Embed Size (px)
DESCRIPTION
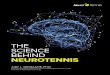
ECC. Science Behind the Guidelines. John M. Field M.D. FAHA, FACC, FACEP Professor Medicine & Surgery PSU College Medicine Penn State Heart and Vascular Institute Senior Science Editor Emergency Cardiovascular Care Programs AHA National Center, Dallas. - PowerPoint PPT Presentation
Citation preview

Science Behind the Guidelines
John M. Field M.D. FAHA, FACC, FACEP Professor Medicine & Surgery
PSU College MedicinePenn State Heart and Vascular Institute
Senior Science Editor Emergency Cardiovascular Care Programs
AHA National Center, Dallas
ECC

The Importance of Early Defibrillation
…the perceived value of antiarrhythmics, vasopressors, advanced airway control and ventilation has declined markedly since 1992- the evidence is disappointingly weak that any of these interventions convey effective benefit to cardiac arrest patients.
CURRENTS AHA September, 2000

…the relative value of early defibrillation by reducing 1-2 minutes the interval between adult sudden cardiac arrest and a first defibrillatory shock does more to improve survival than the benefit from medications, airway interventions and newly designed defibrillation waveforms combined.
CURRENTS AHA September, 2000
The Importance of Early Defibrillation

Cobb, L. A. et al. JAMA 1999;281:1182-1188.
Survival Rates for Out-of-Hospital VF
1975 1977 1979 1981 1983 1985 1987 1989 1991 19993
40
35
30
25
20
15
10
5
0
First Response w
ith AED
%
100
75
50
0
AED

Stiell, I. G. et al. N Engl J Med 2004;351:647-656
Survival to Hospital Discharge
BLS
Variable Adjusted Odds Ration
Age < 75yrs
First Link- Early Access
Second Link- Bystander CPR
Third Link- Early Defib
Fourth Link- ACLS
1.6
4.4
3.4
3.7
1.1

1
Guidelines 2005
• Major changes
• Science Behind The Guidelines
• Major Challenges
G
U
I
D
E
L
I
N
E
S
2
0
0
5

1
Guidelines 2005 SUMMARY• Major changes
• Science Behind The Guidelines
G
U
I
D
E
L
I
N
E
S
2
0
0
5

Weighing the Evidence Grade of Evidence
Data from many large, randomized trials
Data from fewer, smaller randomized trials, careful
analyses of nonrandomized studies, observational
registries
Expert consensus
G
U
I
D
E
L
I
N
E
S
2
0
0
5

Weighing the EvidenceData from clinical trials, significant Rx effects
Data from clinical trials, smaller Rx effects
Prospective non-randomized cohort studies
Historic or case controlled studies
Case series- no control group
Animal or model studies
Extrapolation
Common sense or common practice
ECC
LEVEL 1
LEVEL 8

Class of RecommendationsClass of Recommendations
Intervention is useful and effective
Evidence conflicts/opinions differ but leans towards efficacy
Evidence conflicts/opinions differ but leans against efficacy
Intervention is not useful/effective and may be harmful
II IIaIIa IIbIIb IIIIII

II IIaIIa IIbIIb IIIIIIClass of RecommendationsClass of Recommendations
Intervention is useful and effective
Evidence conflicts/opinions differ but leans towards efficacy
Evidence conflicts/opinions differ but leans against efficacy
Intervention is not useful/effective and may be harmful
No evidence of benefit-not harmful
II
ECC

Atropine (Asystole/PEA)
1mg IV Q 3-5 minutes (total dose-3mg)
No prospective studies support use
LOE – 3, 4, 5, 6
Class Recommendation- Indeterminate
ECCG
U
I
D
E
L
I
N
E
S
2
0
0
5

• Emphasis effective chest compressions
• Ventilations delivered over one second
• Single compression-ventilation ratio
• Single shock followed by immediate CPR
Emphasis advanced airway
• Recommendation intraosseous access (IO)
Emphasis ET drug administration
G
U
I
D
E
L
I
N
E
S
2
0
0
5
Major Recommendations

Key Emphasis
• Performance of High Quality CPR• Integration of CPR-BLS and
ACLSChest Compressions
• Early Defibrillation
G
U
I
D
E
L
I
N
E
S
2
0
0
5

Effective chest compressions
G
U
I
D
E
L
I
N
E
S
2
0
0
5
Major Recommendation

Coronary Perfusion Pressure (Ao diastolic - RA diastolic)Coronary Perfusion Pressure (Ao diastolic - RA diastolic)
CPR SYSTOLE(compression)
CPR DIASTOLE(relaxation)

Survival- Prolonged CPR Survival- Prolonged CPR
Berg RA et al: Circulation 2001;104:2465-70Berg RA et al: Circulation 2001;104:2465-70
00
55
1010
1515
2020
2525
3030
CP
P, m
m H
gC
PP
, mm
Hg
3535
24 hr Surv ROSC-EXP NO ROSC
Paradis

Compression Rate vs ROSC
20
40
60
80
100
QUARTILE
ROSCNRC
OM
PR
ES
SIO
N,
MIN
-1
Yu Circulation 2002;106:368Yu Circulation 2002;106:368
Push hard and push fastG
U
I
D
E
L
I
N
E
S
2
0
0
5

ROSC Chest Compression RateIn-Hospital CPR
0
10
20
30
40
50
60
70
80
90
100
95-140 87-94 72-87 40-72
NO ROSC
ROSC
Abella Circulation 2005:111

Rescue BreathsRescue BreathsWhat really happens-What really happens-
Ewy et al: Circulation 2005;111:2134-42Ewy et al: Circulation 2005;111:2134-42
12
16
00
1010
2020S
eco
nd
s fo
r 2
bre
ath
sS
eco
nd
s fo
r 2
bre
ath
s
14
Lay Med Std Medics

42% 58%
Lay persons: 2 rescue breaths interrupted CC for 16 secondsLay persons: 2 rescue breaths interrupted CC for 16 seconds
Actual CC/min=Actual CC/min=3939±11 Assar, 2000±11 Assar, 2000
16 secs

Myocardial Blood Flow and CPP Myocardial Blood Flow and CPP after 16 seconds of interrupting CPR after 16 seconds of interrupting CPR
5050
6060
7070
8080
9090
100100
1010
1212
1414
1616
1818
2020
2222
MB
F, m
l/100
g/m
inM
BF
, ml/1
00g
/min
CP
P, m
m H
gC
PP
, mm
Hg
Berg RA et al: Circulation 2001;104:2465-70Berg RA et al: Circulation 2001;104:2465-70 ICCM, WT, 10/04ICCM, WT, 10/04
P<0.001P<0.001 P<0.001P<0.001
15:215:2
15:215:2
ContinuousContinuous ContinuousContinuous

Probability - Successful Defibrillation Probability - Successful Defibrillation Interruption Chest CompressionInterruption Chest Compression
55101015152020252530303535404045455050
0 5 10 15 200 5 10 15 20Duration of hands-off, secondsDuration of hands-off, seconds
PPR
OS
CR
OS
C, %,
%
Eftestol T et al: Circulation 2002;105:2270-3Eftestol T et al: Circulation 2002;105:2270-3
n=156n=156

Intrathoracic PressureIntrathoracic PressureIncomplete Chest Recoil Incomplete Chest Recoil
0
5
10
15
20
25
100% 75% 100%
Coronary Perfusion Pressure
Mm
H
g
0
2
4
6
8
10
12
14
100% 75% 100%
Cerebral Perfusion Pressure
% Decompression
Yannopoulos Resuscitation 64:363

Incomplete Relaxation
Aufderheide Resuscitation 2005 64:353-62

0
10
20
30
40
50
60
70
80
90
1 2 3 4 5 6 7
Compressions Linear (Compressions)
Com
pres
sion
s/
min
ute
Minute of Resuscitation
Ashton Resuscitation 2002
Rescuer Fatigue
30% - COULD NOT COMPLETE

1
Effective Chest Compressions
•Push hard and push fast
Limit Interruptions Allow full chest recoil Switch every 2 minutes

0
20
40
60
80
MIP CPP Surv
12
30
mmHg/min mmHg %
RATE/ min
Aufderheide TP Circulation 2004; 109:1960-5
Death by HyperventilationDeath by Hyperventilation

Deliver ventilations over one second
G
U
I
D
E
L
I
N
E
S
2
0
0
5
Major Recommendations
Avoid Hyperventilation-Too fastToo much

Single Compression:Ventilation Ratio
Except- HCP 2 rescuer CPR for infants and children
G
U
I
D
E
L
I
N
E
S
2
0
0
5
Major Recommendations
30:2