Embed Size (px)
Citation preview

Scope of Information Communications Technologyin the Health of Diabetes Patients in Poor Rural Zones
of Panama Through Holistic, Interactive, and PersuasiveModel to Facilitate Self-Care of Diabetes Patients
Miguel Vargas-Lombardo, Ms.C.,1,2,3 Armando Jipsion, Ms.C.,2 Humberto Alvarez, Ph.D.,2
Ernestina Mensalva Ruiz, Ph.D.,3 and Elena Villalba Mora, Ph.D.3
Abstract
Background: In Latin America, public health systems that manage and warrant the health of the population lackmechanisms and technological capabilities that enable them to accept and adopt initiatives focused to guide,look after, and improve the quality of life of millions of patients with diabetes who need attention and specialcare. However, the proposal presented here for a holistic, interactive, and persuasive model to facilitate self-careof diabetes patients (hiPAPD) is the first proposal in Panama, Central America, and the Caribbean Region todevelop and implement information communications technology (ICT) platforms for the care of patients withchronic diseases such as diabetes.Methods: The process of experimentation was initiated with an agreement with all the staff of the project tocomply with the international biomedical studies stipulations, having as reference the Declaration of Helsinki ofthe World Medical Association (Recommendations to Guide to Doctors in Biomedical Research on People).Results: After several months of evaluation and ongoing work the study obtained successful validation of thehiPAPD model. The project had the support of 107 patients with diabetes, their families, friends, doctors, nursesand nursing assistants, and social groups in rural communities. Finally, the project contributed to society with ahighly innovative ICT environment that facilitates self-care of diabetes patients without financial resources andhealth.Conclusions: A timely health treatment at a decisive moment may be the difference in care for patients. Throughthe validation process conducted in this research initiative, it was demonstrated that the hiPAPD model, fromthe perspective of the patient with diabetes, relatives, friends, health workforce (nurses and nursing assistants),doctors, and societal contexts, allowed the improvement of the quality of life of patients with diabetes in poorrural zones of Panama.
Introduction
Experiences in the development of technologies forhealth encourage the necessary approach to achieve the
integration and human-to-human interaction for health,through new information technologies and communications.Other initiatives with similar orientation are currently beingdeveloped: in India, the ‘‘India Diabetes Educator Project’’project; and in the United States, ‘‘The California DiabetesProgram’’ and the ‘‘Chicago Diabetes’’ initiative, amongothers.
The main aspect that most favors the patient with diabetes,relatives, friends, doctors, nurses and nursing assistants, andsociety has been analyzed to develop and implement an in-formation communications technology (ICT) environment,which manages and influences the diabetes patient’s self-careof health and his or her environment, strengthening the rela-tionships and his or her health. On the other hand, newtechnologies of information and communication such as theinternet, sensor networks, intelligent environment, mobilewireless, social networks, virtual organizations, social soft-ware, and touch screens in various mobile devices foster new
1National Secretary of Science, Technology and Innovation of Panama, Panama.2Technological University of Panama, Panama.3Technical University of Madrid, Madrid, Spain.
DIABETES TECHNOLOGY & THERAPEUTICSVolume 12, Number 9, 2010ª Mary Ann Liebert, Inc.DOI: 10.1089/dia.2010.0042
717

efforts on prevention and care of chronic diseases such asdiabetes.
The holistic, interactive, and persuasive model to facilitateself-care of diabetes patients (hiPAPD) model has connectedthe patient, the patient’s friends, doctors, patients, familyhealth workforce (nurses and nursing assistants), and societycontexts, which interact in a joint and systematic manner toeducate, guide, facilitate, and support the self-care of the pa-tient with diabetes. The model applies ambient intelligenttechnologies that are in an environment outside of a hospitalwith sensors, plus external tracking on the part of the patient’smedical professionals. This feature makes this model differentfrom other initiatives (Fig. 1).
In terms of security and data cleansing, there is a frame-work1 to ensure quality and security of data in virtual orga-nizations that is currently being developed and implementedby the Information Technology Office of the TechnologicalUniversity of Panama as part of their strategy to improve thequality of information in health systems. Afterward, thisframework will be implemented in the ICT services of theMinistry of Health and the Social Security System in Panama.
hiPAPD Model
The outermost layers of the hiPAPD model present thecontext of society, which occupies an important position inestablishing cooperation and education for the prevention ofdiabetes. Social support groups aimed at people with diabetesare powerful and constructive because they encourage dia-betes patients to help both themselves and others. The use ofintervention groups for diabetes patients is a highlight ineducational programs.2–4
The health workforce comprises the non-medical work-force, which also promotes health, and nurses and nursingassistants. The support and follow-up of the diabetes patient’scondition is managed in this layer, managing essential med-ical services to ensure their care.
The next layer presents the medical staff context, whichprovides primary medical care services and the diagnosis ofthe diabetes condition, including monitoring the evolutionof the chronic condition of diabetes in the patient. Followingare the friends of the patient layer, which aims to provideexternal support, additional to what the patient’s family couldoffer. In this context, the creation of support groups is possiblefor the diabetes patients, with the purpose of educating andmotivating them. It is the creation of groups with the same orsimilar medical status that is conducive to the social support,recognition, and awareness of new experiences of this illness,from groups of patients with diabetes, enriching the solidaritysupport and motivation among patients.
In the layer closest to the patient—the relatives of the dia-betes patient—the modification and change of behaviors arenecessary to cope with this complex disease and to endurethe long process of support within the family. Depending onthe conceptions the family has on health, the disease, and theresources with which to face it, a disruption in the familycontext, secondary to the impact of the diagnosis, is produced.
The disorganization in the diabetes patient’s environmentwill depend on two variables: the type of the disease, whichincludes features such as pain, inability, treatment, evolution,and ideology (social and family), and the family dynamics,which are based on the degree of cohesion and the solidarityachieved by the family. It is therefore vital that the medicalworkforce provides support and resources to facilitate ori-entation and appropriate guides that accompany the familyduring this long process of adaptation and acceptance.
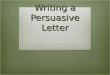
The layer corresponding to the diabetes patients (diabetespatient context) pursues persuading and motivating the self-care of the patient; also, its goal is to orient, instruct, andeducate the patient, offering new technologies that will facil-itate his or her day-by-day life. At this point, the patient isoffered noninvasive medical equipment. The patient with di-abetes may use various devices without third-party support.These devices may be managed by the patient on his or herown (self-care), as in the case of devices such as glucometers,body weight scales, pedometers, blood pressure monitors,and a tablet PC (Fig. 2).
To achieve an effective synchronization of the contexts, thehiPAPD model relies on persuasive technology, which makesemphasis on the capacity of computers and software servicesto persuade people to use them, seeking to achieve a change inattitude, world vision, and motivation.5 Computing is for Fogget al.6 an interactive technology tool that changes people’sattitudes. Similarly, on these aspects it has been proposed asthe core of the Emotional Design model.7–9 The framework ofthe Emotional Design supports the recognition of the morecomplex features of the brain structures of human beings and,in the design focus centered on users to deliver high qualityand usability, interfaces facilitating interaction of softwareservices and devices with the contexts of the diabetes patient.
To complete the model, explicit input and output relationsare carried out generated by the patient and his or her envi-ronment; in addition, there are managed systematized graph-ical interfaces that hide processes and actions actively takenby the patient. To integrate the model, relationships of im-plied interaction of input and output devices are linked to theambient intelligent environment. With an implicit entry itaccomplishes the extraction of data that subsequently generateprecise information on medical diagnosis of diabetes patients
FIG. 1. A diabetes patient using all the Bluetooth-enableddevices (pedometer, glucometer, and blood pressure monitor(Taidoc Inc. [Wugu, Taipei County, Taiwan] medical device)for the daily activity of self-care. Devices are managedthrough a free software environment. Color images availableonline at www.liebertonline.com/dia.
718 VARGAS-LOMBARDO ET AL.

(glucose, blood pressure, body mass index, and other aspectsof self-care).
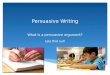
Meanwhile, in the implicit output lies the automatic processof medical protocols and the health services that enable closingthe implicit relationship. As can be seen in Figure 2, graphicsinterfaces are responsible for hiding underlying technology
from the patient’s senses and his or her environment. Figure 3shows the concepts structure for the hiPAPD model.
These interfaces must be adaptive. They must demonstratethe ability to adapt immediately to a patient’s physical andpsychological context in real time. The patient should feel thathe or she controls the system through user interface graphics,
FIG. 3. Main features of the holistic, interactive, and persuasive model to facilitate self-care of diabetes patients. Colorimages available online at www.liebertonline.com/dia.
FIG. 2. A patient with diabetes using the web service 2.0 of the holistic, interactive, and persuasive model to facilitate self-care of diabetes patients model, managing his information. GUI, user interface graphics; ICT, information and communi-cation technology. Color images available online at www.liebertonline.com/dia.
SELF-CARE OF THE DIABETES PATIENT (HIPAPD) 719

and this is possible with the touch screen provided by the tabletPC. The patient should immediately feel at the touch of thescreen the element in the interface with which he or she wantsto be in contact, or to interact in the most natural way possibleonce he or she uses the touch the tablet PC’s touch screen.
The Patient with Diabetes and His or HerSelf-Care Surroundings
An interactive and persuasive holistic model (hiPAPD) hasbeen developed and implemented to facilitate self-care of
Table 1. Improvement of Patients with Use of the Holistic, Interactive, and Persuasive Model
to Facilitate Self-Care of Diabetes Patients Model
Patients improve with hiPAPD in each region
Barrios Unidos Pocrı Aguadulce Cabecera
Question I agree I disagree I agree I disagree I agree I disagree
1. Do you consider your health has improved? 74.07% 25.93% 88.89% 11.11% 77.14% 22.86%2. If your blood sugar level is affecting your health,would you follow the instructions given byyour doctor through this program?
77.78% 22.22% 77.78% 22.22% 71.43% 28.57%
3. If your hypertension levels are affecting your health,would you follow the instructions given by yourdoctor through this program?
77.78% 22.22% 86.67% 13.33% 82.86% 17.14%
4. If your levels of HDL/LDL are affecting your health,would you follow the instructions given by your doctorthrough this program?
70.37% 29.63% 77.78% 22.22% 77.14% 22.86%
5. If your cholesterol/triglyceride level is affecting yourhealth, would you follow the instructions given byyour doctor through this program?
70.37% 29.63% 86.67% 13.33% 85.71% 14.29%
6. If your keratinized triglyceride level is affecting yourhealth, would you follow the instructions given by yourdoctor through this program?
74.07% 25.93% 91.11% 8.89% 88.57% 11.43%
7. If your body mass index is affecting your health, wouldyou follow the instructions given by your doctorthrough this program?
62.96% 37.04% 88.89% 11.11% 77.14% 22.86%
HDL, high-density lipoprotein; hiPAPD, holistic, interactive, and persuasive model to facilitate self-care of diabetes patients; LDL, low-density lipoprotein.
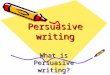
FIG. 4. Glycemic indexes of the patients with diabetes before participating in the environment of the holistic, interactive,and persuasive model to facilitate self-care of diabetes patients model. Color images available online at www.liebertonline.com/dia.
720 VARGAS-LOMBARDO ET AL.

patients with diabetes types 1 and 2. The patients require dailyactivities of individual attention and care for themselves. Thesolution proposed requires such adaptive processes of tech-nologies as combined glucometer and blood pressure monitor(embedded two in one), Bluetooth� (Bluetooth SIG, Kirkland,WA)-enabled weight scale, Bluetooth-enabled pedometer,and tablet PC with system software on the patient with thehighest level of ubiquity in them. This means the systemshould be designed and built for the patient, with high-qualityusable and interactive interfaces, which represents a greatchallenge forresearchers.However, this integrationisachievedthrough the model presented and the implementation of themodel through the hiPAPD system web services 2.0.
The system being built through the model consists of webservices that manage devices and sensors that interact aroundthe context of the patient with diabetes. Yet more advanced inthe process of ubiquity of the hiPAPD system, the modelmanages self-care of the diabetes patient, by activating thefamily of the patient, friends of the patients, doctors, medicalworkforce, and society contexts. This entails that these par-ticipants and situations that occur around the patient withdiabetes are fully monitored and that the patient is notabandoned to his or her fate. From the tablet PC informationinputs are received from devices and sensors relative to thepatient with diabetes, for example, blood pressure, weightscale, calories consumed (pedometer) and blood sugar (gluc-ometer). Similarly, self-care involves offering new services forthe patient with diabetes in their contexts; some of these ser-vices are:
� Recording of medications, tests (high-density lipopro-tein, low-density lipoprotein, cholesterol, triglycerides,creatinine, and other tests)
� Information about new treatments and care of the skin,eyes, mouth, and feet
� Information and test on stress management, anxiety,and depression
� Monitoring of the diabetes patient’s condition at all timesby family members and medical and health personnel
� Establishment of social networks and virtual commu-nities for the exchange of experiences and motivationalsupport for the patients and their families from otherdiabetes patients with the same pathological condition
� Forums to facilitate the exchange ideas and truthful andtimely information on the prevention and detection ofdiabetes, aimed at a society that does not have knowl-edge of the diabetes pandemic and all its problems
� Alarm services for situations as high glycemia and highor low blood pressure, as well as the case of abnormalhigh-density lipoprotein, low-density lipoprotein, cho-lesterol, or triglyceride or high creatinine
All these services are geared to facilitate self-care of patientswith diabetes, through the hiPAPD model, allowing thefamily of the patient, friends of the patient, and medical andhealth staff contexts be integrated into the system.
Validation of the hiPAPD Model
In determining the prevalence of diabetes mellitus andsome risk factors associated with the population over 25 yearsold, three health centers in the District of Aguadulce, Provinceof Cocle, located on Panama’s Pacific Coast, were selected; thearea presents clear socioeconomic conditions of extremepoverty, with at least one-daily meal diet, without any healthinsurance, and with a high illiteracy rate.
A transversal analytical study was conducted during themonths of June–October 2009. The sample comprised 107 in-dividuals of both sexes from a total of 15,000 people over 25years old, selected from a probabilistic sampling of a mono-etapic cluster, the research and sampling unit of the poor areasof Barrios Unidos, Pocrı, and Aguadulce.
A prevalence of diabetes mellitus type 2 of 95.54% and ofdiabetes mellitus type 1 of 0.046% was found; also, the type 2prevalence among males was 44.1% and among females was
FIG. 5. Glycemic indexes of the patients with diabetes after taking part in the holistic, interactive, and persuasive model tofacilitate self-care of diabetes patients model environment. Color images available online at www.liebertonline.com/dia.
SELF-CARE OF THE DIABETES PATIENT (HIPAPD) 721

55.8%. On the other hand, the prevalence of diabetes mellitustype 1 in males was 40% and in females was 60%. An analysisof the reason for prevalence of risk factors studied shows thatthe presence of family history is statistically significant(30.84%) for the appearance of diabetes mellitus types 2 and 1;in addition, factors such as obesity (9.35%), deficient feeding(33.64%), physical inactivity (7.48%), and high blood pressure(18.69%) were detected.
Table 1 shows the importance that new information tech-nologies bring to the health of patients of the three marginalgroups studied. Many of the diabetes patients perceived thatthe hiPAPD model environment has facilitated the control oftheir blood sugar and improved their quality of life.
The results shown in Table 1 are very encouraging becausethey show in both groups of patients that the environment hashelped them to take care of their health and the environmentcan help them understand the health activities they must thusdevelop daily. On the other hand, patients expressed that theparticipants in their family, their friends, and society in thehiPAPD model help them take care of their health. The threeglycemic index groups were studied before and after the hi-PAPD model was applied.
As seen in Figures 4 and 5, blood sugar levels dropped,once the patient has been integrated to the hiPAPD environ-ment, which is satisfactory for this experiment.
Conclusions
This project is part of a pioneer initiative for CentralAmerica and the Caribbean Region, in the context of pro-viding free and high-quality health services through newICTs, using as an example the population of diabetes patientsthat is increasingly growing in Panama. Panama is the startingpoint of this ICT platform for self-care of patients with chronicdiseases, and the success of the progress will be marked by itssocial acceptance and its integration into the public healthsystem in Panama. It is also of great satisfaction that the socialgroups that supported us in this validation process experi-enced new technologies for their benefit. Finally, the ICTservices proposed will facilitate diabetes education, self-care,and prevention and will integrate the environment of diabetespatients and their families.
Further Work
As a follow-up to this project, the researchers are proposingto continue the study in other rural and urban areas (centralprovinces such as Los Santos, Herrera, Veraguas, Cocle, andPanama City). In addition, contacts have been made in Cen-
tral America and Caribbean with clinics and hospitals in ruralzones, to start developing a pilot study in the use of the hi-PAPD model.
Author Disclosure Statement
No competing financial interests exist.
References
1. Vargas-Lombardo M, Jipsion A, Arrendondo MT: A frame-work for the quality of data in data grid systems for virtualorganizations. In: Arabnia HR, Gravvanis GA, eds. Proceed-ings of the 2009 International Conference on Grid Computing& Applications, GCA 2009, July 13–16, 2009, Las Vegas Ne-vada, USA. CSREA Press, Las Vegas, 2009:59–64.
2. World Health Organization: Primary Health Care—NowMore Than Ever. The World Health Report. Geneva: WorldHealth Organization, 2008.
3. Vinter-Repalust N, Petricek G, Katic M: Obstacles which pa-tients with type 2 diabetes meet while adhering to the ther-apeutic regimen in everyday life: qualitative study. CroatMed J 2004;45:630–636.
4. Warshaw HS, Pape J: Real-Life Guide to Diabetes. Alexan-dria, VA: American Diabetes Asociation, 2006.
5. Fogg BJ: Persuasive Computers: Perspectives and ResearchDirections. New York: ACM Press/Addison-Wesley Pub-lishing Co., 1997. doi.acm.org/10.1145/274644.274677.
6. Fogg BJ, Marshall J, Laraki O, Osipovich A, Varma C, Fang N,Paul J, Rangnekar A, Shon J, Swani P, Treinen M: Elementsthat affect web credibility: early results from a self-reportstudy. In: Proceedings of ACM CHI 2000 Conference onHuman Factors in Computing Systems, Vol. 2. New York:ACM Press, 2000:287–288.
7. Norman DA: Emotional Design: Why We Love (or Hate)Everyday Things. Barcelona: Ferran Meler Orti, EdicionesPaidos, 2003.
8. Demir E, Desmet PMA: Roles of products in product emo-tions: an explorative study. In: Undisciplined! Design Re-search Society 2008 Conference. shura.shu.ac.uk/504/(accessed June 9, 2010).
9. Demir E, Desmet PMA, Hekkert P: Appraisal patterns ofemotions in user-product interaction. Int J Des 2009;3(2):41–51.
Address correspondence to:Miguel Vargas-Lombardo, Ms.C.
P.O. Box 029009#PTY 36366
Miami, FL 33102-9009
E-mail: [email protected]
722 VARGAS-LOMBARDO ET AL.