Embed Size (px)
Citation preview

Psychiatry Research 57 (1995) 155- 167
PSYCHIATRY
RESEARCH
Schizophrenic patients’ perceptions of their relatives’ attitudes
Martha C. Tompson*a, Michael J. Goldsteinayb, Malta B. Lebellb“, Lois I. Mintzb, Stephen R. Marderb3c, Jim Mintzb
“UCLA Family Project, Department of Psychology, Universitv of California at Los Angeles, 405 Hilgard Avenue, Fran: Hall.
Los Angeles, CA 90024-1563, USA bDepartment of Psychiatry, University of California at Los Angeles, Neuropsychlatric Institute, 760 Westwood Plaza,
Los Angeles, CA 90024, USA ‘Psychiatry Service (116A), West Los Angeles Veterans Administration Medical Center, Brentwood Dir’ision.
II301 Wilshire Boulevard, Los Angeles, CA 90073. USA
Received 4 February 1994; revision received 9 August 1994: accepted 7 November 1994
Abstract
Although the attitudes of family members as revealed by measures of expressed emotion (EE) have been shown to be associated with the course of schizophrenic illness, little is known about how patients perceive these attitudes. A detailed interview was used to assess patients’ perceptions of their family members’ behaviors toward them. Family members’ EE was assessed with the Five-Minute Speech Sample (FMSS). Overall, patients’ perceptions of criticism
were congruent with a component of the FMSS-EE that measures criticism. Results indicated that when family members had high EElcritical scores, patients perceived them as displaying more instances of critical behavior. All cases in which patients’ perceptions of criticism were incongruent with measures of FMSS-EE occurred among ethnic minority group members. Although the FMSS-EE did not predict outcome in this study, patients who perceived their
relatives as higher in criticism had more negative outcomes at 1 year. These findings suggest that when family environments are examined in patients from ethnic minority groups, the patient’s perspective may be a more potent predictor of outcome than traditional measures of EE.
Keywords; Family environment; Speech, content analysis; Expressed emotion; Prognosis; Psychotic exacerbation
1. Introduction
Expressed emotion (EE), a measure of critical and emotionally overinvolved attitudes on the part of family members toward a mentally ill patient, has frequently been examined as a predictor of
* Corresponding author, Tel: +I 310 825-3798; Fax: +l 310 206-7832.
psychiatric outcomes (for review, see Hooley, 1985; Leff and Vaughn, 1985). Indeed, patients with relatives who have high EE have been found to have higher rates of relapse in a number of stud- ies. Measures of EE have traditionally been made by counting the number of criticisms and rating emotional overinvolvement in the Camberwell Family Interview (CFI; Vaughn and Leff, 1976b). An alternative approach is the Five-Minute
0165-1781/95/$09.50 0 1995 Elsevier Science Ireland Ltd. All rights reserved SSDI 0165-1781(95)02598-Q
156 M.C. Tompson et al. /Psychiatry Research 57 (199.5) 155-167
Speech Sample (FMSS; Gottschalk and Gleser, 1969), which provides a brief method of estimating EE (Magana et al., 1986). Both the CFI and the FMSS obtain information from an individual in- terview with the patient’s relative. Thus, while trained raters assessing the interview with the rela- tive may evaluate him or her as critical or emo- tionally overinvolved, it is not clear that the patient’s perceptions of the relative are similar. Schizophrenic patients’ perceptions of their family members’ EE have not been directly compared to traditional EE measures.
Evidence that patients’ perceptions of the family may be important is found in a recent study of depressed patients. Using a prospective design, Hooley and Teasdale (1989) examined the rela- tionships between EE, perceived criticism, and relapse in 39 patients hospitalized for depression. To assess EE, a CFI was administered to each patient’s spouse; perceived criticism was rated by patients on a IO-point Likert-type scale; and relapse was assessed at follow-up evaluations 3 and 9 months after discharge. Patients’ ratings of perceived criticism were highly predictive of relapse at both follow-up times. In fact, all patients who rated their spouses as r6 points on the lo- point perceived-criticism scale relapsed. The cor- relations between EE measures and patients’ perceptions of criticism were moderate, and both were predictive of outcome.
While the results of the above study are pro- vocative, they may not generalize readily to those with schizophrenic disorders. Schizophrenic pa- tients have been found to be poor judges of others’ emotional states when compared with normal sub- jects, particularly in ambiguous situations (Cramer et al., 1989). Scott and his associates (Scott and Alwyn, 1978; Scott et al., 1993) have conducted a series of studies examining schizophrenic patients’ perceptions of their family members’ attitudes. They used the Family Interpersonal Perception Test, in which all participating family members rate how they see themselves, how they see the other family members, and how they believe the others see them. In a recent study (Scott et al., 1993), in which patients were followed for 2 years, patients’ expectations about how they were seen by their parents predicted outcome. Those who ex-
pected their parents to view them negatively were significantly more likely to relapse than those who expected their parents to view them positively. In- deed, the patient’s viewpoint was the best predic- tor of outcome. Only among those patients who relapsed, however, was there a significant correla- tion between the parents’ view of the patient and the patient’s expectation.
Using the Parental Bonding Instrument (Parker et al., 1979) Warner and Atkinson (1988) found an interaction between patients’ perceptions and degree of contact in predicting psychiatric out- come. Patients in high contact (at least once week- ly) who rated a family member as high risk (low in care and/or high in protection on the Parental Bonding Instrument) had more and longer hospi- tal admissions and longer periods of exacerbation; by contrast, those in low contact with family members whom they rated as high risk had fewer, shorter hospitalizations and shorter periods of ex- acerbation. Indeed, this effect was independent of medication compliance.
In our recent study of l-year psychiatric out- comes in a group of schizophrenic patients (Lebell et al., 1993), respondents were asked to rate both their feelings about their relatives and their relatives’ feelings about them. Ratings were made on 5-point Likert-type scales from “mostly very strong positive feelings and thoughts” to “mostly very strong negative feelings and thoughts.” In ad- dition, family members completed the Patient Re- jection Scale (Kreisman et al., 1979). Survival analyses indicated that although the Patient Rejec- tion Scale did not predict outcome, patients’ ratings of their perceptions of their family members’ feelings toward them were highly predic- tive of psychiatric outcome at 1 -year followup. Pa- tients with more positive ratings had a lower risk of symptomatic exacerbation. Indeed, the lowest risk of relapse was associated with patients’ posi- tive ratings and a high degree of contact, sug- gesting that family environments that are perceived by patients as supportive may have a protective impact for patients.
In sum, there is evidence that patients’ percep- tions of their relatives’ attitudes, as well as EE, may predict psychiatric outcomes. Yet, the global ratings in our prior study yield little information
h4.C. Tompson et al. /Psychiatry Research 57 (199.0 155-167 157
about the actual nature of schizophrenic patients’ perceptions of their relatives’ attitudes. Ratings of high EE may be based on criticism or emotional overinvolvement, but it is not clear whether these two attributes are perceived differently by pa- tients. In addition, little is known about what other attributes of schizophrenic patients may be associated with their perceptions of EE.
This study was designed to examine and clarify three questions: (1) How do schizophrenic patients perceive their family members’ attitudes as ascer- tained by an EE measure? (2) Are certain at- tributes of schizophrenic patients associated with their perceptions of their family members? (3) Which is a better predictor of outcome - EE or patients’ perceptions of their family members’ atti- tudes? Assessments of family members’ EE levels were made with the FMSS (Magana et al., 1986). Patients were administered an interview designed to assess their perceptions of their relatives’ attitudes and their family environments.
2. Methods
2.1. Subjects Participants were drawn from a larger sample
(n = 81) of patients involved in an ongoing 2-year study of early prediction of relapse in schizophrenic patients on low doses of neuroleptic medication. (For a more detailed description of the larger study, see Marder et al., 1991.) Patients in the larger study group were recruited from the inpatient and outpatient facilities of the West Los Angeles VA Medical Center, Brentwood Division, and participated voluntarily. Criteria for inclusion in the study were (1) a DSM-III-R (American Psychiatric Association, 1987) diagnosis of schizophrenia based on information taken from the Present State Examination (Wing et al., 1974) (2) age of 18-60 years, (3) competency to give informed consent, and (4) suitability for mainte- nance on low doses of neuroleptic medication. Subjects were excluded from the study if they showed evidence of organic impairment, severe alcoholism, or chronic substance abuse. All pa- tients were stabilized on a dose of 5-10 mg of injectable fluphenazine decanoate every 2 weeks.
Within the larger study was nested a smaller
study of family factors and their relationship to schizophrenic illness (see Lebell et al., 1993). The 33 male outpatients in this study were those who had at least one family member with whom they were in frequent contact. They ranged from 32 to 49 years of age (mean age = 35.7) and had on aver- age 13 years of education. African-Americans represented the largest ethnic group (46%) follow- ed by Caucasians at 30%, Latinos at 15%, and Asian-Americans at 9%. The patients had an aver- age age of onset of schizophrenia of 25.8 years and had been ill an average of 9.25 years. The majority of patients (70%) lived with their relatives. Although the Lebell et al. (1993) project, of which this study is a part, included 39 subjects, six of these patients were excluded from the present investigation, as their “significant other person” was not a close relative. Thus, a total of 33 patients were included. Relatives were primarily parents (n = 30) and spouses (n = 4) although one sibling and one aunt who had caretaking roles in the patients’ lives were also included. As three of the patients were in dual-parent families they conse- quently had interview data about two different relatives and FMSS-EE data from both their relatives. To avoid a lack of independence of observations, the relative who had the most con- tact with the patient was selected for the analyses, and data for the other relative were dropped. Thus, a total of 33 patient-relative dyads were examined.
2.2. Treatment protocol All patients in the study were stabilized on a
dose of 5-10 mg of injectable fluphenazine decanoate every 2 weeks. In addition, many pa- tients received oral medication (Cogentin, Artane) for extrapyramidal side effects that resulted from the neuroleptic treatment.
2.3. Monitoring of exacerbations The Brief Psychiatric Rating Scale (BPRS;
Overall and Gorham, 1962) was used to monitor clinical changes and measure psychotic exacerba- tions. It was administered on a monthly basis (more frequently if ratings suggested a worsening of symptoms) by several raters who were unaware of the subjects’ medication condition.
158 h4. C. Tompson et al. /Psychiatry Research 57 (1995) 155-167
Cluster scores, each of which combined several subscales on the BPRS, were calculated. The clusters, derived from factor analysis, were defined as follows: (1) Psychoticism - conceptual disorganization, hallucinatory behavior, and un- usual thought content; (2) paranoia - hostility, suspiciousness, and uncooperativeness. A total BPRS score was also obtained by summing the patient’s scores on all the items. A psychotic ex- acerbation (terminology for relapse in this study) was defined as an increase ~3 points above base- line on either the psychoticism or paranoia clusters of the BPRS or an increase r4 points on the two clusters combined.
2.4. Assessments - relatives
As soon as possible after each patient was clinically stabilized and had consented to the pro- cedure, his relative was contacted by a staff person at the VA (because of logistic constraints, not all relatives were contacted immediately; however, all subjects were collected within the first 15 weeks of their stabilization and entry into the study). If the relative consented to participate, he/she was in- vited to the VA hospital. The relative was seen in a single session, approximately 30 min in duration, at which the following measures were ad- ministered: (1) the FMSS (Magana et al., 1986) and (2) a measure assessing the relative’s frequency of contact with the patient (which was dichot- omized to yield two scores: high, defined as 135 h/week; and low, defined as <35 h/week).
The instructions for the FMSS are as follows: A little later I’m going to be asking you some ques- tions about [patient’s name], but first I’d like to hear your thoughts about [him/her] in your own words and without my interrupting you with ques- tions or comments. So when I ask you to begin, I’d like you to speak for 5 min, telling me what kind of a person [patient’s name] is and how you get along together. After you’ve begun to speak, I’d prefer not to answer questions until the 5 min are over. Do you have any questions before we begin? [Standard response to questions] Anything you think would be important for me to understand [patient’s name] and how you get along together. Okay, please begin [start stopwatch].
In addition, several additional scales were com-
pleted that were not a part of the present study. These scales are discussed in Lebell et al. (1993).
Sixteen of the 36 relatives were unable to come to the hospital, and thus the procedure was carried out over the telephone for this group. A previous study, which used a telephone version of the FMSS, found no differences in the rates of low and high EE for relatives interviewed on the telephone and those interviewed in person @bell, 1983). In addition, a x2 test of association revealed no sig- nificant relationship between relatives’ FMSS-EE ratings and type of interview (on phone or in per- son) for the present sample (x2 = 0.295, NS). Four of the FMSS interviews were conducted in Spanish (these protocols were scored by a bi- lingual rater).
The FMSS ratings for EE were performed according to criteria developed by Magana et al. (1986). The coding system for the FMSS-EE in- cludes four scoring categories: (1) the quality of the initial statement, (2) a relationship rating, (3) the number of critical comments, and (4) a rating of emotional overinvolvement. Although there is some overlap in coding categories with those used for scoring the CFI, different criteria are employed for assigning high EE ratings. As with the CFI, a relative is given a high EE rating on the basis of criticism or emotional overinvolvement.
High EE - critical. The criteria for a rating of high EE based on criticism are any of the follow- ing: (1) a negative initial statement, (2) an overall negative rating for the patient-relative relation- ship, or (3) one or more critical comments about the patient.
High EE - emotionally overinvolved. The cri- teria for a rating of high EE based on emotional overinvolvement (EOI) include any of the follow- ing: (1) a report of self-sacrificing/overprotective behavior, (2) an emotional display during the in- terview, or (3) a combination of two of the follow- ing: excessive detail about the past, one or more statements of positive attitude, and excessive praise (five or more positive remarks). An individ- ual can be rated as high EE for both criticism and EOI.
All FMSS ratings were completed by a trained rater. Ten protocols were completed by an ad- ditional rater to assess reliability. The K statistics
M.C. Tompson et al. /Psychiatry Research 57 (1995 I 155-167 159
(Cohen, 1960) for the FMSS-EE ratings were as follows: Overall FMSS-EE (K = 0.74) and FMSS- EElcritical (K = 1.00). Raters agreed on the EE/EOI categorization for 9 of the 10 protocols.
2.5. Assessments - patients After speaking with the relative, the same exam-
iner interviewed the patient and administered: (1) the FMSS (which was not examined in this study), (2) an amount-of-contact questionnaire, which assessed how close the patient lived to the relative (or with the relative) and how many hours of con- tact he had with the relative each week (amount of contact has been an important mediating variable in previous investigations; Vaughn and Leff, 1976a), and (3) the Patient Interview for Assessing Patient Perceptions of Family Relationships (PPI; designed by Lois Mintz, Malta Lebell, and Michael J. Goldstein). The PPI was designed to elicit the patient’s perceptions of his family rela- tionships and of the key relative’s emotional atti- tudes toward him.
The PPI consisted of questions about the rela- tionship in nine areas and focused on eliciting descriptions of the patients’ perceptions about the behavior of their relatives. The nine areas included four groups of questions about the relatives’ criticism, four about EOI, and one about how much the relative nags the patient.
The four groups of questions designed to elicit perceptions of criticism included the following areas: (1) relationship difficulties, (2) unrealistic expectations by the relative, (3) disagreements with the relative over other interpersonal relationships, and (4) conflicts with the relative. The four groups of questions designed to elicit perceptions of EOI covered the following areas: (1) overprotec- tiveness, (2) the relative’s propensity to worry, (3) excessive involvement in the patient’s other in- terpersonal relationships, and (4) the relative’s in- trusiveness. For the above areas, if the patient answered a question aflirmatively or in any other way suggested that difficulties existed in the rela- tionship, the interviewer probed to ascertain the nature of these difficulties. The final group of questions began with the inquiry “do you ever feel that [relative] nags you about things?” and specifically asked about 13 areas in which relatives
might nag, including chores, medication compli- ance, excessive sleep, and money management.
2.6. Rating of patients' perceptions of relatives’ EE The Manual for Coding Patients’ Perceptions of
Their Relatives’ EE, specifically designed for this study, was used to assess the amount of criticism and EOI that patients reported. Perceptions were divided into the following three categories, each of which consisted of a frequency count of the num- ber of statements the patient made indicating a perception in that category:
Perceived criticism. The category included any statement by the patient (or an aflirmative answer to any question) indicating that he/she found the relative to be critical of, disapproving of, annoyed by, or angry toward him/her. Scores ranged from 0 to 15 (mean = 3.6, SD = 3.3).
Perceived nagging. The category included any affirmative response to any of the questions about the specific areas in which the patient may feel the relative sometimes nags, harasses, “bugs,” grumbles at, or otherwise complains about the patient’s behavior. There are 13 areas covered plus one additional area specified by the patient. Scores ranged from 0 to 8 (mean = 3.1, SD = 2.0).
Perceived EOI. The category included any state- ment by the patient (or affirmative answer to a question) indicating that the patient found the relative to be intrusive, excessively involved in his/her life, or overly protective. Scores ranged from 0 to 11 (mean = 3.9, SD = 2.8).
These data will subsequently be referred to as frequency of perceptions of (1) critical behavior, (2) nagging, or (3) EOI behavior. To assess the re- liability of these ratings, 10 interviews were dually rated. The K coefficients for each category were as follows: perceptions of critical behavior (K = O.86), perceptions of nagging (K = 0.92). and perceptions of EOI behavior (K = 0.90).
3. Results
The following questions were examined: (1) What is the relationship between relatives’ FMSS- EE ratings and patients’ perceptions? (2) Is there a relationship between demographic and illness- related variables, relatives’ FMSS-EE, and pa-
160 M.C. Tompson et al. /Psychiatry Research 57 (1995) 155-167
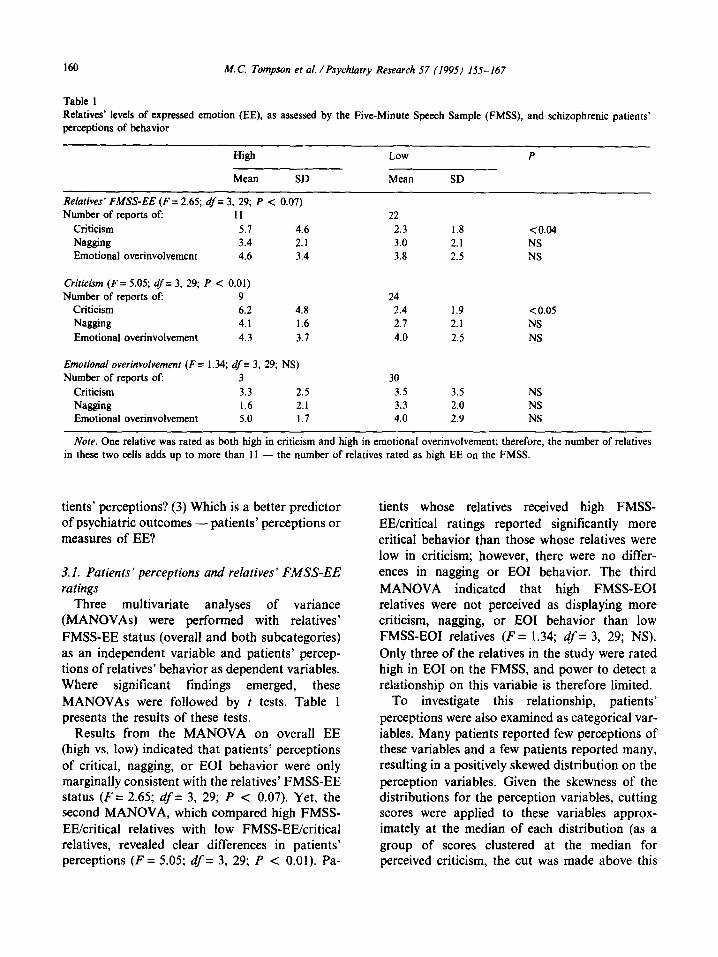
Table 1 Relatives’ levels of expressed emotion (EE), as assessed by the Five-Minute Speech Sample (FMSS), and schizophrenic patients’ perceptions of behavior
High Low P
Mean SD Mean SD
Relatives’ FMSS-EE (F= 2.65; df= 3, 29; P < 0.07) Number of reports of: II 22
Criticism 5.7 4.6 2.3 1.8 <0.04 Nagging 3.4 2.1 3.0 2.1 NS Emotional overinvolvement 4.6 3.4 3.8 2.5 NS
Criticism (F= 5.05; df= 3, 29; P < 0.01) Number of reports of: 9 24
Criticism 6.2 4.8 2.4 1.9 < 0.05 Nagging 4.1 1.6 2.7 2.1 NS Emotional overinvolvement 4.3 3.7 4.0 2.5 NS
Emotional overinvolvement (F = 1.34; df = 3, 29; NS) Number of reports of: 3 30
Criticism 3.3 2.5 3.5 3.5 NS Nagging 1.6 2.1 3.3 2.0 NS Emotional overinvolvement 5.0 I.7 4.0 2.9 NS
Note. One relative was rated as both high in criticism and high in emotional overinvolvement; therefore, the number of relatives in these two cells adds up to more than 1 I - the number of relatives rated as high EE on the FMSS.
tients’ perceptions? (3) Which is a better predictor of psychiatric outcomes - patients’ perceptions or measures of EE?
3.1. Patients’ perceptions and relatives’ FMSS-EE ratings
Three multivariate analyses of variance (MANOVAs) were performed with relatives’ FMSS-EE status (overall and both subcategories) as an independent variable and patients’ percep- tions of relatives’ behavior as dependent variables. Where significant findings emerged, these MANOVAs were followed by t tests. Table 1 presents the results of these tests.
Results from the MANOVA on overall EE (high vs. low) indicated that patients’ perceptions of critical, nagging, or EOI behavior were only marginally consistent with the relatives’ FMSS-EE status (F = 2.65; df = 3, 29; P < 0.07). Yet, the second MANOVA, which compared high FMSS- EE/critical relatives with low FMSS-EE/critical relatives, revealed clear differences in patients’ perceptions (F = 5.05; df = 3, 29; P < 0.01). Pa-
tients whose relatives received high FMSS- EE/critical ratings reported significantly more critical behavior than those whose relatives were low in criticism; however, there were no differ- ences in nagging or EOI behavior. The third MANOVA indicated that high FMSS-EOI relatives were not perceived as displaying more criticism, nagging, or EOI behavior than low FMSS-EOI relatives (F = 1.34; df = 3, 29; NS). Only three of the relatives in the study were rated high in EOI on the FMSS, and power to detect a relationship on this variable is therefore limited.
To investigate this relationship, patients’ perceptions were also examined as categorical var- iables. Many patients reported few perceptions of these variables and a few patients reported many, resulting in a positively skewed distribution on the perception variables. Given the skewness of the distributions for the perception variables, cutting scores were applied to these variables approx- imately at the median of each distribution (as a group of scores clustered at the median for perceived criticism, the cut was made above this
M.C. Tompson et al. /Psychiatry Research 57 (1995) 155-167 161
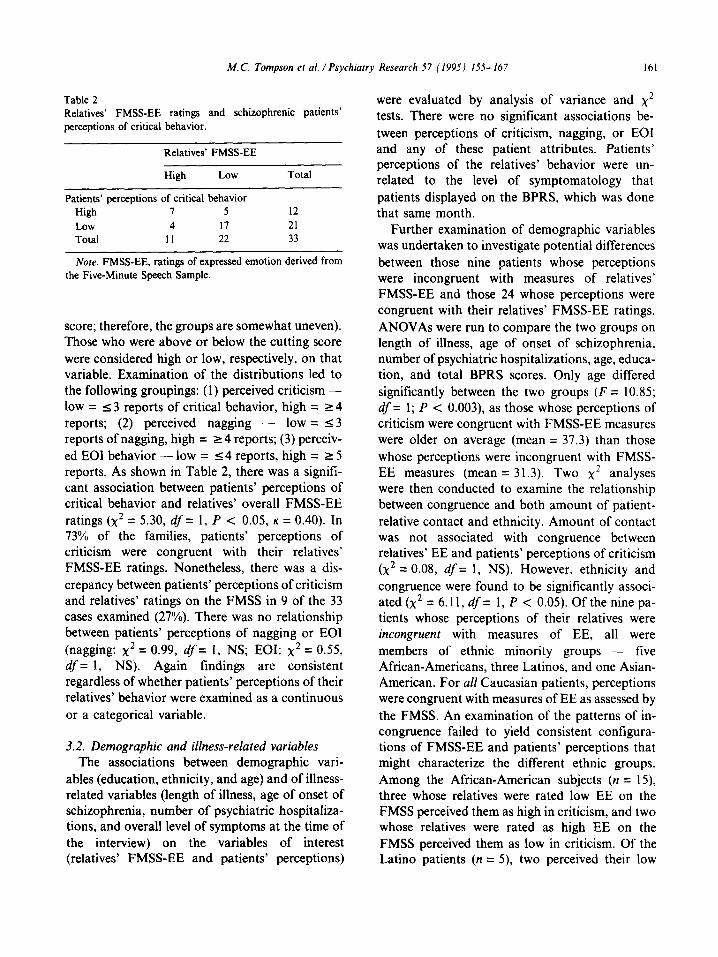
Table 2 Relatives’ FMSS-EE ratings and schizophrenic patients’ perceptions of critical behavior.
Relatives’ FMSS-EE
High Low
Patients’ perceptions of critical behavior
Total
High 1 5 I2
Low 4 I7 21
Total II 22 33
Note. FMSS-EE, ratings of expressed emotion derived from the Five-Minute Speech Sample.
score; therefore, the groups are somewhat uneven). Those who were above or below the cutting score were considered high or low, respectively, on that variable. Examination of the distributions led to the following groupings: (1) perceived criticism - low = 5 3 reports of critical behavior, high = L 4 reports; (2) perceived nagging - low = 53 reports of nagging, high = r 4 reports; (3) perceiv- ed EOI behavior - low = 5 4 reports, high = L 5 reports. As shown in Table 2, there was a signifi- cant association between patients’ perceptions of critical behavior and relatives’ overall FMSS-EE ratings (x2 = 5.30, df= 1, P < 0.05, K = 0.40). In 73% of the families, patients’ perceptions of criticism were congruent with their relatives’ FMSS-EE ratings. Nonetheless, there was a dis- crepancy between patients’ perceptions of criticism and relatives’ ratings on the FMSS in 9 of the 33 cases examined (27%). There was no relationship between patients’ perceptions of nagging or EOI (nagging: x2 = 0.99, df = 1, NS; EOI: x2 = 0.55, df = 1, NS). Again findings are consistent regardless of whether patients’ perceptions of their relatives’ behavior were examined as a continuous or a categorical variable.
3.2. Demographic and illness-related variables The associations between demographic vari-
ables (education, ethnicity, and age) and of illness- related variables (length of illness, age of onset of schizophrenia, number of psychiatric hospitaliza- tions, and overall level of symptoms at the time of the interview) on the variables of interest (relatives’ FMSS-EE and patients’ perceptions)
were evaluated by analysis of variance and x2 tests. There were no significant associations be- tween perceptions of criticism, nagging, or EOI and any of these patient attributes. Patients’ perceptions of the relatives’ behavior were un- related to the level of symptomatology that patients displayed on the BPRS, which was done that same month.
Further examination of demographic variables was undertaken to investigate potential differences between those nine patients whose perceptions were incongruent with measures of relatives’ FMSS-EE and those 24 whose perceptions were congruent with their relatives’ FMSS-EE ratings. ANOVAs were run to compare the two groups on length of illness, age of onset of schizophrenia, number of psychiatric hospitalizations, age, educa- tion, and total BPRS scores. Only age differed significantly between the two groups (F = 10.85; df = 1; P < 0.003), as those whose perceptions of criticism were congruent with FMSS-EE measures were older on average (mean = 37.3) than those whose perceptions were incongruent with FMSS- EE measures (mean = 31.3). Two x2 analyses were then conducted to examine the relationship between congruence and both amount of patient- relative contact and ethnicity. Amount of contact was not associated with congruence between relatives’ EE and patients’ perceptions of criticism (x2 = 0.08, df= 1, NS). However, ethnicity and congruence were found to be significantly associ- ated (x2 = 6.11, df = 1, P < 0.05). Of the nine pa- tients whose perceptions of their relatives were incongruent with measures of EE, all were members of ethnic minority groups - five African-Americans, three Latinos, and one Asian- American. For all Caucasian patients, perceptions were congruent with measures of EE as assessed by the FMSS. An examination of the patterns of in- congruence failed to yield consistent configura- tions of FMSS-EE and patients’ perceptions that might characterize the different ethnic groups. Among the African-American subjects (n = 15), three whose relatives were rated low EE on the FMSS perceived them as high in criticism, and two whose relatives were rated as high EE on the FMSS perceived them as low in criticism. Of the Latin0 patients (n = 5), two perceived their low
162 M. C. Tompson et al. /Psychiatry Research 57 (1995) 155-167
FM!%-EE relatives as critical, while one perceived a high FMSS-EE relative as low in criticism. Of the Asian-American patients (n = 3), one perceiv- ed a high FMSS-EE relative as low in criticism. Thus, while there may be an effect for ethnicity on the congruence between patients’ perceptions and relatives’ FMSS-EE ratings, consistent patterns of association are not apparent.
3.3. Psychotic exacerbation and relatives’ FMSS-EE
Survival analyses were used to examine the rela- tionship between relatives’ FMSS-EE ratings and patients’ subsequent clinical course. Relatives’ ratings on overall FMSS-EE, FMSS-EE/critical, and FMSS-EE/EOI were also entered as predictor variables in separate nonparametric survival models. Log-rank tests of the equality of the survi- val curves indicated that none of these variables significantly predicted psychotic exacerbation at 1 year.
0.8
3.4. Psychotic exacerbation and patients’ percep- tions of relatives’ behavior
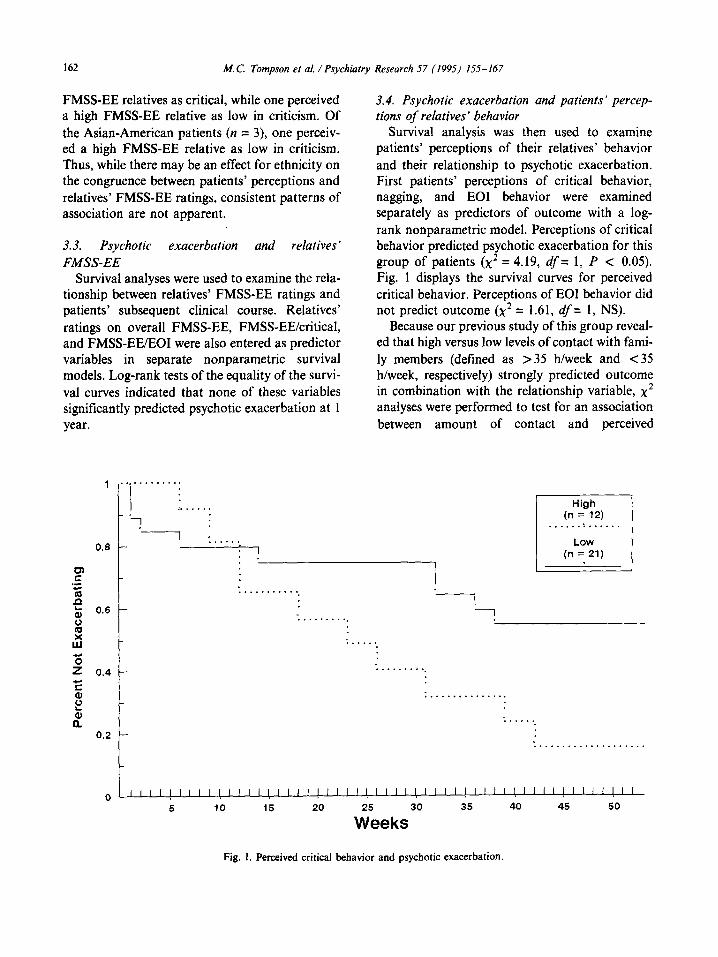
Survival analysis was then used to examine patients’ perceptions of their relatives’ behavior and their relationship to psychotic exacerbation. First patients’ perceptions of critical behavior,
nagging, and EOI behavior were examined separately as predictors of outcome with a log- rank nonparametric model. Perceptions of critical behavior predicted psychotic exacerbation for this group of patients (x2 = 4.19, df = 1, P < 0.05). Fig. 1 displays the survival curves for perceived critical behavior. Perceptions of EOI behavior did not predict outcome (x2 = 1.61, df = 1, NS).
Because our previous study of this group reveal- ed that high versus low levels of contact with fami- ly members (defined as >35 h/week and <35 h/week, respectively) strongly predicted outcome in combination with the relationship variable, x2 analyses were performed to test for an association between amount of contact and perceived
High (n = 12) l-----l . . . . . . . . . . . . .
LOW (n = 21)
F I
‘L i------j
2 1 . ’ . * * . - - . : -1 & 0.6 - ‘1
is . . . . . . . . . .
I3 :.....
ij 2 0.4 - . . . . . . . . . .
2 b
. . . . . . . . . . . . . . .
t a T.....
0.2 - : . . . . . . . . . . . . . . . . . . .
I 0 ““““‘~““~““~““~““~““~““~““~ I I I I I I I
i5 10 15 20
Ii&eks
30 35 40 45 50
Fig. 1. Perceived critical behavior and psychotic exacerbation.
M.C. Tompson et al. /Psychiatry Research 57 (19951 155-167 163
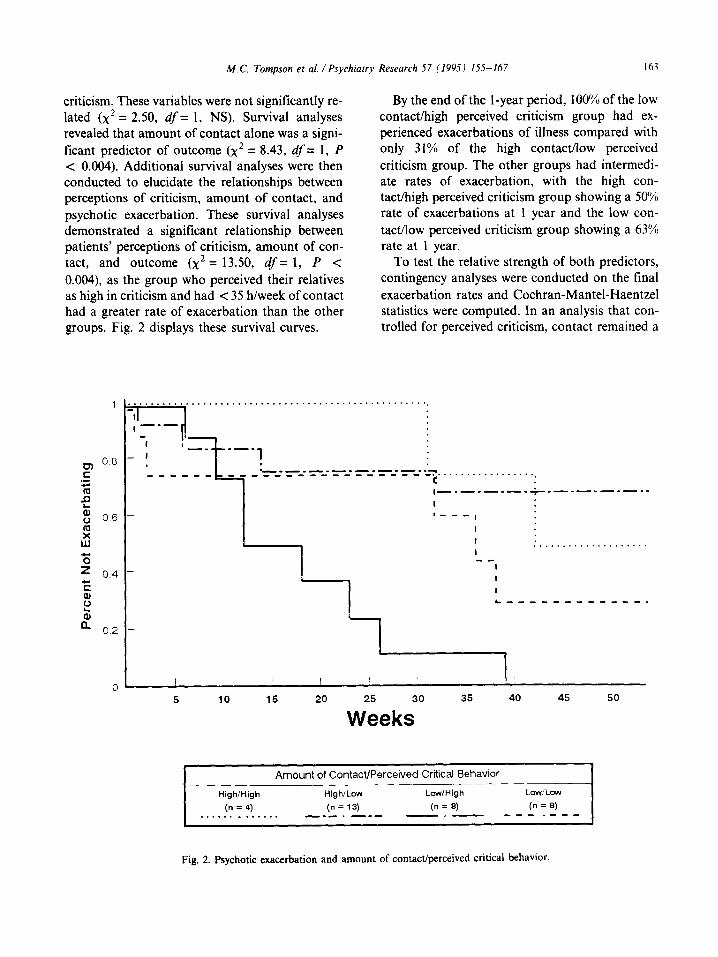
criticism. These variables were not significantly re- lated (x2 = 2.50, df= 1, NS). Survival analyses revealed that amount of contact alone was a signi- ficant predictor of outcome (x2 = 8.43, d’= 1, P < 0.004). Additional survival analyses were then conducted to elucidate the relationships between perceptions of criticism, amount of contact, and psychotic exacerbation. These survival analyses demonstrated a significant relationship between patients’ perceptions of criticism, amount of con- tact, and outcome (x2 = 13.50, df= 1, P < 0.004), as the group who perceived their relatives as high in criticism and had < 35 h/week of contact had a greater rate of exacerbation than the other groups. Fig. 2 displays these survival curves.
By the end of the l-year period, 100% of the low contact/high perceived criticism group had ex- perienced exacerbations of illness compared with only 31% of the high contact/low perceived criticism group. The other groups had intermedi- ate rates of exacerbation, with the high con- tact/high perceived criticism group showing a 50% rate of exacerbations at 1 year and the low con- tact/low perceived criticism group showing a 63% rate at 1 year.
To test the relative strength of both predictors, contingency analyses were conducted on the final exacerbation rates and Cochran-Mantel-Haentzel statistics were computed. In an analysis that con- trolled for perceived criticism, contact remained a
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -1
I -.-
-1 I -_ _-- - I ! L--.-----.-e--c-.
_ _ _ _ _ _ _ ____ _ _ _ _ _ _ _ _ _ _ _ _ e................... *Ii c i i ,-_-_-_-_+.__-.--a--
I - ‘__‘,
I
I . . . . . . . . . . . . . . . . . . . . I __
I -
I
I
-
‘1 ‘I___________.
5 10 15 20 25 30 35 40 45 50
Weeks
Amount of Contact/Perceived Critical Behavior
High/High
(n = 4) . . . . . . . . . . . . .
High/Low Low/High Lcw/Low
(n = 13) (n = 8) (n = 8) ___. ___ - ~ - _ _ - . _ - -
Fig. 2. Psychotic exacerbation and amount of contact/perceived critical behavior.

164 M.C. Tompson et al. /Psychiatry Research 57 (1995) 155-167
significant predictor of outcome (common odds ratio estimate = 6.083, q’s= 1, P < 0.05). In an analysis that controlled for amount of contact, perceived criticism was somewhat weakened as a predictor of outcome (common odds ratio estimate = 3.132, df = 1, P = 0.077). Computation of a Breslow-Day statistic revealed no interaction between amount of contact and perceived criticism in predicting outcome by the end of the followup period (Breslow-Day = 1.389,. df = 1, NS). There was a trend, however, toward an interaction at the 6-month followup point (see Fig. 2).
Because earlier analyses indicated potential ethnic differences in patients’ perceptions of their relatives, analyses were conducted to examine the relationship between outcome and patients’ perceptions of criticism within the separate ethnic groups in the study. A series of x2 analyses exam- ined the relationship between presence or absence of psychotic exacerbation at 1 year and both amount of contact and patients’ perceptions of criticism within the difference ethnic groups.
Although there was a high rate of exacerbation (80%) among the 10 Caucasian patients, it is interesting to note that nine of the 10 Caucasian patients were in low contact with their relatives and eight of these patients had a psychotic exacer- bation. The only Caucasian patient who was in high contact with a relative did not have a psychotic exacerbation. Thus, contact with relatives correctly predicted outcomes for 90% of the cases. For the Caucasian patients, there was no relationship between psychotic exacerbation and perceptions of criticism (log-rank x2 = 1.67, df = 1, NS). A low degree of contact was maintain- ed despite the fact that 60% of the patients lived with their relatives, and the interviews suggested that low contact was almost always initiated by the patients.
Conversely, among the African-Americans, con- tact was not related to outcome (log-rank x2 = 1.25, df = 1, NS). However, patients’ percep- tions of their relatives’ criticism correctly predicted outcome in 87% of the cases (log-rank x2 = 6.25, df = 1, P < 0.02). In five of the six cases in which patients perceived their relatives as highly critical, the patient had experienced an exacerbation of ill- ness by 1 year. By contrast, in only one of the nine
cases in which patients perceived little criticism did the patient have a psychotic exacerbation,
In the remaining subgroup, which included eight patients from several ethnic backgrounds (three of whom experienced exacerbations), there was neither a relationship between amount of contact
(x2= 1.65, df = 1, NS) nor a relationship between patients’ perceptions of criticism and psychiatric outcomes (x2 = 0.18, df = 1, NS). Failure to observe significant relationships could reflect both the small number of subjects and the ethnic hetero- geneity of this composite subgroup.
4. Discussion
While there was not complete overlap, overall patients’ perceptions and relatives’ FMSS-EE were congruent. Patients with high FMSS-EE relatives tended to perceive them as behaving in a more critical manner than did those with low FMSS-EE relatives. These findings are also consistent with previous work with the same group of patients (Lebell et al., 1993) which found a moderate cor- relation between patients’ rating of their relatives’ attitudes and feelings and a measure of relatives’ attitudes (the Kreisman Patient Rejection Scale) but differential prediction of outcome by these two measures. While FMSS-EE ratings, patients’ perceptions of nagging, and patients’ perceptions of EOI behavior did not predict outcome, patients’ perceptions of critical behavior, in particular, were associated with a higher risk of psychotic exacer- bation at 1 year. When patients’ perceptions of criticism were combined with amount of contact, a higher degree of prediction was achieved. In- deed, in the most deleterious situation, where contact was low and perceptions of criticism were high, all patients relapsed. These patients may rep- resent a particularly socially isolated and unsup- ported group. Conversely, when contact was high and perceptions of criticism were low, only 31% relapsed by 1 year. In this group, contact with the relative seemed to provide a measure of protec- tion, buffering the patient from stress and leading to better outcomes. Again, these findings are con- sistent with the earlier study of these patients by Lebell et al. (1993), in which those who rated their relationships negatively and reported little contact
M.C. Tompson et al. /Psychiatry Research 57 (199s) 155-167 165
with their family members were at the greatest risk for psychotic exacerbation within 1 year.
Although patients’ perceptions were congruent with FMSS-EE measures in 75% of families, ap- proximately one-quarter of patients, all ethnic minority group members, perceived their relatives’ behavior as different from that which a measure of EE might reflect. For Caucasian patients, percep- tions were 100% congruent with FMSS-EE mea- sures, but only amount of contact, not patients’ perceptions, predicted outcome. In the subgroup of African-American patients, perception of criticism was a potent predictor of outcome, sug- gesting that traditional measures of EE may be less valuable in predicting outcome than patients’ perceptions of their relatives’ attitudes, particular- ly in ethnic-minority populations.
Previous studies of EE in non-Caucasian populations have revealed different rates for various ethnic groups. Examining EE in the families of schizophrenic individuals in both urban and rural populations in India, Wig et al. (1987) found that ratings of high EE were very rare. In addition, in contrast to studies of British popula- tions, where warmth and criticism were seldom coupled, family members in the Indian study fre- quently expressed criticism and warmth simultaneously. A study of Spanish-speaking Mexican-American families with a schizophrenic member in southern California also found low rates of EE (Jenkins et al., 1986). Alternatively, in a low-income urban sample, the majority of whom were African-Americans, investigators found high rates of criticism on the CFI (Moline et al., 1985). However, when using the traditional cutting score of six criticisms on the CFI to define high EE status, these investigators found only a weak rela- tionship between EE and outcome. Using a higher cutting score of nine criticisms yielded a more ac- curate prediction of outcome. Still, among the sub- sample of African-Americans, Moline et al. (1985) found that no cutoff score was effective in predict- ing outcome.
If family environment and relatives’ attitudes are conceptualized as potentially affecting out- comes in schizophrenia, it seems that patients’ perceptions of these family attributes may be more important than an outsider’s assessment of them.
Various researchers have suggested the importance of examining the meaning of EE within a cultural context (Jenkins and Karno, 1992). Indeed, the present findings highlight the importance of understanding potential cultural differences in the perception and interpretation of affect within families. By assessing patients’ perceptions, re- searchers tap into an “insider’s view” and thus may more clearly explicate the impact and mean- ing of such differences.
Two limitations of this study are apparent: (1) Use of the FMSS to assess EE. Most researchers who have examined the relationship between EE and outcome have used the CFI to assess EE. However, one followup study using the FMSS is currently available, and it indicates a high level of prediction of l-year outcome for children with de- pression (Asarnow et al., 1993). Those children with high FMSS-EE parents were much more like- ly either to relapse or to have a continuing mood disorder at l-year followup than those children with low FMSS-EE parents. Yet, there are no comparable data for schizophrenic populations. Thus, the relationship between FMSS-EE mea- sures and outcome in this population has yet to be clarified. In view of the lower overall base rate for assigning high EE status when the FMSS is used, it is certainly possible that some cases rated as low FMSS-EE in this study would have had high EE ratings if the CFI had been used. (2) Limited num- ber of relatives on whom data were available. Only one relative was assessed for all but three of the 33 patients. Thus, not all relatives who were centrally involved with the patients were included. Indeed, for several patients in dual-parent families, only one relative was interviewed. In addition, several patients had stepparents whose FMSS-EE was not assessed. Such missing data may be important in defining the overall impact of the family on outcome.
In sum, past studies indicate that rates of family members’ negative attitudes, as well as their im- pact, may differ as a function of ethnic and cultural background. The present study suggests, however, that it is the meaning of EE which may differ cross-culturally. Various ethnic groups may indeed have different criteria for defining critical and EOI behavior and attitudes. When a definition
166 M.C. Tompson et al. /Psychiatry Research 57 (1995) 155-167
based on the criteria of the dominant culture is ap- plied to subgroups within that culture, important family variables may be inaccurately defined. That which is labeled “critical” by the dominant culture may not be so recognized by other groups who hold divergent definitions of critical behavior. Thus, by simply altering the cutting score for the number of criticisms to define high EE in various ethnic groups, researchers may miss some impor- tant aspects of the family environment.
In view of the small number of patients upon which of these analyses were based, the results must be examined cautiously. However, while such findings may not confirm the nature of ethnic dif- ferences in these processes, they highlight the im- portance of looking at differences between ethnic minority groups in studying family factors and in understanding the impact of cultural norms on the relationship between the family and psycho- pathology.
Acknowledgments
This research was supported by a predoctoral fellowship to the first author (National Institute of Mental Health Training Grant MH-14584), the Department of Veterans Affairs Medical Research Service, National Institute of Mental Health (NIMH) Grant MH-41573 (S.R. Marder, princi- pal investigator), and the UCLA Clinical Research Center for the Study of Schizophrenia, NIMH Grant MH-30911 (R.P. Liberman, Director). Special thanks go to Kim Hughes, Ana Magana- Amato, Sandra Malik, Helen Widlansky, Laura Woudstra, Lisa Yuan, and Sibyl Zaden for their assistance in this project.
References
American Psychiatric Association. (1987) DSM-III-R: Diag- nostic and Statistical Manual of Mental Disorders. 3rd rev. edn. American Psychiatric Press, Washington, DC.
Asamow, J.R., Tompson, M.C., Goldstein, M.J. and Guthrie, D. (1993) One-year outcomes of depressive disorders in child psychiatric inpatients: evaluation of the prognostic power of a brief measure of expressed emotion. J Child Psycho1 Psychiatry 34, 129- 137.
Cohen, J. (1960) A coefficient of agreement for nominal scales. Educ Psycho1 Meas 20, 37-46.
Cramer, P., Weegman, M. and O’Neil, M. (1989) Schizo- phrenia and the perception of emotions: how accurately do schizophrenics judge the emotional states of others? Br J Psychiatry 155, 225-228.
Gottschalk, L.A. and Gleser, G.C. (1969) The Measurement of Psychological States Through the Content Analysis of Verbal
Behavior. University of California Press, Berkeley, CA. Hooley, J.M. (1985) Expressed emotion: a review of the critical
literature. Clin Psycho1 Rev 5, 119-139. Hooley, J.M. and Teasdale, J.D. (1989) Predictors of relapse in
unipolar depressives: expressed emotion, marital distress, and perceived criticism. J Abnorm Psycho1 94, 229-235.
Jenkins, J.H. and Karno, M. (1986) The meaning of expressed emotion: theoretical issues raised by cross-cultural research. Am J Psychiatry 149, 9- 12.
Jenkins, J.H., Kamo, M., De la Selva, A., Santana, F., Telles, C., Lopez, S. and Mintz, J. (1986) Expressed emotion of relatives, maintenance drug treatment, and relapse in schizophrenia and mania. Psychopharmacol Bull 22, 621-627.
Kreisman, D.E., Simmons, S.J. and Joy, V.D. (1979) Rejecting the patient: preliminary validation of a self-report scale. Schizophr Bull 5, 220-222.
Lebell, M.B. (1986) Family affect and schizophrenic relapse: An exploratory study of four assessment procedures. Un- published doctoral dissertation, Institute for Clinical Social Work, Los Angeles, CA.
Lebell, M.B., Marder, S.R., Mintz, J., Mintz, L.I., Tompson, MC., Wirshing, W., Johnston-Cronk, K. and McKenzie, J. (1993) Patients’ perceptions of family emotional climate and outcome in schizophrenia. Br J Psychiatry 162, 751-754.
Leff, J. and Vaughn, C. (1985) Expressed Emotion in Families: Its Significance for Mental Illness. Guilford Press, New York.
Magana, A.B., Goldstein, M.J., Kamo, M., Miklowitz, D.J., Jenkins, J. and Falloon, I.R.H. (1986) A brief method for assessing expressed emotion in relatives of psychiatric pa- tients. Psychiatry Res 17, 203-212.
Marder, S.R., Mintz, J., Van Putten, T., Lebell, M.B., Wirsh- ing, W. and Johnston-Cronk, K. (1991) Early prediction of relapse in schizophrenia: an application of receiver operat- ing characteristics (ROC) methods. Psychopharmacol Bull
27, 79-82. Mohne, R.A., Singh, S., Morris, A. and Mehzer, H.Y. (1985)
Family expressed emotion and relapse in schizophrenia in 24 urban American patients. Am J Psychiatry 142,
1078-1081. Overall, J.E. and Gorham, D.R. (1962) The Brief Psychiatric
Rating Scale. Psycho1 Rep 10, 799-812. Parker, G., Fairley, M., Greenwood, J., Jurd, S. and Silove, D.
(1982) Parental representations of schizophrenics and their association with the onset and course of schizophrenia. Br J Psychiatry 141, 573-581.
Scott, R.D. and Alwyn, S. (1978) Patient-parent relationships and the course and outcome of schizophrenia. Br J Med Psycho1 51, 343-355.
Scott, R.D., Fagin, L. and Winter, D. (1993) The importance

M. C. Tompson et al. /Psychiatry Research 57 (19951 155-167 167
of the role of the patient in the outcome of schizophrenia.
Br J Psychiatry 163, 62-68. Vaughn, C.E. and Leff, J.P. (1976a) The influence of family
and social factors on the course of psychiatric illness: a
comparison of schizophrenic and depressed neurotic
patients. Br J Psychiarry 129, 125-137. Vaughn, C. and Leff, J. (1976b) The measurement of expressed
emotion in the families of psychiatric patients. Br J Sot
Psycho1 15, 157-165.
Warner, R. and Atkinson, M. (1988) The relationship between
schizophrenic patients’ perception of their parents and the
course of the illness. Br J Psychiatry 153, 344-353. Wig, N.N., Menon, D.K., Bedi, H., Ghosh. A., Kuipers, L.,
Leff, J., Korten, A., Day, R., Sartorius, N., Ernberg. G. and
Jablensky (1987) Expressed emotion and schizophrenia in
North India. Br J Psychiatry 151. 156-173.
Wing, J.K., Cooper, J.E. and Sartorius, N. (1974) Descriprion
and Classification of Psychiatric Symptoms.. An Instruction Manual for the PSE and CATEGO Systems. Cambridge
University Press, London.