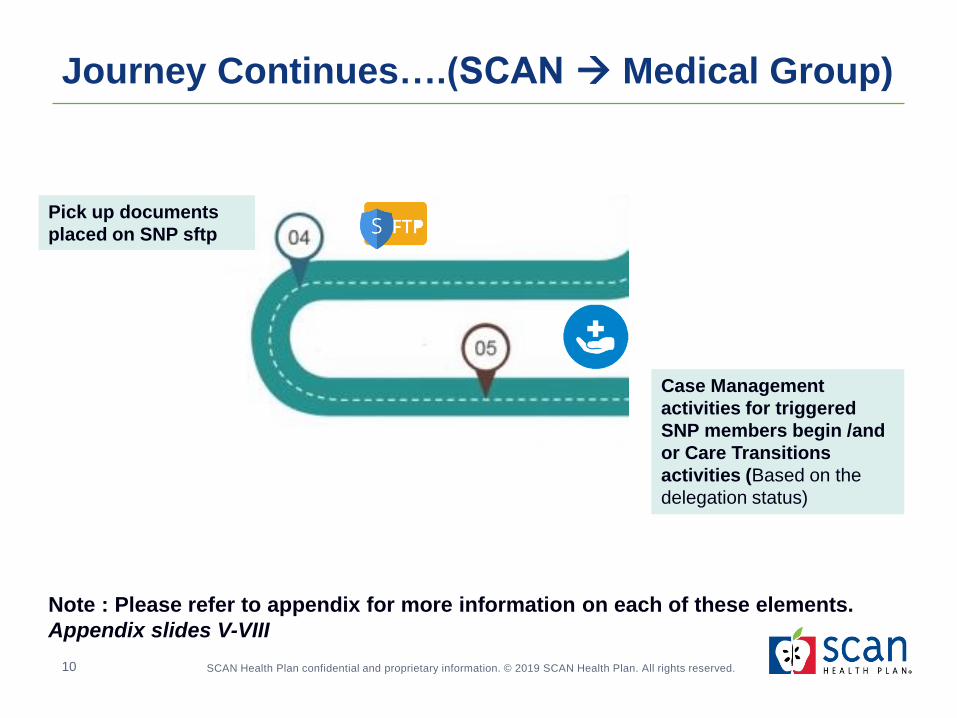
Journey Continues…. SNP Care Management
Obtain SCAN
Trigger Report
Member
Assignment
Assessment and
Problem/Opportunity
Identification
Care Plan
Development from
HRA/Member/Medical
Review
Member agreement
with Care Plan
Interdisciplinary
Care Team
Care Plan
Implementation and
Coordination of ICT
Re-evaluation of
Care Plan and
ongoing Follow-up
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.12
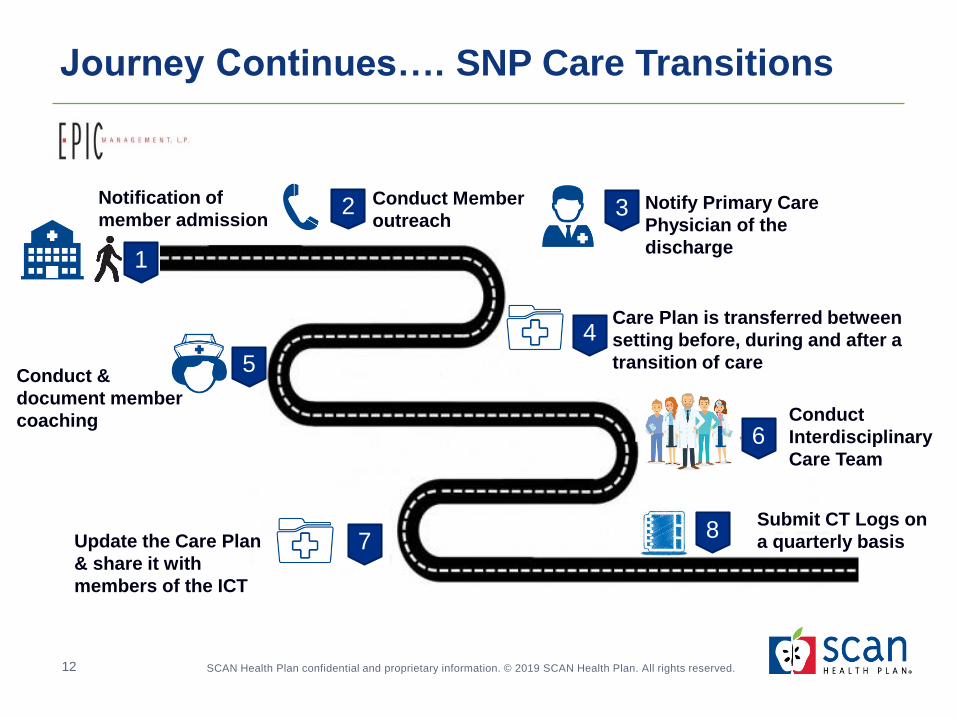
Journey Continues…. SNP Care Transitions
1
Notification of
member admissionConduct Member
outreach Notify Primary Care
Physician of the
discharge
Conduct &
document member
coaching
Care Plan is transferred between
setting before, during and after a
transition of care
2 3
4
5
Update the Care Plan
& share it with
members of the ICT
6Conduct
Interdisciplinary
Care Team
78
Submit CT Logs on
a quarterly basis

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.13
Polling Questions
When should an individualized care plan be written or revised?
a) After completing the HRA with the member
b) When discussing the health care concerns with the patient
c) Following discharge from a facility
d) If the patient raises health concerns
e) All of the above

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.14
Polling Questions
What is the minimum composition of an ICT?
a) Case Manager Assigned to member, Care Coordinator
b) Case Manager Assigned to member, Care Coordinator, Medical expert
c) Case Manager Assigned to member, Care Coordinator, Medical expert,
Member/caregiver
d) Medical expert, Member/caregiver
e) None of the above

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.15
Polling Questions
True/ False
Documentation should indicate members contacted within 5
business days post discharge from one setting to another

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.16
Audit & oversight preparedness

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.17
Audit & oversight preparedness
Ongoing Delegation Oversight
Audits
- Chart review
- Policy & Procedure Review
- Corrective Action Plans
(CAPs)
CMS Audit Preparedness
- Notification
- Chart requests (Case
Management documentation)
- End to End Case walkthroughs
(live webinars)

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.18
Questions

Thank you

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.
Initial Health
Assessment/
Staying Healthy
Assessment
Annual Provider TrainingMay/June 2019
Lisa Amin Desai
Manager, Care Coordination

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.21
Regulatory Requirements
Medicare
• Initial Assessment within 90
days of enrollment (Welcome
to Medicare)
• Annual Assessment (Annual
Wellness Visit or AWV) – once
per year
21
Medi-Cal
• Initial Health Assessment
(IHA) within 120 days of
enrollment
• Must use Staying Healthy
Assessment (SHA) Form
(DHCS approved form)
• Annual Assessment – within
365 days of previous
assessment
* SCAN Policy is for IHA/SHA to be completed within 90 days of
enrollment.

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.22
Regulatory Requirements- Specific for Medi-Medi Members
22
Initial Health Assessment
• Comprehensive Exam with PCP
• Documentation of all areas assessed
• IHA completed within 90 days of enrollment
Staying Healthy
Assessment (SHA)
• DHCS Approved Form
• Included as part of Medical Record
• Note if member declines to complete
Initial or Annual or
Preventative Visit Code
• Appropriate coding for initial and annual visits
• Code list included with IHA ASAP report
DHCS requirement to complete Initial Health Assessment
(IHA)/Staying Healthy Assessment (SHA) w/in 120 days of enrollment and annually: Title 22, CCR, Section 53851 (b)(1)

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.23
Benefits of Comprehensive Assessments
23
Patients
• Increased engagement – connect
behavior to health outcomes
• Building patient condition
awareness
• Greater patient accountability and
improved health literacy
• Increase patient ability to self
manage
Providers
• Comprehensive assessments
help identification of patient
care needs
• More accurate patient coding
• Greater ability to promote
preventative care
• Decreased acute utilization
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.24
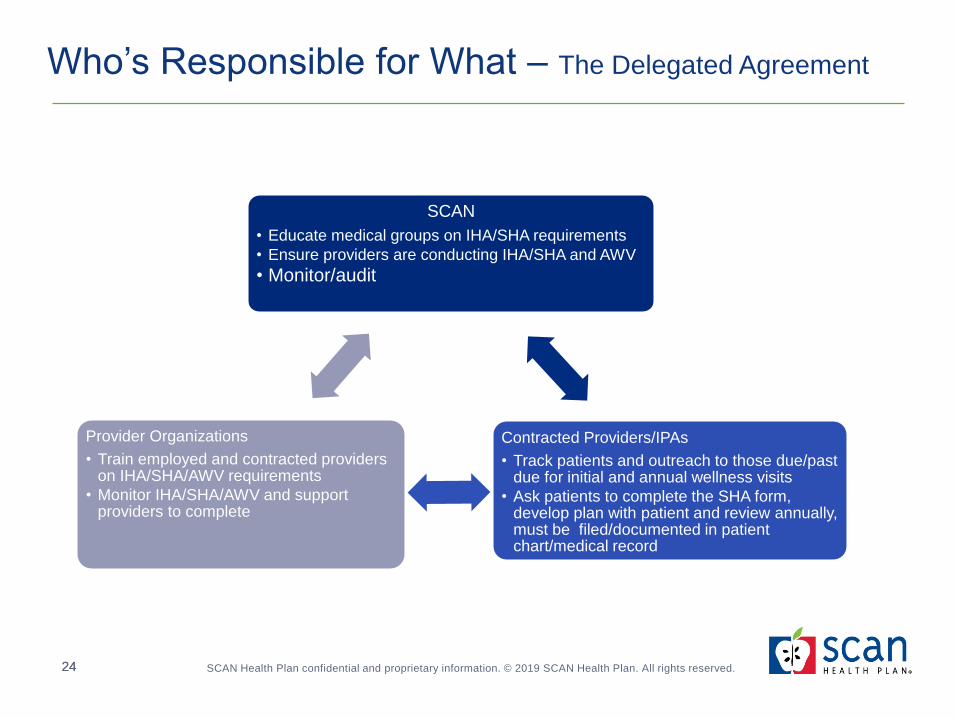
Who’s Responsible for What – The Delegated Agreement
SCAN
• Educate medical groups on IHA/SHA requirements
• Ensure providers are conducting IHA/SHA and AWV
• Monitor/audit
Contracted Providers/IPAs
• Track patients and outreach to those due/past due for initial and annual wellness visits
• Ask patients to complete the SHA form, develop plan with patient and review annually, must be filed/documented in patient chart/medical record
Provider Organizations
• Train employed and contracted providers on IHA/SHA/AWV requirements
• Monitor IHA/SHA/AWV and support providers to complete
24

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.25
Provider Group Expectations
Policies and Procedures around IHA/SHA and AWV expectations for employed and contracted
Providers
• Delineate Provider Group role in monitoring, training and supporting the completion of the
IHA/SHA and AWV
• Initial and Annual Provider Training
Monthly monitoring of completion of IHA/SHA and AWV
• Track using SCAN Provider Portal Report – IHA_ASAP Report (must access by the 15th of every
month)
• Outreach to Providers
• Outreach to Patients
Ensure Provider documentation (patient chart) includes:
• The SHA form
• Risks identified are addressed, including appropriate tests/screenings
• Areas of low risk are documented indicating why corresponding tests/screenings are not needed
25

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.26
Partnering with SCAN
26
SCAN calls each new medi-medi
member to educate on IHA/SHA during
welcome call-offers to facilitate IHA appointment
SCAN sends the SHA form to PCP
with cover letter for each new Medi-
Medi requiring IHA and SHA
You can use this PowerPoint training
presentation to train PCPs
Assigned Delegation
Oversight and HCS support point of
contact

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.27
Implementation
How do you use new patient forms?
Can the SHA form be added to new patient forms?
How frequently are patient forms updated?
Can the SHA standards be merged with you current protocol?
What are your quality monitoring processes around initial and annual
wellness PCP visits?
Can it be adjusted to meet the Medi-Cal and Medicare guidelines?
How do you promote wellness visits/preventative care with your
employed/contracted physicians?
Can the Medi-Cal and Medicare standards be integrated into your
current process?
27
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.28
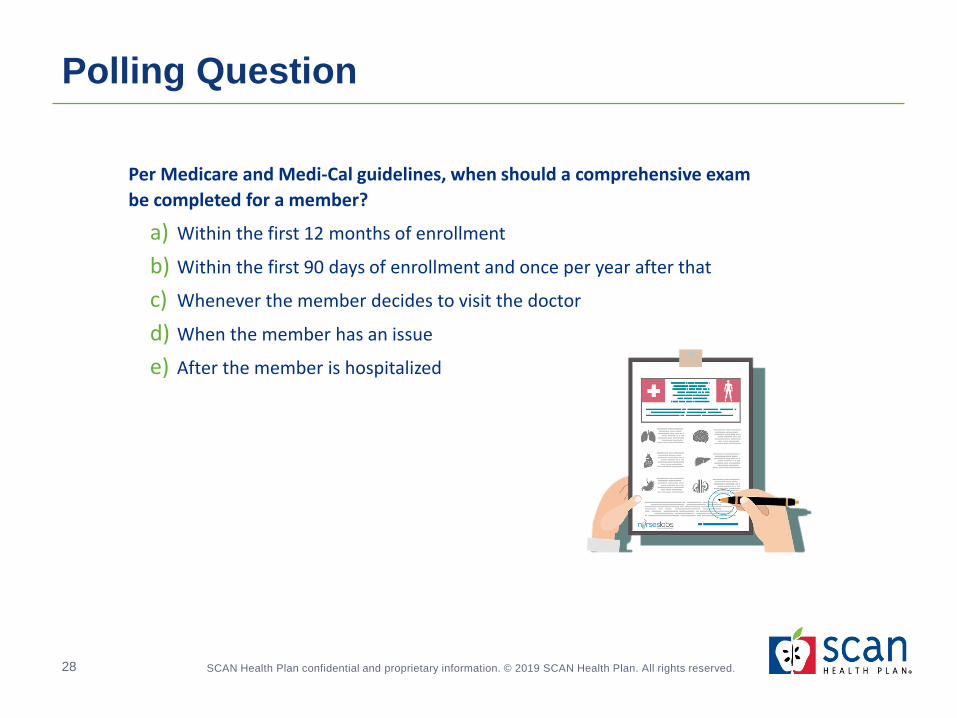
Polling Question
Per Medicare and Medi-Cal guidelines, when should a comprehensive exam
be completed for a member?
a) Within the first 12 months of enrollment
b) Within the first 90 days of enrollment and once per year after that
c) Whenever the member decides to visit the doctor
d) When the member has an issue
e) After the member is hospitalized

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.29
Resources
DHCS fact sheet/FAQ:
http://www.dhcs.ca.gov/formsandpubs/forms/Documents/MMCD_
SHA/GenDocs/SHA_FAQs.pdf
SHA forms:
http://www.dhcs.ca.gov/formsandpubs/forms/pages/stayinghealth
y.aspx
Policy Letter 13-001 (Revised):
http://www.dhcs.ca.gov/formsandpubs/Pages/PolicyLetters.aspx
United States Preventative Services Task Force:
https://www.uspreventiveservicestaskforce.org/BrowseRec/Index
29

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.30
Questions
Thank you

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.32
Appendix – IHA/SHA
I. Components of a comprehensive assessment
II. How to identify members who need IHA/SHA
III. Preparing for a DHCS audit
32

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.33
I. Components of a Comprehensive Assessment
Complete history and physical (includes, but not limited to):
• Present and past illness(es) with hospitalizations, operations, meds
• Physical exam including review of all organ systems
• Height, weight, BMI, BP, cholesterol screening
• Preventative services per USPSTF A and B Guidelines for 65-year
old (age appropriate assessments such as TB screening, clinical
breast exam, allergy, chlamydia, mammogram, pap smear)
Social history
• Current living situation/marital status
• Work history/education level
• Sexual history/use of alcohol, tobacco and drugs
33
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.34
I. Components of Comprehensive Assessment
Mental health and status evaluation
Assessment of risk factors- using the Staying Healthy Assessment (SHA)
• REQUIRED for all Dually Enrolled Medi-Cal/Medicare members
• Development of behavioral risk health education – to include assessment
of:
– Nutrition
– Functional status (including ADL/IADLs)
– Physical Activity
– Environmental Safety
– Dental/Oral Health
Diagnoses and plan of care
Clinical Based guidelines as best practice in development of plan of care
34

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.35
II. How to identify SCAN members who need
IHA/SHA
SCAN provides list of new members on monthly basis
SCAN provides detailed patient-level data through IHA ASAP Report
• To access the report on the SCAN provider portal:
– Access the SCAN Provider Portal
– Click on SCAN Documents
– Click on Network
– Access the IHA_ASAP folder
Providers are required to make reasonable attempts to contact
members and schedule IHA. SCAN recognizes best practice of
three good-faith attempts. Documented attempts that demonstrate
unsuccessful efforts to contact members to schedule IHA will be
considered evidence in meeting requirement.
35

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.36
III. Preparing for the DHCS Audit
36
Medical record request will include
checklist for all required
components
Prepare to show attestations that all PCPs were trained
on the IHA and SHA requirements
Webinar audit will include review of patient’s EMR/ Medical Record-
live in system

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.37
I. SCAN’s Mission
II. SNP types and eligibility
III. SNP goals and purpose of a SNP
IV. Division of responsibilities (plan vs. group)
V. Detailed requirements for trigger report, care plan updates,
documentation of ICT, and CT
VI. SNP sftp operations
VII. SCAN SNP resources
VIII. CMS SNP resources
Appendix – SNP MOC

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.38
I. SCAN’s Mission
SCAN Health Plan (SCAN) is the nation’s fourth largest not-for-profit
Medicare Advantage (MA) plan, serving over 180,000 members in
California.
SCAN’s mission is to keep seniors healthy and independent. We do
this is by providing comprehensive medical coverage, prescription
benefits, and support services specifically designed to meet the
unique needs of seniors.

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.39
II. SNP types and eligibility
• Eligibility verified 30 days post enrollment
• Balance Plan: Diabetes
• Heart First Plan: CHF, Arrhythmia, CAD, PVD, Chronic Venous Thromboembolic Disorder
• VillageHealth Plan: ESRD
Chronic
Special Needs Plan
(C-SNP)
• Eligibility verified monthly
• Designed for members who have both Medicare Part A and Part B, Full Medicaid benefits and FIDE SNP
• Connections and Connections at Home Plan
Fully Integrated Dual
Eligible Special Needs Plan
(FIDE-SNP/D-SNP)
• Eligibility verified by outside vendor
• Meet state criteria for Nursing Facility Level of Care (NFLOC)
• Healthy at Home Plan - Must reside in the community and not a facility (I-SNP is Institutional-Equivalent)
Institutional
Special Needs Plan
(I-SNP)

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.40
III. SNP goals and purpose of a SNP
Improve member health outcomes
Ensure appropriate utilization of services for preventative health and chronic conditions
Enhance care transitions across all healthcare settings
Improve coordination of care and ensure appropriate delivery
of services through the alignment of the HRA, ICP and ICT
Improve access and affordability to member healthcare needs
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.41
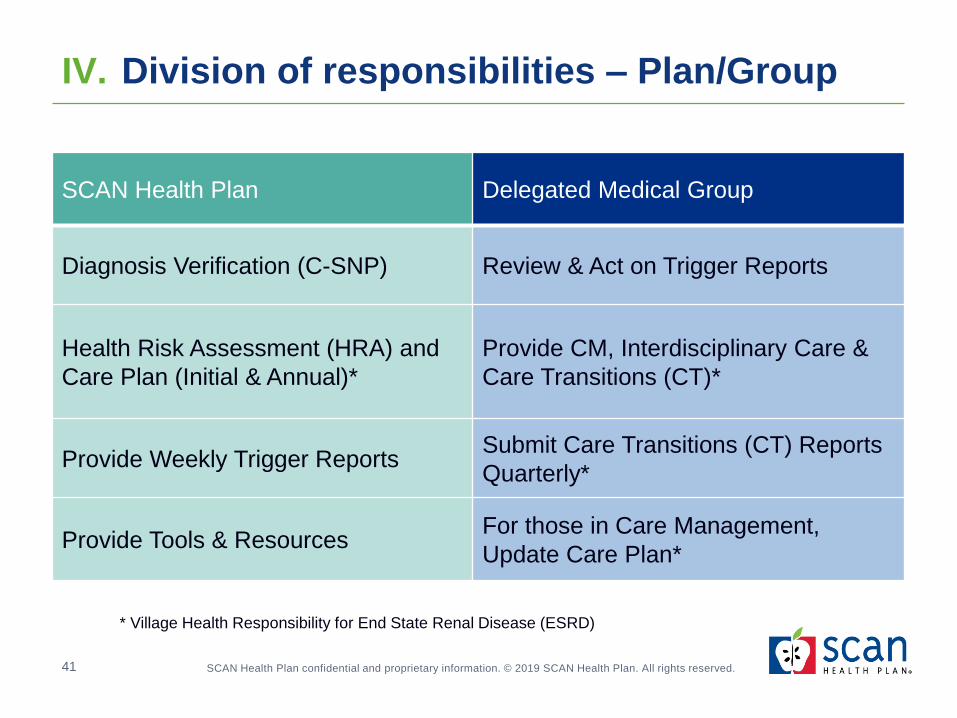
IV. Division of responsibilities – Plan/Group
Enhance care transitions across all healthcare settings
SCAN Health Plan Delegated Medical Group
Diagnosis Verification (C-SNP) Review & Act on Trigger Reports
Health Risk Assessment (HRA) and
Care Plan (Initial & Annual)*
Provide CM, Interdisciplinary Care &
Care Transitions (CT)*
Provide Weekly Trigger ReportsSubmit Care Transitions (CT) Reports
Quarterly*
Provide Tools & ResourcesFor those in Care Management,
Update Care Plan*
* Village Health Responsibility for End State Renal Disease (ESRD)

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.42
V. Health Risk Assessment (HRA)
SCAN
SCAN is responsible for the Health Risk Assessment (HRA)
• Conducted within 90 days of enrollment and annually prior to 365 days from last
Contact attempts to members include telephonic outreach, as well as letters that
include paper HRA forms to complete and return by mail
Minimum outreach attempts to member is three, we often make at least five attempts
Other SCAN assessments meet requirement of HRA (NFLOC)
HRA addresses required domains of medical, functional, psychosocial, mental health
and cognition
Screens SNP members for care coordination, complex care management (and long-
term services and supports for D-SNP)
SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.43
V. Health Risk Assessment (HRA)
Delegated Medical Group Expectation
Delegates required to retrieve HRAs, care plans and trigger reports within 7 calendar days
of posting on SCAN’s SNP sftp site (trigger reports are sent the Monday after assessment)
Delegates are required to do (within 30 calendar days of receiving the trigger report) in the
members’ records:
• Document the date the trigger report was reviewed
• Document clinical review and outreach attempts (min. 3 attempts within 2 weeks)
• Address care management triggers by analyzing findings from HRA and other
assessments and inputs and document the following:
• If unable to reach members or members decline to participate, follow organization
protocol to complete the activities based on information available in the organization’s
system and update the documentation
• Document next steps/plan of care going forward (sent letter, etc.)
• If member not enrolled in care management, reason (failed contact, declined)
• ICT documentation for all SNP members that triggers regardless of level of acuity

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.44
V. Individualized Care Plan (ICP)
SCAN
Individualized Care Plan (ICP) is developed following completion of the
initial health risk assessment (HRA) upon the members’ enrollment and
updated with each discharge from a facility or a change in health status
The ICP includes any triggers identified during the HRA process, any
concerns voiced by members during the HRA process and/or specific
concerns members would like to address with their PCP
The ICP is a dynamic document that’s updated at least annually; it may
be changed more frequently if there is a change in the members’ status
The ICP is shared via mail or electronically with members, primary care
physicians and other members of the ICT

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.45
V. Individualized Care Plan (ICP)
Delegated Medical Group Expectation
Identification of measurable goals, including prioritized goals that consider
the members’ and caregivers’ goals, preferences and desired level of
involvement in the care management plan
Measurable goals include the current status, progress to meeting the goal
and the desired outcome
Address all documented triggers with goals on the ICP
Documentation shows review and revision of the ICP as changes in health
status, function and psychosocial needs are identified (does documentation
address the member issues?)
Evidence of communication of ICP and revisions to members and primary
care physicians (was care plan sent to members and primary care
physicians?)
ICT recommendations are documented in the care plan

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.46
V. Interdisciplinary Care Team (ICT)
Delegated Medical Group Expectation
All triggered SNP members and SNP members received thru referral process need to have an
Interdisciplinary Team (ICT) completed regardless of acuity level within 30 days of referral
Minimum ICT composition (collaboration between any of the following):
• CM assigned to member
• Care coordinator (from SCAN)
• Medical expert (primary care physician, specialist, etc.)
• Members/caregivers if available
Interactions and collaborations can occur in person, telephonically or electronically (a formal ICT
meeting not necessary for all)
ICT documentation must include evidence of the following:
• Date of ICT collaboration
• List of all ICT participants (including all recommended providers)
• Interventions/recommendations
• Evidence that copy of care plan was provided to/available to ICT participants and members
Documentation that all ICT participants completed SNP MOC training

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.47
V. Care Transitions (CT)
Delegated Medical Group Expectation
Care Transitions documentation must include:
• Members contacted (or attempts made) within five business days post-
notification of discharge from one setting to another
• Notification to PCP within five business days of discharge
• Ensure follow-up services and appointments are scheduled and performed
within 5 business days of transition
• Care is provided by appropriate persons
• Care plan transferred between settings before, during, after transition of care
• Member coaching occurred
• Members of the ICT and members/caregivers have access to the plan of
care
Submission of care transition logs to SCAN SNP sftp on a quarterly basis:
• SCAN provides oversight to ensure regulatory and compliance
requirements are met

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.48
VI. SNP sftp Operations
SNP Report Job ScheduleDay of the Week
Report is Sent
Completed HRA
and Care PlansWeekly Saturdays
Trigger Reports Weekly Mondays
SNP Census Monthly 2nd of Month

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.49
VII.SCAN SNP Resources
SCAN Health Plan Website

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.50
VII.SCAN SNP Resources
SCAN Health Plan Website

SCAN Health Plan confidential and proprietary information. © 2019 SCAN Health Plan. All rights reserved.51
VIII.CMS SNP Resources
CMS Website
https://www.cms.gov
• Medicare Managed Care Manual Chapter 5
• Medicare Managed Care Manual Chapter 16b

1
SNP MOC Training 2019 – FAQ Sheet
1. What are the requirements/expectations for SCAN Trigger Report in terms of outreach, ICP, ICT? Delegates must demonstrate that the following has been completed within 30 calendar days of receiving the trigger report through documentation in the patient’s record:
Retrieval and review of the trigger report
Clinical review (HRA, assessment, utilization data, other relevant clinical data – see definition attached)
Outreach to the patient (minimum of 3 attempts within 2 weeks)
Outcome of patient conversation and identification of plan of care
Activities taken when patient unable to be contacted/declined care management
Development or update of the Care Plan (ICP) based on all identified triggers
Interdisciplinary care team (ICT) activities
Plan of care communicated to the patient and PCP
2. Some of the RN NFLOC reports are 10-12 plus pages. What are the expectations to capture all of this data? Some have 39 parts to the care plan.
The nursing facility level of care (NFLOC) is a state mandated assessment to identify those members that are at a higher need level of care that meet nursing facility level of care. These members receive additional benefits.
The care plan is provided to delegates to support their care management process in the identification of triggers, patient concerns, and interventions.
Delegates must demonstrate review and consideration of each care plan element and integration into their care management review.
3. Are members on the Trigger Report the same ones that we get from the HRA? Would there ever be a
member on the Trigger report that there is no HRA? How come for some members, we only received ICP but no HRA?
Yes, members on the trigger report are the same as the HRA report.
All members on the trigger report should have a corresponding HRA, however there are a couple of instances when you will not receive an associated HRA:
When a member is unable to be reached to complete the HRA, SCAN creates a generic care plan to support the member and delegate’s care management process.
If SCAN has pended the HRA, the HRA will be delivered at a later date
4. If the NFLOC is an HRA, why do we sometimes get both a few weeks to months apart? After we receive the HP HRA, we reach out to the member, then we receive the RN NFLOC, do we reach out to the member once again?
Generally, HRAs are completed prior to the NFLOC assessment. If the member was identified as needing Long-Term Services and Supports, they are referred for a NFLOC assessment. Hence there may be multiple HRAs.
Delegates must demonstrate that the following has been completed within 30 calendar days of receiving the trigger report, through documentation in the patient’s record:
Retrieval and review of the trigger report Clinical review (HRA, assessment, utilization data, etc.) Outreach to the patient (minimum of 3 attempts within 2 weeks) Outcome of patient interview and identification of plan of care Activities taken when patient unable to be contacted/declined CM Development or update the Care Plan (ICP) Interdisciplinary care team (ICT) activities Plan of care communicated to the patient and PCP
Health Risk Assessment (HRA)

2
SNP MOC Training 2019 – FAQ Sheet (cont...)
5. Please clarify for unable to reach members, we need to "share the care plan"?
It is a SNP requirement that all members are assessed and have a care plan
For members that you are unable to reach, a care plan must be developed based on available member data including, but not limited to:
Clinical documents, trigger reports, medication lists, utilization data (authorizations, claims), diagnoses, social information, or SDOH challenges.
The care plan is then sent to the member and PCP.
6. Do care plans need to be diagnosis based?
No. Care plans are a documented process to identify the member’s medical and non-medical issues and concerns (problems) to ensure that everyone on the care team is supporting the interventions and member outcomes.
Care plans address all triggers and member concerns identified during the HRA process and lists interventions and actions to be addressed in the future.
Individualized Care Plan (ICP)
7. Is a Social Worker required for the ICT?
The interdisciplinary care team (ICT) should include those care team members to support the members identified issues and needs.
These team members can change over time based on changes in member’s condition and identified needs.
8. What is the definition of "Medical Expert" to participate in the ICT? Do they have to be physically present at the formal ICT or can the CM discuss case over the phone with the "medical expert".
A “Medical Expert” can be a PCP, Specialist, Geriatrician or other physician provider.
ICT can be done through collaboration with the appropriate “Medical Experts” on the phone, in a formal meeting, via email, etc.
Delegates must demonstrate collaboration in their documentation.
Care Transitions (CT)
Interdisciplinary Care Team (ICT)
9. What if there is no care plan for a member undergoing a transition?
If there has been no care plan developed and the member is in transition, the delegate must demonstrate that the following has been completed through documentation:
Clinical review (HRA, assessment, utilization data, etc.) Outreach to the patient (minimum of 3 attempts within 2 weeks) Outcome of patient interview and identification of plan of care Activities taken when patient unable to be contacted/declined CM Development or update the Care Plan (ICP) Interdisciplinary care team (ICT) activities Plan of care communicated to the patient and PCP
10. Do you need to call a member on transition between settings (ex: hospital to SNF) or only once discharged
home? Presenter stated once home.
Best practice is to initiate care transitions prior to discharge (from any facility) to ensure that the patient’s needs will be met upon discharge.
Delegates must demonstrate patient outreach and care transition activities within 5 business days of discharge.

3
11. What if member discharge to hospice. Do we still do Care transition, create care plan, call member, and log
to Care transition log?
For members transitioning to hospice, it is important to remember that coordination of standard (non-hospice) care remains the responsibility of the medical group.
Delegates must demonstrate that the care plan has been updated based on the identified needs of the member and collaboration with the hospice provider to ensure the member’s needs are being met.
12. Some of hospital follow up appointments take more than 2 weeks due to volume. How do we address?
The expectation is that the groups follow the “Access and Availability standards” to coordinate with their Medical Directors to provide member care.
13. For the 5 days member outreach and PCP notification, what regulatory body requires it: NCQA? CMS?
We adopted the ICE template recommendations and changed from 3 days to 5 days for discharge notification for both member and PCP outreach. We want to align our expectations with other health plans. The industry collaborative (ICE) worked with area health plans to identify timelines for the CT intervention.
14. What are the parameters for home visits?
All D-SNP members identified as being eligible for LTSS benefits require a NFLOC assessment performed by a SCAN Field Care Manager.
15. What is the SCAN requirements for member outreach? We reach out to the member with two phone calls
and the third is a letter will this be okay?
Documentation must demonstrate 3 telephonic patient outreach attempts. (Minimum of 3 separate attempts, daily, within a 1 - 2 week timeframe).
16. I always understood a SNP case could not be closed. However, presenter stated that they will close after
30, 60, 90 days. So, a case can be closed if patient meets goals or no longer wants to participate?
Please follow your organizational care management protocol.
SNP cases may be closed after meeting organizational criteria
17. With all these audits and requirements from CMS and DHS, who and what IT or some kind of AI assistance entity has SCAN consulted or looking into consulting to assist w/ making all these care planning and audits sustainable, consistent and replicable so nurses can focus on empowering wellness w/our members than paperwork focused so much?
SCAN acknowledges the challenges you experience in applying these requirements and agree that the focus must be on empowering wellness. Please work with your assigned HCS contact and auditor to collaborate on quality improvement opportunities. We look forward to working with you.
18. Will you please provide us with the most recent information about the pals program and how to contact
them?
Enclosed is a fact sheet on the PAL team, including a contact email for Lisa Desai at SCAN for more information or to connect directly with a member's PAL.
19. Are the PALs available to talk with the Medical Group case managers? Or are they only for the members.
The Personal Assistance Line (PAL) Program is a dedicated, non-clinical care coordination unit with specialized SCAN employees trained to respond to questions about Medicare and Medicaid benefits and to assist with care coordination, identification and access to needed care and services.
Yes, you can call our PALS.
SNP MOC Training 2019 – FAQ Sheet (cont...)
Other

4
11.
SNP MOC Training 2019 – FAQ Sheet (cont...)
20. Is there a way that social workers can identify those members who are Medi-Medi (Connections or Connections at Home)? Many times, we cannot determine what plan they are on to assist with social work outreach, especially with HRA's we receive for follow up? Is there a plan code that we can utilize?
Refer to the SNP Monthly Membership Report that is posted on the SNP sftp site on the 2nd day of each month.
This report identifies all SNP members that are active with your medical group and their current plan type description.
Initial Health Assessment (IHA)
21. Slide 22 referenced IHA due at 120 days and 90 days. Confused as to time frame IHA needs to be done by. Is a medicare IHA due by 90 of enrollment and Medical 120? Or are you changing the requirement to be for both medi-CAL and Medicare to be within 90 days?
The Special Need Plan (SNP) members are members with Medicare and Med-Cal benefits. Based on the dual eligibility, the Medi-Cal guidelines apply for these members.
The Medi-Cal requirement for IHA/SHA is 120 days and Medicare is 90 days. To make it consistent, SCAN require 90 days for all.
22. When will these days of IHA requirement be enforced? For future audit timeline.
These guidelines are currently in effect.

Care Transition
Clinical Review Components: Patient/Member demographics
a. Age
b. Language
c. Availability of transportation
d. Social support and living situation
Benefits
HRA Responses
NFLOC
Trigger Report
Presence of Advance Directive or End of Life Plan (AHCD, POLST, DPOA) a. Goals of care
Care Level / Acuity based on criteria (identification of acuity and existing acuity)
Problem List (Concerns and Management)
a. Observed and reported
Current medical records
a. CM Notes/Assessments
i. 6 months of notes
b. Office visits (PCP and Specialists)
i. 12 months of care visits including Urgent Care
c. Medication list
i. Pharmacy claims data, refill gaps, High risk meds, are members on 8+ meds
d. Lab reports (especially related to chronic conditions)
e. Facility admits/discharges within past 12 months
i. Care Transitions
f. Patient/Member education
g. Current care plan (PGIs)
i. Care plan updates within past 6 months
h. Behavioral Health needs / Substance Use
Interdisciplinary Care Conferences
Change in Health Status: 1. Access to care challenges
2. Admission/Discharge from a facility (e.g., acute, rehab, SNF, LTC)
3. Additional chronic diagnosis since last review
4. New medications, high risk medications, or changes in medications (Why, Education, Understanding)
5. New Patient/Member concern(s)
6. Changes in lab data related to chronic condition (e.g., HbA1c, Cholesterol)
7. Changes in functional status (e.g., falls, cognition, ADLs, IADLs)
8. Adherence challenges (appointments, medications, plan of care)
9. Other pertinent conditions
Clinical Review & Change in Health Status Guidelines

Fact Sheet
March 2019
Personal Assistance Line (PAL) SCAN offers a dedicated customer service unit with specialized SCAN employees trained to respond to questions from Dual Eligible Members about their Medicare and Medi-Cal benefits and to assist with care coordination and identification and access to needed care and services. The SCAN Personal Assistance Line (PAL) conducts outbound calls to welcome dual eligible members to SCAN and receives inbound calls on a dedicated toll-free number.
Criteria:
Dually enrolled members - members with Medicare and Medicaid
Interventions:
Welcome Call conducted within the first 90 days of enrollment o Reviews SCAN Medicare and Medicaid benefits o Reviews how the managed care system works: the primary care physician’s role,
how to get referrals to specialists, medications, etc. o Facilitates an Initial Health Assessment (IHA) and Staying Healthy Assessment
(SHA) appointment with the primary care physician o Identifies continuity of care issues, such as getting authorization with the new
medical group for oxygen, hospital beds, and specialist services o Completes initial and annual Special Needs Plan Health Risk Assessments (HRA) o Screens the member for case management needs based on pre-established
criteria, as well as long-term services and support needs
Follows up with medical groups and providers to ensure that members receive their referrals, acts as a liaison between the member, medical groups, and SCAN case management programs
Assists members with their transportation benefit to medical appointments
Identifies and assists with Medi-Cal eligibility issues
Educates the member on Grievance and Appeals process/State Fair Hearings
Goals:
Improve customer service and experience
Provide culturally and linguistically appropriate services
Increase member satisfaction and retention
Reduce barriers and access to care issues
For more information, contact Lisa Amin Desai, Manager, Care Coordination, at 562-637-1228 or [email protected]