Embed Size (px)
Citation preview

'5I
SCIATIC PAIN *By H. LOVELL HOFFMAN, M.D., M.R.C.P.
Honorary Assistant Physician to the Royal United Hospital, and the Royal National Hospitalfor Rheumatic Diseases, Bath
There is no need for me to stress the chaoticstate of our ideas in the past regarding sciaticpain. The fault lies undoubtedlv with thosewho, from the depths of their armchairs, pro-pounded theories based on inadequatepathological evidence, or succumbed to thealmost overwhelming temptation to adopt asimple explanation for all cases. To the latterWalshe has tritely replied in discussing thisparticular subject, ' Nature is not interested insimplicity.'
Being faced with the task of producing foryou some order out of this chaos, it is my aimto steer a course midway between the Scylla ofdogmatism and the Charybdis of sheer vague-ness. With regard to sciatic pain we needfacts, and first I propose to mention brieflythose which are incontravertible.
Proved Causes of SciaticaIt is quite definite that sciatic pain may arise
when the nerve or its central connections areaffected by a pathological process such asherpes zoster, tabes, new growth or theneuritis of diabetes, alcohol or arsenic; dis-seminated sclerosis is 'a very rare cause. Itmay also be due to disease in the vicinity of thenerve's course or central connections., and thefollowing conditions may be cited as examples.In the meninges, arachnoiditis, syphilis ormeningioma. In the vertebral bodies, caries,osteomyelitis, Paget's disease and new growth.In the pelvis, inflammation or new growtheither in the bones or viscera, or inflammatorychanges in the sacro-iliac joint.
It is also certain that sciatic pain may beproduced by herniation of the nucleus pul-posus of a lumbar intervertebral disc. Thelesion has now been verified at countless
operations, and its removal has relieved thesymptoms. We also know that sciatica wasjust as common before the discovery.of thiscondition, and that patients recovered withoutoperation. The inference to be drawn fromthis fact is that healing or reduction of thelesion may in some cases occur without sur-gical intervention.These are the causes of sciatic pain of which
we have no doubt. We must now considerother possible causes based on less certainpathological grounds.
Less Certain Causes of SciaticaSciatic neuritis or interstitial neuritis
I have already mentioned that this may occurwhen due to diabetes, alcohol, or arsenic. Weknow also that interstitial, neuritis of othernerves is not uncommon, ahd examples such asoccipital or supra-orbital neuritis, and brachialneuritis may be mentioned. These con-ditions may arise, like other rheumatic mani-festations, after exposure to damp or cold, andbe part of what we have termed a local orgeneral ' fibrositis,' although the pathologicalbasis of this lesion is a rather vague one.Although I feel sure that a true brachialneuritis or neuralgia of this nature does exist,many cases of pain in the arm with definiteroot signs, have recently been proved to becaused by a cervical disc lesion, which need notnecessarily cause signs of cord compression.Our ideas regarding the symptom are there-fore falling more into line with our conceptionof sciatica. Spurling and Scoville (I944);Elliott and Krerner (I945).
It has been argued that an inflamed sciaticnerve has rarely been seen and examined;naturally there are few opportunities for this.
* A PQstgraduate lecture delivered at the RoyalNational Hospital for Rheumatic Diseases, August,1946.
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.257.151 on 1 March 1947. D
ownloaded from

£52 POST-GRADUATE MEDICAL JOURNAL March, J947
-1- -2- -3-
One case was described by Denny Brown(I933) in a woman who died after oxygen hadbeen therapeutically injected into the thigh.The author found exudate under the per-ineurium of the individual nierve fibres, butcertain other changes which he discovered,may have been due to the oxygen injection.More recently Holmes and Sworn (I946)
hiave found evidence of what was termed'radiculitis ' at operation. 'I his consistedeither of swelling of a nerve root, or adhesionsaround it, for whic4, they were unable to find amechanical cause.The general impression, with which I
personally concur, is that sciatic ' neuritis ' orrqdiculitis does exist, but is rare. It was res-ponsible for or ly 3 per cent. of a series of casesz,ollhted by Jacksor in 1943 (vide infra).
Referred sciatica and the role offibrositisKellgren produced pain referred to the
corresponding root distribution by injecting anirritant substance into the interspinous liga-ments. It is certain that sciatic pain can be re-ferred from disease of the sacro-iliac joint, as inearly ankylosing spondylitis, or from osteo-arthritis of the hip. Steindler (I940) states thatsimilar pain !may be referred from areas oftrauma or ' fibrositis ' in the back and glutealmuscles, which are in the territory of theposterior primary divisions of the spinal nerves,the anterior primary divisions of which go toform the sciatic trunk. He further states thatrelief is obtained by injecting novocaine intothese myalgic areas. Elliott (I944), however,has pointed out that similar tender areas are
found in the upper gluteal regior of cases withundoubted disc lesions, and I have confirmedthis observatiop on several occasions. Byelectromyographic study of these spots he hasfound spontaneous motor activity in themuscle, and considers that they are due -to in-voluntary spasm of small groups of musclefibres, caused by irritation of the nerve rootmore centrally. He repeated Kellgren's experi-ment and in some cases found continuousmotor discharge from muscles in the area of.referred pain. He therefore suggests thatlocalized, spasm can be induced through areflex path which involves the anterior horncells, and that the source of excitation may bein, or outside the nerve root. He has recordedsimilar motor activity in the so-called fibrositisof the shoulder girdle associated with cervicalosteoarthritis, and in the extensor muscles ofthe arm in brachial neuritis with or withoutroot signs.
This work is of great interest and importancesuggesting a new conception not only of re-ferred pain, but also of that mysterious con-dition ' fibrositis.' As regards the latter, it isfascinating to postulate a vicious circle,initiated, perhaps, by cold or minor trauma,producing muscle spasm and pain. By reflexaction through the cord, this pain may producea motor impulse causing further muscle spasmin the affected segment, and so on. Such areflex process could explain the sudden onsetof fibrositis, so unlike an inflammation, and ourtreatment at once becomes rational, breakingthe vicious circle at various points. Heat andimmobilization. tend to reduce muscle spasm,
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.257.151 on 1 March 1947. D
ownloaded from

March, '947 SCIATIC PAIN 153
and nfvQQCaine injvtion relieves pain. Later,m4spage and manipulation will further freethe muscle fibres and encourage them toresume their normal activity. In a recentarticle which, inter alia describes myalgic Areassecondary to visceral disease, Kelly (1946)favours a similar hypothesis, and suggeststhat.... nervous reflexes are instrumental inthe causation of fibrositic lesions in general.'
It is not my intention to theorize further re-garding the nature of fibrositis, in the absenceof rnore definite pathological proof. It shouldbe remembered that gout, gonorrhoea andfocal sepsis may play a part in its causation.The condition has been said to producesciatic pain in two ways, either by referencefrom remote areas, or by direct spread to thenerve itself. From what has already beenstated it seems reasonable to assume that re-ferred sciatica may be so caused, but the con-ception of fibrositis spreading directly to thenerve is more difficult to accept in the light ofnew theories.
The role of lumbar osteoarthritis
Harris (I933) and Putti (1927) describecases where the nerve roots are compressed atthe foramina by arthritis of the intervertebraljoints. A spine, however, may bristle withosteophytes and yet produce no symptoms;further, in advanced ankylosing spondylitissciatic pain is rare. Burt (1933) explained thisfact by pointing out that the latter condition isa sclerosing arthritis, without effusion, whichrapidly immobilizes the spine. It is probablethat certain cases of sciatica are due to vertebralosteoarthritis, especially in older subjects, andthat cold, damp and trauma play a part ininitiating the symptoms; but it is generallyagreed that the soft tissue changes of thearthritis, not the bony ones, are responsible forthe pain. Great care is necessary in makingthis diagnosis, as radiological signs of spinalosteoarthritis are common in cases with proveddisc lesions.The following table is reproduced from an
article by Jackson (I943). He states that, ofthe doubtful cases, seven were probably due todisc lesions, and the series gives a good idea ofthe relative frequency of the causes of sciaticain Service personnel.
Diagno4iF. NumberDoubtful ..2Fibrositis (local) ..cRuptuLred intervertebral dist. . 8Hysteria .. ..Fibrositis and neurosis 8Congenital bony abnormaliti, 4Fibrositis (generalized) .. 3Sciatic neuritis 3Malingering 2Sacro-iliac strain 2Lumbo-sacrao strain 2Spinal osteo-arthritis I..Bony infection INeoplasm of cauda equinaPolyradiculitis .. .. ..Secondarv carcinoma ..Disseminated sclerosis. . ISpastic paraplegia (? aetiology) . I
IOO
Sciatica Pain due to Protruded Inter-vertebral Disc
The intervertebral disc consists of theannulus fibrosus which is weaker posteriorlythan anteriorly, a cartillaginous plate above andbelow, and the nucleus pulposus, which liesslightly more to the posterior part of the disc.As a result of trauma and degenerative changes,the annulus fibrosus may rupture partially, andthe nucleus pulposus will herniate either incertain postures only, or permanently. If theannulus ruptures completely, the nucleus pro-lapses, and part or all of it will come to lieunder the posterior longitudinal ligament.Owing to the position of the nucleus in theposterior part of the disc, and the relativeweakness of the posterior part of the annulus,these protrusions tend to occur posteriorly, thenucleus being squeezed like a pea out of a podwhen the spine is in flexion. Compression ofa nerve root may result. The fifth lumbar rootis most commonly compressed by the fourthdisc, the first sacral root by the fifth disc andso on.
Th. clinical history and physical signs ofthe syndrome vary- from case to case, and ifcertain possibilities are borne in mind it iseasy to see how these vaiiations may occur. Ihave already mentioned that the nucleus mayherniate temporarily and only in certainpostures. This accounts for the intermittent
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.257.151 on 1 March 1947. D
ownloaded from

POST-GRADUATE MEDICAL JOURNAL
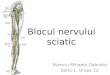
charactet of the symptoms in some cases. Thefigure shows the possible anatomical relation-ship of the hemiation to'the' nerve root. It iseasy to see that the nerve may slip off theherniation; this explains the relief ofsymptoms, which is sometimes brought aboutby spinal manipulation' or epidural injection ofsaline and novocaine, the root being 'floatedoff' the projection. Further, it may be that-the three possible positions account for thevariability of the scoliosis in these cases.Scoliosis may be either towards the affectedside, away from it, or alternating. In manycases adhesions form between the nerve andthe protrusion, in which case it would bereasonable to expect more intractable symp-toms. Flexion of the spine or straight legraising puts the theca on the stretch and willtend to aggravate pain by stretching theaffected nerve root over the projection.Flexion, however, opens up the intervertebralforamina and may relieve pressure oni anoedematous nerve root. Extension of thespine has precisely the opposite effect, andmay aggravate pain by causing increasedpressure on the root at the intervertebralforamen. Capener (i944).
Clinical HistoryA history of frank -trauma initiating the
symptoms was given by 23 per cent. of Macey'scases (1940). Bradford and Spurling (I94I)give the figure as 50 per cent. The traumamay be an actual fall on the back, a straincaused by lifting a heavy weight with the spineflexed, a false swing at golf, or similar suddenmovement. There may be no rememberedhistory of injury, or the patient's occupationmay suggest that he has suffered repeatedsmall strains over a prolonged period. Preg-nancy and labour are sometimes responsiblefor the lesion. Usually the first symptomis a fairly sudden onset of backache, and it isfair to assume that this is due to rupture ofthe annulus fibrosus. Sciatic pain may developat the same time or be delayed for days ormonths, occurring, most probably, whenactual protrusion of the nucleus takes place andcompresses a nerve root. The distribution ofthe pain varies according to which root is com-pressed, and the areas affected may be sum-marized thus, Connell (I946)
L.4 Anterior crural to medial malleolus.IL.5 Posterior crural to dorsum and medial
margin of foot.S. i Posterior crural to sole- and lateral mar-
gin of foot.The pain is usually relieved only when the
patient lies absolutely still. It is aggravated bymovement and by sneezing or coughing. Thisaggravation is supposed'to be due to a rise incerebrospinal fluid tension with consequentpressure on the nerve root, and has been con-sidered to be a diagnostic feature of root in-volvement. I cannot believe that this is true.On coughing, all the trunk and buttockmuscles contract, and I am sure that it iscontraction of the latter, including the pyri-formis in close relation to the sciatic nerve,which produces the exacerbation of pain.Paraesthesiae may be experienced in the samedistribution as the pain, and consist of tingling,numbness, pins and needles or a burningsensation.
Physical SignsThese are orthopaedic and neurological,
both being of importance in the recognitionand lo'calization of the lesion.
Orthopaedic. The normal lumbar lordosismay be lost or diminished. Sometimes a slightkyphosis is encountered in the lumbar region.Scoliosis is common, usually to the side of thelesion, but may be away from it, or even varyfrom time to time in the same patient. Some-times the scoliosis is not present when standingerect, but becomes evident only when an'attempt is made to flex the spine. Movementsof the lumbar region are limited, especiallyflexion, which nearly'always increases the pain.An important sign is the presence of tender-ness, either in the mid line over the affectedinterspace, or just lateral to it, on the side ofthe lesion. This tenderness is best elicited byfirm pressure with the thumb. If, in additionto local tenderness, there is an exacerbation ofpain in the corresponding dermatome, theevidence is strongly in favour of root com-pression by a disc lesion, 'Little (I946).
Neurological. There may be slight wastingof the buttock, posterior thigh, or calf muscleson the affected side, but this is not usually verymarked. Muscle weakness is most commonlyfound in the dorsiflexors of the ankle, but mav
March ' 1947'1154copyright.
on June 5, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.257.151 on 1 M
arch 1947. Dow
nloaded from

c SCIATIC PAIN
be present' in any of the muscles supplied bythe affected roots. Sometimes the only weak-ness discovered is in dorsiflexion of the greattoe and this sign should always be sought insuspected cases of disc protrusion. Sensoryloss is not always present. It is ,usually slightin degree, consisting of blunting to pin prickor loss of sense of light touch. In my ex-perience it rarely involves the completedermatome as illustrated in the text books.This is because there is considerable overlapand variation of the skin areas supplied by the'spinal roots. Thus in a lesion of the fifthlumbar root, loss of sensation will occur in thearea of skin supplied solely'by this root. Thepicture is further complicated by the fact thattwo nerve roots may be involved by a singledisc protrusion, Spurling and Grantham(I940). Moreover the lumbo-sacral plexusmay be pre- or post-fixed, and it will thus beseen that a reliable localization of 'the disclesion is not always possible from considera-tion of the sensory signs alone. The sciaticnerve is often tender at its exit from the pelvisand in the posterior thigh. Other tenderareas may be found in the gluteal region, thesignificance of which has already been dis-cussed. Straight leg raising, or extension ofthe knee with the hip flexed to a right angle(Lasegue's sign) may be limited by pain on theaffected side. If these manipulations atestopped just short of producing pain, neckflexion or dorsiflexion of the ankle may causeit to appear. Neck flexion carried out in thisway acts by stretching the affected nerve rootor the theca, and if pain results, it is goodevidence that a root lesion exists. Lasegue'ssign itself, on the other hand, is often positivein cases of referred sciatica, and it seemsreasonable to assume that this may be due, inpart at least, to stretching of the spastic ham-string muscles. Naffziger's test for root in-volvement consists of bilateral jugular com-pression, and is positive when pain orparaesthesiae result in the affected area. TheCSF pressure is raised, and further tensionresults in the compressed nerve root. Ifpositive, the sign is of considerable diagnosticvalue.
In lesions of the fourth lumbar root theknee jerk will tend to be diminished or absent;with a lesion of the fifth lumbar root the ankle
jerk 'many be diminished or normal, while ifthe first sacral root' is involved the ankle' jerkis usually lost or at least diminished. As in thesensory supply of the limb, there is con-siderable overlap in the roots subserving thereflexes, and individual variations are res-ponsible for inconstancy both of reflex andsensory signs. Occasionally a disc protrusionis so large that the cauda equina is compressed,in which case there will be signs as of a tumourin this region, with bladder disturbance andanaesthesia in the saddle area.
Special InvestigationsCSF. This may show a raised protein,
especially if lumbar puncture is performedbelow the level of the lesion, e.g. in theL.5-S.I interspace. As the nuclear protrusionis relatively small, conmplete spinal block witha positive Queckenstedt's test and Froln'ssyndrome 'seldom occurs, but slight rise inprotein up to 6o mgms. per cent. is a fairlycommon finding. The reversed Queckenstedttest is carried out with a manometer attachedto a needle in the lumbar theca, whilz s4line isinjected into the epidural space aKt -;he sacralhiatus. If the' pressure if ,to xse in themanometer, a block may be assumed to existbetween the two needles.
X-ray. Straight X-rays sometimes shownarrowing of the intervertebral space corres-ponding to the affected disc, but this is notusual. Developmental anomalies of the'lumbo-sacral region are sometimes seen in cases ofdisc protrusion; for example, .there may besacralization of the fifth lumbar vertebra,unilateral alteration of the plane of the articularfacets, or spondilolithesis. These need notnecessarily be the direct cause of sciatic pain,as has previously been supposed. It seemsmore likely that, by upsetting the spinalmechanics, they can predispose to degenera-tion of the annulus, and consequent nuclearprotrusion. It is important to realize that thelumbar spine is an extremely complicatedsystem of joints, liable to all the diseases andinsults which may affect the other joints of thebody, and that many different signs andsymptoms may arise therefrom. It is alsoimportant to view disc lesions in their properperspective. The disc is merely a part of thejoint, comparable to the fibro-cartillage of other
March 7 1947 I5.5copyright.
on June 5, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.257.151 on 1 M
arch 1947. Dow
nloaded from

POST-GRADUATE MEDICAL JOURNAL
joints; but it is also the focal point throughwhich abnormalities of the spinal meehanicswill most frequently produce gct4 nerve rootcompression, and so give rise to sciatica.Myodil is now being used for myelograhy
in place of lipiodol. It is a stable compound,c'using little irritation and is slowly absorbedby the spmal canal. It is of low viscosity andcan therefore be removed through a lumb4rpunctige needle. I have no experience ofmyelography in disc lesions; the techniqueand positioning is complicated and time con-suming, but many consider that it is of greatvalue in these cases. Personally I agree with'those who hold that a disc lesion can bediagnosed and located on clinical groundsalone.
Differential Diagnosis.Sciatic Neuritis. It is almost impossible to
differentiate with certainty between this con-dition and a disc lesion. In neuritis one ismore likely to see signs of involvement of thewhole nerve than of its individual roots.Walshe (I946) states that single attacks ofacute onset and relatively short duration aremore likely to be due to this cause.
Root Compression from neoplasm. Here thesigns are more insidious in onset and steady inprogression. Weakness, wasting, and sensoryloss are always more marked and bladder dis-turbance more common. If the growth ismalignant, there are likely to be signs ofcachexia.
Referred Sciatica. In referred pain therewill be no signs of actual nerve involvement;thus, sensory loss, marked weakness or wasting,and absent tendon reflexes will not be found.The pain of root compression is always felt inthe territory of that root, whereas referred painis far more diffuse and vague in its distribution.Pain i eferred from osteoarthritis of the hiptends to radiate to the anterior part of thethigh, there will be limitation of movement ofthe joint, and percussion of the heel may causepain. X-rays of the pelvis should always beexamined carefully for lesions of the sacroiliacjoint such as tuberculosis or early ankylosingspondylitis, which are important causes ofreferred sciatica.
IIysteria. Although sciatic pain or purelyhysterical origin is rare, it is extremely common
to find a hy§terical prolongation of a previousorganic sciatica. Such cases are difficult toassess because there may be residual neuro-logical signs as a legacy of the anteceedentattqck, It is most important in all such casesto look for positive signs of hysteria rather thanfor negative signs of organic disease, and toseek possible escapist motives, and unsettledcompensation claim. These patients mayshow an exaggerated or even fantastwc limp.They will, with great show of emotion, resistall movements of the limb, irrespective ofthose which should actually cause pain. Areasof anaesthesia may be. typically hysterical, in-volving the patient's conception Qf a limbsegment and bearing no relation to nerve orroot distribution; such areas, moreover, mayeasily be suggested to the patient. Occasionallyit will be found that bending forward from theerect posture or straight leg raising is bitterlyresisted, as the patient has learnt from previousexaminations that this should cause pain. Yethe may be induced, without complaint, tobend forward and touch his toes while sittingon a couch, showing that the movements,which are essentially the same in each case,are really not painful at all.
TreatmentIn all cases of sciatica, unless there are sure
signs of cord or cauda equina pressure, then con-servative treatment should first be tried. Restin bed is the first essential and should be main-tained for four to six weeks if necessary. Apillow under the affected knee may give relief,or the leg may be immobilized with sandbagsor a long Liston splint; weight extension isoften useful. During this period local heat inthe form of hot water bottles, electric pads,radiant heat and mud packs may be employed.Analgesic drugs are usually essential in theearly stages, and aspirin, phenacetin, veganin,or sonalgin may be used. In some cases,however, only morphia will give relief. If, atthe end of this time, pain is relieved, massageand exercises to the spine are carried out tocorrect faulty posture which may have beenresponsible for weakening of the annulus andconsequent disc protrusion; these may, withadvantage, be carried out in a hot pool.
If rest is not successful, it is the practice ofour orthopaedic department, under Mr. John
156 Mar,ch, 1947copyright.
on June 5, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.257.151 on 1 M
arch 1947. Dow
nloaded from

March, I947 CAESAREAN SECTION IN MODERN OBSTETRICS
Bastow, to give an epidural injection of 120c.c.s of half per cent. procaine in saline underpentothal anaesthesia, followed by gentlerotatary manipulation of the spine, and straightleg raising. A plaster corset is then appliedwhich is worn for three months. At the end
of this period, massage and exercises arecarried out as above. Should these measuresnot give relief, and other signs point to thepresence of a disc lesion, laminectomy, withremoval of the prolapsed nucleus pulposus, isconsidered.
REFERENCESBRADFORD, F. K., and SPURLING, R. G. (I94I) 'The Inter-
vertebral Disc,' Springfield and Baltimore.BURT, J. BARNES (1933), Proc. Roy. Soc. Med., 26, 1396.CAPENER (X944), 'Annals of the Rheumatic Diseases,' 4, 29.DENNY BROWN, D. (933), Proc. Roy. Soc. Med., 26 I399.ELLIOTT, F. A. (1944), Lancet, I, 47.ELLIOTT, F. A., and KREMER, M. (I945), Lancet, I, 4.HARRIS, W. (x933), Proc. Rov. Soc. Med., 26, 1389.HOLMES, J. MACD., and SWORN, B. R. (1946), Brit. Med. J.,
I, 946.JACKSON, W. P. V. (I943), Ibid., I, 776.
LITTLE, N. (1946), Med. _'ourn. of Australia, I, 33.MACEY, H. B. (1940), Arch. Surg., 40, 433.O'CONNELL, J. E. A. (1946), Brit. M1ed. j., I, I22.PUTTI, V. (1927), Lancet, 2, 53.SPURLING, R. G., and GRANTHAM, E. G. (1940), Arch.
Surg., 40, 375.SPURLING, R. G., and SCOVILLE, W. B. (1944), Surg. Gynaec.
Obstet., 78, 350.STEINDLER, A. J. (1940), J. Bone and Joint Surg., 22, 28.WALSHE, F. M. R. (1946), 'Diseases of the Nervous System,'
Edinburgh, E. and S. Livingstone.
THE PLACE OF CAESAREAN SECTION INMODERN OBSTETRICS
By JOSEPHINE BARNES, M.A., D.M., M.R.C.P., F.R.C.S., M.R.C.O.G.Assistant, Obstetric Unit, University College Hospital
One of the most striking developments inmodern obstetrics has been the immense in-crease in the number of women delivered byCaesarean section. Two hundred years agothe Caesarean operation was regarded as thelast resort in a desperate emergency whendelivery was possible by no other means. Themortality was exceedingly high-in fact re-covery from the operation was considered veryremarkable. Smellie (eighth posthumousedition) wrote concerning the operation that itmight be occasionally indicated ' because themother and child have no other chance to besaved, and it is better to have recourse to anoperation which has sometimes sufcceeded thanto leave them both to inevitable death.'Today the position is very different. It has
become necessary for eminent obstetricians towarn their colleagues against the abuse of anoperation which, thanks to the development ofanaesthesia, of aseptic and antiseptic technique,and to a lesser extent of chemotherapeuticmethods has become, in some hands, a meansof avoiding even the slightest difficulty inlabour. These warnings are timely since noother procedure is more open to abuse. Nohigh degree of operative skill is needed,certainly not for the classical operation, butonly wide obstetrical experience can give the
judgment needed to decide when delivery bythe natural passages is likely to provesufficiently dangerous to mother or child thatoperative delivery is to be preferred.
The Advantages of Caesarean SectionIt must not be assumed that because the
operation of Caesarean is so easily open toabuse that its wider employment is not, on thewhole, a great advance, in midwifery. Theadvantage of reasonably safe abdominal de-livery in cases such as those of severely con-tracted pelvis where natural delivery would behazardous, if not impossible, are self-evident.The advantages of abdominal delivery may besummed up under two main headings.
Firstly, it avoids the danger of delivery bythe vagina and there are' many circumstances,as will be seen, where it is inadvisable even toattempt such delivery, while in other cases thecourse of labour may be seen to be so un-favourable that it seems unwise to allow it toproceed further. Secondly, Caesarean sectionoffers a rapid method of terminating pregnancyand may thus be considered as an alternativeto induction of labour. The methods of in-duction in current use, admirable though theyare in favourable cases, are all very uncertain
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.257.151 on 1 March 1947. D
ownloaded from