Embed Size (px)
Citation preview
School-Based Autism
Assessments: Review of Current
Practices & Guidelines for a
Comprehensive Assessment
Angela Davis, Ph.D.
Jeanne Anne Carriere, Ph.D.
Kelly Kennedy, Ph.D.
Goals for Today’s Workshop
1. Introduction to ASD/assessment
2. Review data on a survey completed by California school psychologists
3. Discuss relevant case law for school-based autism assessments
4. Openly discuss planning and conducting of a comprehensive school-based autism evaluation
Why conduct research in this area?
• A meta-analysis examined the content of ASD
research in six school psychology research
journals (McKenney et al., 2015).
• Researchers found that only 38 articles over a
10-year span (2002-2012) discussed autism-
related topics. Out of these articles, only five
reviewed assessment and identification of ASD.

Reasons for Increased Attention &
Improved Identification of ASD
• Early identification and treatment can change the
course of the disorder.
• Given “increased rates”, educators are more likely to
encounter students with ASD.
• Students under an Autism eligibility have increased four fold between
1999 and 2012 (currently 10% of SWD and 1% of K-12 population)
• The majority of children with autism are identified
through school resources.
• Average age of ASD identification is about 4 years of age.
• African American & Latino children often diagnosed 1 ½ years later than
the average.
(Brock, 2009; Durand, 2014; Mandall, etal, 2002;Wilkinson, 2009)
Semantics Matters: Eligibility &
Diagnosis
Eligibility Diagnosis
Educational Educational Eligibility Diagnosis
Educational Clinical Evaluations Evaluations
When we try to equate these things we confuse ourselves and confuse families. This causes problems
for everyone.
Federal: IDEA 2004
(i) Autism means a developmental disability
significantly affecting verbal and nonverbal
communication and social interaction, generally evident before age three that adversely affects a
child's educational performance.
Other characteristics often associated with autism are engagement in repetitive activities and
stereotyped movements, resistance to
environmental change or change in daily routines, and unusual responses to sensory experiences.
California Code of Regs
Autism means a developmental disability significantly
affecting verbal and nonverbal communication and
social interaction; generally evident before age three
that adversely affects a student's educational
performance. Other characteristics often associated
with autism are engagement in repetitive activities and
stereotyped movements, resistance to environmental
change or change in daily routines, and unusual
responses to sensory experiences. The term does not
apply if a student's educational performance is
adversely affected primarily because the student has
an emotional disturbance. A student who manifests the
characteristics of autism after age three could be
identified as having autism if the criteria are satisfied.
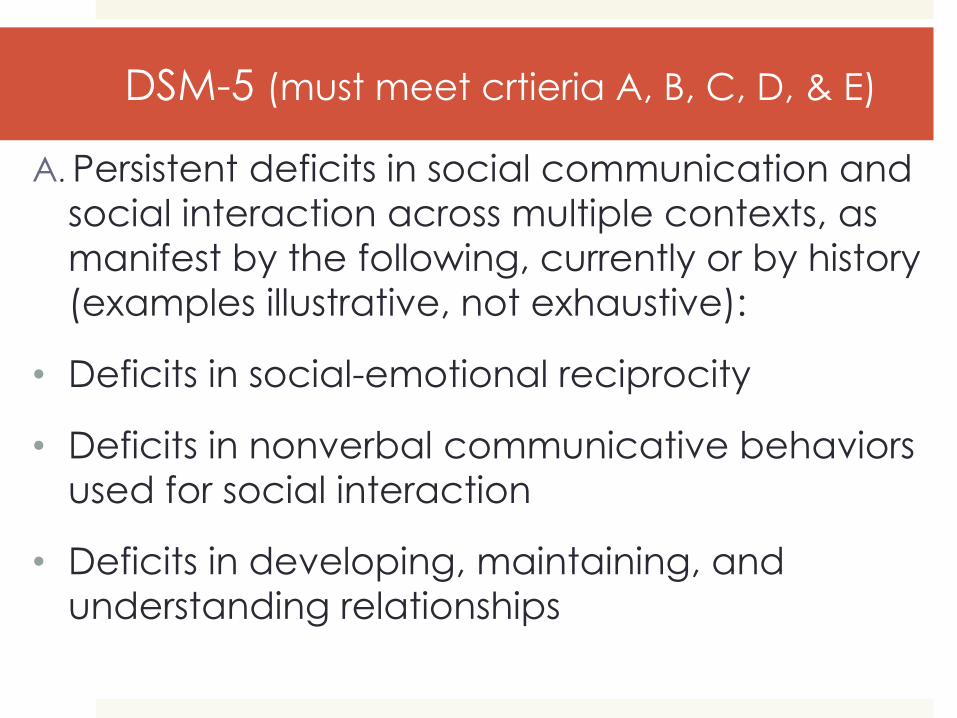
DSM-5 (must meet crtieria A, B, C, D, & E)
A. Persistent deficits in social communication and
social interaction across multiple contexts, as
manifest by the following, currently or by history
(examples illustrative, not exhaustive):
• Deficits in social-emotional reciprocity
• Deficits in nonverbal communicative behaviors
used for social interaction
• Deficits in developing, maintaining, and
understanding relationships
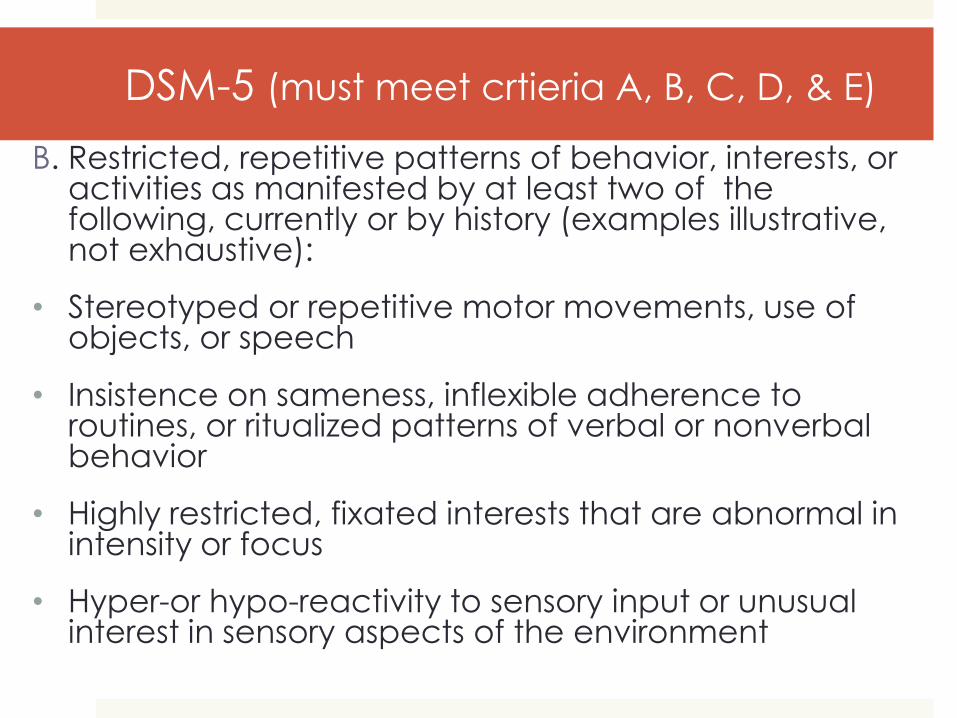
DSM-5 (must meet crtieria A, B, C, D, & E)
B. Restricted, repetitive patterns of behavior, interests, or activities as manifested by at least two of the following, currently or by history (examples illustrative, not exhaustive):
• Stereotyped or repetitive motor movements, use of objects, or speech
• Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior
• Highly restricted, fixated interests that are abnormal in intensity or focus
• Hyper-or hypo-reactivity to sensory input or unusual interest in sensory aspects of the environment
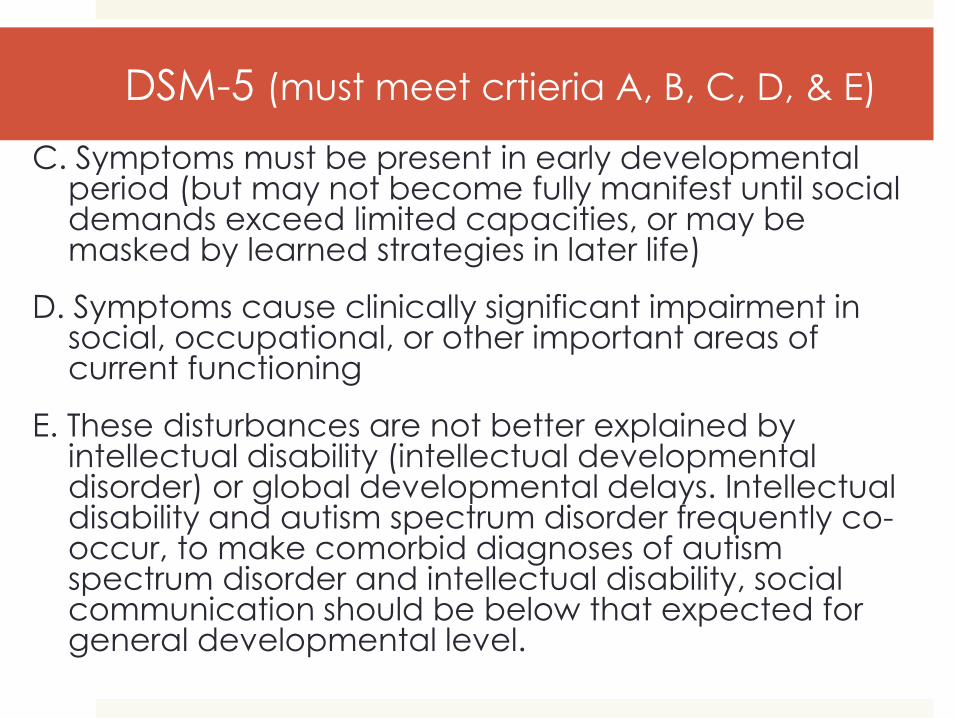
DSM-5 (must meet crtieria A, B, C, D, & E)
C. Symptoms must be present in early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life)
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delays. Intellectual disability and autism spectrum disorder frequently co-occur, to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
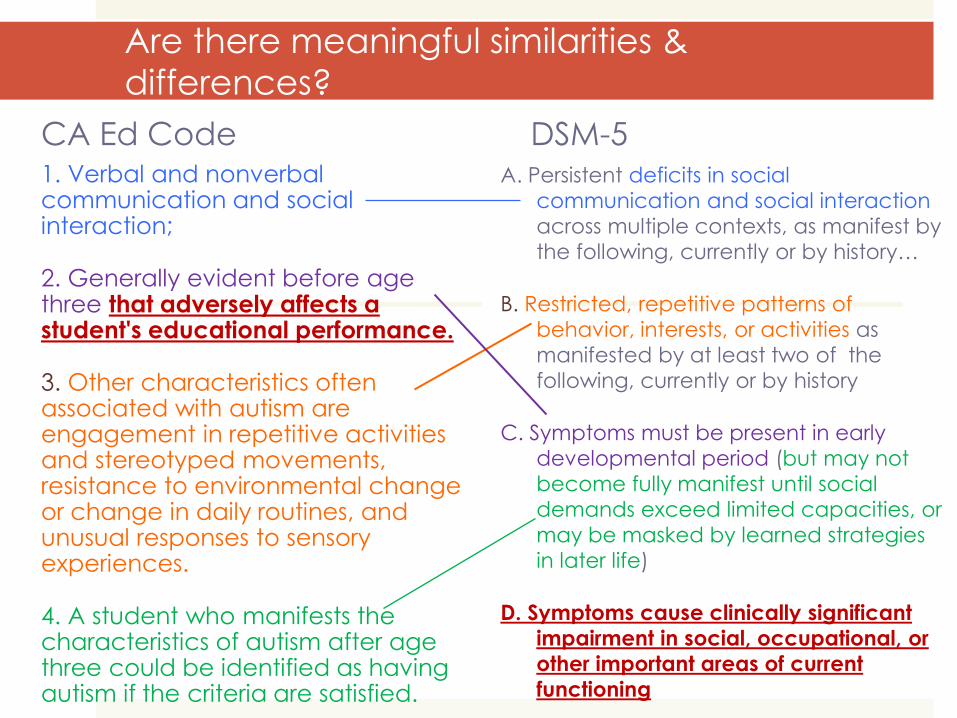
Are there meaningful similarities & differences?
CA Ed Code 1. Verbal and nonverbal communication and social interaction;
2. Generally evident before age three that adversely affects a student's educational performance.
3. Other characteristics often associated with autism are engagement in repetitive activities and stereotyped movements, resistance to environmental change or change in daily routines, and unusual responses to sensory experiences.
4. A student who manifests the characteristics of autism after age three could be identified as having autism if the criteria are satisfied.
DSM-5 A. Persistent deficits in social
communication and social interaction
across multiple contexts, as manifest by
the following, currently or by history…
B. Restricted, repetitive patterns of
behavior, interests, or activities as
manifested by at least two of the
following, currently or by history
C. Symptoms must be present in early
developmental period (but may not
become fully manifest until social
demands exceed limited capacities, or
may be masked by learned strategies
in later life)
D. Symptoms cause clinically significant
impairment in social, occupational, or
other important areas of current
functioning
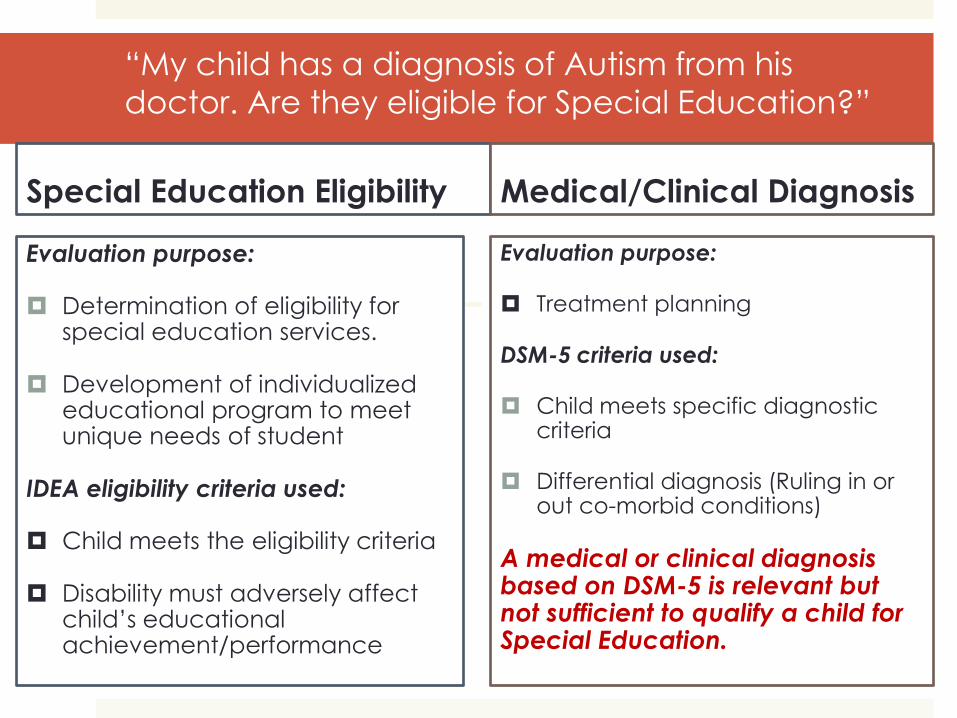
“My child has a diagnosis of Autism from his
doctor. Are they eligible for Special Education?”
Special Education Eligibility
Evaluation purpose:
Determination of eligibility for special education services.
Development of individualized educational program to meet unique needs of student
IDEA eligibility criteria used:
Child meets the eligibility criteria
Disability must adversely affect child’s educational achievement/performance
Medical/Clinical Diagnosis
Evaluation purpose:
Treatment planning
DSM-5 criteria used:
Child meets specific diagnostic criteria
Differential diagnosis (Ruling in or out co-morbid conditions)
A medical or clinical diagnosis based on DSM-5 is relevant but not sufficient to qualify a child for Special Education.
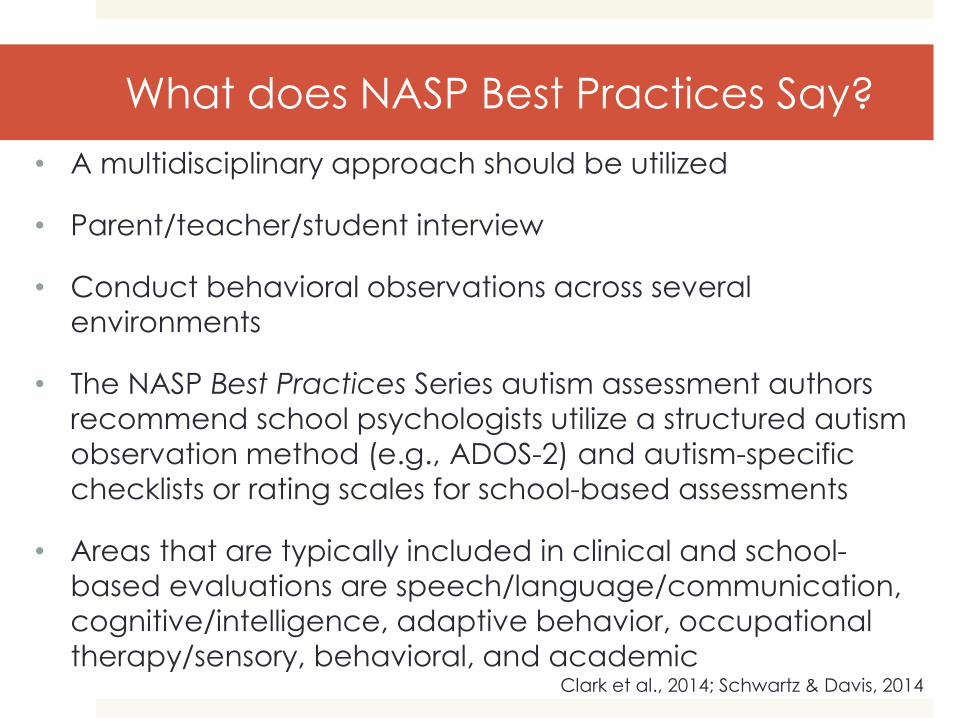
What does NASP Best Practices Say?
• A multidisciplinary approach should be utilized
• Parent/teacher/student interview
• Conduct behavioral observations across several
environments
• The NASP Best Practices Series autism assessment authors
recommend school psychologists utilize a structured autism
observation method (e.g., ADOS-2) and autism-specific
checklists or rating scales for school-based assessments
• Areas that are typically included in clinical and school-
based evaluations are speech/language/communication,
cognitive/intelligence, adaptive behavior, occupational
therapy/sensory, behavioral, and academic Clark et al., 2014; Schwartz & Davis, 2014
Survey of Current Practices on
School-Based Autism Assessments
Survey Contents
Consisted of 50 questions- 49 close-ended
questions and 1 open-ended question
Created based on the NASP Best Practice
series guidelines on autism assessments,
California Code of Regulations for the autism
eligibility criteria, California Statutes
Education Code for assessment reports, and
general impressions/practices of school-
based autism assessments
Data Collection Procedures
Emails were sent to CASP members from July
to August 2016
The survey was on the CASP website for 7
weeks
A total of 7 emails were sent to CASP
members to ask them to complete the survey
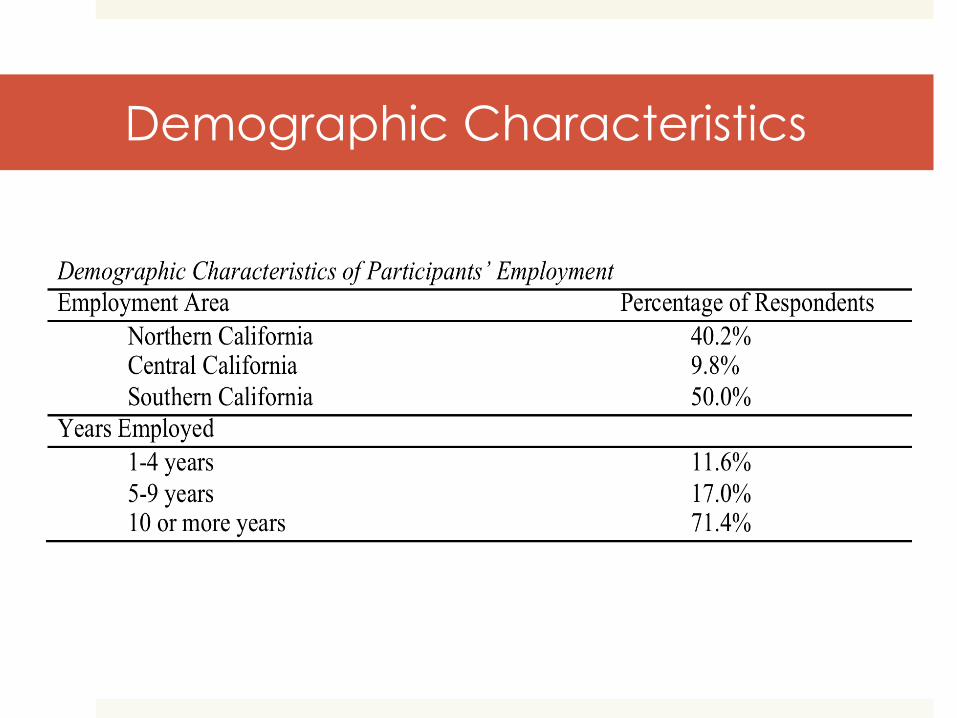
Demographic Characteristics
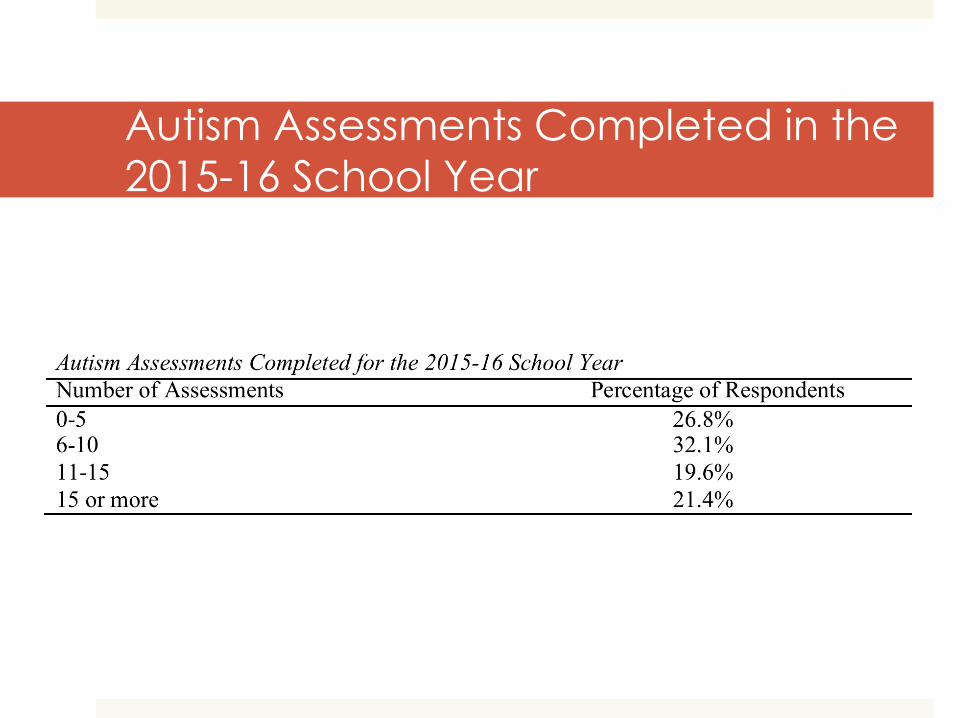
Autism Assessments Completed in the
2015-16 School Year
Current Assessment Practices for CA School
Psychs
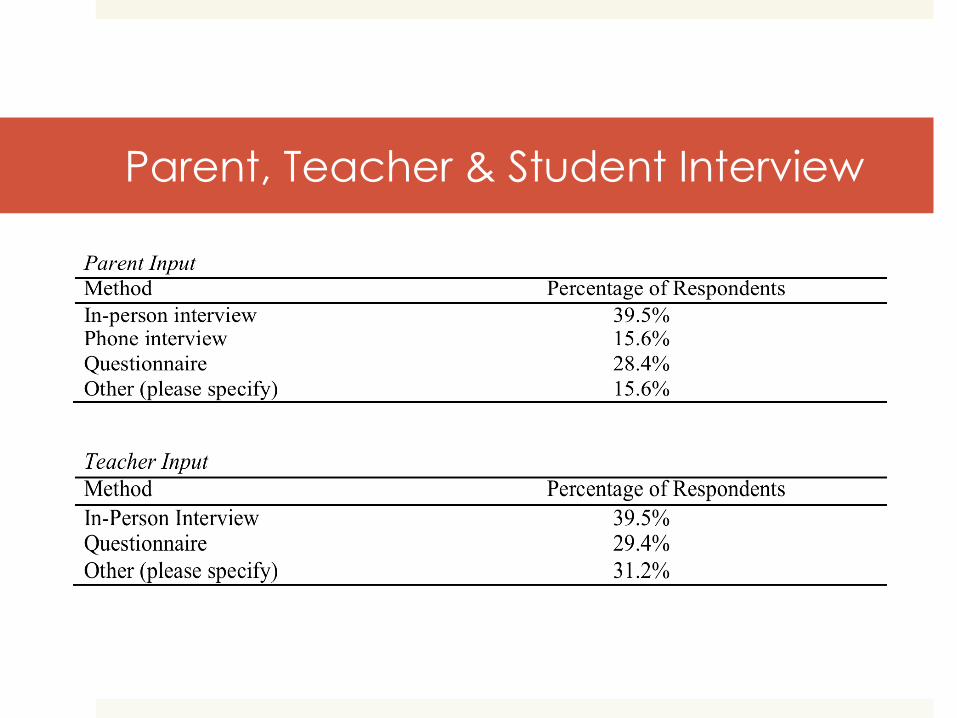
Parent, Teacher & Student Interview
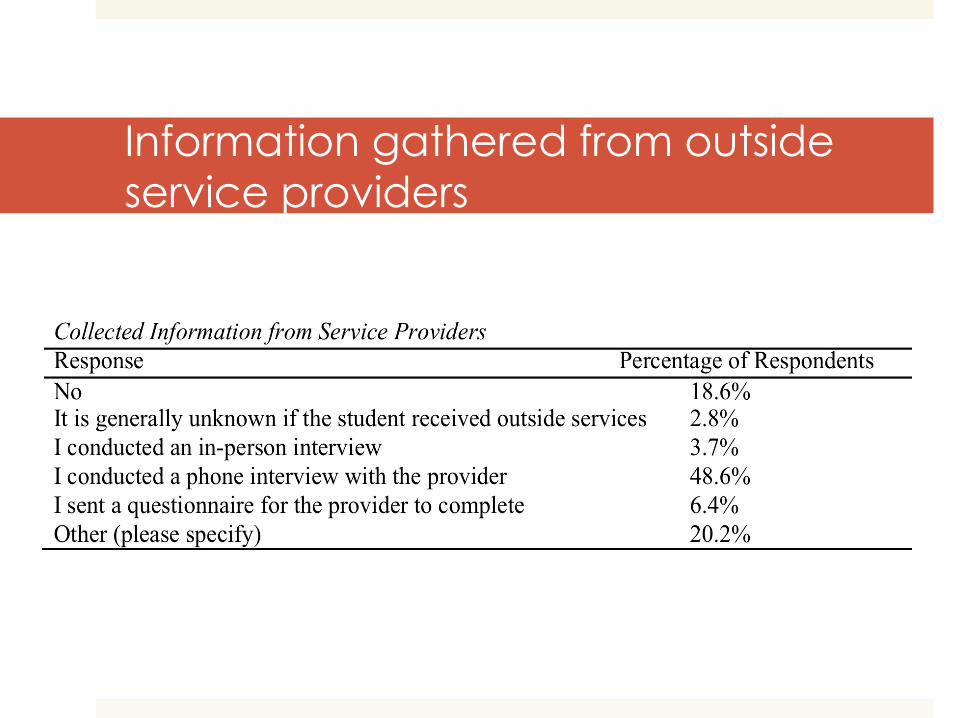
Information gathered from outside
service providers
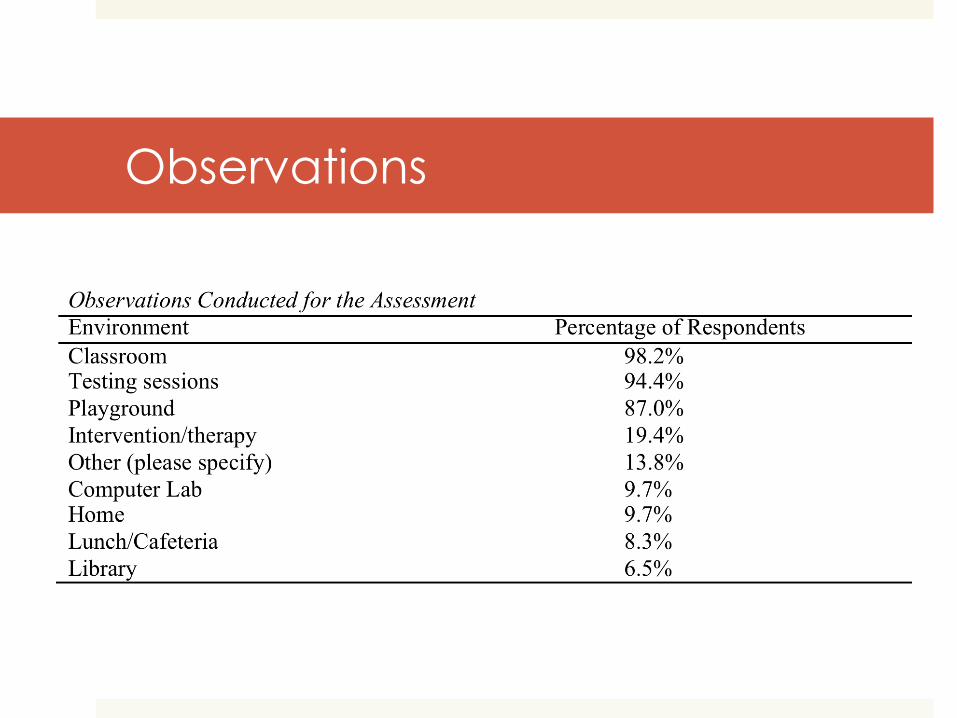
Observations
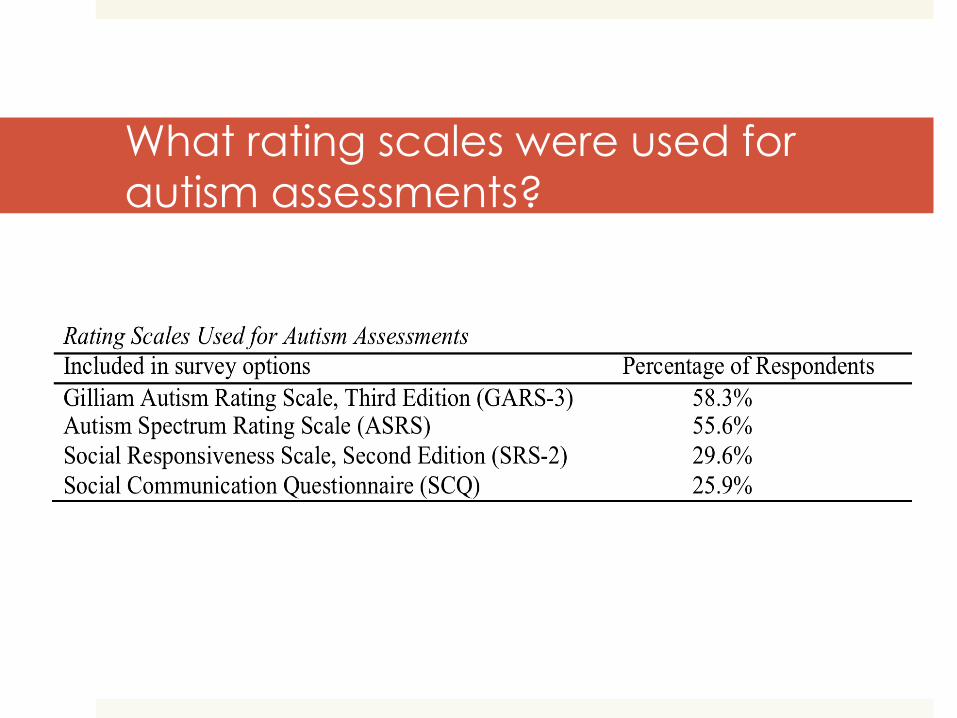
What rating scales were used for
autism assessments?
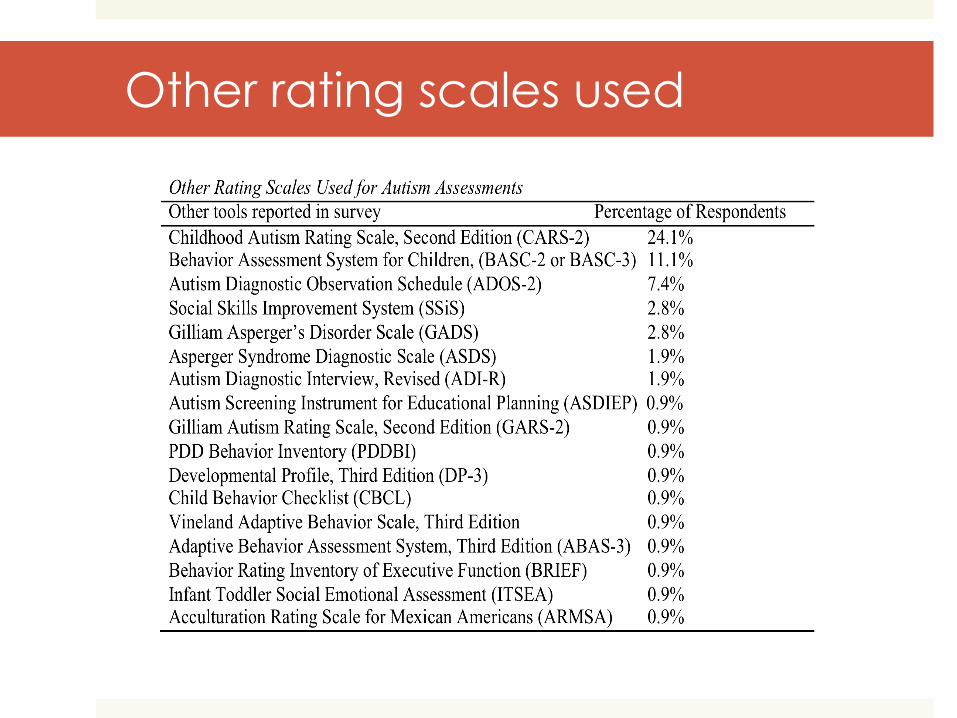
Other rating scales used
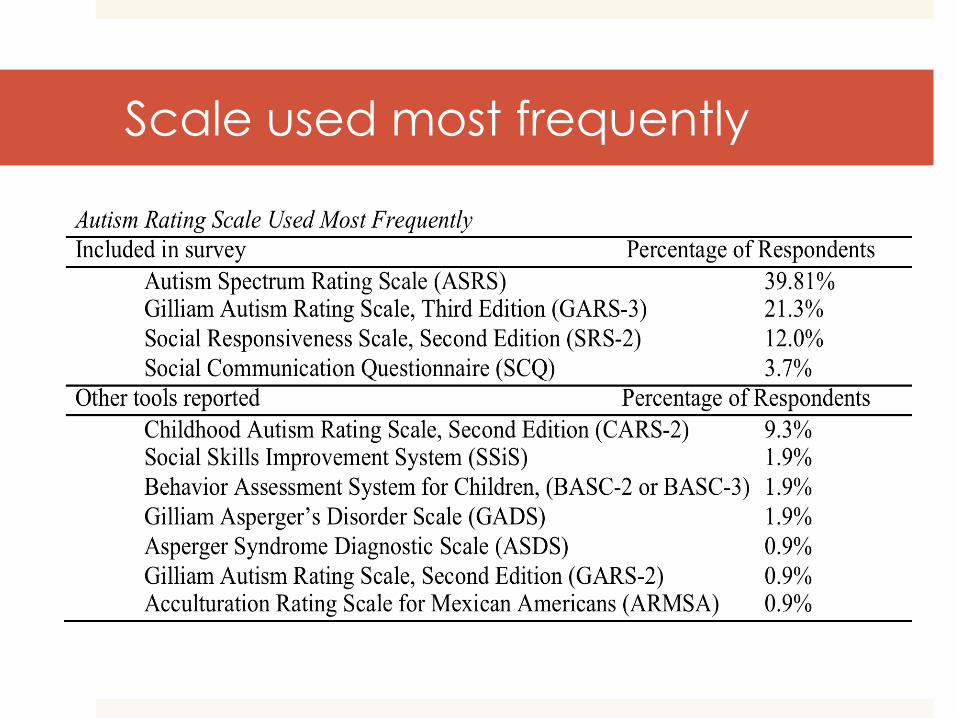
Scale used most frequently
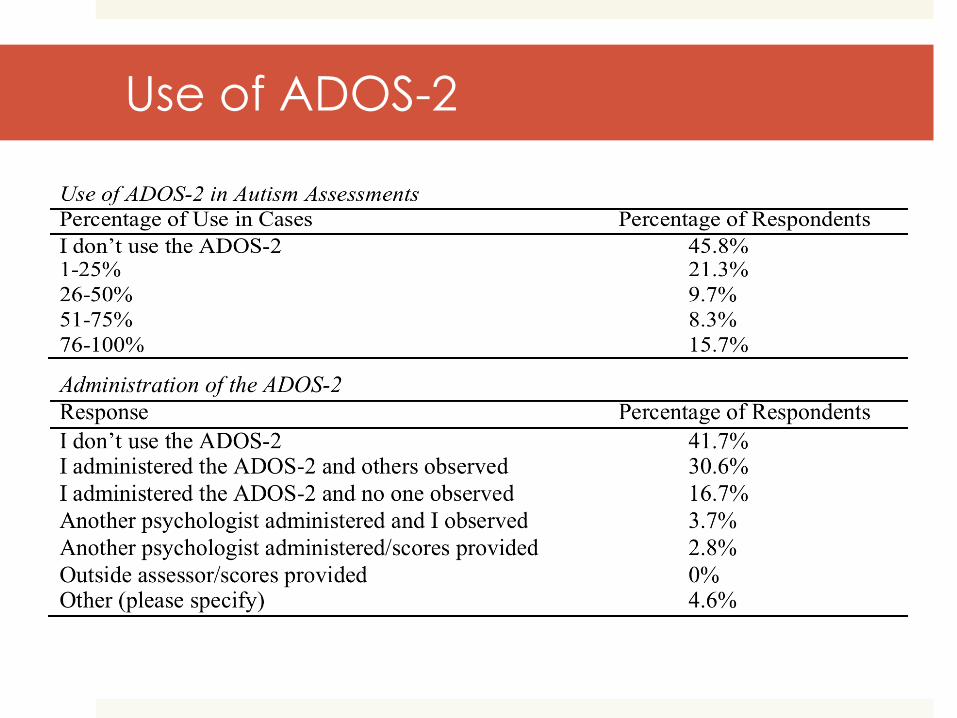
Use of ADOS-2
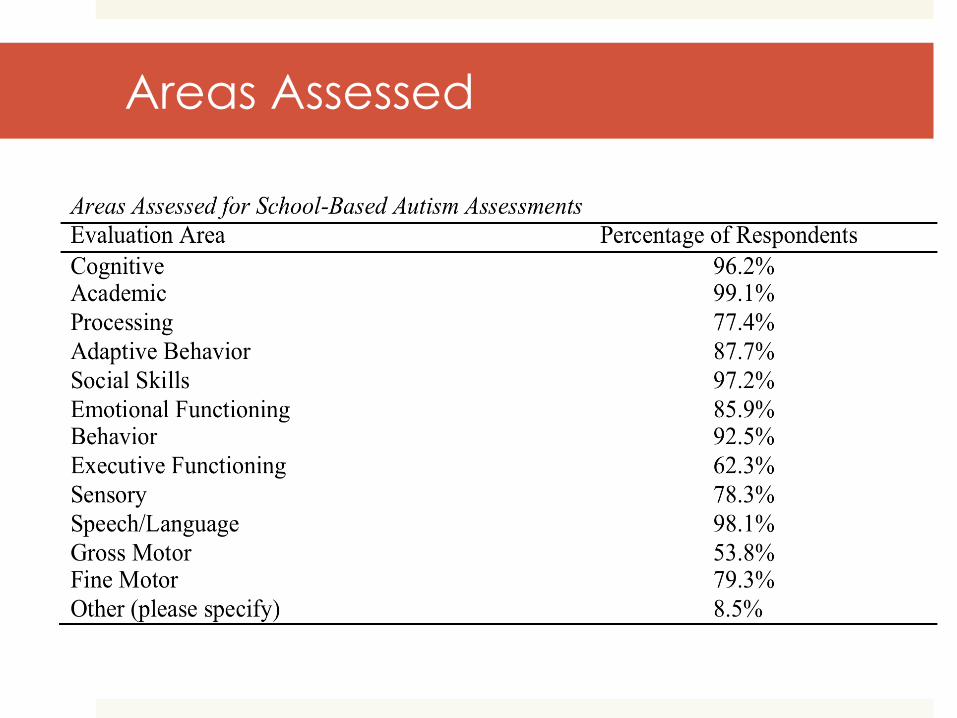
Areas Assessed
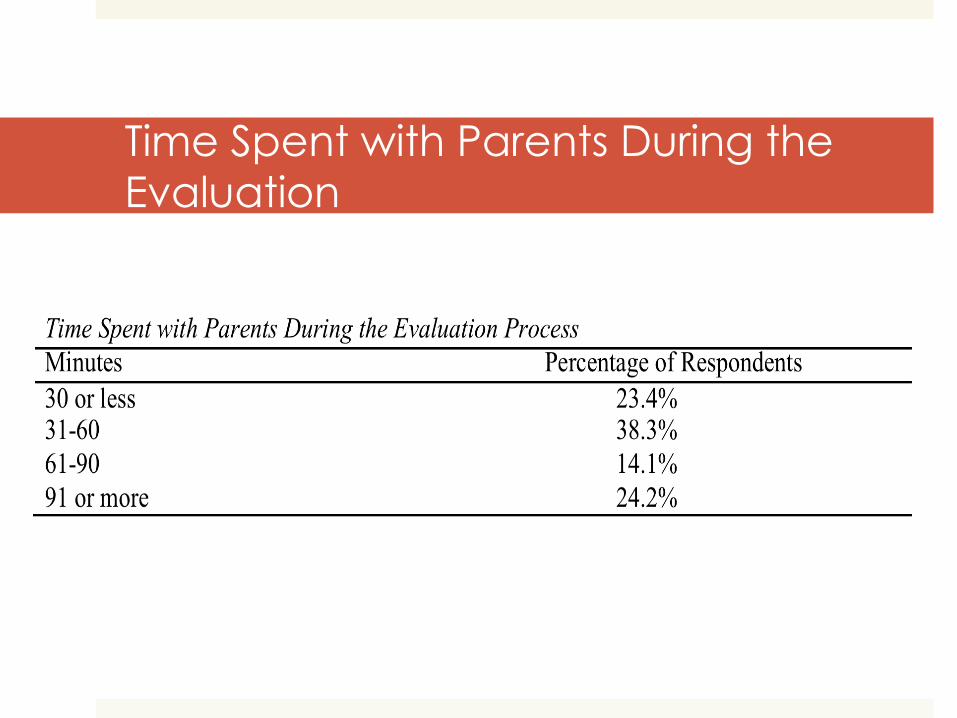
Time Spent with Parents During the
Evaluation
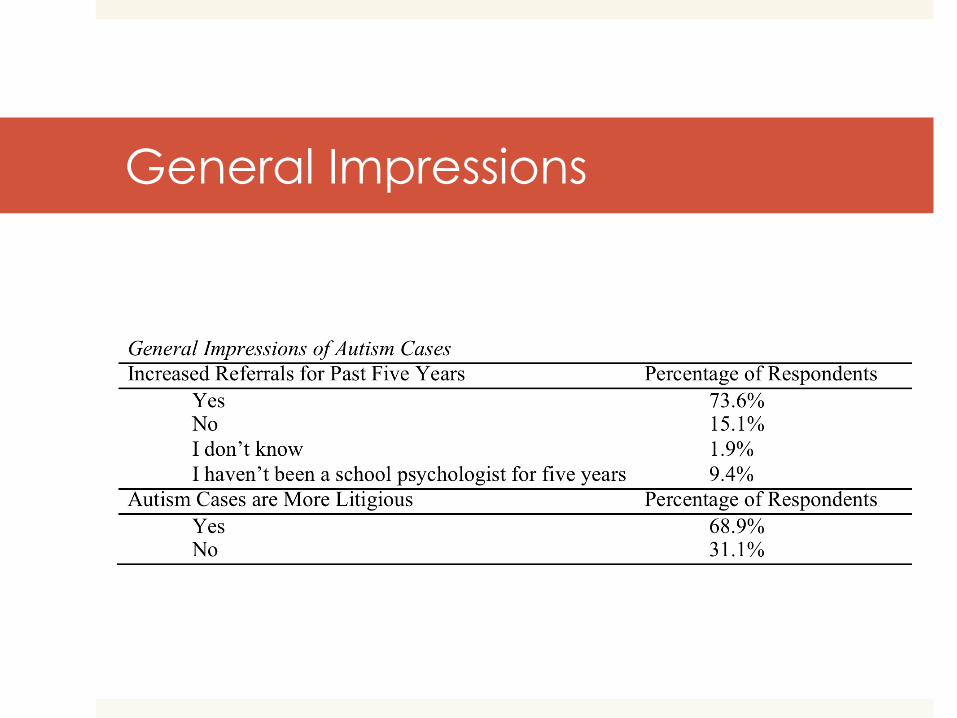
General Impressions
Litigious Reasons for ASD cases
amount of services requested by
parent/advocate/attorney;
factors regarding the district (perception,
relationship, and resources);
factors regarding parents (resources, education
level, grieving, understanding their rights/laws);
outside agencies/professionals advocating for
services deemed inappropriate per school district;
adequacy of autism assessments.

Legal Trends/Case Law
OAH Case Search
July 1, 2005-July 20, 2016
Search terms:
Autism
Assessment
Best Practice
A total of 233 cases were found
10 cases met the criteria- issues regarding the appropriateness of the psych eval
80% of the cases met the legal requirements
Discussion
Considering the litigious reasons for ASD cases, discuss
the follow questions with the person(s) seated next to
you:
1. Did all of the cases include a parent interview?
2. How about the ADOS?
3. Was adaptive behavior assessed in each case?
Themes of OAH Cases
Best Practices Terminology
School Psychologist’s Training and Expertise
Inadequate Assessments
“Best Practices”
Each case had a expert witness that discussed “best
practices”
Some judges sided with these “best practices”
recommendations and stated “not adhering to best
practice did not render the psychoeducational
assessment as legally noncompliant” but other
judges decided the case was inadequate if the
psychologist did not follow “best practice”
recommendations
School Psych’s Training & Experience
In the cases reviewed, the school psychologist’s
training and experience in administering autism-
specific measures (i.e., ADOS-2) was challenged in
two OAH cases
Both psychs did not attend the ADOS-2 workshop
ALJ deemed they were qualified to administer the
ADOS-2
Not Recommended
Inadequate Assessments
Two cases that found assessment inadequate:
1. The school psychologist did not adhere to best
practice assessments per the testimony of a
clinical psychologist
2. The school psychologist incorrectly used a
rating scale and used terminology not
included in the autism eligibility criteria when
determining if a student qualified for special
education services
Conduction Comprehensive
Assessments
We are evaluating… “A singular presentation of a global disorder”
Marilyn J. Monteiro, PhD Autism Conversations, 2013
A Comprehensive Assessment, according to IDEA, CA Education Code, NASP & APA Ethical Guidelines
1. Assessment tools are chosen and used so that they are not
racially, sexually, or culturally discriminatory.
2. Assessments must be conducted in the language and form most
likely to yield accurate information on what the student knows and can do academically, developmentally and functionally unless
the assessment plan indicates why it is not feasible to provide or
administer.
3. For students with Limited English Proficiency the assessment instruments are selected and administered in a manner that
ensures that the assessment measures what is intended rather than
the student’s English language skills.
4. For students with sensory, motor, or speaking impairments the assessment instruments are selected and administered in a
manner that ensures the assessment measures what is intended
rather than the student’s sensory, motor, or speaking skills.
A comprehensive assessment
continued… 5. Assessment tools and strategies are selected to provide information
on the student’s specific areas of educational need.
6. Assessment instruments are reliable and have been validated for the purposes for which they are going to be used.
7. Assessments are only conducted by qualified professionals.
8. No single measure or assessment is used as the sole criterion for determining whether a student has a disability. The assessment covers all areas related to the student’s suspected disability and all areas of need.
9. A variety of assessment tools and strategies should be used to gather relevant functional and developmental information about a child.
10. Assessment results should be provided in written language that is understood by the consumer.
11. Reports should emphasize meaning and make recommendations that help the readers in their work with children
In summary…
The evaluation should…
• be comprehensive
• use a variety of evaluation tools or approaches that gather functional and relevant data
• be fair
• use valid and reliable tools and procedures
• be completed by a competent evaluator
• be written into a report that is useful and understandable
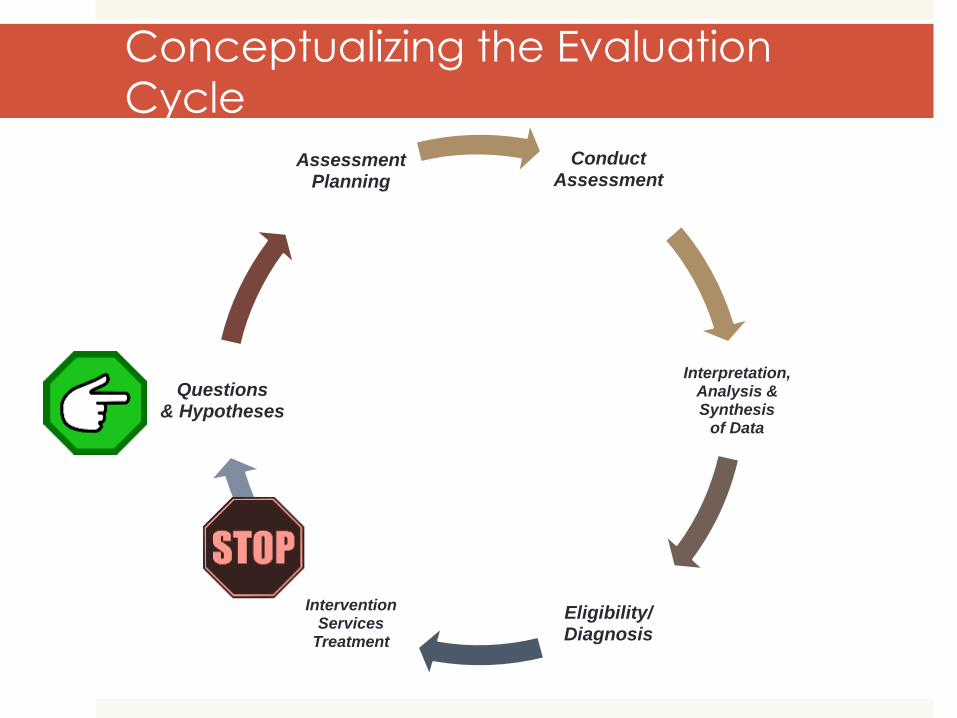
Conceptualizing the Evaluation
Cycle
Conduct Assessment
Interpretation, Analysis & Synthesis
of Data
Eligibility/ Diagnosis
Intervention Services
Treatment
Questions & Hypotheses
Assessment Planning
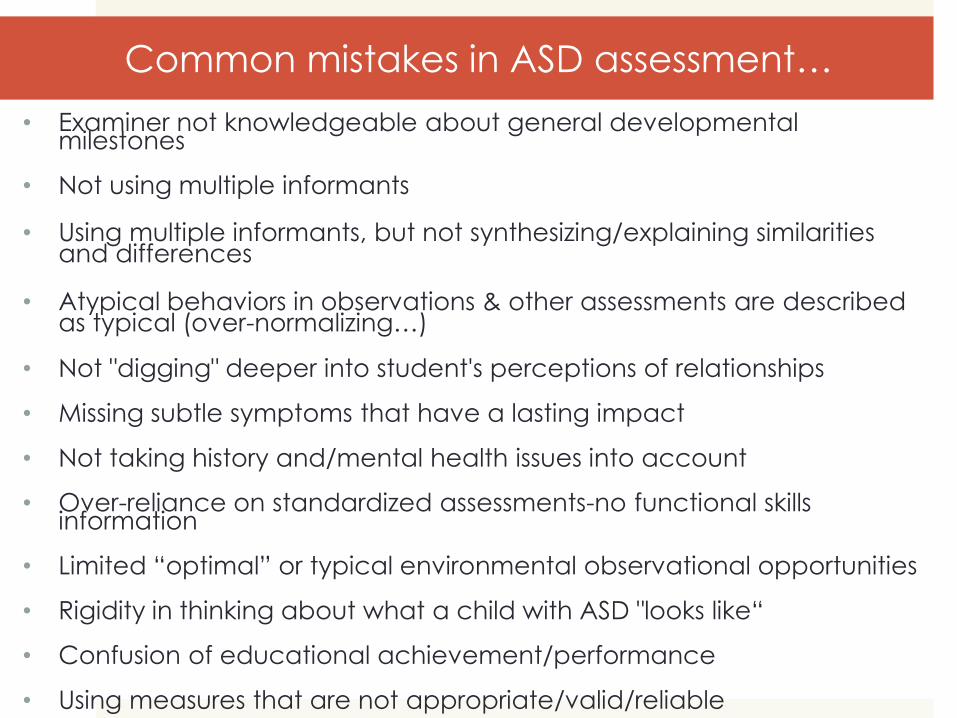
Common mistakes in ASD assessment…
• Examiner not knowledgeable about general developmental milestones
• Not using multiple informants
• Using multiple informants, but not synthesizing/explaining similarities and differences
• Atypical behaviors in observations & other assessments are described as typical (over-normalizing…)
• Not "digging" deeper into student's perceptions of relationships
• Missing subtle symptoms that have a lasting impact
• Not taking history and/mental health issues into account
• Over-reliance on standardized assessments-no functional skills information
• Limited “optimal” or typical environmental observational opportunities
• Rigidity in thinking about what a child with ASD "looks like“
• Confusion of educational achievement/performance
• Using measures that are not appropriate/valid/reliable
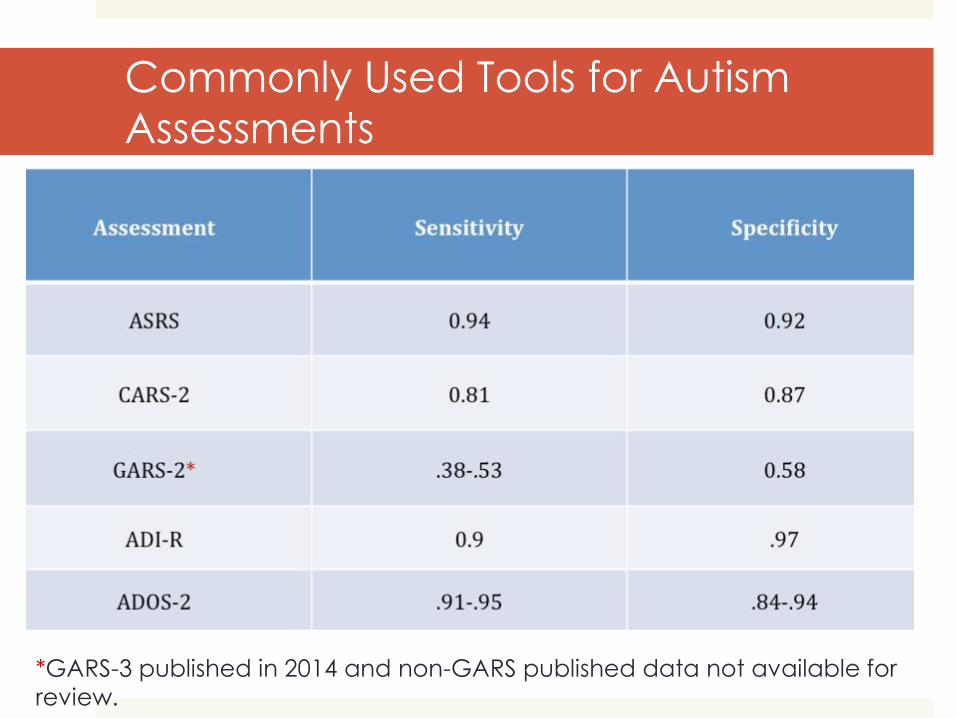
Commonly Used Tools for Autism
Assessments
*GARS-3 published in 2014 and non-GARS published data not available for
review.
Working
Collaboratively to
create a
Comprehensive
Autism
Assessment
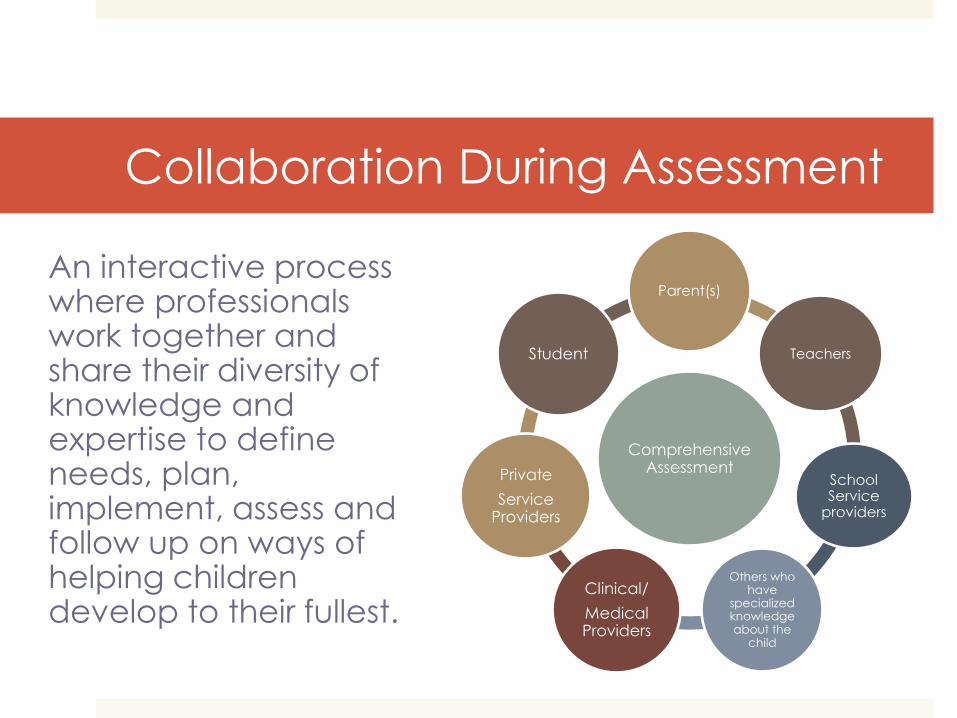
Collaboration During Assessment
An interactive process where professionals work together and share their diversity of knowledge and expertise to define needs, plan, implement, assess and follow up on ways of helping children develop to their fullest.
Comprehensive Assessment
Parent(s)
Teachers
School Service
providers
Others who have
specialized knowledge about the
child
Clinical/
Medical Providers
Private
Service Providers
Student
Assessment Planning
When reviewing records and making initial contact with families and teachers where ASD is a concern, ask yourself:
• What is the specific referral concern? (i.e., social interaction, cognition, behavior, language development)?
• Developmentally, what are the signs associated with ASD?
• If previous evaluations have been completed, are the findings valid and or useable?
• What eligibilities/diagnoses best explain the student’s profile?
• What additional information is needed to determine the student’s disabilities?
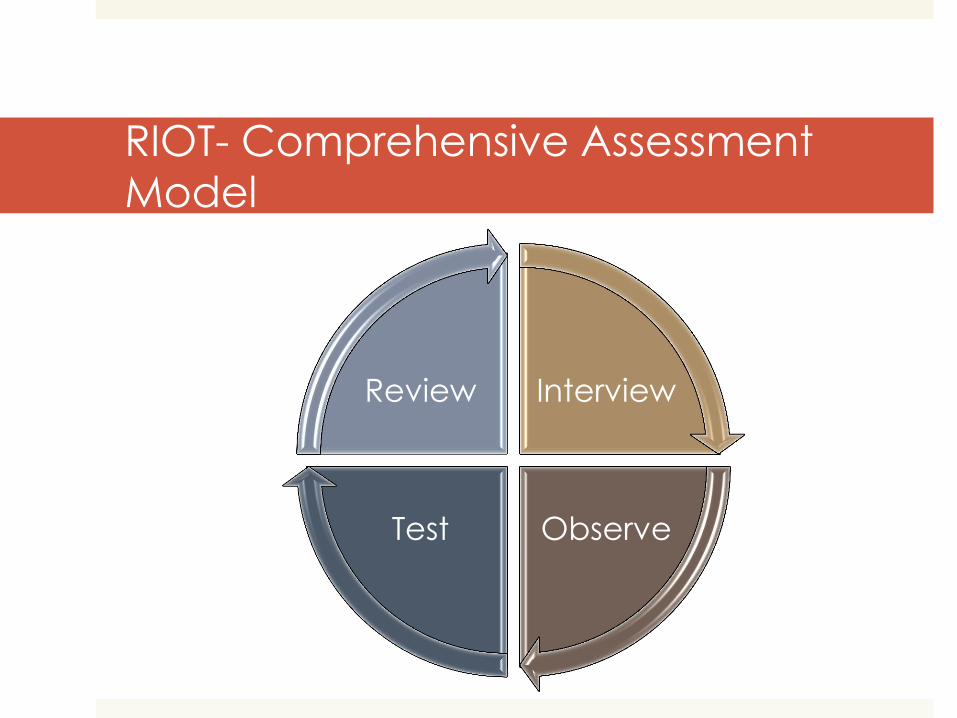
RIOT- Comprehensive Assessment
Model
Interview
Observe Test
Review
RIOT: Review
Review: Preschool Records, School Cumulative Files &
Health File, Prior Assessments, Outside Assessments
and Treatment Summaries
• Signs of behavior patterns present in early childhood
• History of social communication/interaction deficits,
• Signs of other risk factors (e.g., siblings with autism,
other family members with autism)
• Potential complicating factors
Developmental Milestones Resources
CDC Birth to 5 milestones, videos, concern,
Autism case training for professionals
http://www.cdc.gov/ncbddd/actearly/index.
html
CDC Autism signs and symptoms
http://www.cdc.gov/ncbddd/autism/facts.html
RIOT: Interview
Child
ability to warm to interviewer and socially connect
eye-contact, voice, restricted reciprocal interactions
social experiences
Parents
structured developmental histories or more formalized questionnaires
history of restricted/ repetitive behaviors and social communication in early years
structured and semi-structured clinical interview format
functional skills in the community and at home
Teachers
social communication
self-advocacy/initiation behavior
patterns of restricted interests and/or repetitive behaviors
classroom adaptive skills
academic achievement and performance
Parent input is crucial!
Use both informal & structured interviews to gather information about…
Detailed developmental history
Current adaptive functioning
Behavioral concerns
Communication delays and concerns
Friendships/Social skills
Parent Interview: Open Ended ?
Examples… • What are your concerns? When did you first become concerned?
• How did your child’s development differ from that of his siblings?
• How does he let you know when he needs something? How did he let you know when he first started communicating?
• Tell me about his imitation skills; does he spontaneously copy what you do or do you have to teach him? When did he begin imitating you? How did this look?
• What are his interests? What are his favorite toys and games?
• Describe what he did/does with toys and how he played/plays? (Probe for pretend, sequencing, variety, interactions with dolls, animal or action figures)
• When and how does he interact with others?
• How does he get along with his siblings?
Parent Interview Questions Cont.
• Tell me about his friendships and interest in other kids? How does he play with other kids?
• What does he look like at the park or recess? How does he respond when other children approach or invite him to play?
• How does he communicate his feelings to you and others? How does he respond to others when they are sad or upset?
• Describe any sensitivities (sound, touch, texture, food) and lack of sensitivity (pain, temperature).
• How does he respond to changes in routines and schedules?
• Are there any things he seems to have to do in a particular way or order?
• What motivates him/her? What do you enjoy doing together?
• What are his/her strengths? Special skills?
Teacher input is crucial!
• Strengths/concerns
• Behavioral concerns
• Communication delays and concerns
• Friendships/Social skills (classroom and recess)
• Attention
• Transitions between activities
• Understanding abstract concerns (reading comp, Common core math)
• Generalizing skills and concepts
• Performing upon request
• Motivation to perform
• Classroom adaptive skills
• Problem solving skills
• Fine motor, writing, and drawing skills
“Interview”: Rating Scales
Adaptive
Individuals with ASD have adaptive skill deficits
Comprehensive Examples: Vineland-3, Adaptive Behavior
Assessment Scale (ABAS-3)
Social Communication and Skills
Development
Examples: Social Communication Questionnaire-Current or
Lifetime (SCQ), Social Responsiveness Scale-2 (SRS-2), Social Skills Improvement System (SSIS)
“Interview”: Rating Scales cont…
Behavior and Social Emotional Functioning
• We are evaluating for behavioral difficulties and social skills
though poor emotional regulation, limited coping strategies, self
awareness, insight, ability to attend to others’ reactions /
preferences, and flexibility may also impact overall mental
health
• Broad Band Examples: Behavior Assessment System for Children-
3 (BASC-3), Child Behavior Checklist (CBCL), Social Skills
Improvement System (SSIS), Beck Youth Inventories-2 (BYI-2)
• Singular Examples: Multidimensional Anxiety Scale for Children
(MASC)
RIOT: Observations
• General:
• Observe the child in multiple settings over
multiple days:
• arrival and departure, transitions, structured
and unstructured activities, and
classroom/non-classroom settings, with adults
and peers
• Where are there problems? Why?
• Where is the child successful? Why?
Example: Observations
Social Interaction &
Communication • Ability to initiate and sustain social
interactions (reciprocal communication)
• Failure to initiate or respond
• Poorly integrated verbal and nonverbal communication
• Abnormalities in eye contact (too much or too little)
• Ability to express/read emotions
• Tone of voice
• Difficulty with idioms or pragmatic language
• One-sided conversation patterns
• “Directing” play
Behavior Patterns
• Selected interests
• Need for
routines/sameness
• Difficulty with transitions
• Fine and/or gross motor
difficulties
• Stereotypical behaviors:
flapping, rocking,
posturing, etc.
• Other sensory seeking or
stimulating behaviors
Informal (On your own…) Formal (Published)
Anecdotal/Naturalistic
Time Sampling
Event/Frequency
Recording
Environmental/Setting
BASC-2, Structured Observation System
Behavior Observation of Students in School (BOSS)
Childhood Autism Rating Scales-2 (CARS-2)
Autism Diagnostic Observation Schedule-2 (ADOS-2)
Systematic Direct Observations
Structured Observations:
The ADOS-2 ?
Why Use It?
Psychometrically strong
Pulls for ASD-specific
behaviors
Creates context to observe
diagnostic behaviors
Takes into account
expressive language level
and age of child
Yields rich clinical data
(qualitative & quantitative)
Cautions
Requires extensive training
Requires practice and
routine use
Scores based on behavior
exhibited during
administration only
Results in classification, not diagnosis
Use of an incorrect module
can result in over or under
classification
RIOT: Test
Standardized assessment tools alone will not be sufficient in diagnosing or assessing fully
for ASD.
Don't neglect the RIO!
After Review-Interview-Observe (RIO),
determine:
• What areas need to be directly assessed or test?
• How much formal/standardized testing is needed?
• How do we maximize the overall evaluations validity?
BUT…
STUDENTS WITH ASD TEND TO HAVE DIFFICULTY WITH ESSENTIAL TEST
TAKING BEHAVIORS:
Attention span
Response on demand
Imitation
Motivation
Desire to please
Assessment support tools and
strategies
• Give Choices
• Visual Schedule
• Sticky Pads
• White Boards
• Timer
• Tally Marks
• First-Then cards
• Reinforcers/Sticker Charts
• Game/Play/Movement Breaks
Cognitive Assessment Selection
• All instruments are not created equally
• Choose a test that taps into the child’s current abilities
and developmental level
• Measure both verbal and nonverbal skills
• Look at the pattern of strengths and weaknesses
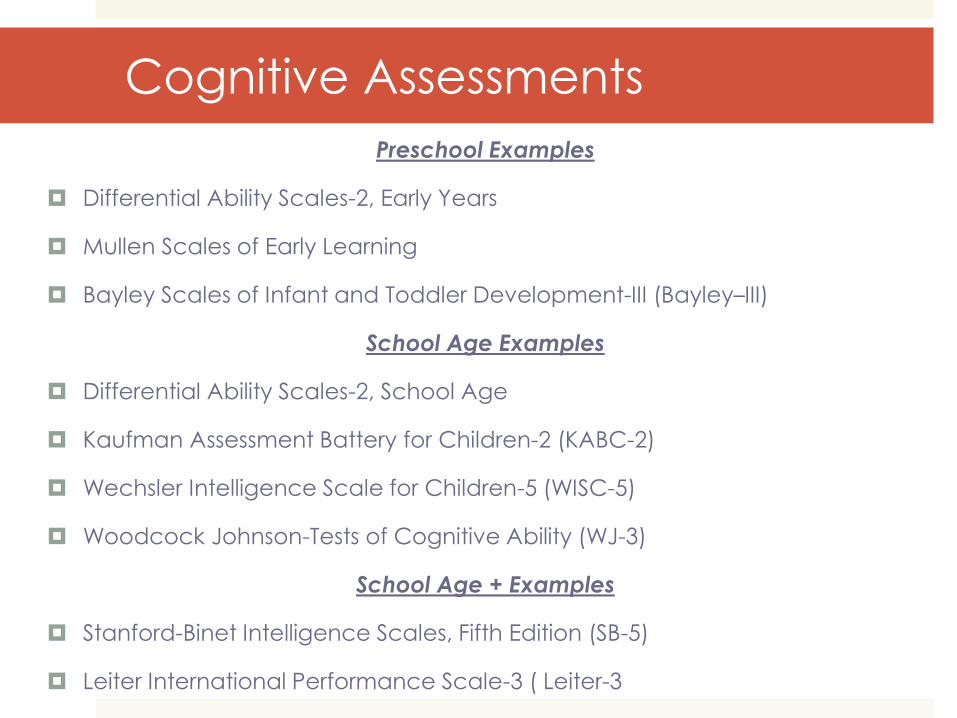
Cognitive Assessments
Preschool Examples
Differential Ability Scales-2, Early Years
Mullen Scales of Early Learning
Bayley Scales of Infant and Toddler Development-III (Bayley–III)
School Age Examples
Differential Ability Scales-2, School Age
Kaufman Assessment Battery for Children-2 (KABC-2)
Wechsler Intelligence Scale for Children-5 (WISC-5)
Woodcock Johnson-Tests of Cognitive Ability (WJ-3)
School Age + Examples
Stanford-Binet Intelligence Scales, Fifth Edition (SB-5)
Leiter International Performance Scale-3 ( Leiter-3
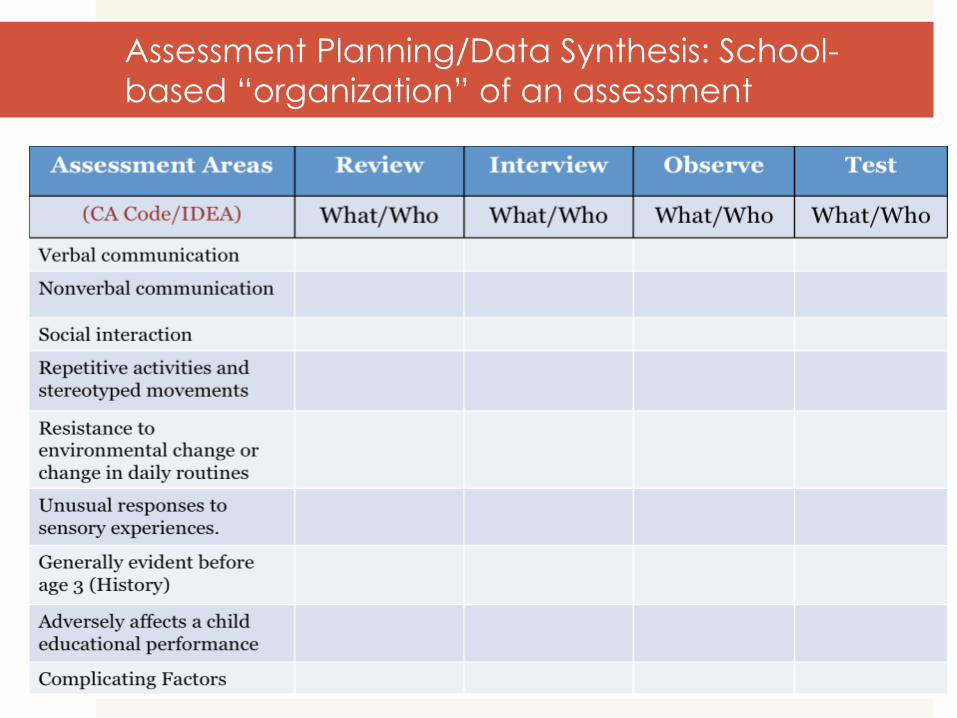
Assessment Planning/Data Synthesis: School-
based “organization” of an assessment
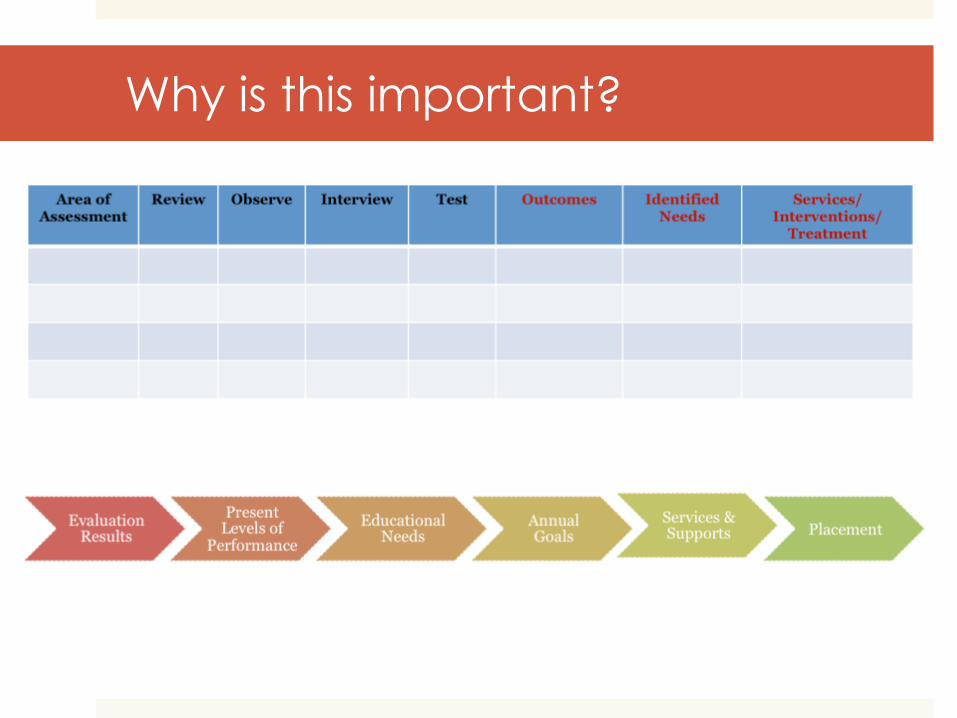
Why is this important?
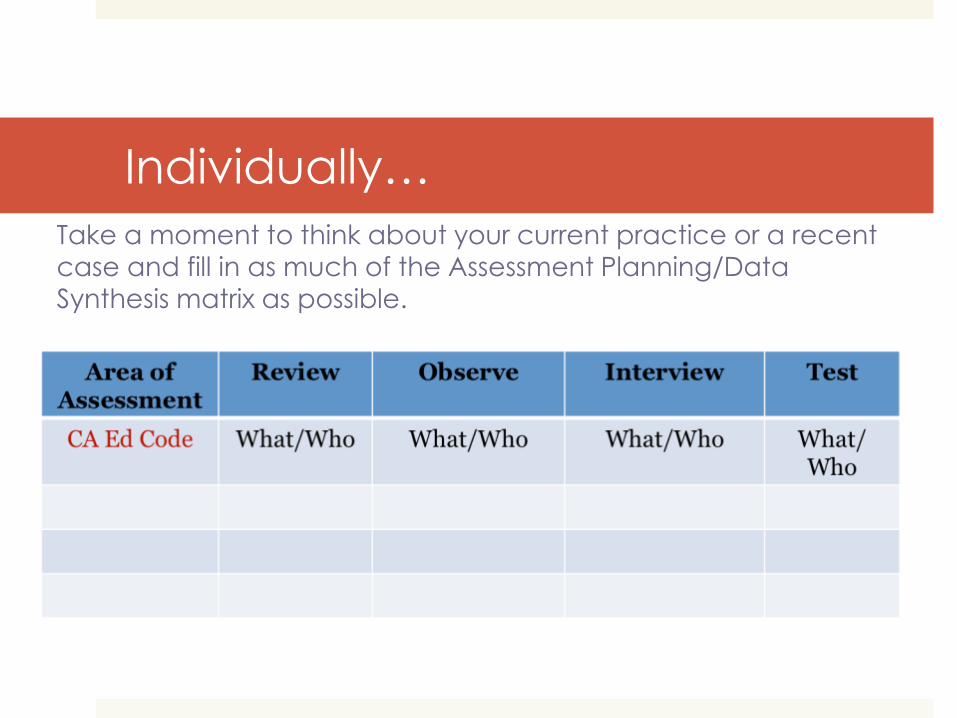
Individually…
Take a moment to think about your current practice or a recent
case and fill in as much of the Assessment Planning/Data
Synthesis matrix as possible.
In small groups, discuss…
What does your assessment of
autism look like?
What are you doing to support
a comprehensive assessment?
Model (Planning tool)?
Convergent data?
Multiple sources/informants?
Is data relevant and
functional?
Supports
intervention/treatment
planning?
What steps or changes can
you make toward a more
comprehensive
evaluations?
What will you take back to
your school, team, and
colleagues?

Questions, comments, concerns?
Angela Davis [email protected]
Jeanne Anne Carriere [email protected]
Kelly Kennedy [email protected]