Embed Size (px)
Citation preview
Clinicat and Experimentat Dermatology 1995; 20: 277-278.
Scottish Dermatological Society AbstractsMeeting: Aberdeen, October 1994
Inducible nitric oxide synthase is upregulated in psoriasis. A.D.Ormerod,N.Benjamin, R.Herriot and S.H.Ralston. Departments of Dermatology,Medicine and Therapeutics and Pathology, University of Aberdeen, UK
Many ceUs bul particulariy macrophages can be induced to produce supra-physiological amounts of niiricoxide, toxic to pathogens, tumour cells and some host cells, as part of a phylogenetically preserved innateimmune response via an induclble nitric oxide synthase (iNOS). In addition to being a potent vasodUator.it is postulated to be pro-inflararaaloty. Keraiinocytes can be induced to synthesise nitric oxide', and increasediNOS in keratinocytes in 11 patients with psoriasis has been shown using PCR^
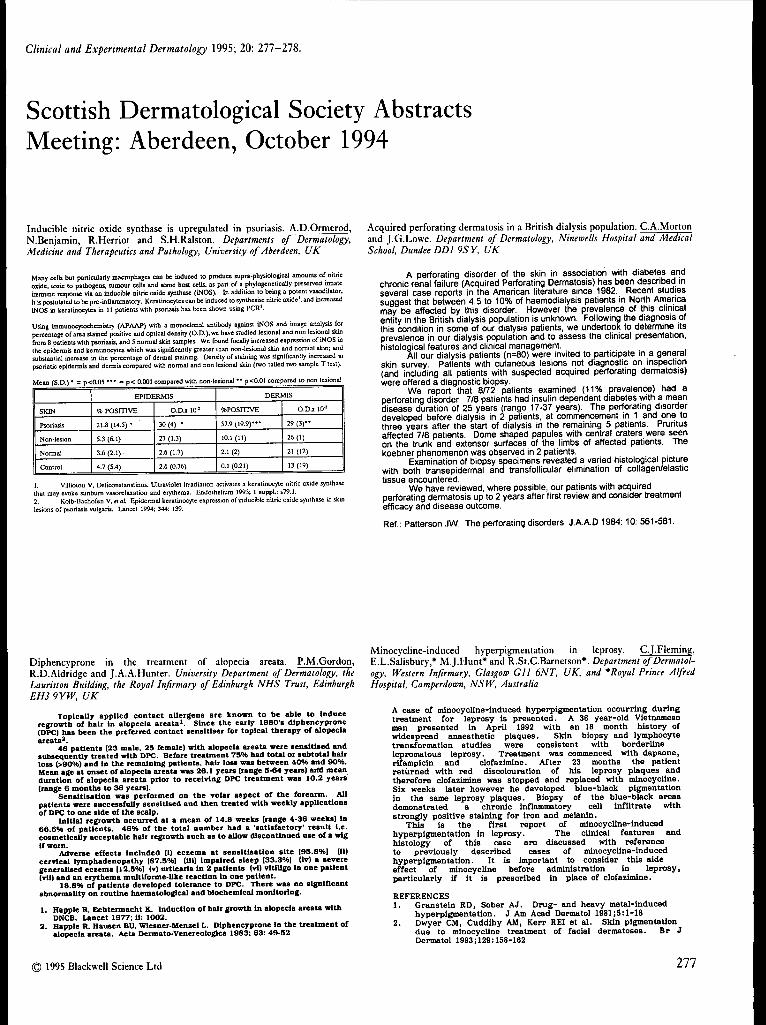
Using immunocytochemisiry (APAAP) with a monoclonal antibody against iNOS and image analysis forpercentage of area stained positive and optical density (O.D.), we have studied lesional and non lesional skin&om 8 patients with psoriasis, and 5 norraal skin samples. We found focally increased expression of iNOS inthe epidermis and keratinocytes which was significantly greater than non-lesional skin and nomia! skin; andsubstantial increase in the percentage of dermal staining. Density of staining was significantly increased inpsoriatic epidermis and dermis compared with normal and non lesional skin (two tailed two sample T test).
Mean (S.D.) • = p<0.05 • " = p < O.CX)1 compared with non-lesiona] " p<0.01 compared to non Icsional
SKIN
Psonasis
Non-lesion
Nomia]
Control
EPIDERMIS
% POSITIVE
21.8 (14.5) •
3.3 (6.1)
3.6 (2.1)
4.7 (5.4)
O . D J I 10 '
30(4) •
27 (1,3)
2.6 (1.7)
2.6 (0.36)
DERMIS
%posinvE
57.9 ( 1 9 . 9 ) ' "
10.1 (11)
2.1 (2)
0.1 (0.21)
O.D.X 10 '
29 ( 3 ) "
26(1)
21 (12)
13 (19)
1. Villiotou V. Deliconstanstinos. Ultraviolet irradiation activates a keratinocyte nitric oxide synthasethat may evoke stjnhum vasortlajiation and erythema. Endothelium 1993; 1 suppl.: s79.1.2. Kolb-Bachofen V.efa/. Epidermal keratinocyte expression of inducible nitric oxide synthase in skinlesions of psoriasis vulgaris. Lancet 1994; 344: 139.
Acquired perforating dermatosis in a British dialysis population. C.A.Mortonand J.G.Lowe. Department of Dermatotogy, Ninewetts Hospitat and MedicatSchoot, Dundee DDl 9SY, UK
A perforating disorder of the skin in association with diabetes andchronic renai failure (Acquired Perforating Dermatosis) has been described inseveral case reports in the American literature since 1982. Recent studiessuggest that between 4.5 to 10% of haemodialysis patients in North Americamay be affected by this disorder. However the prevalence of this clinicalentity in the British dialysis populatipn is unknown. Following the diagnosis ofthis condition in some of our dialysis patients, we undertook to determine itsprevalence in our dialysis population and to assess the clinical presentation,histological features and clinical managemerit.
All our dialysis patients {n=80) were invited to participate in a generalskin survey Patients with cutaneous lesions riot diagnostic on inspection(and including all patients with suspected acquired perforating dermatosis)were offered a diagnostic biopsy.
We report that 8/72 patients examined (11% prevalence) had aperforating disorder. 7/8 patients had insulin dependent diabetes with a meandisease duration of 25 years (range 17-37 years). The perforating disorderdeveloped before dialysis in 2 patients, at commencement iri 1 and one tothree years after the start of dialysis in the remaining 5 patients. Pruritusaffected 7/8 patients. Dome shaped papules with central craters were seenon the trunk and extensor surfaces of the limbs of affected patients. Thekoebner phenomenon was observed in 2 patients.
Examination of biopsy specimens revealed a varied histological picturewith both transepidermal and transfollicular elimination of collagen/elastictissue encountered.
We have reviewed, where possible, our patients with acquiredperforating dermatosis up to 2 years after first review and consider treatmentefficacy and disease outcome.
Ref.: Patterson JW. The perforating disorders. J.A.A.D 1984: 10: 561-581.
Diphencyprone in the treatment of alopecia areata. P.M.Gordon,R.D.Aldridge and J.A.A.Hunter. University Department of Dermatotop, theLauriston Buitding, ttie Royat Infirmary of Edinburgti NHS Trust, EdinburghEH3 9YW. UK
Topically applied contact allergens are known to be able to Induceregrowth of hair In alopecia areata'. Since the early 198O'» diphencyprone(DPC) has been the preferred conUct sensltlser for topical therapy of alopeciaareata'.
4S patients (23 male. 25 female) with alopecia areata were sensitised andsubsequenUy treated with DPC. Before treatment 75% had total or subtotal hairloss (>90%) and in the remaining patients, hair loss was between 40% and 90%.Mean age at onset of alopecia areata was 26.1 years (range 5-64 years) atfd meanduration of alopecia areata prior to receiving DPC treatment was 10.2 years(range 6 months to 36 years).
Sensltlsation was performed on the volar aspect of the forearm. AUpatients were successfully sensitised and then treated with weekly applicationsof DPC to one side of the scalp.
Initial regrowth occurred at a mean of 14.8 weeks (range 4-36 weeks) In66.6% of patients. 46% of the total number had a 'satisfactory' result i.e.cosmetically acceptable hair regrowth such as to allow discontinued use of a wigif worn.
Adverse effects included (I) eczema at sensitlsation site [95.8%1 (ii)cervical lymphadenopathy |87.5%1 (iii) Impaired sleep |33.3%1 (Iv) a severegeneralised eezema 112.5%) (v) urticaria in 2 paUents (vl) vitiligo in one paUent(vU) and an erythema multiforme-Uke reaction ln one patient.
18.8% of patients developed tolerance to DPC. There was no significantabnormality on routine haematological and biochemical monitoring.
1. Happle R. Echtermacht K. induction of hair growth in alopecia areata withDNCB. Lancet 1977; ii: 1002.
2. Happle R. Hausen BU. Wiesner-Menzel L. Diphencyprone In the treatment ofalopecia areata. Acta Dermato-Venereologica 1983: 63: 49-52
Minocycline-induced hyperpigmentation in leprosy. C.J.Fleming,E.L.Salisbury,* M.J.Hunt* and R.St.C.Barnetson*. Department of Dermatot-ogy, Western Infirmary, Gtasgow Gil 6NT, UK, and * Royat Prince AtfredHospitat, Camperdown, NSW, Austratia
A case of minocyoUne-induoed hyperpigmentation occurring duringtreatment for leprosy is presented. A 36 year-old Vietnameseman presented in April 1992 with an 18 month history ofwidespread anaesthetic plaques. Skin biopsy and lymphocytetransformation studies were consistent with borderlinelepromatous leprosy. Treatment was commenced with dapsone,rifampicin and clofazimine. After 23 months the patientreturned with red discolouration of his leprosy plaques andtherefore clofazimine was stopped and replaced with minocycline.Six weeks later however he developed blue-black pigmentationIn the same leprosy plaques. Bicpsy of the blue-black areasdemonstrated a chronic inflammatory cell infiltrate withstrongly positive staining for iron and melanin.
This is the first report of minocycline-inducedhyperpigmentation in leprosy. The clinical features andhistology of this case are discussed with referenceto previously described cases cf minocycline-inducedhyperpigmentation. It is important to consider this sideeffect of minocycline before administration in leprosy,particularly if it is prescribed in place of clofazimine.
REFERENCES1. Granstein RD, Sober AJ. Drug- and heavy metal-induced
hyperpigmentation. J Am Acad Dermatol 1981j5:l-182. Dwyer CM, Cuddihy AM, Kerr REI et al. Skin pigmentoUon
due to minocycline treatment of facial dermatoses. Br JDermatol 1993;129:158-162
1995 Blackwell Science Ltd 277

278 ABSTRACTS
Milia en plaque: a new site and novel treatment. S.G.Keohane,G.W.Beveridge, E.C.Benton and N.H.Cox. University Department ofDermatotop, the Lauriston Buitding, the Royat Infirmary of Edinburgh NHSTrust, Edinburgh EH3 9YW, UK and Department of Dermatotogy, CumbertandRoyat Infirmary, Cartiste, UK
We present two cases of mllla en plaque.CASE 1: a 50 year old dock worker presented with a one year
history of progressive violaceous swelling of both ear lohes. Onexamination the lesions were indurated with comedones. Anautoimmune profile, FBC, ESR, U+Es, glucose and LFTs wereunremarkable. Histology of a skin biopsy demonstrated milia.Oral minocycline (Minocin MR lOOmg) was started and within twomonths of treatment the lesions had almost cleared.
CASE 2: a 54 year old man presented with a six monthhistory of confluent mobile cystic swellings on the pre-auricularareas and on the ear lobes. Skin biopsy was consistent with theclinical diagnosis of miiia en plaque. Treatment has been initiatedwith oral Minocycline.
Miiia en plaque is a rare condition', typically presenting in theretroauricular area without a predisposing cause for miliaformation. Treatment has been limited to topical Retin-A'.Minocycline has not been previously used in this condition.Therefore, these two cases illustrate a new treatment and a novelsite for this unusuai condition.
1. Hubler WR. Rudolph AH. Kelleker RM: MiUa en plaque.Cutis 1978: 22: 67-70.
2. Samlaska CP, Benson PM: MlUa en plaque.Journal ofthe American Academy of Dennatology 1989: 21: 2(1): 311-313.
1995 Blackwell Science Ltd, Clinicat and Experimentat Dermatotogy, 20, 277-278