Embed Size (px)
Citation preview

I. Purpose The purpose of this module is to provide information and skills necessary to engage in community prevention activities.
II. Learning ObjectivesAt the end of the training, the health care professional will have had an opportunity to: Define community-based prevention. Discuss types and levels of prevention. Compare frameworks for preventive interventions. Identify risk and protective factors associated with substance use disorders. Cite theories of behavioral change. Discuss cultural influences on prevention. Define the role of the health professional in prevention. Discuss general and specific strategies for community-based prevention. Identify evaluation aims for community-based programs.
III. Chronology Approximately 1 Hour 30 Minutes Introduction and objectives 5 Minutes Definitions, types and levels of prevention 15 MinutesFrameworks for preventive interventions 15 MinutesPrevention principles 10 MinutesRisk and protective factors and resiliency 15 MinutesRole of health practitioner 5 Minutes
Designing effective prevention programs, theories of change, cultural competence, general and specific strategies, evaluation 20 Minutes Summary and evaluation 5 Minutes
IV. Facilitator Materials Power Point Slides (lecture and discussion)
V. Participant Materials Handouts References
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
1
Module IX: Community-Based Substance Abuse Prevention

Module IX: Community-Based Substance Abuse Prevention
Slide 1: Title Slide - Community-Based Substance Abuse Prevention IntroductionThis is the title slide.
Slide 2: Learning ObjectivesHealth Care Professionals will have the opportunity to:
Define community-based prevention. Discuss types and levels of prevention. Compare frameworks for preventive interventions. Identify risk and protective factors associated with substance use disorders. Cite theories of behavioral change. Discuss cultural influences on prevention.
Slide 3: Learning Objectives (continued) Health Care Professionals will be able to:
Define the role of the health care professional in prevention. Discuss general and specific strategies for community-based prevention. Identify evaluation aims for community-based prevention programs.
Slide 4: Introduction There are compelling reasons why community-based prevention of substance use and abuse should be a major focus for all health professionals. The combined effects of tobacco, alcohol, and other drugs take a greater toll on the health and well-being of Americans than any other single preventable health problem. While the Monitoring the Future (MTF) (2004) survey indicates an almost 7 percent decline from 2003 to 2004 of any illicit drug use in the post month by 8th, 10th, and 12th grades, other areas raise of drug use concern. There was a significant increase in OxyContin use by adolescents during this period and lifetime inhalant use for 8th graders also increased significantly. NIDA’s Community Epidemiology Work Group (CEWG) publishes emerging trends in drug abuse for 21 major U.S. metropolitan areas. The CEWG data for 2002 indicate that cocaine/crack was endemic in all of the areas, heroin indicators continued to be high, prescription opiates appear increasingly in drug indicator data, methamphetamine abuse continues to spread and marijuana is the most frequently used illicit drug in CEWG areas. (Community Epidemiology Work Group, 2003). Studies indicate that 119 million Americans (50.1% aged 12 or older were current alcohol users in 2003 and 70.8 million (29.8%) Americans 12 or older were current smokers during that time (Substance Abuse Mental Health Services Administration, 2004). As indicated by these data substance use disorders occur across the lifespan, so preventive interventions must be targeted for individuals at risk in all age groups. Such interventions should take into consideration the unique developmental tasks of each age group and the risk and protective factors that influence the health behaviors of individuals and communities. According to Perry, “the question in prevention is not why but how” (Perry, 1996). Individuals of all ages are members of communities and there is increasing evidence that the most effective prevention strategies are community-based (Burgoyne, 1991). Moreover, the underlying premise of Healthy People 2010 is that the health of the individual is almost inseparable from the health of the larger community, the state, and the nation (U.S. Department of Health and
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
2

Human Services, 2000). The role of the health professional is to join with community stakeholders to increase the capacity of the community to provide science-based preventive interventions (Marcus, 2000, Chinman, et al 2005; Spoth & Greenberg, 2005). This module provides an overview of community-based prevention: definitions, levels of prevention, selected frameworks and strategies for designing community-based prevention, a summary of the literature related to risk and protective factors, and a brief outline of the role of the health professional in these endeavors.
Slide 5: Definition of PreventionPrevention literally means to keep something from happening. There are, however, different interpretations about what that “something” is; first incidence, frequent use, heavy use, relapse, disability associated with a disorder, or the risk condition itself. According to Pentz (1999), the broadest interpretation related to substance abuse disorders is “blocking the progression of use to abuse, whether in adults or youth.” Defined in strictest terms prevention refers to preventing onset of any use. Because this may not be realistic, clinicians and researchers define preventive interventions as “any program that has as its goal either delay of onset, delay of progression from lower to higher use prevalence (frequency) or consumption (amount) or decrease in use prevalence and consumption” (Pentz, 1999, p 535). The Center for Substance Abuse Prevention (CSAP) definition of prevention states that it is “a proactive process that empowers individuals and systems to meet the challenge of life events and transitions by creating and reinforcing conditions that promote healthy behaviors and lifestyles” (CSAP, 1994). Early prevention activities, primarily education, focused on the individual rather than the environment. Prevention science is now understood to be far more complex and to involve integration of epidemiological, etiological and preventive intervention research. Prevention can be defined holistically as an anticipatory process that prepares and supports individuals, families, communities, and systems in the creation and reinforcement of health behaviors and lifestyles and the conditions that promote them.
Slide 6: Prevention Activities ClassifiedPreventive interventions are classified by approach to drug abuse control (demand vs. supply reduction), level of prevention (universal, selective, indicated) and focus (direct focus on drug use resistance and harm reduction vs. indirect focus on life skills and building protective factors).
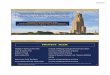
In the traditional public health conceptualization of levels of prevention (primary prevention is targeted at protecting individuals who have not yet begun to use substances, secondary prevention (or early intervention) targets persons in early stages of substance abuse to reduce and/or eliminate use, and tertiary prevention (treatment) seeks to end dependency and addiction and/or ameliorate the negative effects of substance use (Commission on Chronic Illness, 1957; CSAP, 1991). Since this 1957 public health classification of levels of prevention was formulated, there is new appreciation for the complex interplay between and among environmental, cognitive, physical, psychological, social and spiritual factors and health outcomes. A second framework has been used since 1990 to supplement the initial public health classification. That framework, embedded in the Mental Health Intervention Spectrum (Figure 1), categorizes interventions as: universal (delivered to the general population), selective (targeted for “at risk” populations), and indicated (aimed at high risk
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
3

individuals who may have minimal but detectable signs or symptoms of the disorder) (Gordon, 1983; Mrazek & Haggerty, 1994).
Slide 7: Mental Health Approach to Prevention Universal Preventive Intervention is prevention that is desirable for everyone in eligible population. Selective Preventive Intervention is targeted for individuals or subgroups at significantly higher risk than average. Indicated Preventive Intervention is targeted for high-risk individuals with minimal but detectable signs/symptoms.
School education programs conducted by teachers or peers are examples of universal prevention strategies. Similarly, programs that provide opportunities for seniors to remain active in the community would be classified as universal. Individual and group counseling and support groups for youth who are having academic problems or experiencing family or peer difficulties is classified as selective prevention. Education programs about drug interactions and drug and alcohol interactions for seniors taking multiple prescriptions are selective prevention strategies. Indicated prevention strategies focus on youth who exhibit problems such as gang involvement, truancy, criminal activity and conduct disorder.Indicated prevention strategies for the elderly would target individuals who have beginning signs of substance use disorders such as falls or signs of neglect associated with alcohol use.
Slide 8: The Mental Health Intervention Spectrum
Figure 1: The Mental Health Intervention Spectrum
Slide 9: Examples of Research-Based Drug Prevention Programs Specific Examples of Research-Based Drug Prevention Programs for Youth Using These Classifications include:
Life Skills Training (Botvin et al., 1990). A universal classroom program which addresses a wide range of risk and protective factors by teaching 1) drug resistance skills and information, 2) self-management skills, and 3) general social skills.
Project STAR (Pentz et al., 1989). A universal prevention program that reaches the entire community with a comprehensive school program, mass media efforts, a parent program, community organization, and health policy change.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
4
Universal
Selective
Indicated
After-care(Including Rehabilitation)
Compliance withLong-term Treatment(Goal: Reduction inRelapse and Recurrence)
Standard Treatment forKnown Disorders
CaseIdentification
PreventionMaintenance
Treatment

Strengthening Families Program (Kumpfer et al., 1996). A selective multi-component, family-focused program that involves parent training, children’s skills training and family skills training.
Reconnecting Youth Program (Eggert et al., 1994; 1995). An indicated prevention program for youth in grades 9 through 12 with poor school achievement and potential for dropping out. (This includes personal growth class, social activities and school bonding, and a school system crisis response plan.)
(Preventing Drug Use … 1997)
Slide 10: Approaches to Community-Based PreventionAlthough the science of community-based prevention is in its infancy, there are testedapproaches, with corresponding frameworks, to guide program planners. Three frameworks are provided below as examples. They are the Prevention Intervention Research Cycle (Mrazek & Haggerty, 1994), the PRECEDE-PROCEED Model (Green & Kreuter, 1999), and the SAMHSA Prevention Platform. Two distinct, though not antithetical, perspectives on prevention inform the frameworks (National Institute on Alcohol Abuse and Alcoholism, 2000). One a clinical perspective, derived from medicine and psychotherapy, focuses on individual factors and lifestyle issues. From the clinical perspective, community may be defined as a media market that can be reached via messages aimed at individual behavior changes in a general population. The public health, or environmental, perspective derived from epidemiology, and the social sciences, focuses on law, policies, and practices that affect production, distribution, sales, marketing, or behaviors. Prevention work from the public health perspective is done through licensing authorities and community institutions rather than the general population. The two approaches are not competitive but may be integrated to provide comprehensive programs (National Institute on Alcohol Abuse and Alcoholism, 2000; Curry & Kim, 1999). Comprehensive community-based prevention programs focus on both demand and supply aspects of substance use. (Windle, 1999). As an example, Project Northland, an alcohol-specific, multi-component prevention program for young adolescents, includes strategies for individuals and strategies to change laws and policies (Perry et al., 1996; Perry, 1999; Windle, 1999; National Institute on Alcohol Abuse and Alcoholism, 2000). Project Northland consists of school-based curricula, aimed at individual behavior change; parental involvement and education programs; peer leadership opportunities; community task forces and action teams; and a mass media campaign. The program outcomes included decreased alcohol use at the end of 3 years, for early adolescents, and decreased smoking and marijuana use among baseline nonusers (Perry, 1999). Other studies have not yielded such positive results. A large fifteen year study, using the social-influences approach to school-based smoking prevention for youth, reported no long-term deterrence ofsmoking among the participants (Peterson et al., 2000). Because prevention science is in its infancy, full-scale community studies such as Project Northland should be complemented with smaller studies to determine potentially powerful interventions and the best way to deliver those interventions (National Institute on Alcohol Abuse and Alcoholism, 2000) Elements of both the clinical and public health perspectives are evident in the following frameworks or models suggested for planning preventive interventions.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
5

Slide 11: Frameworks for Community-Based PreventionThe Preventive Intervention Research Cycle provides one basic framework for prevention research. The Preventive Intervention Research Cycle, like the Mental Health Intervention Spectrum described in the preceding section, is an outcome of the work of the Committee on Prevention of Mental Disorders. The Committee was appointed by the Institute of Medicine in 1992 in accordance with an agreement with the National Institute of Mental Health. In 1994 the Committee published Reducing Risks for Mental Disorders: Frontiers For Preventive Intervention Research (Mrazek & Haggerty, 1994), a comprehensive guide to the prevention process with recommendations for developing the infrastructure, conducting the research, and gaining the knowledge necessary for preventive interventions in mental health and substance abuse. The Precede-Proceed Model and SAMHRS Prevention Platform are two other useful models
Slide 12: Prevention Intervention Research CycleThe first and second boxes of the cycle call for review of information from many different fields of health research. Boxes three and four speak specifically to the research endeavor. The fifth box depicts the shift from research project to community service program with ongoing evaluation. The feedback loop indicates as exchange of information between and among researchers and community practitioners that should occur throughout the cycle. A suggested worksheet to accompany the Preventive Intervention Research Cycle is provided in Figure 3. This framework has been used for many intervention programs designed for individuals of all ages from infants to the elderly (Mrazek & Haggerty, 1994, 506-511).
Slide 13: PRECEDE – PROCEED ModelThe PRECEDE - PROCEED Model for health promotion provides another framework for approaching community-based prevention (Figure 4) . This comprehensive framework is founded on the disciplines of epidemiology; the social, behavioral, and educational sciences; and health administration. Two propositions are fundamental to the framework: (1) health and health risks are caused by multiple factors; and (2) efforts to effect behavioral, environmental, and social change must be multidimensional or multisectoral (Green & Kreuter, 1999). The framework has two components: (1) a diagnostic or needs assessment phase (PRECEDE, predisposing, reinforcing, and enabling constructs in educational/environmental diagnosis and evaluation) and (2) a developmental stage of health promotion planning that follows the diagnostic assessment and initiates the implementation and evaluation process (PROCEED, policy, regulatory, and organizational constructs in educational and environmental development) (Green & Kreuter, 1999). Unique to this framework is the initial focus on outcomes rather than inputs. The premise is that factors important to the outcome must be diagnosed before the intervention is designed or the intervention may be misdirected (Green and Krauter, 1999).The PRECEDE – PROCEED Model has nine phases:
Phase 1 Social assessment: Consideration of quality of life by determiningsubjectively defined problems of individuals and communities.
Phase 2 Epidemiological assessment: Identification of specific health goals or problems that may contribute to social goals (disability, discomfort, fertility, fitness, morbidity, mortality, physiological risk factors).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
6

Phase 3 Behavioral and environmental assessment: Identification of behavioral factors(compliance, consumption patterns, coping, preventive actions, self care, utilization) and environmental factors (economic, physical, services, social).
Slide 14: PRECEDE – PROCEED Model (continued)Phase 4 Educational and organizational assessment: Identification of predisposing
factors (knowledge, attitudes, beliefs, values, perceptions), reinforcing factors, attitudes and behavior of health and personnel, peers, parents, employers andenabling factors (availability of resources, accessibility, referrals, rules, laws,skills).
Phase 5 Administrative and policy assessment: Assessment of organizational andadministrative capabilities and resources for development and implementation of a program.
Phase 6,7,8 9 Implementation and process, impact and outcome evaluation.
Developed initially as an evaluation model, the PRECEDE-PROCEED framework has evolved into a comprehensive model for planning, implementing and evaluating community-based preventions. For further discussion and details of the model see Green and Kreuter (1999). There is a software training tool (EMPOWER) and a supportive environment for guidance (NETPOWER) available as technological support for the PRECEDE – PROCEED Model. See http:www.ihpr.ubc.ca/preapps.html for examples of applications of this framework.
Slide 15: Substance Abuse Mental Health Services Administration (SAMHSA) Prevention PlatformThe SAMHSA Prevention Platform is an online resource designed to assist professionals and community volunteers to engage in substance abuse prevention. The framework includes the following areas:
Assessment – determining your prevention needs. Capacity – improving your capabilities. Planning – developing a strategic plan. Implementation – putting your plan into action. Evaluation – documenting the outcomes of your work.
Http://preventionplatform.samhsa.gov
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
7

Slide 16: Model
Slide 17: Lessons from Prevention ResearchThe National Institute on Drug Abuse (NIDA) has summarized the results of long-term research studies on the origins of drug abuse behaviors and common elements of effective prevention to arrive at sixteen evidence-based principles. (http://www.nida.nih.gov/infofacts/lesson.html).
Slide 18: Principle 1Prevention programs should enhance protective factors and reverse or reduce risk factors (Hawkins et al. 2002).
The risk of becoming a drug abuser involves the relationship among the number and type of risk factors (e.g., deviant attitudes and behaviors) and protective factors (e.g., parental support) (Wills et al. 1996).
The potential impact of specific risk and protective factors changes with age. For example, risk factors within the family have greater impact on a younger child, while association with drug-abusing peers may be a more significant risk factor for an adolescent (Gerstein and Green 1993; Dishion et al. 1999).
Early intervention with risk factors (e.g., aggressive behavior and poor self-control) often has a greater impact than later intervention by changing a child’s life path (trajectory) away from problems and toward positive behaviors (Ialongo et al. 2001).
While risk and protective factors can affect people of all groups, these factors can have a different effect depending on a person’s age, gender, ethnicity, culture, and environment (Beauvais et al. 1996; Moon et al. 1999).
Slide 19: Principle 2Prevention programs should address all forms of drug abuse, alone or in combination, including the underage use of legal drugs (e.g., tobacco or alcohol); the use of illegal drugs (e.g., marijuana or heroin); and the inappropriate use of legally obtained substances (e.g., inhalants), prescription medications, or over-the-counter drugs (Johnston et al. 2002).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
8

Slide 20: Principle 3Prevention programs should address the type of drug abuse problem in the local community, target modifiable risk factors, and strengthen identified protective factors (Hawkins et al. 2002).
Slide 21: Principle 4Prevention programs should be tailored to address risks specific to population or audience characteristics, such as age, gender, and ethnicity, to improve program effectiveness (Oetting et al. 1997).
Slide 22: Principle 5Family-based prevention programs should enhance family bonding and relationships and include parenting skills; practice in developing, discussing, and enforcing family policies on substance abuse; and training in drug education and information (Ashery et al. 1998).
Family bonding is the bedrock of the relationship between parents and children. Bonding can be strengthened through skills training on parent supportiveness of children, parent-child communication, and parental involvement (Kosterman et al. 1997).
Parental monitoring and supervision are critical for drug abuse prevention. These skills can be enhanced with training on rule-setting; techniques for monitoring activities; praise for appropriate behavior; and moderate, consistent discipline that enforces defined family rules (Kosterman et al. 2001).
Drug education and information for parents or caregivers reinforces what children are learning about the harmful effects of drugs and opens opportunities for family discussions about the abuse of legal and illegal substances (Bauman et al. 2001).
Brief, family-focused interventions for the general population can positively change specific parenting behavior that can reduce later risks of drug abuse (Spoth et al. 2002b).
Slide 23: Principle 6Prevention programs can be designed to intervene as early as preschool to address risk factors for drug abuse, such as aggressive behavior, poor social skills, and academic difficulties (Webster-Stratton 1998; Webster-Stratton et al. 2001).
Slide 24: Principle 7Prevention programs for elementary school children should target improving academic and social-emotional learning to address risk factors for drug abuse, such as early aggression, academic failure, and school dropout. Education should focus on the following skills (Conduct Problems Prevention Research Group 2002; Ialongo et al. 2001):
Slide 25: Principle 7 (continued) self-control; emotional awareness; communication; social problem-solving; and academic support, especially in reading.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
9

Slide 26: Principle 8Prevention programs for middle or junior high and high school students should increase academic and social competence with the following skills (Botvin et al. 1995; Scheier et al. 1999):
Slide 27: Principle 8 (continued) study habits and academic support; communication; peer relationships; self-efficacy and assertiveness; drug resistance skills; reinforcement of anti-drug attitudes; and strengthening of personal commitments against drug abuse.
Slide 28: Principle 9Prevention programs aimed at general populations at key transition points, such as the transition to middle school, can produce beneficial effects even among high-risk families and children. Such interventions do not single out risk populations and, therefore, reduce labeling and promote bonding to school and community (Botvin et al. 1995; Dishion et al. 2002).
Slide 29: Principle 10Community prevention programs that combine two or more effective programs, such as family-based and school-based programs, can be more effective than a single program alone (Battistich et al. 1997).
Slide 30: Principle 11Community prevention programs reaching populations in multiple settings—for example, schools, clubs, faith-based organizations, and the media—are most effective when they present consistent, community-wide messages in each setting (Chou et al. 1998).
Slide 31: Principle 12When communities adapt programs to match their needs, community norms, or differing cultural requirements, they should retain core elements of the original research-based intervention (Spoth et al. 2002b), which include:
Structure (how the program is organized and constructed); Content (the information, skills, and strategies of the program); and Delivery (how the program is adapted, implemented, and evaluated).
Slide 32: Principle 13Prevention programs should be long-term with repeated interventions (i.e., booster programs) to reinforce the original prevention goals. Research shows that the benefits from middle school prevention programs diminish without follow-up programs in high school (Scheier et al. 1999).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
10

Slide 33: Principle 14Prevention programs should include teacher training on good classroom management practices, such as rewarding appropriate student behavior. Such techniques help to foster students’ positive behavior, achievement, academic motivation, and school bonding (Ialongo et al. 2001).
Slide 34: Principle 15Prevention programs are most effective when they employ interactive techniques, such as peer discussion groups and parent role-playing, that allow for active involvement in learning about drug abuse and reinforcing skills (Botvin et al. 1995).
Slide 35: Principle 16Research-based prevention programs can be cost-effective. Similar to earlier research, recent research shows that for each dollar invested in prevention, a savings of up to $10 in treatment for alcohol or other substance abuse can be seen (Aos et al. 2001; Hawkins et al. 1999; Pentz 1998; Spoth et al. 2002a).
Slide 36: Risk and Protection FactorsThe Preventive Intervention Research Cycle and the evidenced-based principles incorporate information on risk and protective factors. While there has been extensive research on identification of risk and protective factors, particularly for adolescent substance use, some issues remain to be addressed in future studies in order to optimize the value of this literature. One issue is the need to recognize the dynamic bidirectional interactions between risk and protective factors and problem behaviors. For the individual, these factors may vary according to age, psychosocial development, ethnic/cultural identify and environment (Windle, 1999; Mrazek & Haggerty, 1994). Risk and protective factors may be identified as antecedents or buffers to better convey the dynamic nature of their relationship to behaviors. See Simoneau and Bergeron (2000) for an etiologic model of alcoholism, from a developmental ecological perspective that postulates risk and protective factors across the lifespan. Scientific understanding of risk and protective factors is in its infancy so a word of caution is necessary. Module 6 presents additional information on this topic as it relates to children of alcoholic parents. Recent studies grounded on assessment of risk and protective factors provided evidence for this approach to prevention (Sanders, 2000; Wallace & Muroff, 2002; Marcus et al, 2004; Orlando et al, 2005; Murray & Belenko, 2005).
Slide 37: Risk FactorsRisk factors have been defined as characteristics that occur more often for those who develop substance use problems (Hawkins et al, 2004). They are indicators for potential problem occurrence or vulnerability. The more risk factors children experience, the more likely it is that they will experience substance use disorders and related problems in adolescence or young adulthood.
Slide 38: Protective FactorsProtective factors on the other hand are not merely the absence of or opposite of risk factors, but the presence of positive influences that help protect a person from developing substance use problems (NIAAA, 1990). They balance and buffer risk factors (Hawkins et al., 2004).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
11

Slide 39: Resilience When all areas of a young person’s life support healthy development and promote resilience, young people are more likely to withstand the negative influences and risks to which they will inevitably be exposed. Garmezy has defined resilience (Hazelden, 1996) as an absence of deviant outcomes regardless of exposure to risk. Wolin and Wolin (1995) define it as successful adaptation despite risk and adversity.
Slide 40: Six Life AreasRisk and protective factors can be grouped by life areas. In one very straightforward theoretical framework of substance use, six life domains—individual, peer, family, school, community, and society – are used. It is important to note that these domains interact with the individual placed at the core of the model, and that all stimuli are processed, interpreted, and responded to based upon those characteristics that the individual brings the situation.
Knowledge about specific risk factors, as noted by Hawkins et al., 2004, is crucial in preventing substance use disorders and related problem behaviors. Further, they indicate that although levels of risk may vary from one community and ethnic/cultural group to another, effects of risk factors are fairly consistent across races, cultures, and social classes.The literature on protective factors and resilience is more diffuse than for risk factors, and there is less clarity about which factors are most important in the prevention of substance use disorders. Nevertheless, a growing sense exists that certain protective factors are critically important. Following is an overview of types of risk and protective factors.
SLIDES 41 through 45 describe Individual/Personal Risk and Protective Factors
Slide 41: Risk FactorsIndividual/Personal. Many of the most important personal/individual risk factors can be categorized as unmodifiable. These include genetic predispositions toward alcohol use (CSAP, 1993, p 8) and age and gender. Over the years research on twins and adoptees has shown strong genetic influence especially in males whose fathers have alcohol use disorders. The earlier the age at onset of substance use, the greater the risk for later substance-related problems (Kandel, 1982; Grant and Dawson, 1998). More amenable to change are personal attitudes and predispositions related to drug use, especially an individual’s perception of risk (Brounstein et. al., 1989).
Slide 42: Risk Factors (continued)Individual/Personal. Other predispositions include increased levels of impulsivity, hostility, or disinhibition; increased alienation from the dominant values of society; and greater levels of rebelliousness (CSAP, 1993, p. 7). Prevention programs often aim at correcting or overcoming deficits in social skills. Principal among these are early aggressive behavior (Hawkins et al., 1988) and alienation (CSAP, 1993, p. 9).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
12

Slide 43: Risk Factors (continued) Individual/Personal. Also closely linked with substance use and abuse among youth are related problem behaviors such as juvenile delinquency, violence, teen pregnancy, and dropping out of school (Hawkins et al., 1992).
Slide 44: Protective FactorsIndividual/Personal. CSAP’s review of the individual domain (CSAP, 1993, p. 13) identifies three primary categories of protective factors:
Positive temperament characteristics, which include social skills and social responsiveness, cooperativeness, emotional stability, positive sense of self, flexibility, problem-solving skills, and low levels of defensiveness.
An emotionally supportive parental/family milieu, including parental attention to children’s interests, attachment to parents, orderly and structured parent-child relationships, and parent involvement in homework and school-related activities.
Supportive societal institutions that reinforce the child’s coping efforts, elements of which include parental identification and satisfaction, commitment to school, regular involvement in church, and belief in society’s values.
Less easily definable, but perhaps just as important, is social competence, including having good communication skills, responsiveness, empathy, caring, a sense of humor, and an inclination toward prosocial behavior (Elias et al., 1997). Social competence also includes problem-solving skills, a strong sense of autonomy and independence, and a sense of purpose and of the future, e.g., goal-directness
Slide 45: Protective Factors (continued)Individual/Personal. There are also genetic/biomedical factors. These can be described with the following example:
Genetically controlled variation of aldehyde hydrogenase (ALDH2), called ALDH2-2, in 10% of Asians creates intense reaction to alcohol.
Lower alcoholism risk is also associated with genetically controlled variants of alcohol dehydrogenase (ADH2, ADH3) in Asians and several other ethnic groups.
SLIDES 46 through 48 describe Family Risk and Protective Factors
Slide 46: Risk FactorsFamily. From the prenatal stage through late childhood, the family--parents, caregivers or parent surrogates, siblings, and close relatives--is the main influence in the development of children and youth, and it is also the crucible in which problem behaviors are shaped. Kumpfer (1993) has observed, for example, that remaining in an abusive or conflict-ridden family is far more detrimental to children than divorce. Kumpfer also notes that, according to research, marital discord is a stronger predictor of delinquency than family structure (such as a single-parent family). Other major family risk factors include:
Economic deprivation; Reduced supervision; Formal controls and social supports;
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
13

Living in impoverished neighborhoods characterized by high crime rates and alienation;
Differential family acculturation;
Slide 47: Risk Factors (continued)Family. Poor family management, discipline, and problem solving practices are also important factors. (Kumpfer, 1993; Hawkins et al., 1992). Also important in predicting substance use among youth is parental use of alcohol and drugs and both parental permissiveness and positive attitudes toward alcohol and drugs (Hawkins et al., 1988).
Slide 48: Protective Factors Family. Perhaps the single most important family-related protective factor is positive bonding within the family setting. As Warner (1990) observed, “despite the burden of parental psychopathology, family discord or chronic poverty, most children identified as resilient have had the opportunity to establish a close bond with at least one person who provided them with stable care and from whom they received adequate and appropriate attention during the first year of life” (quote in Bernard, 1991, p. 6). Other key family protective factors include:
High levels of warmth and absence of severe criticism (Rutter, 1979). A sense of basic trust (Erickson, 1950/1985). High parental expectations (Bernard, 1990). Clear rules and expectations for children, including children’s participation in
family chores and responsibilities (Hawkins et al., 1992).
SLIDES 49 and 50 describe School Risk and Protective Factors
Slide 49: Risk Factors School. One of the strongest predictors of substance use and related problem behavior is school failure (CSAP, 1993, p. 11; Hawkins et al., 1988). Some school-related factors are believed to exacerbate preexisting problems and dispositions. Principal among these are:
Negative, disorderly, and unsafe school climate; Low teacher expectations of student achievement; and Lack of clear school policies regarding drug use.
(Hawkins et. al., 1992).
Slide 50: Protective FactorsSchool. Key protective factors within the school setting are similar to those for the family. Principal among these are caring and support; high expectations; clear standards and rules for appropriate behavior; and youth participation, involvement, and responsibility in school tasks and decisions (Elias et al., 1997).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
14

SLIDES 51 and 52 describe Peer Group Risk and Protective Factors
Slide 51: Risk FactorsPeer Group. The negative influence of peers is well established as one of the most important factors in the onset of drug and alcohol use among youth through young adulthood (Swisher, 1992). According to Swisher (1992) adolescents who are strongly peer-oriented hold “more negative views of themselves, see themselves as less dependable, more hostile, more likely to disobey adults, less interested in academics, less future-oriented, and have traditionally weak bonds with traditionally positive norms such as those espoused by the family, community , or religion.” One or more of the preceding vulnerabilities to peer influence can lead to the surest predictor of substance use, involvement with peers who use alcohol and drugs and engage in other forms of problem behavior (Hawkins et al., 1988).Slide 52: Protective FactorsPeer Group. One of the most important factors in young people’s ability to resist negative peer influences is involvement with positive peer group activities and norms (Swisher, 1992). Also, helping young people resist negative peer influences through involvement in groups with social competencies such as decision-making skills, assertiveness, and interpersonal communication (Swisher, 1992).
SLIDES 53 through 55 describe Community Risk and Protective Factors
Slide 53: Risk Factors Community. In a review of research related to community risk factors for substance use disorders, Emshoff et al., (1992) identified seven that appear to have a direct influence:
Community norms that promote or permit substance use. Poverty/lack of empowerment. Lack of community bonding and community disorganization. Cultural disenfranchisement—i.e., a perception among youth that the
dominant/mainstream culture is not relevant to them; that they are discriminated against because of their culture, race, or ethnicity; or that little value is attached to their ethnicity and culture.
Slide 54: Risk Factors (continued)Community. The balance of the seven identified community risk factors are:
Policies that encourage or fail to discourage substance use—tolerance of sales of tobacco and alcohol to minors.
Pro-use messages in the general media. Pro-use messages specifically in advertising—e.g., youth-oriented cigarette
advertising has been consistently linked with the onset of smoking.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
15

Slide 55: Protective Factors Community. Elements found in caring communities are similar to the protective factors within families and schools and include:
Caring and support—social networks and support systems that can promote and sustain social cohesion within the community (Battistich et al., 1996).
High expectations—cultural norms that set high standards of behavior for young people, including clear norms regarding the use of alcohol and drugs, and that also value youth as community members.
Opportunities for participation—ways for youth to function as active and contributing members of the community and participate in cooperative learning and shared decision making (Battistich et al., 1996).
SLIDES 56 and 57 describe Societal Risk and Protective Factors
Slide 56: Risk Factors Societal. Society-level risk factors relate to national economic and employment conditions, discrimination, and marginalization of groups which increases their risk for substance use and abuse.
Slide 57: Protective FactorsSocietal. Societal-level characteristics or policies can also work to protect youth from initiating substance use. Messages promoting substance use via the media may lose their impact if children are taught to become media literate or if these same media channels also carry counter-advertising messages describing the harmful effects of substance use (Lewit et al., 1981; Wallack and De Jong, 1995). Additionally, decreasing substance accessibility can also protect youth. This can be done through a variety of strategies such as increased prices through taxation, increased purchasing age with enforcement, and stricter driving laws.
Slide 58: Risk Factors for the ElderlySubstance use disorders occur across the lifespan. While many of the risk and protective factors correlated with youthful substance use may effect adults, the literature is sparse in this area. What is known is that alcohol and drug use decreases with age but older adults are particularly susceptible to adverse medical consequences when abuse does occur. (Adams et al., 1996; Fingerhood, 2000). Adults 65 years and older represent 12% of the population but consume 30% of all prescription medications and have a rate of over-the-counter drug uses that is seven times that of the general population (U.S. Department of Health and Human Services, 1998). Twenty-five percent of community-dwelling older individuals use psycho-therapeutic drugs on a regular basis (Fingerhood, 2000). Hence, there is increased risk of drug-drug interactions and toxic effects from polypharmacy.
Research studies typically identify two types of older alcoholics, those who have had alcoholism for many years and survive to age 60 or older (early-onset alcoholics) and those who become problem drinkers later in life (late-onset alcoholics) (Dupree, 1990; Fingerhood, 2000; Simoneau & Bergeron, 2000). Late-onset alcoholics typically drink less, have fewer substance misuse problems and function better socially than early-onset alcoholics (Schonfeld & Dupree, 1990; Brennan & Moos, 1991; Leberto & Oslin, 1995). Late-onset alcoholism is
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
16

precipitated by one or more losses such as health status, friends, or spouse (Simoneau & Bergeron, 2000; Schonfeld & Dupree, 1990; Liberto & Oslin, 1995; Dufour & Fuller, 1995).
Slide 59: Risk Factors for the Elderly (continued)Other frequently cited antecedents to drinking for both groups include depression, loneliness, boredom, sadness, lack of social support and negative cognitive coping style (Schonfeld & Dupree, 1991; Fingerhood, 2000; Simoneau & Bergeron, 2000). Active cognitive coping, high level of social support, and perception of control appear to buffer the risks or antecedents (Welte & Mirand, 1995; Simoneau & Bergeron, 2000). According to Welte and Mirand (1995), there is a very strong relationship between current drinking and drinking later in life, pointing to the importance of prevention of alcoholism in young and middle aged adults.
Unfortunately substance use disorders among older adults often go unrecognized by family members and health professionals. More attention is currently being paid to screening and assessment with this population but community-based prevention activities are few.
Slide 60: Protective Factors for the ElderlyKey protective factors for the elderly include:
Positive coping responses to life changes Supportive family Supportive social networks Informed about potential drug interactions and biologic sensitivity to substances. (Welte & Mirand, 1995; Simoneau & Bergeron, 2000).
Slide 61: Role of Health Care Practitioner The role of health professional in incorporating prevention activities into practice can be:
To identify individuals, especially children, who are carrying risk factors and to check their social support structure (e.g., family and school support). If risks are identified, resources can be mobilized to address them. Sometimes referrals need to be made to other resources such as specialized treatment for substance use disorders or to school counselors;
To help build protective factors by giving healthy prevention messages or brief advice to patients of all ages;
To set up clinic space to promote health and prevent substance use problems;
Slide 62: Role of Health Care Practitioner (continued)In the community the health care professional can have a significant impact by:
Participating in community and school activities directed at supporting families and individuals as a way to help build the social safety net;
Utilizing home visits to find out more about patient risks and the encourage protective factors;
Working with colleagues in professional organizations to promote or sponsor prevention health promotion activities in the community; and
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
17

Advocating with policy makers on all levels to change laws or public policy that prevent substance use problems (e.g. raising excise taxes, limiting the number of alcohol outlets).
Slide 63: Designing Effective Prevention Programs Three common elements underlie effective preventive interventions for all age and cultural groups. Those elements include: 1) attention to promotion of protective factors and reduction of risk factors; 2) grounding in behavioral change theory; and 3) strategies that enhance client-provider interaction, quality of program implementation, and client participation in and exposure to programming (dose-response) (Dusenburg & Falco, 1995; Hansen, 1992; Pentz, 1998; Preventing Drug Use Among Children and Adolescents, 1997; Prevention Programs for Youth, 1998). Knowledge of cultural factors are also critical to the design of preventive interventions.
Slide 64: Theories of ChangeTheories of behavior change inform research and evaluation of prevention programs. Social cognitive theory states that individuals learn behaviors through a process of modeling and reinforcement of behaviors observed in group settings (Bandura, 1986). If those behaviors are deviant they may be perceived by adolescents as normative (Schinke & Cole, 1995). According to problem based theory, substance use may be functional for the adolescent as deviant behavior may assist young people with weak attachments to pro social settings to achieve their goals (Jessor & Jessor, 1997). This particular problem behavior is useful in aligning with peers, overcoming anxiety, relieving boredom, coping with stress and achieving pleasure (Hird et al., 1997). Oetting and Beauvois (1986, 1987) observed that peer interactions greatly influence risk-taking behavior. The resultant constructs, peer cluster theory, may be used in the context of interventions to reinforce positive behaviors (Schinke & Cole, 1995). The theory of ethnic identity posits that ethnic identity, rather than being a static construct, is an ongoing developmental process from naïveté to mature appreciation of ones ethnic group. According to this theory, full self-actualization implies successful completion of the stages (Phinney, 1989; Phinney, 1990; Phinney, 1992; Scheier et al., 1997; Ringwalt et al., 1999). Exploration of this theory as it relates to prevention programs for minority youth is a relatively new area of investigation. See Module III for a discussion of the transtheoretical model of change. Designing programs based on sound theory permit the researcher to determine whether successful behavior change occurred according to the mechanisms of the theory or, if the program was ineffective, the mechanisms were not implemented correctly. (Pentz, 1999; Petraitis et al., 1997).
Slide 65: Cultural CompetenceKnowledge of cultural factors associated with substance use disorders, as well as other health problems, is critical to understanding comprehensive community-based substance abuse prevention (Poss, 1999). There is a clear link between cultural competence and the success or failure of prevention interventions. Wright and Watts (1985) note, for example, that preventing alcohol abuse among African American youth may start with some of the same elements as with other ethnic groups, but issues such as high unemployment levels, pose additional risks for this group. On the other hand, understanding of the rich cultural history, with roots in Africa, is key to assisting African American youth to build the protective self-
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
18

pride necessary to promote positive drinking behaviors. Gerstein and Green (1993) note the serious paradox that African Americans are far less likely than non-Hispanic whites to use drugs, but those who do are far more likely to become dysfunctional. Similarly Hispanic drug use prevalence is lower than for non-Hispanic whites overall, but Hispanics are over-represented in drug-treatment and criminal justice statistics. According to Schinke et al., (2000), Native American youths use tobacco, alcohol and other drugs earlier, at higher rates and with more severe health, social and economic consequences than adolescents of other American ethnic-racial groups.
The most successful prevention programs for these adolescents take into account the two cultures in which they live: the Native American and the dominant non-Indian culture (Schinke et al., 2000). The cultural competence model developed by Campinha-Bacote (1991) is useful in addressing cultural competence in preventive intervention. The model is comprehensive, incorporating cultural awareness, cultural knowledge, cultural skills, and the cultural encounter or personal experience with the group. There is now a growing body of literature to assist the clinician/researcher to assure that preventive intervention are culturally competent (Botvin et al., 1995; Braithwaite et al., 2000; Huff & Kline, 1999; McCubbin et al, 1995; Wilson et al., 1997; Kar, 1999Herd & Grube, 1996, Amaro, et al 2001; Harachi, et al, 2001, Nichter, 2003; Wallace & Muroff, 2002). Refer to Module One for information on cultural competence.
Slide 66: General Prevention StrategiesGeneral prevention strategies include:
Information dissemination Development of life-coping skills Provision of alternatives Community development Advocacy for a healthy environment Problem identification
Slide 67: Elements of Effective ProgramsElements of effective substance abuse prevention programs are:
Use of standardized training materials Use of social learning theory methods Attention to quality of implementation Use of periodic booster sessions Use of techniques to extend program beyond the setting (homework). (Pentz, 1999).
Slide 68: Combined Strategies in Communities are Most EffectiveCombined community strategies incude:
Curriculum in schools Parent involvement Support by community leaders and health professionals Enforcement of policies Use of media to reinforce message
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
19

Slide 69: Settings for Community-Based StrategiesCommunity-Based strategies are effective in the following settings:
Schools Churches Community centers Youth organizations Family centers Senior Centers
Slide 70: Community-Based Participatory ApproachesThe community should be involved in all aspects of preventive interventions: 1) to assure that the program is specifically tailored to the needs of the community; and 2) to increase the capacity of the community to deliver the interventions. Participatory research methods offer a viable means to accomplish the goal of community involvement. Approaches to participatory research include applications variously labeled as action research, participatory action research, community-based action research and advocacy research (North American Primary Care Research Group, 1998).Slide 71: Community-Based Participatory Approaches (continued)These applications provide a common framework which includes community participation, research, and action directed at resolving problems identified by community stakeholders (Cornwall & Jewkes, 1995; Israel et al, 1998; Rains & Ray, 1995). Knowledge and societal change are literally created by interactions between the researcher and the stakeholders all of whom are defined as participants in the research. These approaches are useful in community prevention activities
Slide 72: Evaluation RationaleComprehensive evaluation of community-based prevention programs is critical to advancing the science in this important field. The evaluation plan should include both process and outcome components. Process evaluation means documenting all aspects of implementation of the program. Outcomes are benefits that program participants, families, and communities derive from the intervention. Short-term benefits might be new knowledge, improved skills, and changed attitudes. Longer-term outcomes might be changed client behaviors, reduced risks and enhanced protective factors. An appropriate outcomes evaluation system can provide:
A systematic way to monitor clients’ outcomes that result from intervention. Feedback that reflects the need to make adjustments. Evidence that the program works and is cost effective. Findings that contribute to the development of “best practices” in prevention efforts. A method to disseminate findings to others in the field. (Prevention Programs for Youth, 1998).
Slide 73: EvaluationComponents of evaluation are Process and short and long-term Outcomes.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
20

Process includes documenting all aspects of implementation of the program. Outcomes are divided into short and long-term benefits. Short–term benefits include new knowledge, improved skills and changed attitutdes. Long-term benefits may incorporate changed behaviors, rduced risks and aenhanced protective factors.
Evaluation Tool
Slide 74: The Getting to Outcomes FrameworkThe Center for Substance Abuse Prevention (CSAP) has developed a comprehensive model that summarizes the activities involved in prevention research. The framework includes steps to planning and evaluation as well as a logic mode (Getting to Outcomes, 2000).
Slide 75: Summary Community-based substance abuse prevention is a complex, multifaceted process, involving comprehensive definition of all influences on the target population and informed selection, implementation and evaluation of science-based interventions. Health professionals should consider community-based prevention a component of their role to safeguard the well-being of clients, families, and the general population.(The Risk and Resilience information in this handout have been adapted from: Substance Abuse and Mental Health Services Administration Center for Substance Abuse. Understanding Substance Abuse Prevention Toward the 21st Century: A Primer on Effective Programs. A Monograph. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration Center for Substance Abuse, May 1999, pp. 2-8).
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
21
Objects ofinterest inevaluation
Sources of standards of acceptability in evaluation
Process Impact evaluation
Outcome evaluation
Healthpromotionprogram
Peer Review,Quality con-trol, accredi- tation, audit,
Predisposing, enabling, and reinforcing factors
Changes in knowledge, attitudes, beliefs, skills, resources, social support, policy
Protective behavior, or environment
Changes in frequency, knowledge, attitudes, beliefs, skills, resources, social support, policy
Health
Changes in mortality, morbidity, disability, or risk factors
SocialBenefits
Changes in quality of life

References
Adams WL, Barry KL, Fleming MF. Screening for problem drinking in older primary care patients. JAMA. 1964-1967, 276(24), 1996.
Amaro H, Raj A, Vega RR, Mangione TW, Perez L. Racial/ethnic disparities in the HIV and substance abuse epidemics: communities responding to the need. Public Health Reports 2001; 116:434-448.
Aos S, Phipps P, Barnoski R, Lieb R. The Comparative Costs and Benefits of Programs to Reduce Crime. Vol. 4 (1-05-1201). Olympia, WA: Washington State Institute for Public Policy, May 2001.
Ashery RS, Robertson EB, Kumpfer KL (Eds). Drug Abuse Prevention Through Family Interventions. NIDA Research Monograph No. 177. Washington, DC: U.S. Government Printing Office, 1998.
Bandura A. Social Foundations of Thought and Action. New Jersey: Prentice-Hall, Inc., 1986.
Battistich V, Schaps E, Watson M, Solomon D. Prevention effects of the child development project: Early findings from an ongoing multi-site demonstration trial. J Adolesc Res. 1996; 11(1):6-11.
Battistich V, Solomon D, Watson M, Schaps E. Caring school communities. Educational Psychologist 1997; 32(3):137–151.
Bauman KE, Foshee VA, Ennett ST, Pemberton M, Hicks KA, King TS, Koch GG. The influence of a family program on adolescent tobacco and alcohol. American Journal of Public Health 2001; 91(4):604–610.
Beauvais F, Chavez E, Oetting E, Deffenbacher J, Cornell G. Drug use, violence, and victimization among White American, Mexican American, and American Indian dropouts, students with academic problems, and students in good academic standing. Journal of Counseling Psychology 1996; 43:292–299.
Bernard B. The Case for Peers. Portland, OR: Western Center for Drug-Free Schools and Communities, 1990.
Bernard B. Fostering Resiliency in Kids: Protective Factors in the Family, School, and Community. Portland, OR: Northwest Regional Educational Laboratory, 1991.
Botvin GJ, Baker E, Filazzola AD, Botvin EM. A cognitive-behavioral approach to substance abuse prevention: One-year follow-up. Addict Behav. 1990; 15(1):47-63.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
22

Botvin GJ, Schinke S, Orlandi MA (Eds). Drug Abuse Prevention with Multiethnic Youth. Thousand Oaks, CA: Sage Publications, Inc., 1995.
Botvin G, Baker E, Dusenbury L, Botvin E, Diaz T. Long-term follow-up results of a randomized drug-abuse prevention trial in a white middle class population. Journal of the American Medical Association 1995; 273:1106–1112.
Braithwaite RL, Taylor SE, Austin JN. Building Health Coalitions In the Black Community. Thousand Oaks, CA: Sage Publications, Inc., 2000.
Brennan PL, Moos RH. Functioning life context, and help-seeking among late onset problem drinkers: Comparisons with nonproblem and early-onset problem drinkers. Brit J Addict, 30 (13 & 14): 1799-1818, 1991.
Brounstein PJ, Altschuler DM, Hatry HP, Blair LH. Substance Use and Delinquency Among Inner City Adolescent Males. Washington D.C.: Urban Institute Press, 1989.
Burgoyne K. Communities That Care: Applying The Strategy. Seattle, WA: Developmental Research and Programs, Inc., 1991.
Campinha-Bacote J. The Process Of Cultural Competence: A Culturally Competent Model Of Care. Wyoming, OH: Transcultural Care Associates, 1991.
Center for Substance Abuse Prevention. Prevention Plus III. Assessing Alcohol and Other Drug Prevention Programs at the School and Community Level. DHHS Pub. No. (ADM) 91-1817. Rockville, MD: Department of Health and Human Services, 1991.
Center for Substance Abuse Prevention (CSAP). Prevention Strategies Based On Individual Risk Factors For Alcohol And Other Drug Abuse. (CSAP Technical Report 7). Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, 1993.
Center for Substance Abuse Prevention (CSAP) Medical Specialist Program. Alcohol, Tobacco and Other Drug Problem Prevention: Curriculum for Health Care Professionals. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration (Contract to Society of Teachers of Family Medicine), 1994.
Chinman M, Hanna G, Wandersman A, Ebener P, Hunmter SB, Imm P, Sheldon J. Developing a community science research agenda for building community capacity for effective preventive interventions. American Journal of Community Psychology 2005; 35(3/4):143-157.
Chou C, Montgomery S, Pentz M, Rohrbach L, Johnson C, Flay B, Mackinnon D. Effects of a community-based prevention program in decreasing drug use in high-risk adolescents. American Journal of Public Health 1998; 88:944–948.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
23

Commission on Chronic Illness. Chronic Illness in the United States. Vol. 1. Published for the Commonwealth Fund. Cambridge, MA: Harvard university Press, 1957.
Conduct Problems Prevention Research Group. Predictor variables associated with positive Fast Track outcomes at the end of third grade. Journal of Abnormal Child Psychology 2002; 30(1):37–52.
Cornwall A & Jewkes R. What is participatory research? Social Science & Medicine 1995; 41(12):1667-1676.
Curry SJ, Kim EL. Public health perspective on addictive behavior change interventions: Conceptual frameworks and guiding principles. In J.A. Tucker, D.M. Donovan, & G.A. Marlatt, eds. Changing Addictive Behavior: Bridging Clinical and Public Health Strategies. New York: The Guilford Press. 1999, 221-250.
Dishion T.; McCord J, Poulin F. When interventions harm: Peer groups and problem behavior. American Psychologist 1999; 54:755-764.
Dishion T, Kavanagh K, Schneiger AKJ, Nelson S, Kaufman N. Preventing early adolescent substance use: A family centered strategy for the public middle school. Prevention Science 2002; 3(3):191–202.
Dufour M, Fuller RK. Alcohol in the elderly. Annual Review of Medicine, 46: 123-132, 1995.
Dusenbury L, Falco M. Eleven components of effective drug abuse prevention curricula. J Sch Health. 1995;65:420-425.
Eggert LL, Thomson EA, Herting JR, Nicholas LJ, Dicker BG. Preventing adolescent drug abuse and high school dropout through an intensive school-based social network development program. Am J Health Promot. 1994;8(3):202-215.
Eggert LL, Thompson EA, Herting JR, Nicholas LJ. Reducing suicide potential among high-risk youth: Tests of a school-based prevention program. Suicide Life Threat Behav. 1995;25(2):276-296.
Elias MJ, Zins JE Weissberg RP. Promoting Social And Emotional Learning: Guidelines For Educators. Alexandria, VA: Association for Supervision and Curriculum Development, 1997.
Emshoff J, Erickson S, Thompson M. (unpublished manuscript). Community Factors And Strategies For Substance Abuse. Center for Substance Abuse Prevention, 1992.
Erickson EH. Childhood and Society. New York: W.W. Norton & Co. (1985) (original work published 1950), 1985.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
24

Fingerhood, M. Substance abuse in older people. J American Geri. Soc 48: 985-995, 2000.
Gerstein RD, Green LW (Eds.). Preventing Drug Abuse: What Do We Know? Washington, DC: National Academy Press,1993.
Getting to Outcomes: Methods and Tools for Planning, Self Evaluation and Accountability 2000. Center for Substance Abuse Prevention. National Center for Advancement of Prevention. Conference Edition.
Gordon R. An operational classification of disease prevention. Public Health Rep. 98: 107-109, 1983.
Grant BF, Dawson DA. Age of onset of drug use and its association with DSM-IV drug abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse. 1998;10(2):163-173.
Green LW, Kreuter, MW. Health promotion planning: An educational and ecological approach (3rd edition). Mountain View: Mayfield Publishing Company. 1999.
Hansen WB. School-based substance abuse prevention: a review of the state of the art in curriculum, 1980-1990. Health Educ Res. 1992;7:403-430.
Harachi TW, Catalano RF, Kim S, Choi Y. Etiology and prevention of substance use among Asian American youth. Prevention Science 2001; 2(1):57-65.
Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychol Bull. 1992;112 (1):64-105.
Hawkins, J.D.; Catalano, R.F.; and Arthur, M. Promoting science-based prevention in communities. Addictive Behaviors 90(5):1–26, 2002.
Hawkins JD, VanHorn ML, Arthur MW. Communiyt variation in risk and protective factors and substance use outcomes. Prevention Science 2004; 5(4):231-65.
Hawkins JD, Jenson JM, Catalano RF, Lishner DM. Delinquency and drug abuse: Implications for social services. Soc Serv Rev. 1988; 62 (2):258-284.
Hawkins JD, Catalano RF, Kosterman R, Abbott R, Hill KG. Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatric and Adolescent Medicine 1999; 153:226–234.
Hazelden Foundation. Roots and Wings: Raising Resilient Children. Center City, MN: Hazelden Foundation, 1996.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
25

Herd D, Grube J. Black identity and drinking in the US: A national study. Addiction 1996; 91(6)845-857.
Hird S, Khuri ET, Dusenberg L, Millman RB. Adolescents. In Lowinson, J.H., Ruiz, P., Millman, R.B.& Langrod, J.G. , eds. Substance Abuse: A Comprehensive Textbook. Third Edition. Baltimore: Willliams & Wilkins, 1997:683-692.
Huff RM, Kline MV. Promoting Health in Multicultural Populations: A Handbook for Practitioners. Thousand Oaks, CA: Sage Publications, 1999.
Ialongo N, Poduska J, Werthamer L, Kellam S. The distal impact of two first-grade preventive interventions on conduct problems and disorder in early adolescence. Journal of Emotional and Behavioral Disorders 2001; 9:146–160.
Israel BA, Schulz AJ, Parker EA, Backer AB. Review of community-based research: assessing partnership approaches to improve public health. Annual Review of Public Health, 1998; 19:173-202.
Jessor R, Jessor SL. Problem Behavior and Psychosocial Development. New York: Academic Press, 1997.
Johnston LD, O’Malley PM, Bachman JG. National Survey Results on Drug Use From the Monitoring the Future Study, 1975-1996, Vol. 1: Secondary School Students (NIH Publication No. 94-3809). Rockville, MD, U.S. Department of Health and Human Services, 1997.
Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future National Survey Results on Drug Use, 1975–2002. Volume 1: Secondary School Students. Bethesda, MD: National Institute on Drug Abuse, 2002.
Kandel DB. Epidemiological and psychosocial perspectives on adolescent drug use. J Am Acad Clin Psychiatry. 1982;l21:328-347.
Kar SB (Ed). Substance Abuse Prevention: A Multicultural Perspective. Amityville, NY: Baywood Publishing Company, Inc., 1999.
Kosterman R, Hawkins JD, Spoth R, Haggerty KP, Zhu K. Effects of a preventive parent-training intervention on observed family interactions: Proximal outcomes from Preparing for the Drug Free Years. Journal of Community Psychology 1997; 25(4):337–352.
Kosterman R, Hawkins JD, Haggerty KP, Spoth R, Redmond C. Preparing for the Drug Free Years: Session-specific effects of a universal parent-training intervention with rural families. Journal of Drug Education 2001; 31(1):47–68.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
26

Kumpfer KL. Strengthening America’s Families: Promising Parenting Strategies for Delinquency Prevention. User’s Guide. Washington, DC: U.S. Department of Justice, Office of Juvenile Justice and Delinquency Prevention,1993.
Kumpfer KL, Molraad V, Spoth R. The Strengthening Families Program: for the Prevention of Delinquency and Drug Use. In Peters, R. & McMahon, R., eds. Preventing Childhood Disorders Substance Abuse and Delinquency. Thousand Oaks, CA: Sage Publications, 1996.
Lewit EM, Coate D, Grossman M. The effects of government regulation on teenage smoking. J Law Econ. 1981;24:545-569.
Liberto JG, Oslin DW. Early versus late onset of alcoholism in the elderly. Int J Addict, 30 (13 & 14): 1799-1818, 1995.
Marcus MT, Walker T, Swint JM, Smith BP, Brown C, Busen N, Edwards T, Liehr P, Taylor WC, Williams D, von Sternberg K. Community-based participatory research to prevent substance abuse and HIV/AIDS in African American adolescents. Journal of Interprofessional Care, 2004; 18(4), 347-359.
Marcus MT. Alcohol and other drug abuse in elders. J ET Nurs. 1993; 20: 106-110.
Marcus MT. An interdisciplinary team model for substance abuse prevention in communities. J Prof Nurs. 2000;16(3):158-168.
McCubbin HI, Thompson EA, Thompson AI, Futrell JA. Resiliency in African American Families. Thousand Oaks, CA: Sage Publications, 1995.
Moon D, Hecht M, Jackson K, Spellers R. Ethnic and gender differences and similarities in adolescent drug use and refusals of drug offers. Substance Use and Misuse 1999; 34(8):1059–1083.
Monitoring the Future (2004). http://monitoringthefuture.org
Mrazek PJ, Haggerty RJ (Eds.). Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. Institute of Medicine. Washington, D.C.: National Academy Press, 1994.
Murray LF & Belenko S. CASASTART: A community-based, school-centered intervention for high-risk youth. Substance Use & Misuse 2005; 40:913-933.
National Institute on Drug Abuse Community Epidemiology Work Group (2003). www.drugabuse.gov/about/organization/cewq/Reports.html
National Institute on Alcohol Abuse and Alcoholism. 10th Special Report to the US Congress on Alcohol and Health. U.S. Department of Health and Human Services, June 2000. http://www.niaaa.nih.gov
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
27

National Institute on Drug Abuse. Youth at High Risk for Substance Abuse. Publication BKD06. Rockville, MD: U.S. Department of Health and Human Services, 1990.
Nichter M. Smoking:what does culture have to do with it? Addiction 2003; (98 Suppl 1):139-145.
NIDA InforFacts: Lessons from Prevention Research. http//www.nida.nih.gov/infofacts/lessons.html (revised 2/04). Accessed 10-1-2005.
Oetting E, Beauvois F. Peer cluster theory: Drugs and the adolescent. J Counsel Devel. 1986;65:17-22.
Oetting E, Beauvois F. Peer cluster theory, socialization characteristics and adolescent drug use: A path analysis. J Counsel Psychol. 1987;34:205-213.
Oetting E, Edwards R, Kelly K, Beauvais F. Risk and protective factors for drug use among rural American youth. In: Robertson, E.B.; Sloboda, Z.; Boyd, G.M.; Beatty, L.; and Kozel, N.J., eds. Rural Substance Abuse: State of Knowledge and Issues. NIDA Research Monograph No. 168. Washington, DC: U.S. Government Printing Office 1997; pp. 90–130.
Orlando M, Ellickson PL, McCaffrey DF, Longshore DL. Mediation analysis of a school-based drug prevention program: Effects of Project ALERT. Prevention Science 2005; 6(1):35-46.
Pentz MA. Preventing Drug Abuse Through The Community: Multi-Component Programs Make the Difference. (NIDA Research Monograph). Edited by Sloboda, Z., Hansen, W.B. Washington, DC: National Institute of Drug Abuse, 1998.
Pentz MA. Prevention. In M. Galanter & H.D. Kleber, ed. Textbook of Substance Abuse Treatment, Second Ed. American Psychiatric Press: Washington, DC. 1999:535-544.
Pentz MA, Dwyer JH, MacKinnon DP, Flay BR, Hansen WB, Wang EY, Johnson CA. A multi-community trial for primary prevention of adolescent drug abuse: Effects on drug use prevalence. JAMA. 1989, 261:3259-3266.
Pentz MA. Costs benefits, and cost-effectiveness of comprehensive drug abuse prevention. In: Bukoski, W.J.; and Evans, R.I., eds. Cost-Benefit/Cost-Effectiveness Research of Drug Abuse Prevention: Implications for Programming and Policy. NIDA Research Monograph No. 176. Washington, DC: U.S. Government Printing Office, pp. 111–129, 1998.
Perry CL. Models of effective prevention. The Prev Res. 1996;3(1):1-5.
Perry CL. Creating behavior change: How to develop community-wide programs for youth. Thousand Oaks, CA: Sage Publications, Inc., 1999.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
28

Perry, CL, Williams CL, Veblen-Moatenson S, Toomey TL, Lomro KA, Anstine PS, McGovern PG, Finnegan JR, Forster JL, Wagenaor, AC, Wolfson M. Project Northland: Outcomes of a community wide alcohol use prevention program during early adolescence. Am J of Pub Health. 86(7): 956-965, 1996.
Peterson, AV, Kaley, KA, Mann, SL, Marek, PM, Sarason, IG. Hutchison Smoking Prevention Project: Long-Term Randomized Trial in School-Based Tobacco Use Prevention – Results on Smoking. J Natl Cancer Institute. 2000;92(24):1979-1991. [email protected]
Petraitis J, Flay BR, Miller TQ. Reviewing theories of adolescent substance use: organizing pieces in the puzzle. Psychol Bull. 1999: 67-68.
Phinney JS. Ethnic identity in adolescents and adults: Review of Research. Psychol Bull, 1990; 108 (3): 499-514.
Phinney JS. The multigroup ethnic identity measure: A new scale for use with diverse groups. J Adolesc Res. 1992; 7(2): 156-176.
Phinney JS. Stages of ethnic identity development in minority group adolescents. J Early Adolescy. 1989; 9(1-2): 34-49.
Poss JE. Providing culturally competent care: Is there a role for health promoters? Nurs Outlook. 1999;47:30-36.
Preventing Drug Use Among Children and Adolescents: A Research-Based Guide. NIH Publication No. 97-4212. Washington, DC: National Institute of Drug Abuse, 1997.
Prevention Programs for Youth: A Guide To Outcomes Evaluation, Best Practices, and Successful Funding. Edited by Karienne Stovall. Providence, R.I.: Behavioral Health Resource Press, Manisses Communications Group, Inc., 1998.
Prochaska JO, DiClemente CD. Stages and pro-cesses of self-change of smoking: Toward an inte-grative model of change. J Consult Clin Psychol. 1983;51:390-395.
Rains JW & Ray DW. Participatory action research for community health promotion. Public Health Nursing 1995; 12(4):256-261.
Ringwalt C, Graham P, Sanders-Philips K, Browne D, Paschall MJ. Ethnic identity as a protective factor in the health behaviors of African-American male adolescents. In Kar SD, ed. Substance Abuse Prevention: A Multicultural Perspective. Amityville, NY: Baywood Publishing Company, Inc., 1999.
Rutter M. Protective factors in children’s responses to stress and disadvantage. In M.W. Kent and J.E. Rolf, ed. Primary Prevention of Psychotherapy: Volume 3. Social Competence in Children. Hanover, NH: University Press of New England, 1979.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
29

Sanders MR. Community-based parenting and family support interventions and the prevention of drug abuse. Addictive Behaviors 2000; 25(6):929-942.
Scheier, LM, Botvin, GJ, Diaz T, & Ifilll-Williams M. Ethnic identity as a moderator of psychosocial risk and adolescent alcohol and marijuana use: Concurrent and longitudinal analyses. J Child Adosesc Subst Abuse, 1997; 6(1); 21-47.
Scheier L, Botvin G, Diaz T, Griffin K. Social skills, competence, and drug refusal efficacy as predictors of adolescent alcohol use. Journal of Drug Education 1999; 29(3):251–278.
Schinke S, Cole K. Prevention in community settings. In G.J. Botvin, S. Schinke, & M.A. Orlandi, eds. Drug Abuse Prevention With Multiethnic Youth. Thousand Oaks, CA: Sage Publications. 1995:215-232.
Schonfeld L, Dupree LW. Older problem drinkers – Long-term and late onset abusers: What triggers their drinking? Aging, 361: 5-8, 1990.
Schonfeld L, Dupree LW. Antecedents for early- and late-onset elderly alcohol abusers. J of Studies on Alcohol, 52(6), 587-592, 1991.
Schuckit M. New findings in the genetics of alcoholism. JAMA. 1999; 281: 1875-1876.
Schinke, SP, Tepavac L & Cole KC. Preventing substance use among Native American youth: Three years results. Addict Behav. 2000;25 (3):387-397.
Simoneau H, Bergeron J. An etiologic model of alcoholism from a developmental ecological perspective. Substance Use and Misuse, 35(10), 1329-1368, 2000.
Spoth RL, Greenbery MT. Toward a comprehensive strategy for effective practitioner-scientists partnerships and larger scale community health and well-being. American Journal of Community Psychology 2005; 35(3/4):107-126.
Spoth, R.; Guyull, M.; and Day, S. Universal family-focused interventions in alcohol-use disorder prevention: Cost effectiveness and cost-benefit analyses of two interventions. Journal of Studies on Alcohol 2002a; 63:219–228.
Spoth RL, Redmond D, Trudeau L, Shin C. Longitudinal substance initiation outcomes for a universal preventive intervention combining family and school programs. Psychology of Addictive Behaviors 2002b; 16(2):129–134.
Substance Abuse Mental Health Services Administration, Results from 2003 National Survey on Drug Use & Health: National Findings (Office of Applied Studies, NSDUH Series H-25, OHHS Publication No. SIMA 0-4-3964. Rockville, MD).
Swisher JD Peer Influence and Peer Involvement in Prevention. Rockville, MD: Center for Substance Abuse Prevention, Division of High Risk Youth, 1992.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
30

U.S. Department of Health and Human Services. Healthy People 2010 (Conference Edition in Two Volumes). Washington, DC: January 2000.
U.S. Department of Health and Human Services. Put Prevention Into Practice: Clinician’s Handbook of Preventive Services (2nd Ed.). Washington, DC: 1998.
Wallace JM, Muroff JR. Preventing substance abuse among African American children and youth: Race differences in risk factor exposure and vulnerability. Journal of Primary Prevention 2002; 22(3):235-261.
Wallack L, DeJong W. Mass media and public health: Moving the focus from individual to the environment. In S. Martin and P. Marl, eds. The Effect of the Mass Media on the Use and Abuse of Alcohol (NIAAA Research Monograph No. 28, pp. 253-266). Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism, 1995.
Webster-Stratton C. Preventing conduct problems in Head Start children: Strengthening parenting competencies. Journal of Consulting and Clinical Psychology 1998; 66:715–730.
Webster-Stratton C, Reid J, Hammond M. Preventing conduct problems, promoting social competence: A parent and teacher training partnership in Head Start. Journal of Clinical Child Psychology 2001; 30:282–302.
Welte JW & Mirand AL. Drinking, problem drinking and life stressors in the elderly population. J Studies on Alcohol, 1995; 56: 67-73.
Windle M. Alcohol use among adolescents. Thousand Oaks, CA: Sage Publications, Inc. 1999.
Wolin S, Wolin S Resilience among youth growing up in substance-abusing families. Pediatr Clin North Am. 1995;42(2):415-429.
Wilson DK, Rodrigue JR, Taylor WC (Eds.). Health-Promoting And Health-Compromising Behaviors Among Minority Adolescents. Washington, DC: American Psychological Association, 1997.
Wright R, Watts TD (Eds.). Prevention of Black Alcoholism: Issues and Strategies. Springfield, Illinois: Charles C. Thomas Publisher, 1985.
Interdisciplinary Faculty Development Program in Substance Abuse Education Project MAINSTREAM Syllabus Module IX: Community-Based Substance Abuse Prevention
31