Embed Size (px)
Citation preview

Second Curve- a New Strategy for Bending Healthcare’s Cost Curve
The Tenth National QUALITY COLLOQUIUM on the Campus of Harvard University
Cambridge, MAAugust 14,2012
Martin D. Merry, MD, CM andTom Bigda-Peyton, EdD,Second Curve Systems
www.SecondCurveSystems.com

Presentation outlineIntroduction to Healthcare’s Second Curve
A New Performance Curve and Strategy The Cost of Poor Quality
Overuse, underuse, misuse, and waste of careCompeting on valueToward high-reliability
Improving Quality and Bending the Cost Curve: Current StrategiesGovernment/Policy: Health Reform and the Massachusetts experimentEmployer-Based Initiatives: Getting to 50% Cost Reduction (Hannaford,
Asheville, Milstein)ACOs and health system redesign (cases from the US and Canada)
What’s missing/ the Second Curve contributionReliable System Design: a new leverage pointTransforming the Medical-Legal environmentSCS startup strategy
The Net Effect“Way better care at half the cost”: the US 2015 project
2

3
Does This Resonate?“At this point, we can’t afford any illusions (re: health care): the system won’t fix itself, and there’s no piece of legislation that will have all the answers, either. The task will require dedicated and talented people in government agencies and in communities who recognize that the country’s future depends on their sidestepping the ideological battles, encouraging local change, and following the results. But if we’re willing to accept an arduous, messy, and continuous process we can come to grips with a problem even of this immensity. We’ve done it before.”
- Atul Gawande, MD. “Testing, Testing,” The New Yorker, 12/14/09

4
“No problem can be solved from the same level of consciousness that created it. We must learn to see the world anew.”
- Albert Einstein

5
Time
Circa 1910
Healthcare’s Second Curve: A New Performance Curve and Strategy
(Bifurcation curve: 2011)
First Curve/ 4 sigma
(Craft-Age Culture)
(Craft+Information- Age Culture )
-
Future Performance (Second Curve/
6+ Sigma)
“Crossing the Chasm”
Perf
orm
ance

6
1st
2nd

7
Our 1st 2nd Curve Journey
Why must we move from 1st curve health care?What is 2nd curve health care?How 2nd Curve “Bends the Cost Curve”Leadership

8
“The Four Doctors”
Welch
Halsted
Osler Kelly

9
“The most important event in the history of American and Canadian medical education”
(And the birth of health care’s “1st Curve”)

10
1st Curve Health Care’s Performance Problem
1st Curve Health Care (Craft Culture)90% OK 100,00095% OK 50,00099% OK 10,000
Sigma Defects per million1 690,000
2 308,0003 66,8004 6,2105 2306 3.4

11
The “Stealth” Cost Culprit“Cost of Poor
Quality”?*$390 Billion, Annually
* What IOM labels as “overuse, underuse, misuse
and waste”

12
The INEVITABLE consequence managing highly complex health care with a 4 sigma
quality infrastructure
Medical errors as 5th- 8th leading cause of
death in US
44,000 – 98,000 deaths annually

13

14

Toward High-Reliability and Beyond
Less Bounded System
Adaptive Living
System
Normal>>>RWF Grant
(22>>>10)
Reliable High- Reliability
Begin A3s on Falls>>> Use A3s system-wide (12>>>4>>>0)
>>>Ultrasafe
Mechanistic Organizations
Living Organization
s
More Bounded System

16
“ . . . OK, so it’s confirmed the sun will slam into the earth in 3 days. I don’t
want any more gloom and doom, I want suggestions!”

17
Our 1st 2nd Curve Journey
Why must we move from “1st curve”health care?What is 2nd curve health care?

18
The 21st
Century’s Flexner Report?

19
The Vision: 10 Rules of Performance in a Redesigned/2nd Curve Health Care System
1. Care is based on continuous healing relationships.2. Care is customized based on patient needs and
values.3. The patient is the source of control.4. Knowledge is shared, and information flows freely.5. Decision making is evidence based.6. Safety is a system property.7. Transparency is necessary.8. Needs are anticipated.9. Waste is continuously decreased.10.Cooperation among clinicians is a priority.
- Institute of Medicine, Health Professions Education, 2003

20
Columns 2 & 3 = 2nd Curve
Regulation Hammurabi
Legal system
State Boards
JCAHO
“Inspection”
Fed/State regs
ORYX, EMTALA, HIPAA, Etc.
JC, CMS “core
measures”
Medical Science
Hippocrates
Nightingale, 4 doctors
Flexner, Codman, ACS/Hospital
Standardization
M&M conferences
Donabedian,structure process, outcome
Outcomes, Disease
management
Evidence based care, Hospitalists
Management Science
Industrial Revolution
Taylor: “Scientific
Management”
Shewhart
Deming, Juran, Total Quality
Complexity theory
Six Sigma, Lean, Action Learning, Adaptive Design, Resilience
Columns 2+3 = 2nd Curve
Health Care Reform!

21
1st Curve 2nd CurveEvolved around medical and hospital practicesDisease focus, one patient at a timeHierarchical, physician controlledPerformance problems assumed as people-caused“Culture of blame”Fragmentation of care givers and health care functions, “hand-off” gaps commonMedical records paper, frag-mented, “owned” by caregiverComplexity frequent errors, harm to patientQuality is compliance-oriented, 2-4 sigma commonReactive to “sentinel events”
Designed around patient/ community experienceHealth, prevention focus, patient plus populationTeam-based systems outperform hierarchyRecognition that performance problems 95% systems-based“Just Culture”Integration of all system elements, care “seamless” for patientsEHR, “smart cards” owned by patients Integration of “quality sciences”minimizes error, harmQuality, value oriented toward 6+ sigma performance Proactive, O preventable harm

22
Our 1st 2nd Curve Journey
What is our “1st curve dilemma”?What is 2nd curve health care?How 2nd Curve “Bends the Cost Curve”

23
The Policy Environment: Affordable Care Act
New insurance rules guaranteeing coverageHigh-risk pool for people with pre-existing conditionsProtection for children with pre-existing conditionsCoverage for young adults, to age 26Small business tax creditsPreventive care, free for proven servicesEarly retirees temporary reinsurance“Doughnut hole” rebates for MedicareAnnual review of premium increasesAccess to care: $ Billions for Community Health Centers and the National Health Service Corps for low-income and uninsuredNew incentives for providers (ACOs, CMS rewards and penalties, shared gain provisions)

Improving Quality and Bending the Cost Curve: Current Strategies
Government/Policy: Health Reform and the Massachusetts experimentEmployer-Based Initiatives: Getting to 50% Cost Reduction (Hannaford, Asheville, Milstein)ACOs and health system redesign (cases from the US and Canada)
24

25
The “Deming Cascade:” Simultaneous Quality , Cost , Value (W. Edwards
Deming)
Improve Quality
Decrease Cost
Enhance Value
Increase Market
More Jobs
( Process Improvement)

26
Designing New Structures

27
Board of Trustees
• Credentialing• Departmental (Peer)
Review• Surgical Case
Review• Blood UR• Drug Usage Review• Pharmacy and
Therapeutics• Medical Records
Medical Staff Functions(“Silo 1”)
• Nursing• Ancillary• Laboratory• Radiology• Physiotherapy• Risk Management• Finance, Planning• Regulatory Agencies• Etc.
Hospital Functions(“Silo 2”)
Chief Executive Officer
Medical Staff Executive Committee
Our Structural Heritage, 1917-2011 Our structural “fatal flaw”
Management:(industrial culture)
Physicians:(craft culture)
2011: The Structure Hierarchy, Fragmentation, Communication gaps,
Misunderstanding, Power Struggles, etc.

28
Building New Leadership

29
“Command & Control” Pyramid (Taylorism, circa 1900)
Top Management
Obedience
Commands
Hint: Doesn’tWork Anymore

30
“Stewardship/Servant Leadership” (Covey, Block, others)
Top Management
Resources/Support
Caregivers/InnovationThose We Serve

31
Systemic Leadership (Argyris, Schon, Senge)
Improve Quality
Decrease Cost
Enhance Value
Increase Market
More Jobs
( Process Improvement)

Systemic Leadership (Argyris, Schon, Senge)
Copyright Action Learning Systems 2005 32
BBehavior
Environment
Industry/Sector
Organization
Thoughts, Feelings, Intuitions
Beliefs, Assumptions
Governing Values
Myths, Legends, Heroes
Intended
Consequences
UnintendedConsequences

33
1 stCurve 2nd Curve
Are we ready to board the “2nd Curve boat”?
“Void”

34
Case examples

35

36
The ThedaCare Breakthrough“Realizing that ThedaCare needed change, leaders tried one improvement program after another over the course of many years. Most of the programs offered incrementally better results for a while, until everyone slid back into old habits. Finally . . leaders started thinking about breaking down the divisions between caregivers’specialties, divisions of labor and habits of working to create a unified focus on the patient. Because this would require change in everyone involved, it was clear that hospital units needed a revolution instead of isolated, incremental adjustments.”

Breakthroughs in progress?
Iowa Health System: no falls for____Baylor U. Health System:Ontario Health System: Excellent Care for All Act and StrategyResilience Engineering and Learning Network: Vancouver, B.C.
37

38
In Summary . . . “1st Curve” health care has run its course. It is unsustainable financially and quality-wise, and in search of a new paradigm. Fortunately that new paradigm is already emerging, awaiting our embrace. Emerging now is “2nd Curve” health care, a patient and community-centered system that will be better than we can now imagine.The greatest challenge of moving to the 2nd Curve is for health care leaders, and perhaps uniquely physician leaders, to understand and embrace this paradigm shift. They will be crucial, at the national, regional, and local levels in maximizing our nation’s ability to move toward higher value health care that can fulfill the desires and commitment of virtually all health caregivers
- Martin Merry, MD

What’s missing/ the Second Curve contribution
Reliable System Design: a new leverage point
Transforming the Medical-Legal environment
SCS startup strategy
39

40
Patients and Families as Part of the Care Team
Home care/ Telemety
Team-basedcare
PharmacyNursing/NP/PA Care
Social Work
Spiritual Healing
Reliable System Design
Community Partnerships!
MD
Leadership, Co-Management
AccountableCare
Organizations
Case Mgt

41
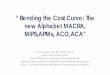
Observed & Expected Operative Mortality
Concord Cardiac Surgery 7/6/98 to 12/31/01
010203040
0 200 400 600
sequential patients
deat
hs 3sd higexpecteobserv
(4.8) Concord Expected
(2.1) Concord Observed(0.3) Salem Observed
All Case Operative Mortality
Concord Expected (NNE Risk Model)
Concord Observed
Salem Observed
All Case Mortality (percent)(When Team- base care, Informatics
entered)

42
And the Caregivers ?Heroes!2 lives saved by ER, ICU and NICU teamsDeeply grateful family
(Does it get any better?!)
2 weeks before trial, all 3 physicians and hospital settle lawsuitsHeadline story in local press1 physician censured by state board of medicine(And can we imagine what it must be like for these physicians today – and for how long?)
(But does anyone believe that the OB office did a “near miss” root cause analysis on their telephone triage practices?)

Transforming the Medical-Legal Environment
Just CultureRelational LawSystemic Law
43

Life Sciences
Life Sciences
Medical
DevicesMedical
Devices
SuppliersPayors and Funders
Increase Access to centers of
excellence
Increase Access to Outpatient CareLack of community services
Need for communitynavigation
Community services need to focus on recovery and medical issues
Increase access to rehab for acute chronic conditions
Lack of awareness of Community programs
Long waits for Services in the community
Taking a regionalperspective on research
Increase connections withPrimary care
Expanding CaregiverPilots
Expand wellness programs– e.g. Fit for Function
Need for strategicCollaborations/partnerships
Increase need for Peer support –
survivor groups
SCS Startup Strategy
Biotech
Technology
Need to focus on transitions
•Improve Care•Reduce Cost•Create Jobs
Need to create systemsperspective on care
Need to collaborate withother strategies – i.e. COPD, Diabetes, cardiovascularImportance of timeliness
of treatment
Increase in options for
community re‐integration
Translate Data into practice
Unique challenges for specific populations of care
Lack of accountability in Hospital Planning
Delivery System
Hospitals, Providers, Care
Networks
Increase partnerships with case management
Coordinated Pediatric Care

45
Time
1910
2 Historical Curves of Health Care Innovation(derived from Kuhn, Toffler, Morrison, Merry)
(Bifurcation curve: 2010)
First Curve/ 4 sigma
(Create and Build
Momentum)
(Transfer/Sustain Momentum)
-
Future Performance (Second Curve/
6+ Sigma)
“Crossing the Chasm”
Perf
orm
ance
“Theoretical Ideal”

Toward Resilient Systems
Today1930 1980
THEORY OF ERRORAnalyze accidents and system failureAvoid unacceptable risk with rules complianceFocus on what
goes wrong because we know how things work
THEORY OF ACTIONFocus and appreciate the barely noticeable traits of everyday safe and productive work Learn how the system adjusts to sustain performance under expected and unexpected conditions
Robus
t
Resili
ent
Source: Erik Hollnagel
Curve ICurve II
46

47
Way Better Care at Half the Cost: the US 2015 Project
Healthy Behavior Credit for all employees, the self-insured, and Medicare/Medicaid recipients;Collaborative Care Model for chronic and persistent conditions;Medical Village Model to create care coordination and patient navigation and align specialists with primary care;Wellness Advantage, a scalable worksite wellness initiative that combines local campaigns with regional and national action learning networks; andCommunity Hearth/Mosaic, a program that combines learnings from the self-help movement, story-based focus groups, and community health outreach to create local self-reliance, improve population health, and build community resilience.

The Net Effect When implemented in an ACO, health system, state, or region, the US 2015/Second Curve program results in the following:
Reduction of the cost of care to globally competitive levels (e.g. from 18% to 12% of GDP);
Improvement of quality to highly reliable levels (on par with high-performing systems in other industries);
Patient safety improvement to the level of ultrasafety, thus making healthcare as safe as commercial aviation;
Economic magnet zones, supported by an economically sustainable community health model.
48

49
2nd
Curve