Embed Size (px)
Citation preview
Gardner-Webb UniversityDigital Commons @ Gardner-Webb University
Nursing Theses and Capstone Projects Hunt School of Nursing
2012
Second-Year Associate Degree Nursing (ADN)Self-Efficacy in Relation to Simulation LabExperiencesSarah W. TateGardner-Webb University
Follow this and additional works at: https://digitalcommons.gardner-webb.edu/nursing_etd
Part of the Medical Education Commons, Nursing Administration Commons, and theOccupational and Environmental Health Nursing Commons
This Thesis is brought to you for free and open access by the Hunt School of Nursing at Digital Commons @ Gardner-Webb University. It has beenaccepted for inclusion in Nursing Theses and Capstone Projects by an authorized administrator of Digital Commons @ Gardner-Webb University. Formore information, please see Copyright and Publishing Info.
Recommended CitationTate, Sarah W., "Second-Year Associate Degree Nursing (ADN) Self-Efficacy in Relation to Simulation Lab Experiences" (2012).Nursing Theses and Capstone Projects. 145.https://digitalcommons.gardner-webb.edu/nursing_etd/145
SECOND-YEAR ASSOCIATE DEGREE NURSING (ADN) SELF-EFFICACY IN
RELATION TO SIMULATION LAB EXPERIENCES
By
Sarah W. Tate
A thesis submitted to the faculty of
Gardner-Webb University School of Nursing
In partial fulfillment of the requirements for the
Degree of Master of Science in Nursing
Boiling Springs
2011-2012
Submitted by: Approved by:
_______________________ _______________________
Sarah W. Tate Mary Alice Hodge, PhD, RN
_______________________ _______________________
Date Date
ii
Abstract
Second-Year Associate Degree Student (ADN) Self-Efficacy in Relation to Simulation
Lab Experiences utilized a convenience sample of second-year associate degree nursing
students to conduct a survey of their perceptions of an increase in self-efficacy or self-
confidence in relation to their simulation lab experiences. Albert Bandura’s theory of
self-efficacy was the theoretical framework for the study. Students who have high levels
of self-efficacy have been shown to handle obstacles with less stress, perseverance, and
success. In this study, 85% of the students agreed that simulation lab experiences were
beneficial in increasing their confidence to perform safely in their preceptorship and as
new graduate nurses.
iii
Table of Contents
Chapter I
Introduction .............................................................................................................1
Statement of the Problem .............................................................................1
Purpose .........................................................................................................3
Background ..................................................................................................3
Significance to Nursing................................................................................4
Theoretical Framework ................................................................................4
Definition of Terms......................................................................................7
Research Question .......................................................................................8
Conclusion ...................................................................................................8
Chapter II
Review of the Literature ..........................................................................................9
Introduction ..................................................................................................9
Literature Review.......................................................................................10
Summary ....................................................................................................16
Chapter III
Method ...................................................................................................................18
Setting & Subjects......................................................................................18
Sampling ....................................................................................................18
Instruments .................................................................................................18
Procedures ..................................................................................................19
Ethical Considerations ...............................................................................20
iv
Data Collection & Data Analysis Procedures ............................................20
Chapter IV
Results ....................................................................................................................21
Statistical Presentation ...............................................................................23
Preparation for precepted experience results .......................................23
Roles and critical thinking results ........................................................24
New nurse graduate responses .............................................................24
Chapter V
Discussion ..............................................................................................................27
Interpretation of Findings ..........................................................................27
Implications for Nursing ............................................................................28
Implications for Further Research .............................................................28
Conclusion .................................................................................................29
References ..............................................................................................................30
Appendices
Appendix A: Simulation Experience Questionnaire ..................................34
Appendix B: Introduction to Survey ..........................................................40
Appendix C: Simulation Experience Survey Consent ...............................42
Appendix D: Comments from Students .....................................................44

v
List of Figures
Figure 1: Concept-Theory-Empirical Research Method Model (CTE)……………..7
vi
List of Tables
Table 1: Second-Year Associate Degree Student (ADN) Self-Efficacy in Relation to
Simulation Lab Experiences ..................................................................................21
Table 2: Descriptive Statistics ...............................................................................22
1
Chapter I
Introduction
Statement of the Problem
Patient safety is one of the highest priorities in nursing care whether in acute care
facilities, non-acute facilities or in the community. Educators of nursing students must
provide opportunities for students to learn how to provide safe care. Simulation
experiences allow educators to provide a safe environment for students to practice care,
learn to handle changes in patient conditions, and manage potential adverse events (Gore,
Hunt, & Raines, 2008). Nursing students need to be able to experience situations with
patients they may encounter during clinical rotations and after graduation from nursing
school as new graduate nurses. Learning how to respond in these situations through
clinical simulations can provide a safe environment in which to practice physical skills,
develop clinical judgment, and critical thinking skills.
Simulation is about the whole learning experience – not just the mannequin. It
incorporates “theory, assessment, pharmacology, pathophysiology, and psychomotor
skills – all of which lead to the development of clinical judgment” (Gore et al., 2008, p.
58). Simulation can be described as low-fidelity to high-fidelity with low-fidelity
including such things as case studies or role-play, low-technology mannequins for
practicing psychomotor skills such as an intravenous (IV) arm or a static head, and trunk
to practice airway management or urinary catheter insertion, and high-fidelity
mannequins that are connected to computers. The military and the field of aviation began
using simulation in the 1970’s for training purposes, and health educators have learned
from their experiences (Jeffries, 2007).
2
Simulation technology has evolved into a level of sophistication and realism in
which the learner can experience a wide range of scenarios that can help in “making
sound decisions in unpredictable health care situations” (Macedonia, Gherman, & Satin,
2003, as cited in Jeffries, 2007). Herm, Scott, and Copley, (2005) found that a simulation
experience to assess the synthesis of knowledge of their students during clinical rounds
provided important insights for the instructors and the students. Some students who were
thought to have a good grasp of the required behaviors and thought processes did not, and
vice versa. One student commented, “I learned more from this simulation exercise than
any other test or paper I’ve written” (p.29). Another student verbalized an understanding
of now I know “what I’m supposed to be doing in clinical” (p.29). The purpose of the
study, Second-Year Associate Degree Nursing (ADN) Student Self-Efficacy in Relation
to Simulation Lab Experiences, was to examine the second year ADN’s perception of
whether simulation experiences during their two-year program of study prepared them for
their clinical preceptorship at the end of their course of study, and for becoming safe and
confident new nurse graduates.
New graduate nurses in the acute care arena have many new roles to adapt to,
perhaps with some expectations in conflict with what they have practiced as a student
(Duchscher, 2008). Duchscher describes transition shock experienced by new nurses as
they acclimate to acute care employment, including stress, frustration, discouragement,
disillusionment, and the high rate of new nurses who change their place of employment
or leave nursing in the first year (2008). Newly graduated nurses who have a high sense
of self-efficacy may be more successful in this journey of transition. Simulation
experiences can bolster confidence levels by providing non-threatening practice
3
opportunities. High self-efficacy can help the new nurse to recover from the frustrations
and discouragement of the first years as a practicing nurse (Bandura, 1994).
Purpose
Nursing is a challenging and rewarding field where much preparation is required
to become a safe and knowledgeable new graduate nurse. There can be opportunities to
build skill and confidence with simulations as the student practices in scenarios before
and during patient contact. The purpose of this study was to measure the second year
student ADN’s perceived positive or negative influence of simulation experiences on
their confidence level in relation to preparing them for a preceptorship and becoming
safely practicing new nurse graduates.
Background
Albert Bandura, psychologist, author, and professor, is the founder of Social
Cognitive Theory and the Theory of Self-Efficacy. Bandura (2004) described efficacy
beliefs of students as having an influence over goals and aspirations, how obstacles are
handled, and the level of perseverance to overcome and be successful. “The stronger the
perceived self-efficacy, the higher the goals people set for themselves and the firmer their
commitment to them . . .” (p. 145). Bandura’s theory supports the reasoning behind the
use of simulation – to increase student self-efficacy, to help them believe in themselves
and have the confidence to be successful in their clinical encounters and as new nurses.
Simulations can be as simple as a body part used to practice a specific skill, such
as an arm to practice inserting an intravenous (IV) catheter, or as complicated as a room
full of high fidelity mannequins that speak and respond with programmed body functions
(Gore et al., 2008). The experience can enhance learning or merely be one more
4
assignment in the long list of nursing school requirements. The quality of the experience
may depend on the instructors, the design of the simulation, and on the preparation of the
students (Smith & Roehrs, 2009).
Significance to Nursing
Self-efficacy is the belief in oneself, the belief that obstacles can be overcome,
that through perseverance, goals are met. Strong self-efficacy supports a can-do attitude
that provides assurance of being able to control threatening situations, and reduces
personal stress (Fritscher, 2009). Bandura’s theory states that the most effective means of
influencing self-efficacy is through mastery experiences (1994).
Simulation can offer the opportunity to master skills, or situations with patients
that could likely occur in the clinical setting. Self-efficacy can be gained through practice
of new skills when the student masters the skills and through social modeling, or
watching others in similar circumstances succeed (Bandura, 1994). Simulation offers
both options when the student is in the primary caregiver role or in the observer role. The
question is whether the ADN student nurse perceives simulation experiences as adding to
their sense of confidence in relation to practicing safely in the clinical preceptorship and
as a new nurse graduate.
Theoretical Framework
Albert Bandura’s Theory of Self-Efficacy was chosen for Second-Year Associate
Degree Nursing (ADN) Student Self-Efficacy in Relation to Simulation Lab Experiences
because this theory defines how people or students regulate their behavior based on their
self-efficacy or “their beliefs in their own capabilities” (Pajares, 2004, para. 28). Within
this framework, efficacy is shown to influence decisions, affect performance, thinking,
5
motivation and success (1994). The use of simulation exercises to promote high levels of
self-efficacy include not only the reinforcement of mastering the skill or situation through
practice, but also vicariously through watching others successfully master the skill or
situation, and by allowing the student to make mistakes without judgment and to practice
until mastery is achieved (Bandura, 1994). In educational research, it has been shown that
students with positive self-efficacy “work harder, persist longer, persevere in the face of
adversity, have greater optimism and lower anxiety, and achieve more” (Pajares, 2004,
para. 29).
There are four major psychological processes involved in self-efficacy. Cognitive
processes involve thought processes. Those with high self-efficacy develop skills to
process information that includes many ambiguities and uncertainties, setting challenging
goals and using analytic thinking (Bandura, 1994). Motivational processes involve
forming beliefs about what can be accomplished and planning courses of action based on
these beliefs. Those with high self-efficacy state that their failures are due to lack of
effort, while those with low self-efficacy state that their failures are due to low ability
(Bandura, 1994). Affective processes involve stress reactions, depression, fear, and
anxiety. Mastery experiences that are integral to simulation practice help to conquer these
feelings and develop higher self-efficacy. Selection processes involve beliefs in personal
efficacy shaping the course taken in life. People undertake activities and situations they
feel capable of handling (Bandura, 1994).
In this study, Second-Year ADN Student Self-Efficacy In Relation to Simulation
Lab Experiences, students were evaluated for their perceptions of self-efficacy. Bandura
discussed the importance of self-belief in determining successful outcomes for the future.

6
Students may not feel confident in their abilities as new nurses due to the reality of high
patient acuities, shorter patient stays and critical staffing shortages, and causes high stress
atmospheres for learning (Jeffries, 2007). Simulation practice in clinical lab affords
students the opportunity to practice in safety, both for them and for the patient. Skills
learned in simulation lab practice can be perfected with repetition. Affective processes of
stress and anxiety can be reduced with practice and repetition. The student can gain in
self-efficacy with practice that allows mastery of the skill or situation. Simulation can
help to develop cognitive processes by having students think their way through situations.
Experiencing many different kinds of experiences will expand the thought processes
needed to work through situations. Having productive experiences in simulation lab can
improve motivation to continue and reach further through active learning (Jeffries, 2007).
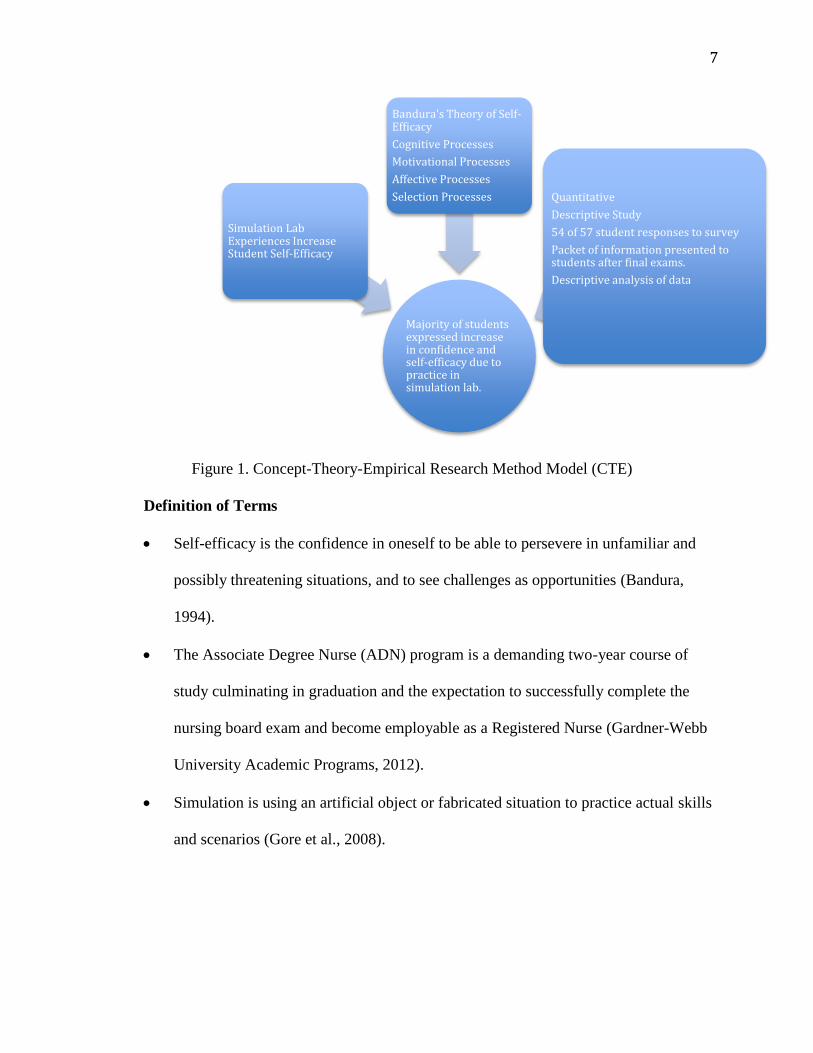
The concept-theory-empirical research method diagram reveals the relationships
between Bandura’s theory of self-efficacy and this study of simulation experiences
and increased self-efficacy.
7
Figure 1. Concept-Theory-Empirical Research Method Model (CTE)
Definition of Terms
Self-efficacy is the confidence in oneself to be able to persevere in unfamiliar and
possibly threatening situations, and to see challenges as opportunities (Bandura,
1994).
The Associate Degree Nurse (ADN) program is a demanding two-year course of
study culminating in graduation and the expectation to successfully complete the
nursing board exam and become employable as a Registered Nurse (Gardner-Webb
University Academic Programs, 2012).
Simulation is using an artificial object or fabricated situation to practice actual skills
and scenarios (Gore et al., 2008).
Majority of students expressed increase in confidence and self-efficacy due to practice in simulation lab.
Simulation Lab Experiences Increase Student Self-Efficacy
Bandura's Theory of Self-Efficacy
Cognitive Processes
Motivational Processes
Affective Processes
Selection Processes Quantitative
Descriptive Study
54 of 57 student responses to survey
Packet of information presented to students after final exams.
Descriptive analysis of data
8
Research Question
The purpose of this study, Second-Year Associate Degree Nursing (ADN)
Student Self-Efficacy in Relation to Simulation Lab Experiences, is based on the question
of whether second- year ADN students perceived that simulation experiences in clinical
laboratory practice increased their self-efficacy for safely practicing in a preceptorship
and as new nurse graduates.
Conclusion
Simulation exercises can provide a means for nursing students to master a skill
needed in the clinical arena without jeopardizing the safety of patients. Bandura’s theory
of self-efficacy supports the use of simulation exercises to promote self-confidence in
nursing students in dealing with new experiences, new skills and new situations in a
productive manner that will lead to successes. The question to be answered was whether
this group of graduating student nurses’ perceived simulation exercises as beneficial to
increasing self-efficacy for completing a preceptorship and for entering the workforce
and practicing safely as a new nurse graduate.
9
Chapter II
Review of the Literature
Introduction
The literature reveals several studies that have examined the use of high fidelity
simulation (HFS) and the relation to student satisfaction and self-confidence (Bambini,
Washburn, & Perkins, 2009; Bearnson & Wiker, 2005; Feingold, Calaluce, & Kallen,
2004; Goldenberg, Andrusyszyn, & Iwasiw, 2005; Henneman & Cunningham, 2005;
Smith & Roehrs, 2009), student anxiety reduction with simulation (Bremner, Aduddell,
& Amason, 2008), and improving therapeutic communication skills (Kameg, Howard,
Clochesy, Mitchell, & Suresky, 2010). These studies were conducted in relation to
specific areas, such as critical care, medical-surgical, obstetrics, mental health, and
postoperative patients. They were all conducted with baccalaureate (BSN) level students
early in their nursing course of study, with the exception of Kameg et al. (2010) who did
not identify participants other than as nursing students.
High-fidelity simulation includes mannequins that are the most realistic and life-
like, are interactive with pulses, breath sounds, bowel sounds, voices, and other attributes,
and scenarios where the equipment and room most resemble an actual clinical situation.
The simulation experience in these instances minimizes the need to pretend that
equipment is available or that the patient has a certain response; however, a complete
high-fidelity simulation lab with several high-technology mannequins and fully stocked
hospital rooms and equipment can cost in the millions of dollars (Jeffries, 2007).
The focus was different in Second Year Associate Degree Nursing (ADN)
Student Self-Efficacy in Relation to Simulation Lab Experiences, where the second-year
10
associate degree nursing student (ADN) was giving their perception of the overall
simulation experience from the previous two years and how it related to self-confidence
in participating in a preceptorship experience, and preparing for the role of new nurse
graduate. These students compared their simulation experiences as a whole instead of
evaluating only their most recent simulation experience. The type of mannequin or
simulation was not figured into the survey and could have been a limiting factor in the
outcome of the survey.
Literature Review
Smith and Roehrs (2009) found a relationship between the design characteristics
of the simulation and the level of satisfaction of the student. These design characteristics
included objectives, support, problem solving, guided reflection and fidelity. Among
these characteristics, problem solving (0.558) and objectives (0.573) were most important
in contributing to self-confidence at a significance level of 0.01. The other characteristics
were significant at a lower rate: support (0.508), guided reflection (0.447) and fidelity
(0.430). This research suggests that the design of the simulation is a very important
aspect of the satisfaction and the self-confidence gained by the student. The limitations of
this study were, a small sample size (68), and it was limited to a group of junior BSN
students in their first medical-surgical course.
Bambini et al. (2009) suggested that simulations improve responses to complex
situations and promote student confidence to deal with ever-changing patient scenarios.
Bandura’s framework of self-efficacy is utilized to explain student gains in self-efficacy
when utilizing simulated experiences in lab settings. Self-confidence in performing a
post-partum exam was measured in this group of students who were preparing for their
11
first clinical experience. The simulation included the skills of performing vital signs,
breast exam, assessing the fundus, assessing lochia, and patient teaching. All were found
to have a significant positive increase for the students in relation to preparation for the
clinical experience. These students expressed an increase of confidence in being able to
communicate with the patient, with the physical skills needed for the assessment of the
patient, and in the ability to recognize priorities of care. A limitation of this study was the
variability of student experiences due to individual interactions during the simulations
that may have caused different learning outcomes. Also, with no control over who chose
to participate in the study, validity could be compromised due to selection threat.
Bremner et al. (2008) found that students expressed a reduction in anxiety for
their first clinical experience when they practiced scenarios with a simulator. The
simulation experience presented a non-threatening atmosphere for practice for these first-
year BSN students. Findings included a need for well-articulated learner outcomes that
clearly related to the course offerings and the clinical objectives.
Kameg et al. (2010) studied student self-efficacy in relation to improving
therapeutic communication skills before students were to participate in a mental health
clinical rotation. The researchers used Bandura’s self-efficacy theory as the theoretical
structure, finding that students often have difficulty and anxiety related to communicating
with mentally ill patients and simulation could bridge the gap in preparation for these
encounters. The survey data of this study showed that the students were generally in
favor of the simulation experience; that it was a valuable learning experience, it should be
included in the curriculum and that the knowledge could be transferred to the clinical
setting. These students did not believe it should be a replacement for experiences in the
12
clinical setting. Limitations of this study included the inability of the simulator manikin
to show facial expressions, which are an integral component of personal communication,
and small sample size of 38.
Radhakrishnan, Roche, and Cunningham (2007) designed a study to measure
clinical skills using a simulation evaluation tool. This study was quasi-experimental with
a control group. The results found a correlation between clinical sessions with
simulations and improved performance in properly identifying patients and assessing
vital signs (p=.001 and p=.009 respectively).
Gore et al. (2008) completed a study using mock hospital rooms and simulation
experiences over a four-hour session. The students were given the chart information for
each patient that included history, laboratory reports, EKG results, radiology reports,
physician orders, medication records, progress notes, nurse’s notes, and interdisciplinary
notes. Each student cared for one patient except, for a post trauma patient that had two
students assigned. One notable incident occurred when a student left her room to help
another student but left the patient bed in a high position with bed rails lowered. The
instructors disconnected the patient from all tubing and placed the patient on the floor.
The student returned and moved the patient back to the bed and reconnected the IV,
urinary catheter, and oxygen, then reported to the instructor charge nurse. These students
learned how to complete an incident report and passed their information along to other
classes about the importance of patient safety. The instructors had no other issues with
patients falling from bed. These students learned through what Bandura would call
modeling. They did not have to experience it themselves to learn the significance.
Limitations of this study included the need to develop reliable tools to monitor outcomes.
13
Students have differing learning styles, and Fountain and Alfred (2009) studied
which learning styles were most conducive to simulation experiences. This was a post-
test study using a convenience sample of 76 baccalaureate-nursing students and showed
that two learning styles were most associated with satisfaction using simulation – the
social learning and solitary learning styles. Social learning styles comprise interacting
with others, comparing and listening and were supported by 76% of the students. The
study supported simulation to be an effective learning tool for students with differing
learning styles. Limitations of this study include small sample size limited to one school
of nursing and potential group perception bias.
Lee, Lee, Wong, Tsang, and Li (2010), established an integrated skills training
center in Hong Kong. Within this training center were high-fidelity simulators, low-
fidelity simulators, virtual reality simulators and static simulators. The researchers found
the static and low-fidelity simulators useful to hone psychomotor skills, the high-fidelity
simulators more useful in integrating critical thinking skills and consolidation of
information, and the virtual reality simulators useful in the mental health arena due to the
student being able to see what the patient sees to get an understanding of care needed.
The researchers expressed the importance of faculty buy-in and adequate training on an
ongoing basis. These researchers recognized the importance of evaluating the impact on
student learning and outcomes and formed a group for those means.
Paskins and Peile (2010) studied final year medical students’ views on
simulation-based teaching. Findings included the importance of feedback, integration into
the curriculum, repetitive practice, confidence, and increased self-efficacy, anxiety,
realism, and teamwork. Over half of the 28 medical school students from the United
14
Kingdom who participated in this study, discussed the technical limitations of the
medium-fidelity simulators. Teamwork was found to be beneficial for those who usually
did not choose the team leader role to be in a position of delegating tasks, and for those
natural leaders to be in the supportive positions helped them to gain a sense of those
roles’ needs. The researchers found that some students felt the simulation exercises were
more stressful than a real-life emergency, and that feedback could profoundly affect
positive or negative confidence levels. Some students were found not to like the role-play
aspect of simulations, where others felt it helped them to grow in their learning styles.
The researchers felt an independent researcher for analysis could possibly improve
reliability and further expressed limitations due to single institution and single clinical
group results. The researchers felt, “further work is needed to expand on the effect of
simulation-based teaching on confidence, anxiety and self-efficacy particularly” (p. 576).
Anthony, Carter, Freundl, Nelson, and Wadlington (2012) discussed the need for
nursing students to become proficient in the care of veterans, who often have special
needs that relate to experiences during tours of duty. Nurses will encounter veterans in
locations other than at veteran’s hospitals, and there is a need for some specialized
knowledge relating to effects of environmental conditions or chemicals the veterans may
have been exposed to, and to their mental states. Many veterans may experience post-
traumatic stress disorder (PTSD), depression, ill effects from traumatic brain injuries,
substance abuse issues, diabetes, Chronic Obstructive Pulmonary Disease (COPD),
congestive heart failure, Parkinson’s disease, ischemic heart disease, prostate cancer, and
other conditions. While most of these conditions also occur in the general population,
15
there may be unique combinations in veterans. There is a movement in the American
Nurses Association since 2008 to increase awareness of veterans’ needs among nurses.
Anthony et al. (2012) devised a simulation scenario to be used to disseminate
information to improve the quality of care for veterans. The researchers’ scenario was
developed to help nursing students increase awareness of veteran’s needs, improve
prioritization in planning and implementing veteran centered care, apply principles of
patient safety, identify symptoms of PTSD, interpret lab values and diagnostic tests, and
communicate effectively with the interdisciplinary team. A difference with this
simulation study mentioned roles of a family member and the voice of the patient, in
addition to the nurse and the nurse reporting to the student. The study gave the whole
scenario including the information given to the student, roles, what the patient says, what
the family says, and the expectations of the student. Debriefing was in a non-threatening
atmosphere using open-ended questions from the faculty, then challenging the students to
identify opportunities for improvement, and finally re-examined for the scenario’s
relation to the nursing process. The scenario developed by the researchers can help to
provide culturally aware care for nursing students and practicing nurses.
Reinhardt, Mullins, De Blieck, and Schultz (2012) studied whether high-fidelity
simulation increased the ability of students to insert an intravenous catheter (IV) over a
task trainer IV arm. Ninety-four junior baccalaureate nursing students were included in
this experimental, randomized, controlled study. Findings included no significant
difference between simulation models (p= .7), and no significant difference in student
confidence score between simulation models. As well, the ability to insert an IV into a
live patient did not correlate with either instruction method.
16
Wilt and King (2012) developed a curriculum of simulation labs for an
accelerated BSN program, discussing the obstacles overcome and the inspirations for
future improvements. Two of the challenges overcome included timing and scheduling
for this accelerated program and the amount of time to orient these students to the
simulation experience. These were overcome by adding another mannequin, scheduling
the students on the other half of the day they had clinicals, and providing video
orientation on Blackboard to decrease the time it took to orient the students to the
simulation lab and process. A goal of this study was to fully involve clinical faculty in the
simulation activities, including developing scenarios and offering feedback to students.
Summary
There are a number of studies that address using simulation as an adjunct to
preparation for clinical experiences. Overall these studies have shown popularity among
nursing students for this method of teaching and learning, and have been shown to be
perceived as increasing self-efficacy in early clinical experiences, individual clinical
experiences for specific specialties such as medical-surgical, mental health, veterans,
post-operative and obstetrics patients, and communication with patients. Second-Year
Associate Degree Nursing Student Self-Efficacy in Relation to Simulation Lab
Experiences studied the perceptions of ADN graduating nursing students in relation to
their self-efficacy from simulation experiences in preparation for preceptorship and as
new nurse graduates.
This study differed from the previous studies in the placement of the evaluation in
relation to the location in the course of study, and in the focus of the study. The group of
students in Second-Year ADN Self-Efficacy in Relation to Simulation Lab Experiences

17
had completed their two-year course of study. Their evaluation of simulation was a
cumulative view of overall experiences with simulation. The focus was based on whether
the students experienced an increase in self-efficacy due to their simulation experiences.
18
Chapter III
Method
Setting and Subjects
Second-Year Associate Degree Nursing (ADN) Student Self-Efficacy in Relation
to Simulation Lab Experiences involved responses from a subset of nursing students in a
private university in the Piedmont region of North Carolina. This university offers pre-
licensure, post-licensure and graduate degrees in nursing. The subjects for this study were
enrolled in the pre-licensure, specifically the associate degree program. The ADN
program was selected due to this class readying for graduation, having finished their
course of study. This class had experienced two years of simulation lab assignments and
was evaluated for their perceptions of increased confidence due to the practice in those
labs.
Sampling
The convenience sample of second-year ADN students, who were readying to
graduate and prepare for their nursing board exam and their first position as new nurse
graduates, were of various ages and both genders. Demographic information was not
collected during the study. The survey questionnaire was offered to the entire class after
completion of their final examinations at the end of the semester. The class consisted of
57 potential research subjects of which 54 participated (95% return rate).
Instruments
A survey tool was designed by the researcher and evaluated by content experts for
relevance and content validity. After revision based on feedback, the survey consisted of
twelve questions with a Likert-type scale (Trochim, 2006), including categories from 1-5,
19
strongly disagree, disagree, undecided, agree and strongly agree, respectively, and a
section at the end of the survey for additional comments. The tool was designed to
measure students’ perceptions of whether simulation experiences during lab sessions
prepared them for their preceptorship, for becoming a new graduate nurse, for
administering medications safely, giving a nursing report, learning patient assessments,
communicating with physicians, and enhancing learning (see Appendix A). The survey
data were scored according to the answer chosen from 1 – 5, with equal intervals between
the numbers representing the scores, with 5 as the highest positive score and 1 as the
lowest positive score. The open-ended comments were evaluated for common themes.
Procedures
The study was presented to the students as a packet of information after they
completed final exams, but while still in the classroom (see Appendices A, B, C). The
instructors who were present to proctor the student exams offered the information to each
student. The researcher was not present during the survey. The packet included an
introduction to the study and to the researcher with contact information, a consent form
with an area for a request of the results of the study that could be detached for anonymity,
a debriefing statement with instructions on how to complete the survey, and the twelve-
question survey. Envelopes were provided to each student and students were asked to seal
the envelopes before turning them in.
Prior to beginning the study, students were presented with the informed consent
document as part of the survey packet (see Appendix C). The informed consent form
detailed the purpose of the study and the rights for participating in the study. Each student
had the opportunity to read and have explained the information on the consent form. At
20
any time during the survey, the subject could have declined to participate in the study.
The consent discussed the anonymity of each participant. No identifying information was
included on the survey and if the participant requested results, they could detach the sheet
with their contact information and turn it in separately.
At the completion of the survey, the instructor collected the sealed envelopes in a
folder provided by the researcher. The completed surveys were held in a locked office for
researcher retrieval.
Ethical Considerations
Prior to survey administration, approval was received from the Institutional
Review Board (IRB) of Gardner-Webb University and consent was obtained from each
study participant. It was determined by the researcher that there was no risk involved for
the participants due to complete anonymity. The researcher had no involvement with the
study participants.
Data Collection and Data Analysis Procedures
Surveys were numbered for reference and data was entered in spreadsheet format
in Microsoft Excel and in Statistical Package For Social Sciences (SPSS, vs.20) software
for analysis. The responses for each question were aggregated according to Likert
categories of, 0=No Answer, 1=Strongly Disagree, 2=Disagree, 3=Undecided, 4=Agree,
5=Strongly Agree. Survey data were analyzed to obtain item descriptive statistics
including mean, standard deviation, frequency and percentage of student responses per
response category and question. The additional comments at the end of each survey were
analyzed for frequency of common themes (See Appendix D).
21
Chapter IV
Results
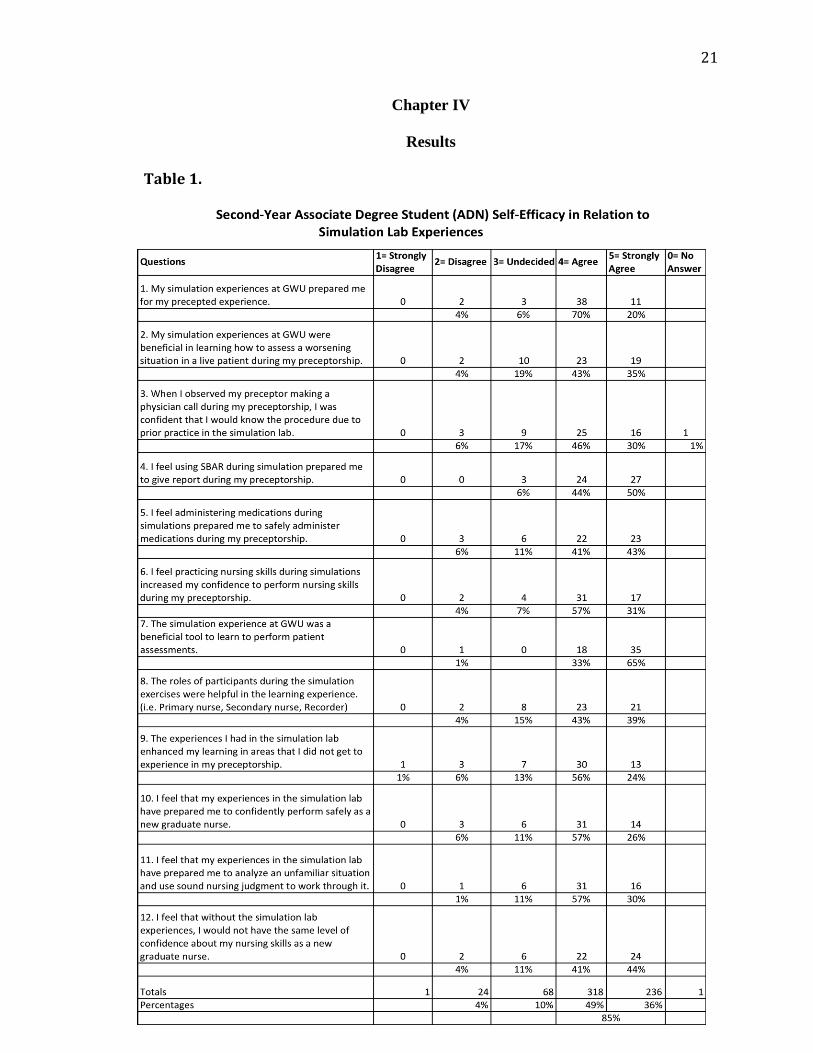
Table 1.
22
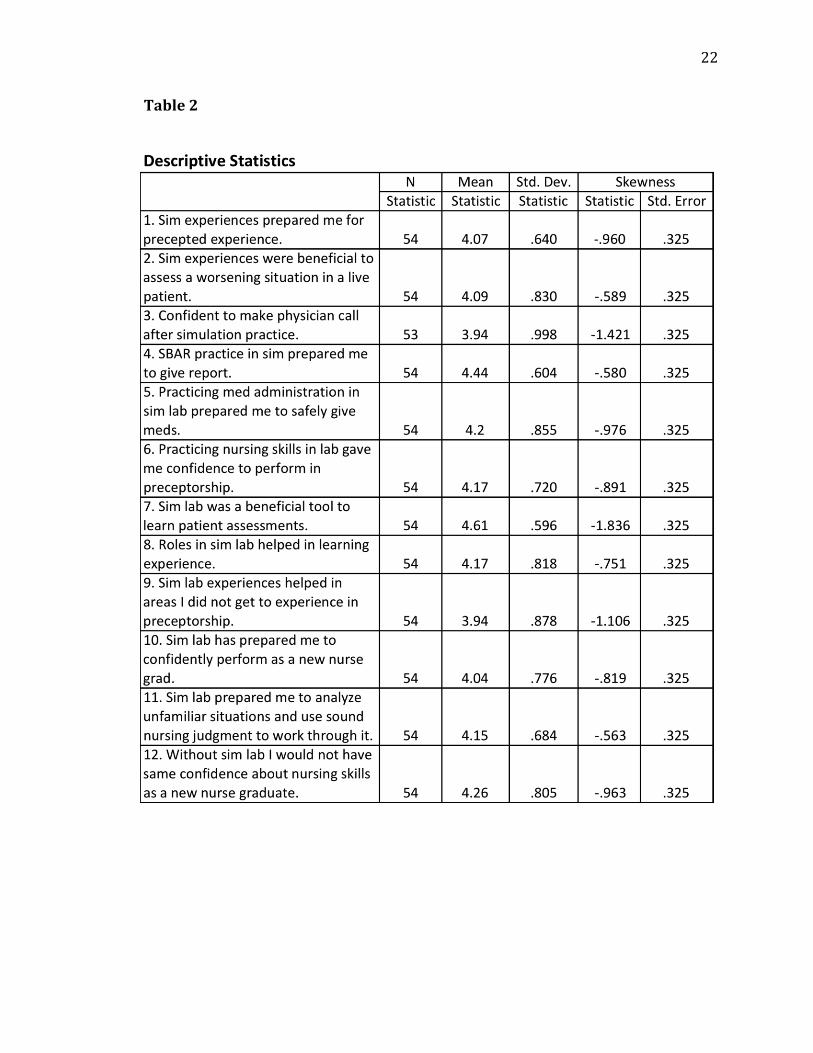
Table 2
23
Statistical Presentation
Table 1 shows the breakdown of answers to the survey by question and by
response category. Each question has six possible answer categories when “no answer” is
added for calculation purposes. There was one question by one respondent with no
answer. There was only one response of strongly disagree to one question. Table 2 shows
the Mean, which is the hypothetical estimate of the “typical” score or the center of a
distribution of scores, the Standard Deviation, which is an estimate of the average
variability or spread of a set of data, and the Skewness, or measure of the symmetry of a
frequency distribution. Symmetrical distributions have a skew of 0. Negative skew shows
that frequent scores are clustered at the higher end of the distribution of scores (Field,
2009).
Preparation for precepted experience results. Ninety percent of respondents
answered with either agree or strongly agree, that their simulation experiences in this
nursing school prepared them for their precepted experience in a clinical location.
Questions 3, observing the preceptor make a physician call and feeling confident in
performing this skill due to simulation practice and Question 4, feeling confident giving
report during clinical due to practicing the Situation, Background, Assessment,
Recommendations (SBAR) method during simulation, were answered with seventy-six
and ninety-four percent respectively, agreeing or strongly agreeing with the question.
Task oriented questions 5, concerning administering medications, 6, involving
performing nursing skills, and 7, performing patient assessments, showed agree and
strongly agree percentages of eighty-four percent, eighty-eight percent and ninety-eight
percent respectively.
24
Roles and critical thinking results. A majority of respondents (82%) felt that the
roles used during simulation exercises such as Primary Nurse, Secondary Nurse and
Recorder were beneficial. Seventy-eight percent answered with agree or strongly agree
that simulation was beneficial in learning how to assess a worsening situation in a live
patient. Eighty-seven percent responded with agree or strongly agree that simulation
experiences prepared them to analyze an unfamiliar situation and use sound nursing
judgment to work through it.
New nurse graduate responses. Eighty-three percent of respondents answered
agree or strongly agree that simulation prepared them to confidently perform safely as a
new nurse graduate. Eighty-four percent responded with agree or strongly agree that
without the simulation lab experiences, they would not have the same level of confidence
about nursing skills as a new nurse graduate.
The findings of Second-Year Associate Degree Student (ADN) Self-Efficacy in
Relation to Simulation Lab Experiences overwhelmingly supported positive perceptions
and experiences of simulation lab with a combined 85% of student respondents
answering that they agreed or strongly agreed with the positive statements in the survey.
Questions 3-7 were task oriented and showed the highest percentage of positive answers
(88%), and the highest combined average mean (4.27). This indicated a strong perception
by the students that simulation is beneficial for task-oriented practice, as found in the
literature (Jeffries, 2007). Among those tasks, Question 3 had the lowest agreement
(76%), concerning observing a preceptor making a call to the physician and feeling
comfortable with it due to simulation practice. This skill practice may warrant further
evaluation since communication with physicians can be intimidating as a new nurse.
25
In another form of communication within the task questions, simulation practice
for the SBAR tool appeared to be beneficial for the students. With a mean of 4.44 and
percentage of positive answers being 94%, this indicated the distribution of scores was on
the higher end of the scale with increased agreement to the question. The majority of
students felt that practicing using the SBAR in simulation lab prepared them to give
report during their preceptorship. The highest scoring task-oriented question was number
seven. This question involved using simulation to learn to perform patient assessments.
Ninety-eight percent of respondents answered positively, (mean=4.61), indicating near
group consensus that simulation was beneficial in learning patient assessments.
The general question 9 indicated that several students were unsure or disagreed
that simulation experiences enhanced learning in areas they did not get to experience in
their preceptorship. Twenty percent (mean=3.94) disagreed or were unsure of whether
they agreed with the statement. Further development of scenarios where students can
experience rare or unusual situations that might not occur during clinical could be added
to the simulation lab. Eighty-two percent felt that roles of the participants in simulation
scenarios (Primary Nurse, Secondary Nurse, Recorder) were helpful in the learning
experience. Of the two critical thinking questions, number 2 and 11, one indicated a high
agreement level with 87% agreeing that their experiences in the simulation lab had
prepared them to analyze an unfamiliar situation and use sound nursing judgment to work
through it. In the other question 78% agreed that their simulation experience was
beneficial in learning how to assess a worsening situation in a live patient during the
preceptorship. Scenarios for simulation can be developed to lead students through

26
changing situations with patients; however, every possible worsening health situation
cannot be prepared for.
The two new graduate nurse questions, 10 and 12 were answered with 83% and
84% positive agreement respectively. A majority of these student nurses agreed that their
experiences in simulation lab prepared them to confidently perform safely as a new
graduate nurse and that without the simulation lab, they would not have the same level of
confidence about their nursing skills. This, along with the 90% agreement of simulation
lab experiences preparing the student for their precepted experience indicates that a
majority of this ADN class experienced an increase in self-efficacy due to experiences in
the simulation lab.
The students were able to write comments at the end of the survey and 13
respondents commented on improvements for simulation, what they did not like about
simulation, and what they approved of. These comments are found in their entirety in
Appendix C. Common constructive criticism themes in the comments included feeling
stressed and judged during simulation with no opportunity to discuss what is going on or
ask questions, simulation not being realistic enough, lack of equipment and need to
pretend, the need to discuss pre-lab assignments for full understanding, not knowing by a
grade exactly what part of the simulation was not acceptable, not enough time for repeat
simulations, only using for check off of a skill. Common positive comments included the
experience that simulation lab allowed students to explore situations unlikely to happen
in preceptorship, and assessment skills improved greatly.
27
Chapter V
Discussion
Interpretation of Findings
This group of students overall felt that simulation was a beneficial tool to learn
skills that are needed in the clinical arena. One area of dissimilar agreement was between
questions 2 and 11, which were very similar in content but received unequal amounts of
agreement. Eighty-seven percent agreed that simulation prepared them to analyze an
unfamiliar situation and use sound nursing judgment to work through it, where as 78%
agreed that their simulation experience was beneficial in learning how to assess a
worsening situation in a live patient. An unfamiliar situation and a worsening situation
would have similarities, although student nurses with limited experiences may not have
compared them as such.
According to Bandura’s theory of self-efficacy, mastery experiences are the most
important tool to increase confidence, along with watching someone else with whom the
student identifies (Bandura, 1994). Simulation offers both types of experiences depending
on whether the student performs as the Primary Nurse, Secondary Nurse or Recorder in
the simulation exercise. As the Primary Nurse, the student has the opportunity to actually
perform the skill, which leads to the mastery of the skill if enough practice is allowed.
Mistakes can be learned from without harming a live patient. Others in the assigned
group can learn both from skills performed well and mistakes made during observation.
Due to these experiences, students can be better prepared and therefore more confident in
their actions and decisions as they grow in knowledge.
28
Implications for Nursing
Even though the majority of participants in this class of second-year ADN
students felt that simulation experiences increased their confidence, there were some
valid points in the comments that should be used for further development of this
simulation lab and the experiences provided. Nursing education can benefit from this
technology, to provide students with the practice needed to build a sense of self-efficacy.
Confident nurses are more prepared to weather the constant changes in the healthcare
field, experience less stress, less transitional shock in moving from a student situation to a
work situation (Duchscher, 2008). Simulation has an important role in the education of
nurses and in raising the skill level and confidence level of students in preparation for the
role of nurses in the workforce.
Implications for Further Research
Second-Year Associate Degree Student (ADN) Self-Efficacy in Relation to
Simulation Lab Experiences supported the question of students gaining self-confidence or
self-efficacy from their simulation experiences. There were limitations involving the
sample size (54), although 54 out of 57 students was a high percentage for a return rate of
a survey (95%). These students completed the survey immediately after completing final
exams, before leaving the room. The fatigue factor did not appear to have a negative
impact in the results. A larger sample size including multiple year students might create
more opportunity to gather insights concerning simulation scenarios or methods that
could best work to increase self-efficacy. This study was limited to one site and one
group of participants at one point in time. The fidelity level of the simulations, including
the realism involved was not measured. There were no demographics of the students
29
recorded for comparison between male and female, age groups, level of prior
involvement with technology or learning styles. Further study should include a
comparison between the use of low fidelity and high fidelity in relation to students’
perceptions of what is learned. A focus on standardization of the best means to conduct
simulations for the most productive outcomes for students would benefit all nursing
programs.
Conclusion
This study of second-year ADN students’ perceptions of simulation experiences
was similar to what was found in other studies. Realism of the simulation is important for
some students to be able to transfer that knowledge to a live situation. Several students
commented on pretending, expressing a desire for complete and plentiful equipment
instead of acting as if the equipment is present. Simulation is useful for increasing
confidence in skill performance and can be made an even better experience with more
opportunities to practice in a non-judgmental atmosphere.
30
References
Anthony, M., Carter, J., Freundl, M., Nelson, V., & Wadlington, L. (2012). Using
simulation to teach veteran-centered care. Clinical Simulation in Nursing. 8(4),
e145-e150. doi:10.1016/j.ecns.2010.10.004
Bambini, D., Washburn, J., & Perkins, R. (2009). Outcomes of clinical simulation for
novice nursing students: communication, confidence, clinical judgment. Nursing
Education Perspectives, 30(2), 79-82.
Bandura, A. (2004). Health promotion by social cognitive means. Health Education &
Behavior, 31(2), 143- 164.
Bandura, A. (1994). Self-efficacy. In V. S. Ramachaudran (Ed.), Encyclopedia of Human
Behavior (Vol. 4, pp. 71-81). New York: Academic Press. (Reprinted in H.
Friedman [Ed.], Encyclopedia of Mental Health. San Diego: Academic Press,
1998). http://www.des.emory.edu/mfp/BanEncy.html
Bearnson, C.S., & Wiker, K.M. (2005). Human patient simulators: A new face in
baccalaureate nursing at Brigham Young University. Journal of Nursing
Education, 44(9), 421-425.
Bremner, M., Aduddell, K., & Amason, J. (2008). Evidence-based practices related to the
human patient simulator and first-year baccalaureate nursing students’ anxiety.
Online Journal of Nursing Informatics, 12,1.
http://ehis.ebscohost.com.ezproxy.gardner-webb.edu
Duchscher J. B. (2008) Transition shock: the initial stage of role adaptation for newly
graduated Registered Nurses. Journal of Advanced Nursing.
doi: 10.1111/j.1365-2648.2008.04898.x
31
Feingold, C.E., Calaluce, M., & Kallen, M.A. (2004). Computerized patient model and
simulated clinical experiences: Evaluation with baccalaureate nursing students.
Journal of Nursing Education, 43(4), 156-163.
Field, A. (2009). Discovering statistics using SPSS. (3rd
ed.). London, England: Sage.
Fountain, R.A., & Alred D. (2009). Student satisfaction with high-fidelity simulation: Does
it correlate with learning styles? Nursing Education Perspectives. 30(2), 96-98. doi:
10.1043/1536-5026-030.002.0096
Fritscher, L. (March 2009). Social cognitive theory. Understanding the effects of social
cognitive theory on phobias. About.com.
http://phobias.about.com/od/causesanddevelopment/qt/socialcogtheory.htm
Gardner-Webb University. (2012). In online academic catalog.
http://gardner-webb.edu/academics/academic-programs/undergraduate-
programs/schools/school-of-nursing/programs/adn/index.html
Goldenbery, D., Andrusyszyn, M.A., & Iwasiw, C. (2005). The effect of classroom
simulation on nursing students’ self-efficacy related to health teaching. Journal of
Nursing Education, 44(7), 310-314.
Gore, T., Hunt, C., & Raines, K. (2008). Mock hospital unit simulation: A teaching
strategy to promote safe patient care. Clinical Simulation in Nursing. 4(3).
doi:10.1016/j.ecns.2008.08.006
Henneman, E.A., & Cunningham, H. (2005). Using clinical simulation to teach patient
safety in an acute/critical care nurse course. Nurse Educator, 30(4), 172-177.
Herm, S., Scott, K., & Copley, D. (2005). “Sim”sational revelations. Clinical Simulation
in Nursing. 3(1). doi: 10.1016/j.ecns.2009.05.036
32
Jeffries, P.R. (Ed.). (2007). Simulation in nursing education. New York, NY: National
League for Nursing.
Kameg, K., Howard, V. M., Clochesy, J., Mitchell, A. M., & Suresky, J. M. (2010). The
impact of high fidelity human simulation on self-efficacy of communication
skills. Issues In Mental Health Nursing, 31(5), 315-323.
doi:10.3109/01612840903420331
Lee, L.Y.K., Lee, J.K.L., Wong, K.F., Tsang, A.Y.K. & Li, M.K. (2010). The
establishment of an integrated skills training centre for undergraduate nursing
education. International Nursing Review. 57, 359-364.
Pajares, F. (2004). Albert Bandura: Biographical sketch.
http://des.emory.edu/mfp/bandurabio.html
Paskins, Z., & Peile, E. (2010). Final year medical students’ views on simulation-based
teaching: A comparison with the Best Evidence Medical Education Systematic
Review. Informa Healthcare. 32, 569-577.
Radhakrishnan, K., Roche, J.P., & Cunningham, H. (2007). Measuring clinical practice
parameters with human simulation: A pilot study. International Journal of
Nursing Education Scholarship, 4(1), 1-11.
Reinhardt, A.C., Mullins, I.L., De Blieck, C., & Schultz, P. (2012). IV insertion
simulation: Confidence, skill, and performance. Clinical Simulation in Nursing.
8(5), e157-e167. doi: 10.1016/j.ecns.2010.09.001
Smith, S. J., & Roehrs, C. J. (2009). High-fidelity simulation: Factors correlated with
nursing student satisfaction and self-confidence. Nursing Education Perspectives,
30(2), 74-78.
33
Trochin, W. M. K. (2006). Research Methods Knowledge Bassed.
www.socialresearchmethods.net/kb/scallik.php.
Wilt, K.E., & King, M. (2012). Time well spent: Integrating simulation into an
accelerated 1-year BSN program. Clinical Simulation in Nursing. 8(3), e103-
e107. doi: 10.1016/j.ecns.2010.10.002

34
Appendix A
Simulation Experience Questionnaire
35
Simulation Experience Questionnaire
By completing this questionnaire, you are agreeing to participate in this research study.
The final report will not include any personally identifiable information such as your
name. You are encouraged to ask any questions you may have. You are not obligated in
any way to take this survey, and your grade will not be compromised if you decline.
Please turn in the survey to your instructor before leaving, sealed in the provided
envelope. Thank you very much for taking the time to complete this survey.
Please answer the following questions based on your perceptions and experiences with
the use of simulation labs in your nursing curriculum.
Use the following scale to rate your answers. Please circle your response.
1 = strongly
disagree
2 = disagree 3 =undecided 4 = agree 5 = strongly
agree
36
Simulation Experience Questionnaire
Please circle your response.
1. My simulation experiences at GWU prepared me for my precepted
experience.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
2. My simulation experiences at GWU were beneficial in learning how to assess a
worsening situation in a live patient during my preceptorship.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
3. When I observed my preceptor making a physician call during my preceptorship, I
was confident that I would know the procedure due to prior practice in the simulation lab.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
4. I feel using SBAR during simulation prepared me to give report during my
preceptorship.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
37
5. I feel administering medications during simulations prepared me to safely administer
medications during my preceptorship.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
6. I feel practicing nursing skills during simulations increased my confidence to perform
nursing skills during my preceptorship.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
7. The simulation experience at GWU was a beneficial tool to learn to perform patient
assessments.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
8. The roles of participants during the simulation exercises were helpful in in the
learning experience. (i.e. Primary nurse, Secondary nurse, Recorder)
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
38
9. The experiences I had in the simulation lab enhanced my learning in areas that I did
not get to experience in my preceptorship.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
10. I feel that my experiences in the simulation lab have prepared me to confidently
perform safely as a new graduate nurse.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
11. I feel that my experiences in the simulation lab have prepared me to analyze an
unfamiliar situation and use sound nursing judgment to work through it.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
12. I feel that without the simulation lab experiences, I would not have the same level of
confidence about my nursing skills as a new graduate nurse.
1 = strongly
disagree
2 = disagree 3 = undecided 4 = agree 5 = strongly
agree
39
Thank you for completing this survey about your simulation lab experiences. Please add
any comments you feel appropriate concerning your simulation experiences
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________

40
Appendix B
Introduction to Survey
41
Simulation Experience
My name is Sarah Tate. I am working to complete my MSN at Gardner-Webb
University with a concentration in education. This survey is a vital part of my Thesis. My
contact email is [email protected], if you have any questions. I would greatly appreciate
your participation in this brief survey. It involves 12 questions about your experiences
with the simulation lab while attending GWU School of Nursing, and an area for further
comment if you so choose to add comments.
This survey is totally anonymous. I will not know your name. I only will know
that you are a second year ADN nursing student, getting ready to graduate and become a
new nurse. I wish you the best of luck in your career, and in passing the nursing board
exam.
Thank you for your participation. If you would like to know the results of this
survey, please use the consent page to list your email and I will send the results when my
thesis is complete. By detaching this sheet from the survey, I will not be able to identify
you in relation to your survey or even know if you completed the survey.
By completing this survey, you are agreeing to participate in this research study.

42
Appendix C
Simulation Experience Survey Consent
43
Simulation Experience Consent
This student survey will be used to collect information concerning how you feel
about your simulation experiences while in nursing school. You may decline to
participate in the survey if you wish. This survey information will be used in a research
study that will look at student self-efficacy in relation to simulation experiences.
No personally identifiable information will be used in the study. The results will
be given as anonymous group results. You are under no obligation to complete a survey.
The final report will not include any personally identifiable information such as your
name. You are not obligated in any way to take this survey, and your grade will not be
compromised if you decline.
If you choose to complete the survey, please turn in the completed survey in the
provided sealed envelope to the instructor. Thank you for your assistance in this study.
You may request information about the results of this study by writing your name,
address, and/or telephone number and email on this paper and the researcher will be in
contact with you after this study is complete.
I would like to know the results of this study:
Name: ________________________________________________________
Address: _______________________________________________________________
Telephone: ________________________________
Email: _____________________________________
Preference to be contacted:
Address Telephone Email

44
Appendix D
Comments from Students
45
Comments from students:
"I was always more stressed in lab than in clinical, so I learned infinitely more
through clinicals than labs. Because all of our simulations were graded and we
couldn't ask questions, I never felt I learned much through them."
"I like the idea of different roles but I often felt like one person did all the work. If
my group members didn't know how to do a head-to-toe assessment, I would be
penalized, yet if I had been Primary, I would have completed the entire
assessment. In general, I think the Primary has a lot of pressure on them in each
situation."
"I feel like my preceptorship was more beneficial to me than simulation. I believe
after I completed my preceptorship that I was more confident in lab simulation."
"The grading with simulation the last semester of nursing school should be the
same throughout all of the simulations. It would allow you to be more aware of
errors."
"I feel that simulation is vital to nursing school and should be an
assessment/learning tool. However, the environment should be a learning
environment not judgmental and stressful. How can I learn if every week is a test,
but I still don't know how to properly set up a PCA pump? I think that each week
should be a simulation that is conducted where questions can be asked and we are
taught new assessment and critical thinking skills. Then have quarterly "test"
simulations." This student answered undecided for questions about assessing a
worsening situation and administering medications due to feeling those topics
were not fully addressed.
46
"Lab simulations are not real life. They do not prepare you for your preceptorship.
I would much rather practice nursing skills and become proficient at those
instead of learning them one time and never using them again."
"Labs still don't seem realistic enough for me. A lot of the time we didn't have
certain meds or equipment that we needed and often ‘pretended' that we did. I
think that we still need more time and experience with skills. It's hard to
remember exactly how to do something when you only do it once for a check off
then never again. There are many skills I did not get to perform in clinical and I
think the professors assume that every student gets a chance to perform most
skills, not always true."
" I feel that the current simulations are not yet up to optimum learning experience.
Right now we learn through bad grades and after the fact. If it was more inductive
[sic] to instructor/student interactions before and during the simulations, I believe
we would learn better from our mistakes by correcting them when they happen
rather than just seeing a bad grade and not knowing exactly what we did wrong at
what point. Also, I think it would be better if the prelab was fully discussed before
the simulations so a better understanding of the situation would help drive our
knowledge on what to do."
"Simulation lab allowed students to experience many situations that we would not
have likely had the opportunity to see in clinical. Many simulations were needed
to become accustomed to the process. I feel like everyone's assessment skills
improved greatly! The lab can be quite nerve-wracking at times but is beneficial
to students."

47
"A little more PCA practice would be useful. But overall, simulation was a good
skill-practicing and confidence-building experience."
"I really liked how our teachers made us come at different times throughout the
semester so we could get to experience everything from the beginning to the end."
"I believe simulation could be very helpful if they were always fully stocked with
equipment and we never had to 'fake' a skill or giving a med."
"Labs still need work. Med room still has problems. Too much pretending. Need
to go over lab pre-work before lab or at least post answers so we know where we
went wrong."