Embed Size (px)
Citation preview
School of MedicineDepartment of Medicine
Division of General Internal Medicine and Geriatrics
IU Center forAging Research
Noll Campbell, PharmD, FASCP, BCPP
Mick Murray, PharmD, MPH
Malaz Boustani, MD, MPH
Sujuan Gao, PhD
Medication Management in Older Adults with Cognitive Impairment
IU Geriatrics
Objectives
• Identify current evidence regarding medication adherence in older adults with cognitive impairment
• Discuss possible solutions to the problem of medication adherence in cognitive impairment
IU Geriatrics
The Problem: Case of Mrs. C
• 87 yo AA female with H/O CHF, CAD, CKD, HTN, hyperlipidemia, anemia, osteoarthritis
• Chief complaint: SOB and “heart fluttering”• Not taking meds previously prescribed, hasn’t
seen PCP in a few years• Dx of new-onset Atrial fibrillation and d/c with:
Metoprolol 100mg every 12 hoursSimvastatin 20mg every nightWarfarin 2.5mg daily at 1700
IU Geriatrics
The Problem: Case of Mrs. C
• Admitted on 2/27/11 with CC of SOB• Stopped meds one month after previous
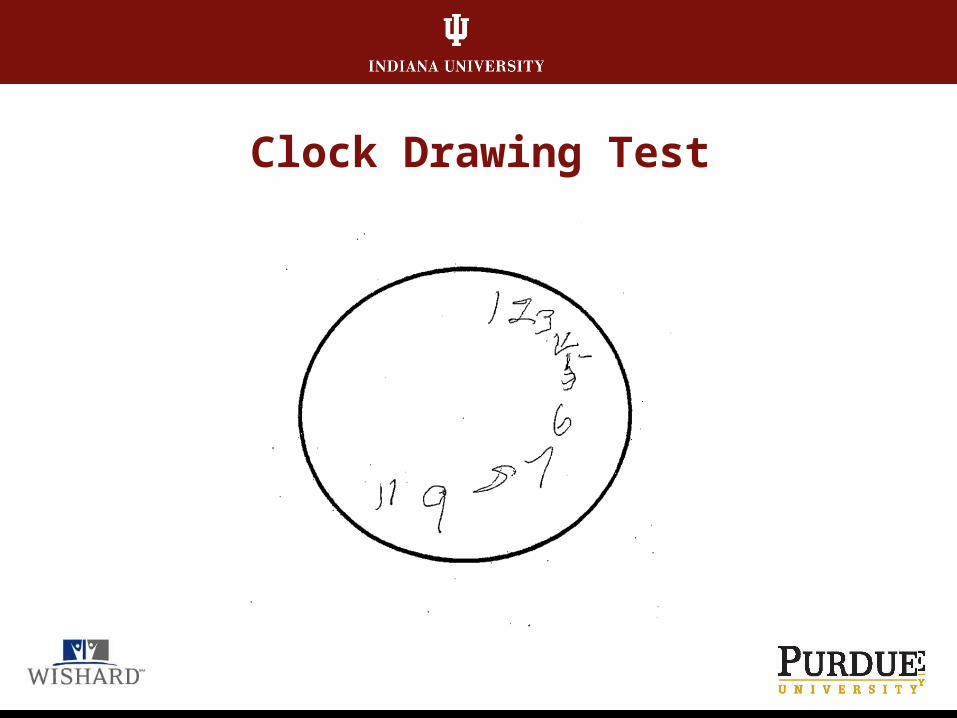
discharge, states she “Just felt better”• Diagnosis – same as previous diagnosis• Lives in own house with grandson• MMSE 24/30 - Indep with ADL, most IADL• CAM negative, abnormal CDT
IU Geriatrics
Clock Drawing Test
IU Geriatrics
The Problem: Case of Mrs. C
• Following hospitalization, home visit reveals patient has correct medications at home:Medication distributed between two boxesMed box contains variable doses of 2/5 discharge
medsWarfarin doses in med box range from 2.5-15mg
Patient unaware of what her prescribed dose should be -
IU Geriatrics
WHAT INTERVENTIONS IMPROVE MEDICATION
ADHERENCE IN OLDER ADULTS
WITH CI?
Results of a systematic review
IU Geriatrics
Search criteria and sources
• Inclusion criteriaRandomized controlled trialBlinded outcome assessmentsAdults aged 45 years or greaterDiagnosis of cognitive impairment
• Search sourcesMedline, PsycINFO, CINAHL, Google ScholarPublished articles or abstracts from 1966-Nov. 1, 2010
IU Geriatrics
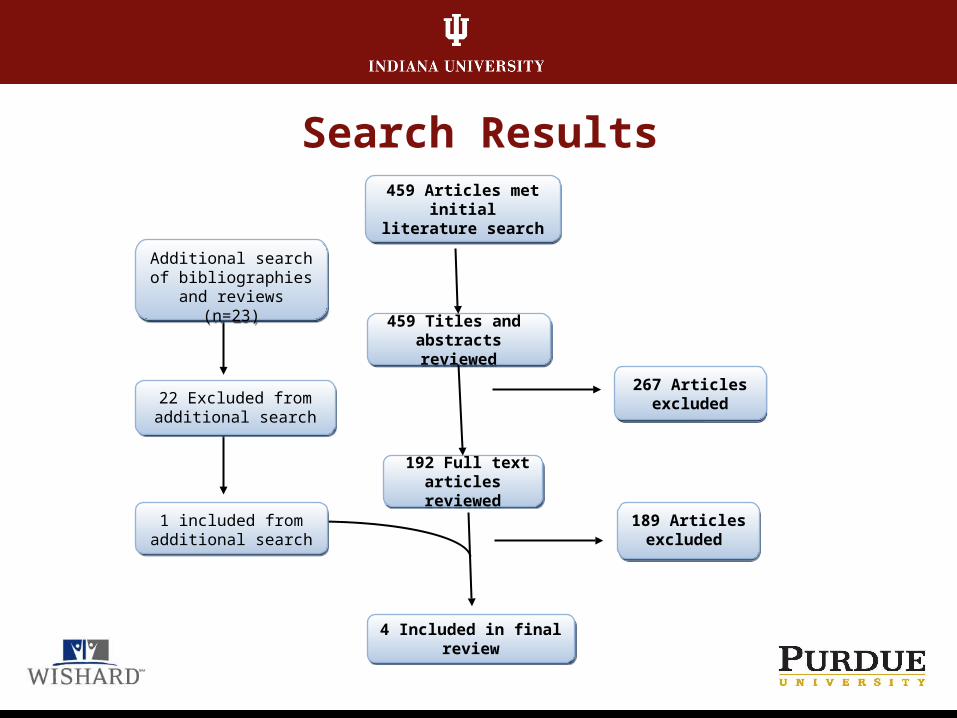
Search Results
192 Full text articles reviewed
192 Full text articles reviewed
267 Articles excluded
267 Articles excluded
189 Articles excluded
189 Articles excluded
22 Excluded from additional search22 Excluded from additional search
459 Titles and abstracts reviewed
459 Titles and abstracts reviewed
Additional search of bibliographies and
reviews (n=23)
Additional search of bibliographies and
reviews (n=23)
459 Articles met initial literature search
459 Articles met initial literature search
1 included from additional search1 included from
additional search
4 Included in final review4 Included in final review
IU Geriatrics
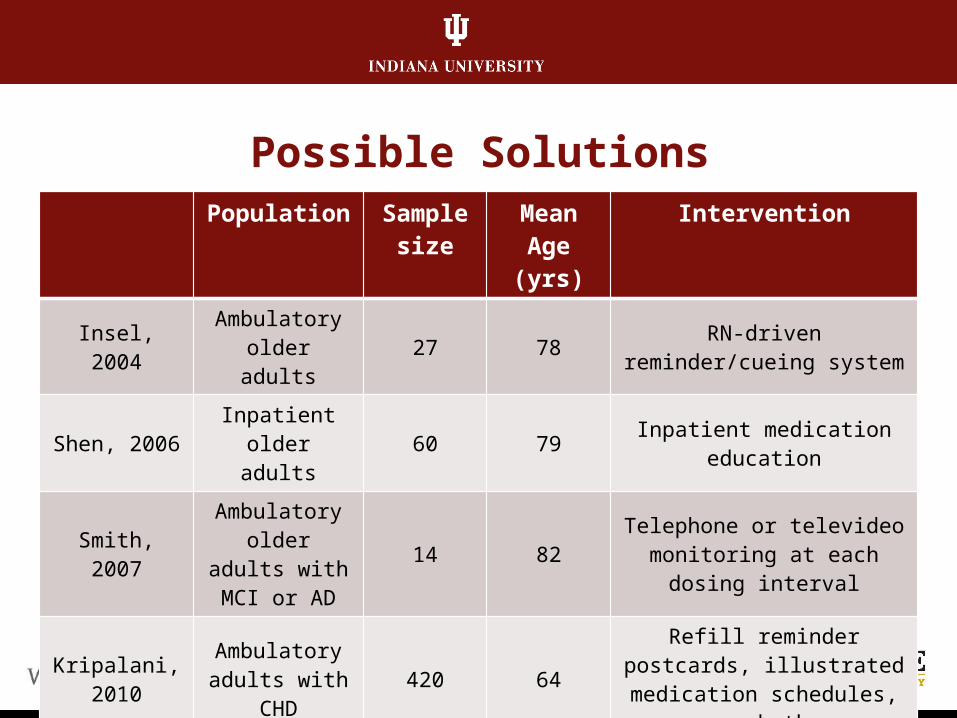
Possible SolutionsPopulation Sample
sizeMean
Age (yrs)Intervention
Insel, 2004 Ambulatory older adults 27 78 RN-driven reminder/cueing
system
Shen, 2006 Inpatient older adults 60 79 Inpatient medication
education
Smith, 2007Ambulatory older adults
with MCI or AD14 82
Telephone or televideo monitoring at each dosing
interval
Kripalani, 2010
Ambulatory adults with
CHD420 64
Refill reminder postcards, illustrated medication
schedules, or both
IU Geriatrics
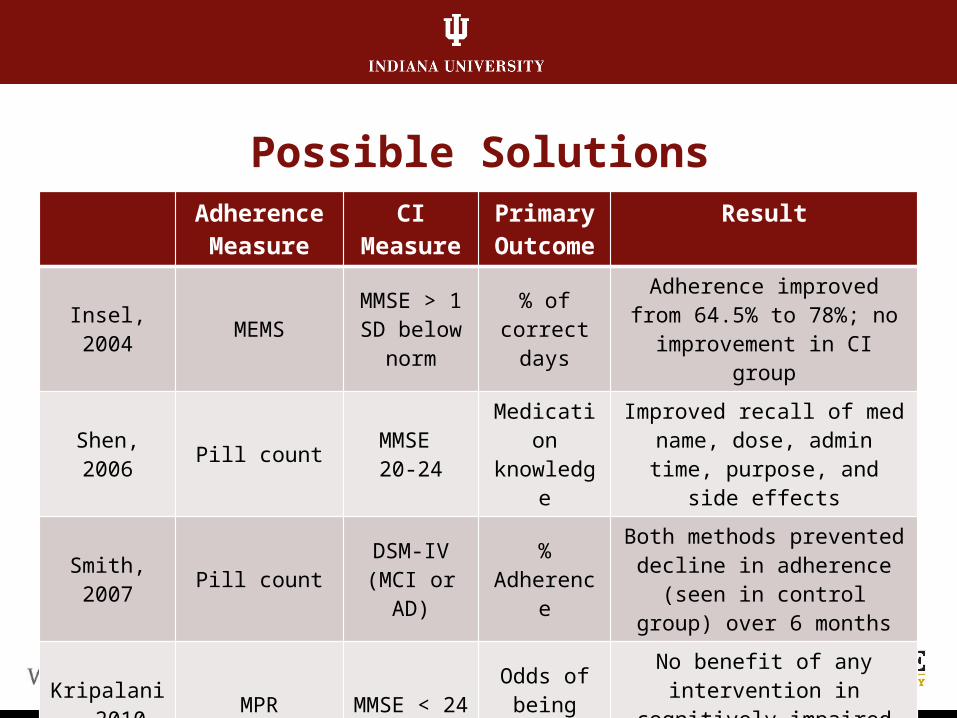
Possible SolutionsAdherence
MeasureCI
MeasurePrimary
OutcomeResult
Insel, 2004 MEMSMMSE > 1 SD below
norm
% of correct days
Adherence improved from 64.5% to 78%; no
improvement in CI group
Shen, 2006 Pill count MMSE 20-24
Medication knowledge
Improved recall of med name, dose, admin time, purpose,
and side effects
Smith, 2007 Pill count DSM-IV (MCI or AD)
% Adherence
Both methods prevented decline in adherence (seen in control group) over 6 months
Kripalani, 2010 MPR MMSE < 24
Odds of being
adherent
No benefit of any intervention in cognitively impaired group
IU Geriatrics
Summary of Interventions
• Three interventions studied medication adherence in subjects with CI: Behavioral cueing and reminder systems Telephone/televideo monitoring Inpatient medication education
• Two of three interventions revealed positive results Medication education improved knowledge Telemonitoring prevented decline in adherence
• Behavioral and reminder interventions had no impact
IU Geriatrics
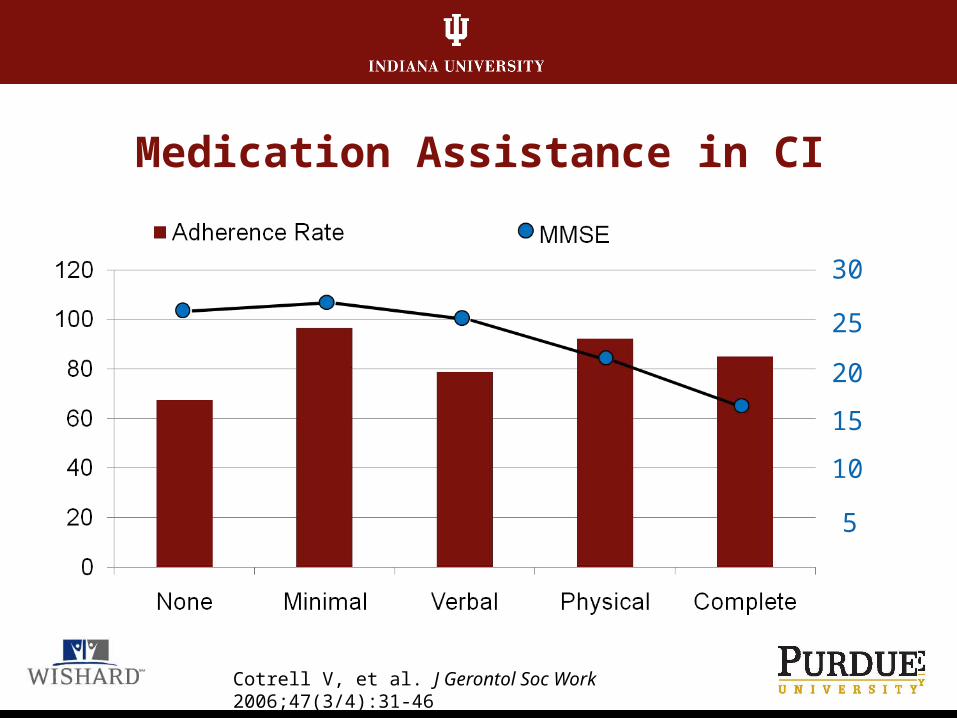
Medication Assistance in CI
30
25
20
15
10
5
Cotrell V, et al. J Gerontol Soc Work 2006;47(3/4):31-46
IU Geriatrics
Potential Targets
• Caregivers report hassles with medication administration schedulesMore frequent amongst employed carers or those
caring for > 1 loved one
• Keeping multiple prescriptions filled• Medication administration difficult during “conflict
periods” Verifying response if dose not administered
• How to react to emergency or safety situations
Travis S, et al. J Gerontol A Biol Sci Med Sci 2000;55(7):M412-7
IU Geriatrics
Potential Targets
• Lack of understanding (drug vs. disease)
• Dexterity & vision (ability to open drug container)
• More frequent changes in regimen
• Higher pill burden and cost
• Forgetfullness/planning
Nikolaus T, et al. Eur J Clin Pharm 1996;49(4):255-9.Borah, et al. Curr Med Res Opin 2010;26:1957-65.Hayes T, et al. J Aging Health 2009; 21(4):567-580.
IU Geriatrics
Potential Targets
• Older adults open to electronic interventions, but not willing to payCost ranges from $40-$750Clinicians rated dispensing devices not usable by those
with cognitive impairmentAuthors felt participants were unlikely to use device
Wakefield, et al. J Gerontol Nursing 2008;34(7):15-25.
IU Geriatrics
Deliberation:
• What methods have success at individual level?
• What content should be considered?
• How should the content be delivered?
• How might an intervention change with degree of cognitive function?





























