-
The Fetal Medicine Foundation
Screening for fetal growth restriction
King’s College Hospital and Medway Maritime Hospital, UK
-
The Fetal Medicine Foundation
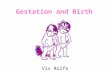
Cnattingius S et al., BMJ, 1998
0
5
10
15
20
25
30
35
40
45
50
Still
birt
h >
28 w
ks (p
er 1
000
birt
hs)
FGRnone
FGRmild
FGRsevere
• 10 yr population study
• 1,083,367 births
• Excluding fetal defects
• 222,975 FGR
• 26,664 severe FGR
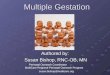
0.0
0.2
0.4
0.6
0.8
1.0
< 3rd4th-5th6th-10th11th-15th16th-25th26th-75th
5 min Apgar < 3
Neonatal death
Seizures < 24 hrs
Neonatal sepsis
Cord pH < 7.0
Intubation at delivery
Birth weight percentile
McIntyre D et al., NEJM, 1999
Screening for SGA / FGRWhy should we screen ?
-
The Fetal Medicine Foundation
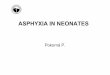
24 26 28 30 32 34 36 38 40 42 44
Gestational age (wks)
Birt
h w
eigh
t (g)
0
1000
2000
3000
4000
5000
50th
90th
10th
Screening for SGA / FGRAssociation with stillbirth
Screening studyKing’s College + Medway MaritimeMarch 2006 – Oct
2015
Study population (n=113,415)Antepartum stillbirths (n=396)
Impaired placentation (n=230)Unexplained + other (n=166)
Yerlikaya G, Akolekar R, McPherson K, Syngelaki A, Nicolaides
KH: Prediction of stillbirth from maternal demographic and
pregnancycharacteristics. Ultrasound Obstet Gynaecol 2016;
48:607-612.
-
The Fetal Medicine Foundation
24 26 28 30 32 34 36 38 40 42 44
Gestational age (wks)
Birt
h w
eigh
t (g)
0
1000
2000
3000
4000
5000
50th
90th
10th
SGA : 71% 44% 27%
Screening for SGA / FGRAssociation with stillbirth
Screening studyKing’s College + Medway MaritimeMarch 2006 – Oct
2015
Study population (n=113,415)Antepartum stillbirths (n=396)
Impaired placentation (n=230)Unexplained + other (n=166)
Yerlikaya G, Akolekar R, McPherson K, Syngelaki A, Nicolaides
KH: Prediction of stillbirth from maternal demographic and
pregnancycharacteristics. Ultrasound Obstet Gynaecol 2016;
48:607-612.
-
The Fetal Medicine Foundation
Starved
The majority of starved fetuses are not SGA
Birth weight percentile0 50th10th 100
Well fed
SGA AGA
?
Screening for SGA / FGRAssociation with BW centile
-
The Fetal Medicine Foundation
Reduced nutrition
Hypoxia
Birth weight percentile0 50th10th 100
Well fed
SGA AGA
Screening for SGA / FGRAssociation with BW centile
-
The Fetal Medicine Foundation
Nicolaides KH, Soothill PW, Rodeck CH, Campbell S. Ultrasound
guided sampling of umbilical cord and placental blood to assess
fetal wellbeing.Lancet 1986;1:1065
18 30 32 34 3624 26 2820 22Gestation (wks)
38
Feta
l blo
od P
O2
(mm
Hg)
10
20
40
30
0
60
70
50
Soothill PW, Nicolaides KH, Campbell S. Prenatal asphyxia,
hyperlacticaemia, hypoglycaemia and erythroblastosis in growth
retarded fetuses. BMJ1987;294:1051
‘Birth asphyxia can precede
labor and is not necessarily
due to the process of birth’
Cordocentesis in SGASome SGA fetuses are hypoxic
pO2 ↓, pCO2 ↓, pH ↓, lactate ↑glucose ↓, erythroblasts ↑
-
The Fetal Medicine Foundation
Nicolaides KH, Bilardo KM, Soothill PW, Campbell S. Absence of
end diastolic frequencies in the umbilical artery a sign of fetal
hypoxia and acidosis.BMJ 1988;297:1026
Cor
d bl
ood
∆ pO
2 (k
Pa)
Cor
d bl
ood
pH
SGA fetuses with umbilical artery AEDF
If abnormal blood flow in theumbilical artery is as good amarker
of prenatal asphyxia inwell grown fetuses as they are insmall
fetuses, this test mayreplace measurement of fetal sizefor the
antenatal prediction offetal asphyxia
Cordocentesis in SGASome SGA fetuses are hypoxic
-
The Fetal Medicine Foundation
Monitoring /timely delivery
12w
36w
22w
Therapy
32w
Lindqvist PG, Molin J: Does antenatal identification of
small-for-gestational age fetuses significantly improve their
outcome? Ultrasound ObstetGynecol 2005;25:258-264.
Pregnancies n = 26,968
SGA: Prenatal detection n = 681
SGA: Postnatal detection n = 573
Adverse outcome• Death: Fetal / neonatal• Brain damage /
hemorrhage• Apgar5
-
The Fetal Medicine Foundation
• Reducing smoking in pregnancy
• Raising awareness of reduced movements
• Risk assessment for growth restriction
• Effective monitoring in labour
Saving Babies’ LivesA care bundle for reducing stillbirths
0
10
20
30
4050
60
80
90
100
70
Det
ectio
n ra
te (%
)
Lindhart et al., The implications of introducing the
symphyseal-fundal height-measurement. A prospective randomized
controlled trial. BJOG 1990; 97: 675-680.
Symphysis fundal height (SFH) measurement in pregnancy for
detecting abnormal fetal growth. Cochrane Database Syst Rev 2015;
97: CD008136.
No difference between measurementof SFH and abdominal
palpation.
Screening for SGA / FGRRCOG Risk assessment
-
The Fetal Medicine Foundation
Screening for SGA / FGR1st trimester assesment
0
10
20
30
40
50
60
70
80
90
100
-
The Fetal Medicine Foundation Preventing stillbirths
Screening for SGA / FGR
Study population:- KCH, MMH 2006 - 2016- Singleton pregnancy-
Dating by CRL at 11-13w- Normal neonate
Total n = 116,758Stillbirth n = 484 (0.4%)
Stillbirth:< 32 w: 41%32-36 w: 19%> 37 w: 40%
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
20 22 24 26 28 30 32 34 36 38 40 42Gestational age (w)
Birt
h w
eigh
t (g)
FMF BW chart
Stillbirth: SGA+/- PE
< 32 w: 80%32-36 w: 51%> 37 w: 27%
-
The Fetal Medicine Foundation
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
20 22 24 26 28 30 32 34 36 38 40 42Gestational age (w)
Birt
h w
eigh
t (g)
Tan et al. Prediction and prevention of small for gestational
age neonates: evidence from SPREE and ASPRE. Ultrasound Obstet
Gynecol 2018. doi: 10.1002/uog.19077.
Stillbirths n = 198
SGA
-
The Fetal Medicine Foundation
12 w
22 w
32/36 w
Assessment at 22 w
Moderate-risk(16%)
Low-risk(60%)
High-risk (0.5%)
90% SGA32-36w
90% SGA> 37 weeks
100% SGA < 32w
Review at32-36 wks
Review at 36 wks
Review at 26-28 wks
Not delivered
Not delivered
Poon LC, Lesmes C, Gallo DM, Akolekar R, Nicolaides KH.
Prediction of small-for gestational-age neonates: screening by
biophysical and biochemical markers at 19-24 weeks. Ultrasound
Obstet Gynecol 2015;46:437-45.
Screening for SGA / FGR2nd trimester assessment
-
The Fetal Medicine Foundation Screening for SGA / FGR
• Use of EFW vs. fetal AC
• Selection of EFW and BW charts
• Gestational age for the 3rd trimester scan
• Additive value of growth velocity
• Additive value of biomarkers
• New proposal for management
3rd trimester assessment
-
The Fetal Medicine Foundation
Screening for SGA / FGREFW vs fetal AC
Model Author All BW< 2500 gBW
> 4000 gBPD Willocks et al., 1964 20.5 35.0 20.9AC Hadlock et
al., 1984 9.9 13.2 8.1FL Warsof et al., 1977 14.8 21.7 17.7AC, FL
Hadlock et al., 1985 8.6 10.0 7.7BPD, AC Warsof et al., 1977 9.5
11.8 8.4HC, AC Hadlock et al., 1984 8.6 10.6 9.4BPD, AC, FL
Ben-Haroush et al., 2008 8.9 12.9 8.1HC, AC, FL Hadlock et al.,
1985 7.8 9.1 8.2BPD, HC, AC, FL Hadlock et al.,1985 8.3 9.8 7.4
Euclidean distance
Euclidean distance: Measure of the proportion of pregnancies
with
EFW within 10% of BW
Hammami A, Mazer Zumaeta A, Syngelaki A, Akolekar R, Nicolaides
KH. Ultrasonographic estimation of fetal weight: development of new
modeland assessment of performance of previous models. Ultrasound
Obstet Gynecol 2018; 52: 35-43.
-
The Fetal Medicine Foundation
Screening for SGA / FGRSelection of growth charts
In reported reference ranges the median BWwith gestational age
for babies born preterm issubstantially lower than that of the
EFW.
90th
50th10th
0500
100015002000250030003500400045005000
20 22 24 26 28 30 32 34 36 38 40 42Gestational age (w)
Wei
ght (
g)
BW chartEFW chart
Nicolaides KH, Wright D, Syngelaki A, Wright A, Akolekar R.
Fetal Medicine Foundation fetal and neonatal population weight
charts. Ultrasound ObstetGynecol 2018; 52: 44-51.
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
20 22 24 26 28 30 32 34 36 38 40 42Gestational age (w)
EFW
/ B
W (g
)
EFW and BW have the same median with GA
-
The Fetal Medicine Foundation
Screening for SGA / FGRGestational age for the scan
Ciobanu A, Khan N, A, Syngelaki A, Akolekar R, Nicolaides KH.
Routine ultrasound at 32 versus 36 weeks’ gestation: prediction of
small forgestational age neonates. Ultrasound Obstet Gynecol 2019;
doi: 10.1002/uog.20258
Routine ultrasound scan• 31+0 - 33+6 w: n=21,989• 35+0 - 36+6 w:
n=45,847
100806040200
100
80
60
40
20
0
Det
ectio
n ra
te (%
)
False positive rate (%)
100806040200
100
80
60
40
20
0
Det
ectio
n ra
te (%
)
False positive rate (%)
Birthweight
-
The Fetal Medicine Foundation
Screening for SGA / FGRAddition of growth velocity
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
202224262830323436384042
Gestational age (w)
Estim
ated
feta
l wei
ght (
g)
B
A
Interval (d)
Growth velocity =B – A / interval
Ciobanu A, Formuso C, Syngelaki A, Akolekar R, Nicolaides KH.
Prediction of small for gestational age neonates at 35-37 weeks’
gestation: contribution of maternal factors and growth velocity
between 20 and 36 weeks. Ultrasound Obstet Gynecol 2019; 53;
488-495.
Ciobanu A, Anthoulakis C, A, Syngelaki A, Akolekar R, Nicolaides
KH. Prediction of small for gestational age neonates at 35-37
weeks’ gestation: contribution of maternal factors and growth
velocity between 32 and 36 weeks. Ultrasound Obstet Gynecol 2019;
53; 630-637.
Scan at 22 and 36 w n=44,043
100
80
60
40
20
0
20
Det
ectio
n ra
te (%
)
0 40 60 80 100
False positive rate (%)
90
70
50
30
10
10 30 50 70 90
EFW + GV
EFW
Scan at 32 and 36 w n=14,497
100
80
60
40
20
0
0 20 40 60 80 100
Det
ectio
n ra
te (%
)
False positive rate (%)
EFW + GV
EFW
-
The Fetal Medicine Foundation
Screening for SGA / FGRAddition of biomarkers
Ciobanu A, Rouvali, A, Syngelaki A, Akolekar R, Nicolaides KH.
Prediction of small for gestational age neonates: screening by
maternal factors, fetalbiometry and biomarkers at 35-37 weeks’
gestation. Am J Obstet Gynecol 2019;220:486.e1-11.
100
80
60
40
20
0
0 20 40 60 80 100
Det
ectio
n ra
te (%
)
False positive rate (%)
Maternal factors+ Estimated fetal weight+ Biomarkers
Routine ultrasound scan • 35+0 - 36+6 w: n=19,209
• Estimated fetal weight• Uterine artery PI• Umbilical artery
PI• Middle cerebral artery PI• Serum PLGF and sFLT-1
-
The Fetal Medicine Foundation
Screening for SGA / FGR
Selection of EFW cut-off
Ciobanu A, Khan N, A, Syngelaki A, Akolekar R, Nicolaides KH.
Routine ultrasound at 32 versus 36 weeks’ gestation: prediction of
small forgestational age neonates. Ultrasound Obstet Gynecol 2019;
doi: 10.1002/uog.20258
0
10
20
30
40
50
60
70
80
90
100
-
The Fetal Medicine Foundation
Screening for SGA fetusesTwo-stage approach
0
10
20
30
40
50
60
70
80
90
100
≤2 2.1-4 >4
%
High-risk 12% (EFW
-
The Fetal Medicine Foundation Screening for SGA fetuses
• Screen at 12 weeks – Aspirin for high-risk
• Screen at 22 weeks – Stratify for follow-up
• Use of EFW vs. fetal AC
• Selection of FMF EFW and BW charts
• 36 w better than 32 w scan
• No additive value of growth velocity
• Minimal additive value of biomarkers
• New proposal for management
Thank you
-
The Fetal Medicine Foundation
Preventing stillbirthsAssessment at 36 weeks
P