Embed Size (px)
Citation preview
R.H.Swartz, University of Toronto.
Secondary Stroke Prevention
Acute stroke conference,
Sunnybrook EstatesJanuary 20, 2011
Rick Swartz HBSc, MD, PhD, FRCPC
Assistant Professor, Department of Medicine,
Divisions of Neurology and Obstetrical Medicine,
Director, University of Toronto Stroke Program
Sunnybrook Health Sciences Centre, University of Toronto
Disclosures
Salary support:
• Heart and Stroke Foundation Centre for Stroke Recovery
• CIHR/CSN “Focus on Stroke”
Advisory Boards:
None.
Speaker’s Honararia:
GTA stroke conference, Ontario Stroke Day.
Bristol-Myers Squibb Canada
Trials:
None.
No stock in pharmaceutical companies
R.H.Swartz, University of Toronto.
R.H.Swartz, University of Toronto.
• To review basic epidemiology of stroke and
rationale for stroke prevention efforts
• To review secondary prevention strategies and
outline an approach to the art & science of
secondary prevention
Objectives
Stroke is a “brain attack”
R.H.Swartz, University of Toronto
• sudden loss of specific brain functions from
damage to one part of the brain secondary to:
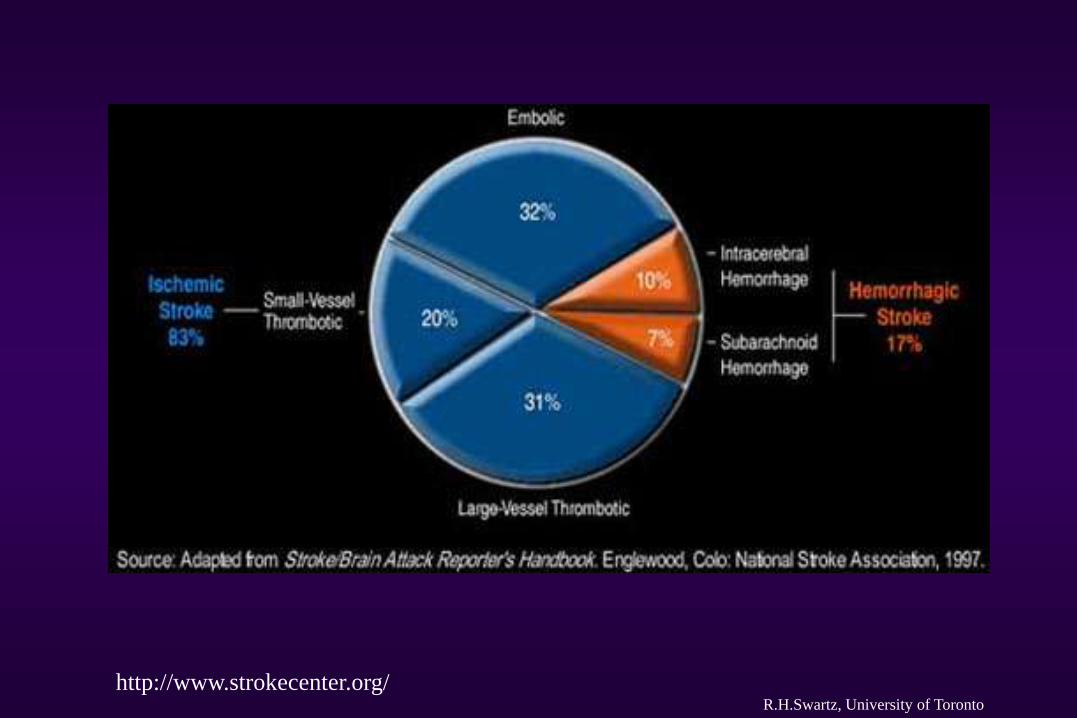
• an interruption of that region’s blood supply
(ischemic ~ 85%)
OR
• bleeding into that area of brain
(hemorrhagic ~15%)
R.H.Swartz, University of Toronto
http://www.strokecenter.org/
Basic epidemiology of stroke
R.H.Swartz, University of Toronto
• 1 stroke every 10 minutes in Canada
• #1 leading cause of adult disability in Canada
• 2nd leading cause of death worldwide
• Overall, ~20% fatal; 60-75% some disability
• ~50,000 Canadians annually have strokes
resulting in death or serious disability.
http://www.canadianstrokenetwork.ca/
World Stroke Day Proclamation, Stroke 2008;39
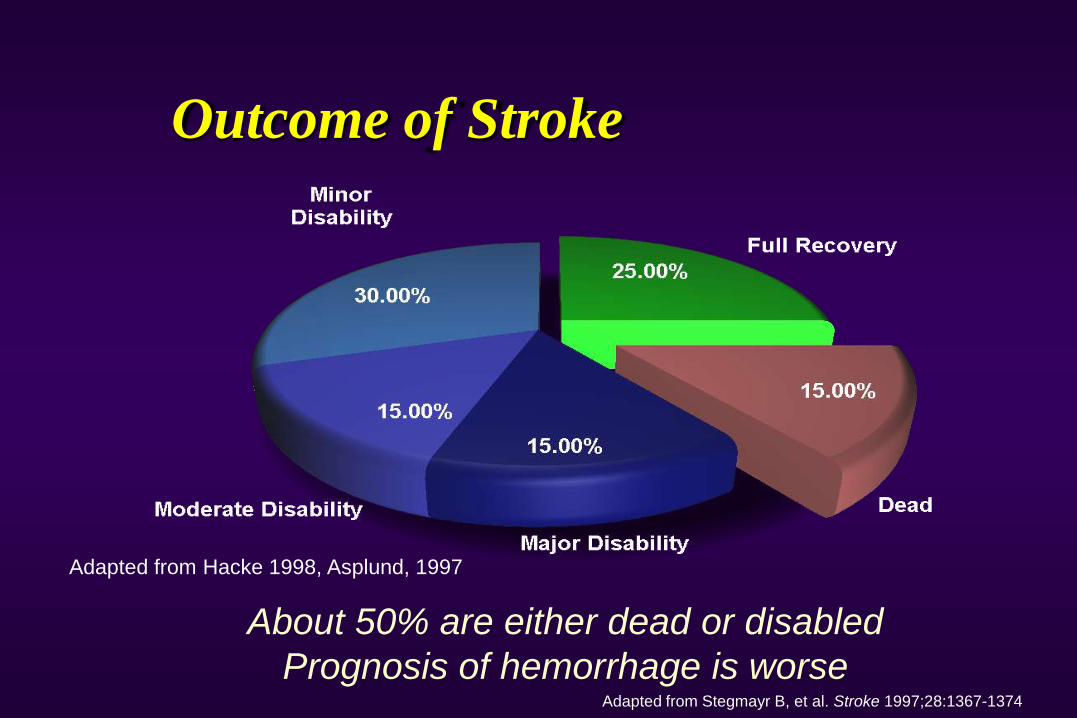
Outcome of Stroke
Adapted from Stegmayr B, et al. Stroke 1997;28:1367-1374
About 50% are either dead or disabled
Prognosis of hemorrhage is worse
Adapted from Hacke 1998, Asplund, 1997
Stroke outcome in round numbers
• For every 10 stroke patients…
• 2 will die
• 2 will recover
• 6 will be left with disability
ICES data, 2001
Dr. David Gladstone, 2004
Basic epidemiology of stroke
R.H.Swartz, University of Toronto
• ~300,000 Canadian survivors live at risk for:• another stroke (20% in 2 years)
• post-stroke dementia & post-stroke depression.
• < 50% survivors return to work… lost income.
• 50% caregivers develop emotional illness
within 1 year (care for the caregivers).
• Estimated direct and indirect costs of stroke are
~$4 BILLION annually in Canada.http://www.canadianstrokenetwork.ca/
So…
R.H.Swartz, University of Toronto
• Strokes are common (and “silent” strokes = 3x symptomatic!)
• Strokes kill and disable people.
• Fortunately, some of this burden is also
preventable
• Stroke is common, serious and treatable…
we can make a difference
A brief interlude for motivation…
R.H.Swartz, University of Toronto
• We will “cure” more people by aggressively
managing risk factors than we will EVER cure
with tPA.

http://www.strokebestpractices.ca/
Primary Prevention of Stroke
R.H.Swartz, University of Toronto
• Primary prevention means treating us…
modifying risk factors before symptoms or
illnesses occur (individuals & populations)
• We treat far more people for primary prevention,
and the event you’re trying to prevent is rarer.
• Thus, treatments have to be VERY safe and
effective in populations.
Primary Prevention of Stroke (& heart disease)
R.H.Swartz, University of Toronto
• Blood pressure lowering
• Atrial fibrillation (CHADS2)
• Smoking cessation
• Diabetes treatment
• Cholesterol treatment
• Weight loss / abdominal obesity / exercise
• Low-risk drinking guidelines
http://www.preventstroke.ca Stroke. 2006;37:577-617
Secondary Stroke Prevention
R.H.Swartz, University of Toronto
• Treatment of those with prior stroke or TIA,
regardless of etiology
1) Why treat?
2) When to treat?
3) Who to treat?
4) What to treat?
• In people with TIAs discharged from ER:
• 12% are readmitted to hospital within 30 days
• 9 – 12% recurrent stroke or death within 30 days!• 9% for TIA with speech deficit
• 12% for TIA with motor deficit
• Also need to treat FAST…
Secondary Prevention 1) Why treat?
Gladstone et al. CMAJ 2004 R.H.Swartz, University of Toronto
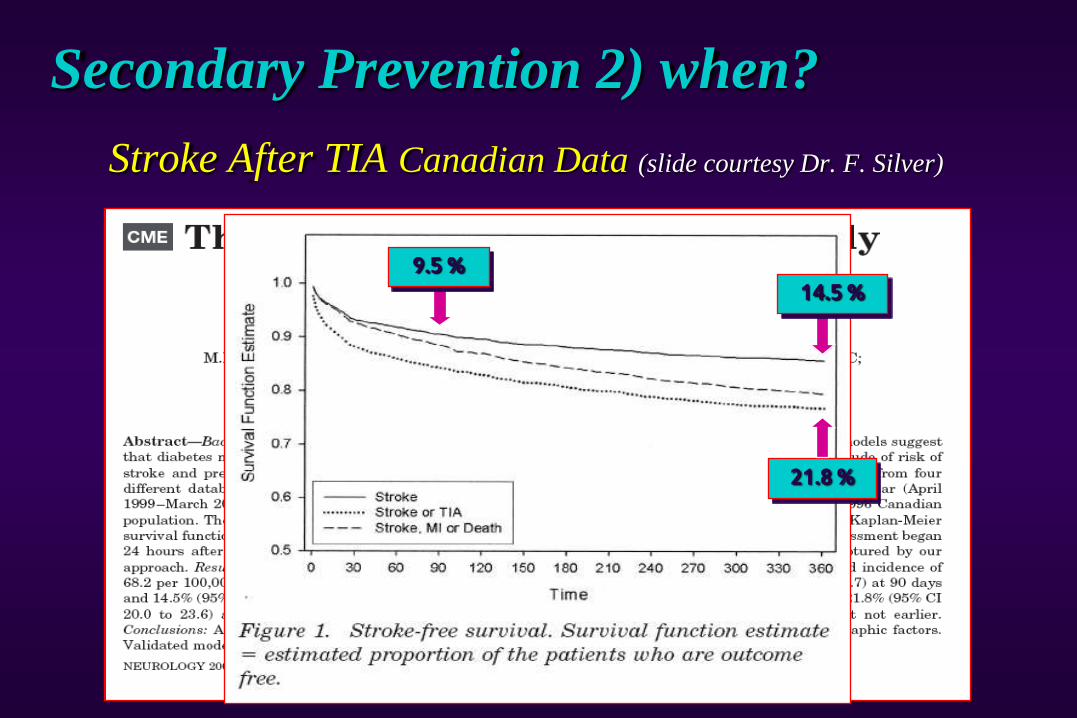
Stroke After TIA Canadian Data (slide courtesy Dr. F. Silver)
9.5 % 14.5 %
21.8 %
Secondary Prevention 2) when?
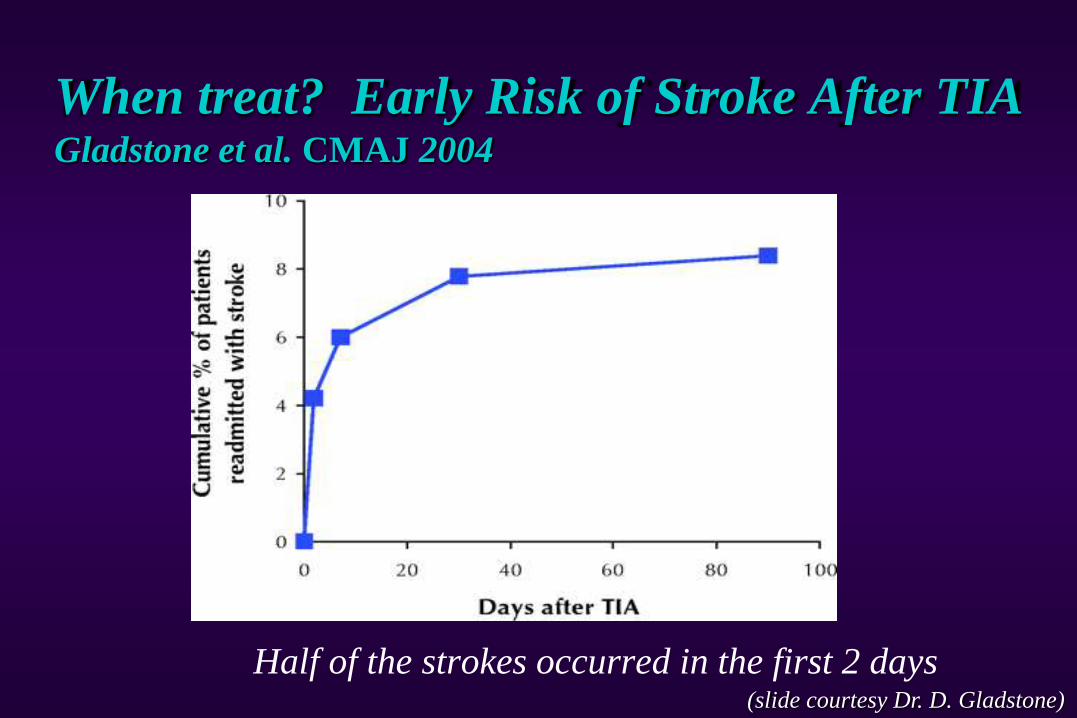
When treat? Early Risk of Stroke After TIAGladstone et al. CMAJ 2004
Half of the strokes occurred in the first 2 days(slide courtesy Dr. D. Gladstone)
pooled analysis from population and RCT’s (OXVASC, OCSP, UK-TIA and ECST).
Rothwell & Warlow, Neurology, 2005;64:817-20.
23% of patients with ischemic stroke have had a TIA
before their stroke
• 17% occur the day of the stroke,
• 9% the previous day,
• 43% had a TIA during the 7 days prior to the
stroke.
2) When to treat?
R.H.Swartz, University of Toronto
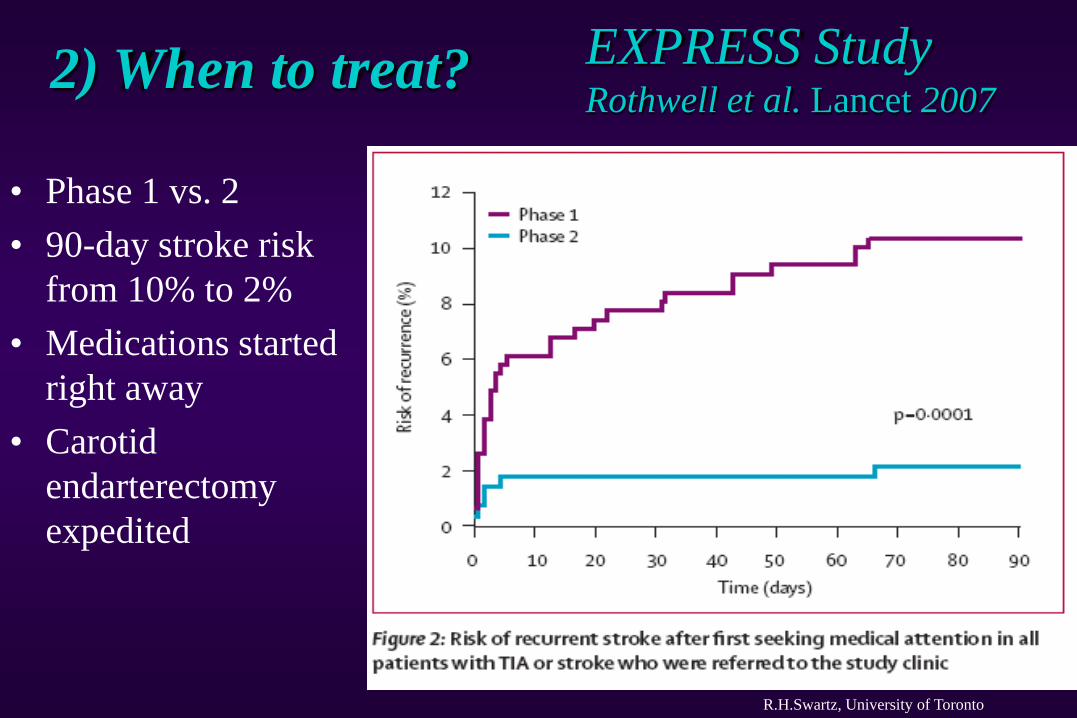
• Phase 1 vs. 2
• 90-day stroke risk
from 10% to 2%
• Medications started
right away
• Carotid
endarterectomy
expedited
EXPRESS StudyRothwell et al. Lancet 2007
2) When to treat?
R.H.Swartz, University of Toronto
FASTER Kennedy et al. Lancet Neurology 2007
• Fast Assessment of Stroke and TIA to prevent Early
Recurrence
• ASA +/- clopidogrel +/- simvastatin in 24 hours
• Stroke risk: 10.8% vs. 7.1% in favour of
ASA/clopidogrel combination (n.s.)
2) When to treat? Urgent assessments
prevent stroke
SOS-TIA Lavallee et al. Lancet Neurol 2007
• 24 hours TIA unit had lower event rates than
expected from ABCD2 score (1.24% vs. 5.96%)
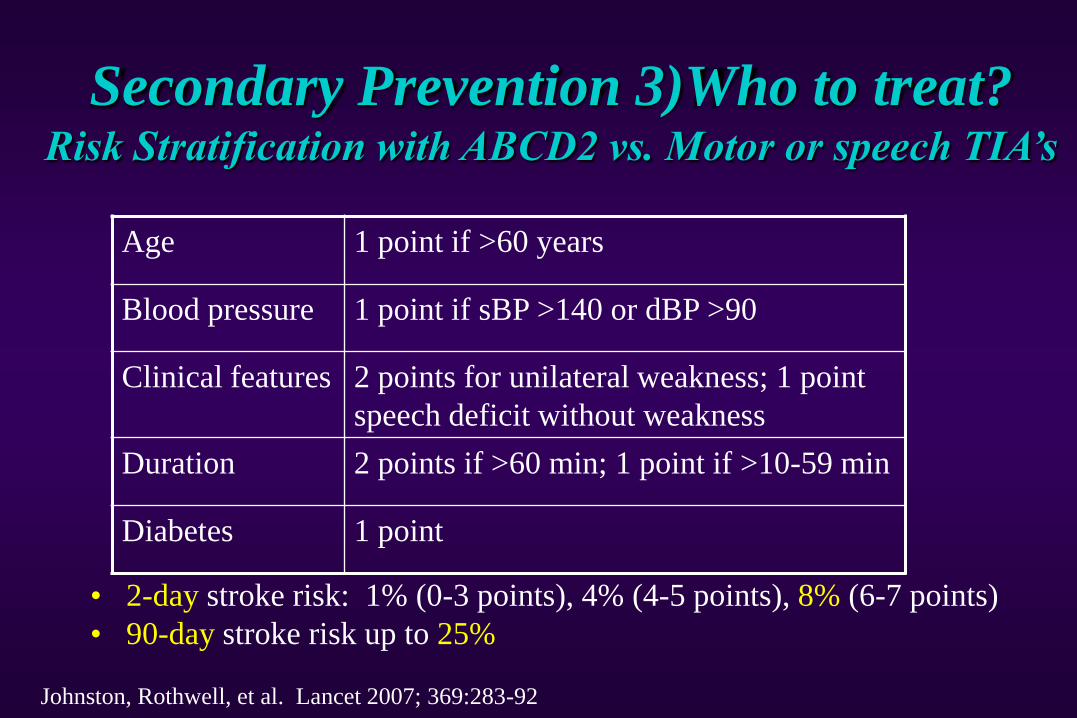
Age 1 point if >60 years
Blood pressure 1 point if sBP >140 or dBP >90
Clinical features 2 points for unilateral weakness; 1 point
speech deficit without weakness
Duration 2 points if >60 min; 1 point if >10-59 min
Diabetes 1 point
• 2-day stroke risk: 1% (0-3 points), 4% (4-5 points), 8% (6-7 points)
• 90-day stroke risk up to 25%
Secondary Prevention 3)Who to treat? Risk Stratification with ABCD2 vs. Motor or speech TIA’s
Johnston, Rothwell, et al. Lancet 2007; 369:283-92
• It isn’t always as simple as the “ABC’s”
• For example:
• 61 y.o. woman with mild HTN and diet controlled
DM, who had >2 hours of dizziness
• 58 y.o. man without diabetes or hypertension but had
a 15 minute episode of right face, arm and leg
weakness, with speaking gibberish and not
understanding speech.
Who to treat? The problem with ABCD’s
Gladstone et al. CMAJ 2004 R.H.Swartz, University of Toronto
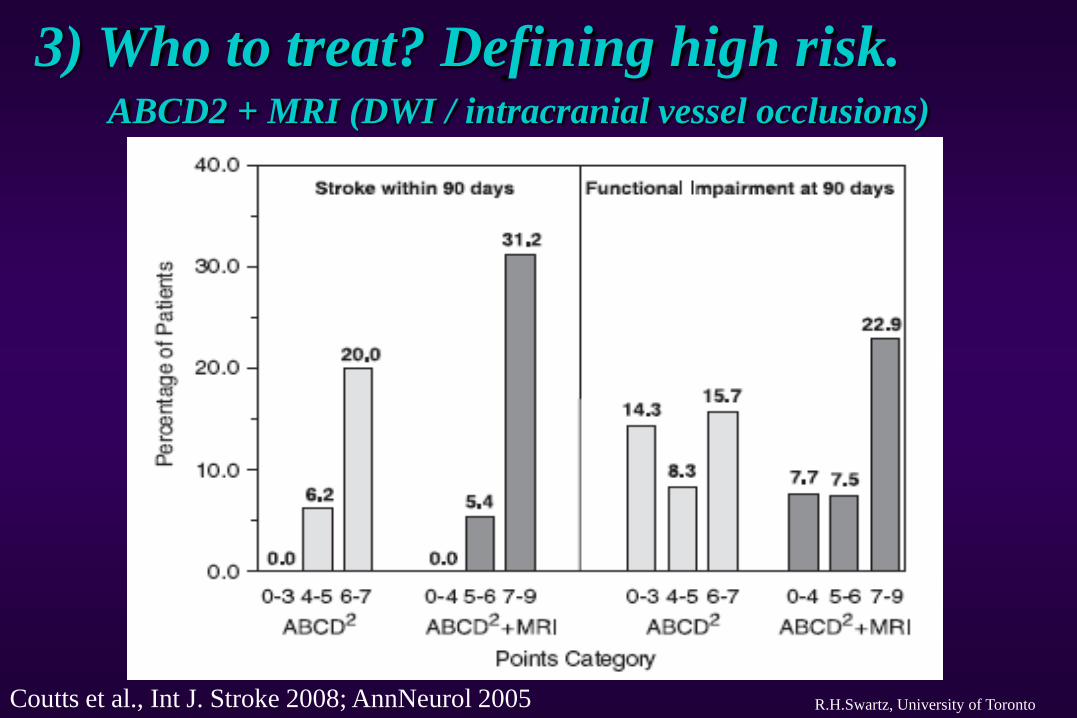
3) Who to treat? Defining high risk.
Coutts et al., Int J. Stroke 2008; AnnNeurol 2005
ABCD2 + MRI (DWI / intracranial vessel occlusions)
R.H.Swartz, University of Toronto
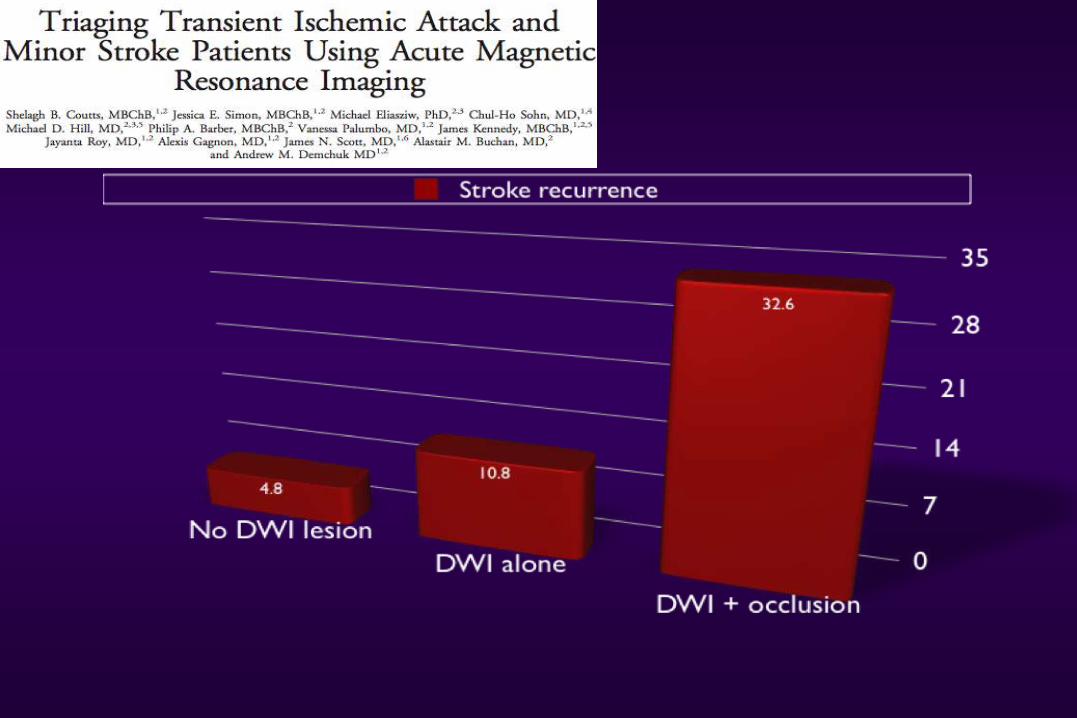
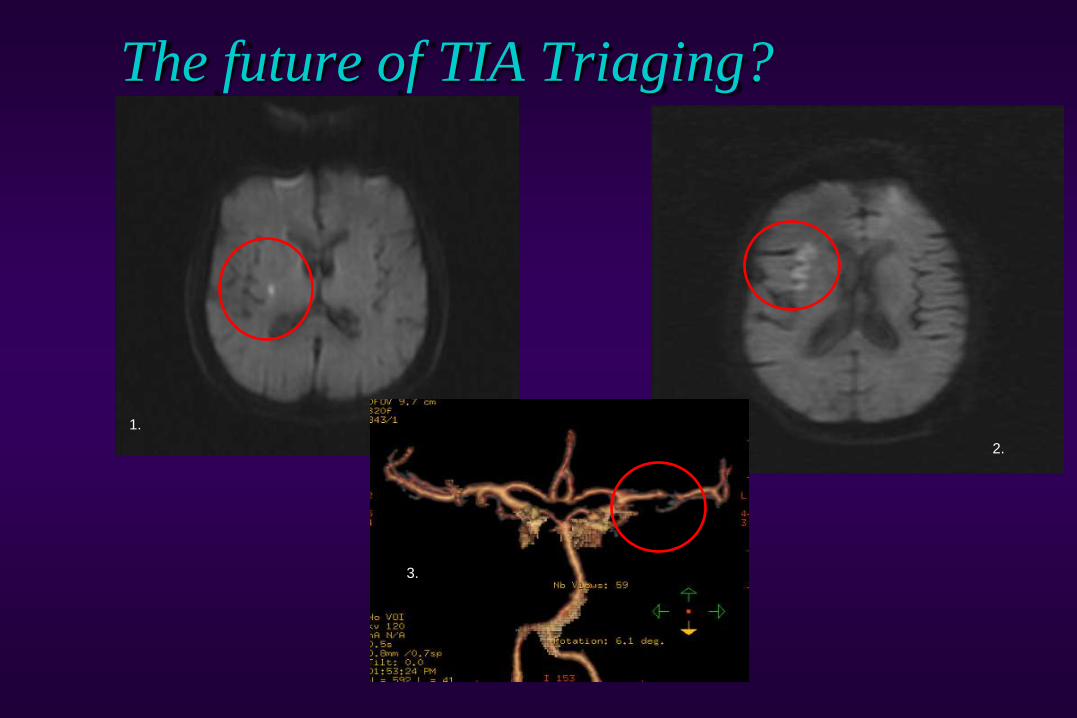
The future of TIA Triaging?
1.
2.
3.
1) Look at the intracranial vessels: atherosclerosis,
moya-moya, inflammatory diseases
2) Look at the neck: Carotid stenosis, dissections…
3) Look at the heart: Atrial fibrillation (+/- valve etc.)
4) Look at the blood: Platelet, APLA etc.
5) Look at the patient: risk factor modification
(hypertension, high cholesterol, diabetes, smoking,
drinking, diet/exercise, social situation)
Secondary Prevention 4) What to treat?
R.H.Swartz, University of Toronto
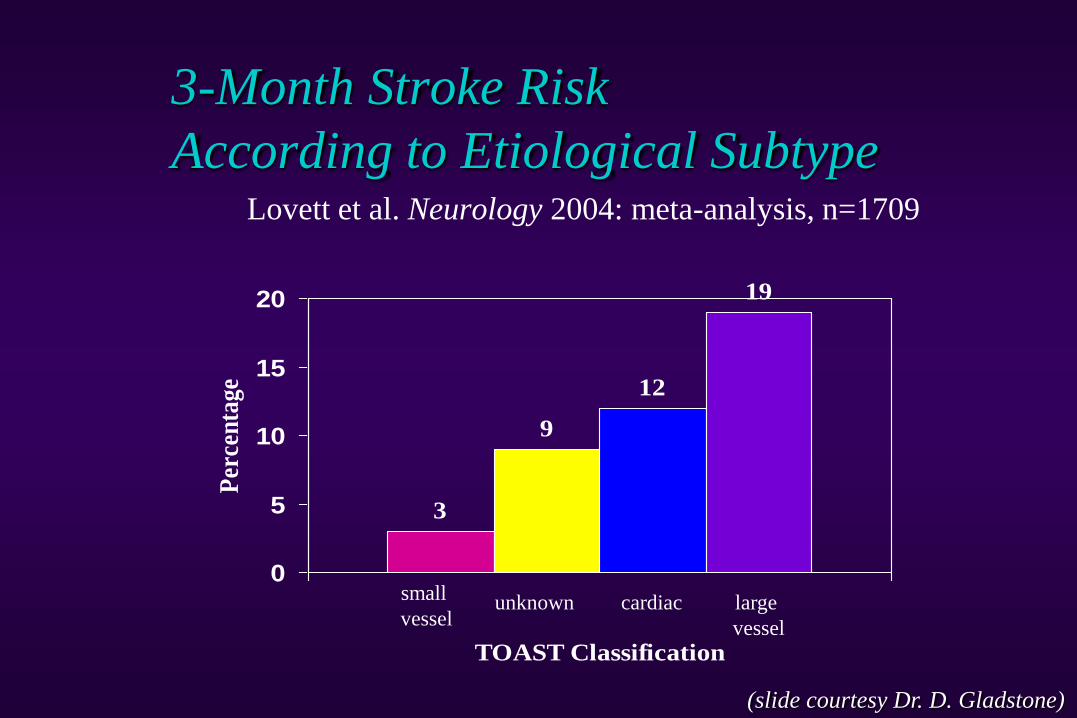
3-Month Stroke Risk
According to Etiological SubtypeLovett et al. Neurology 2004: meta-analysis, n=1709
3
9
12
19
0
5
10
15
20
TOAST Classification
Per
cen
tage
small
vesselunknown cardiac large
vessel
(slide courtesy Dr. D. Gladstone)
What to treat: A) Symptomatic Carotid Stenosis
• Severe stenosis (70-99%)
surgery highly beneficial (NNT=3*)
• Moderate stenosis (50-69%)
surgery beneficial (NNT=7*)
• Mild stenosis (<50%) – No surgery
(slide courtesy Dr. D. Gladstone)
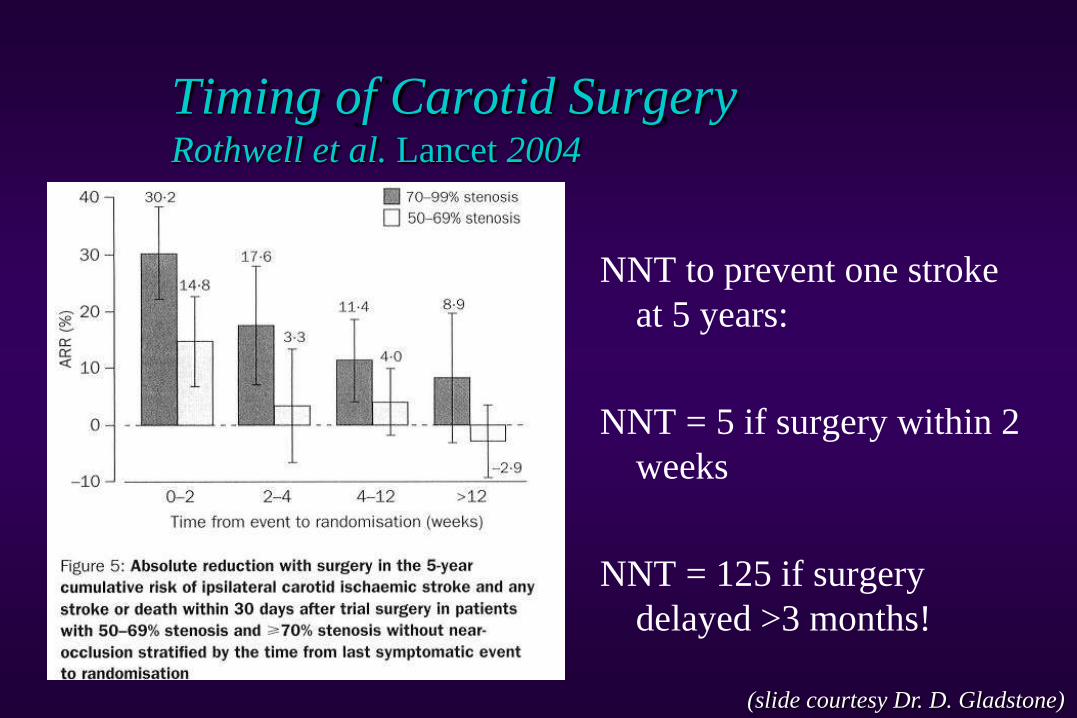
Timing of Carotid SurgeryRothwell et al. Lancet 2004
NNT to prevent one stroke
at 5 years:
NNT = 5 if surgery within 2
weeks
NNT = 125 if surgery
delayed >3 months!
(slide courtesy Dr. D. Gladstone)
Management of “Surgical” Carotid Disease
• 2008 Canadian Best Practice Recommendations
• TIA or non-disabling stroke and ipsilateral 70%–99% ICA
stenosis should be offered carotid endarterectomy within 2
weeks unless contraindicated
• Appropriate antiplatelet therapy depends on timing:
• Surgery in ≤ 24 hours: consider ASA
• Surgery in 1-2 weeks: consider combination ASA +
clopidogrel
• Ensure optimal management of vascular risk factors
* CMAJ 2008;179(12 Suppl):S1-S25.
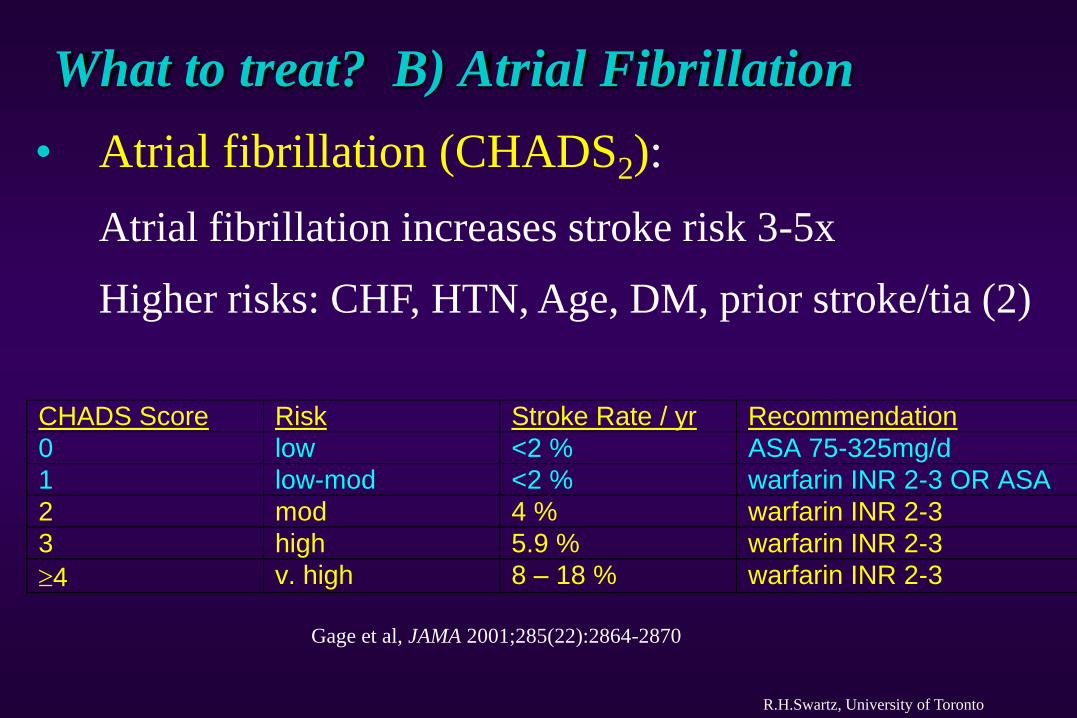
What to treat? B) Atrial Fibrillation
R.H.Swartz, University of Toronto
• Atrial fibrillation (CHADS2):
Atrial fibrillation increases stroke risk 3-5x
Higher risks: CHF, HTN, Age, DM, prior stroke/tia (2)
CHADS Score Risk Stroke Rate / yr Recommendation
0 low <2 % ASA 75-325mg/d
1 low-mod <2 % warfarin INR 2-3 OR ASA
2 mod 4 % warfarin INR 2-3
3 high 5.9 % warfarin INR 2-3
4 v. high 8 – 18 % warfarin INR 2-3
Gage et al, JAMA 2001;285(22):2864-2870
Stroke Prevention
R.H.Swartz, University of Toronto
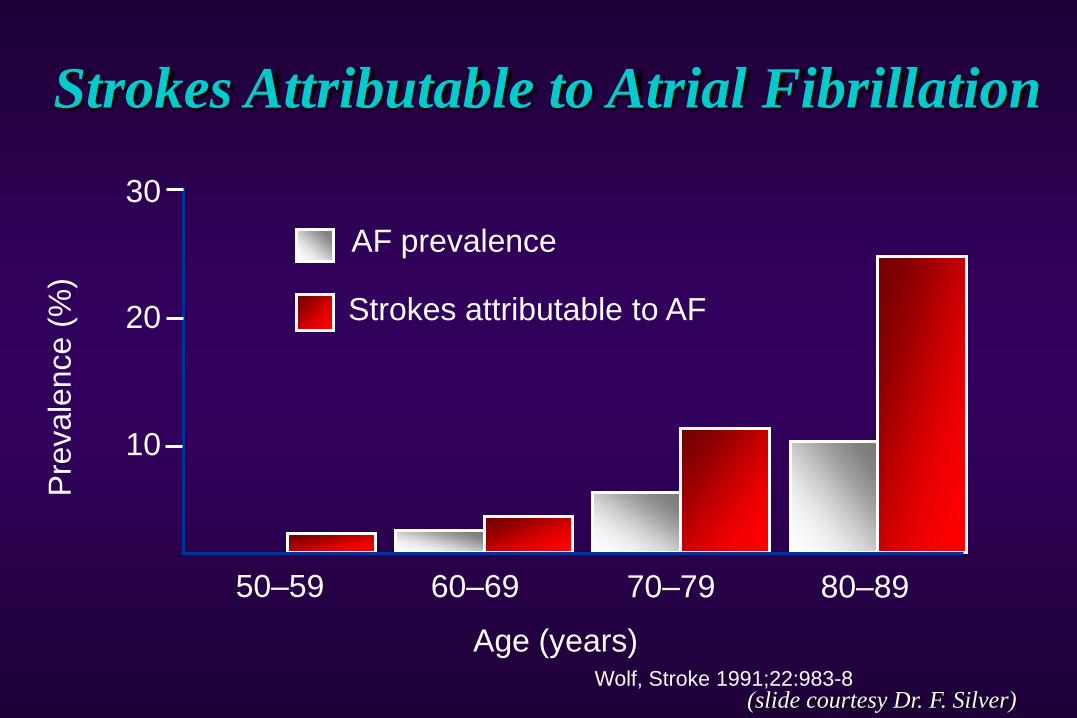
10
20
30
50–59 60–69 70–79 80–89
AF prevalence
Strokes attributable to AF
Age (years)
Pre
vale
nce (
%)
Wolf, Stroke 1991;22:983-8
Strokes Attributable to Atrial Fibrillation
(slide courtesy Dr. F. Silver)
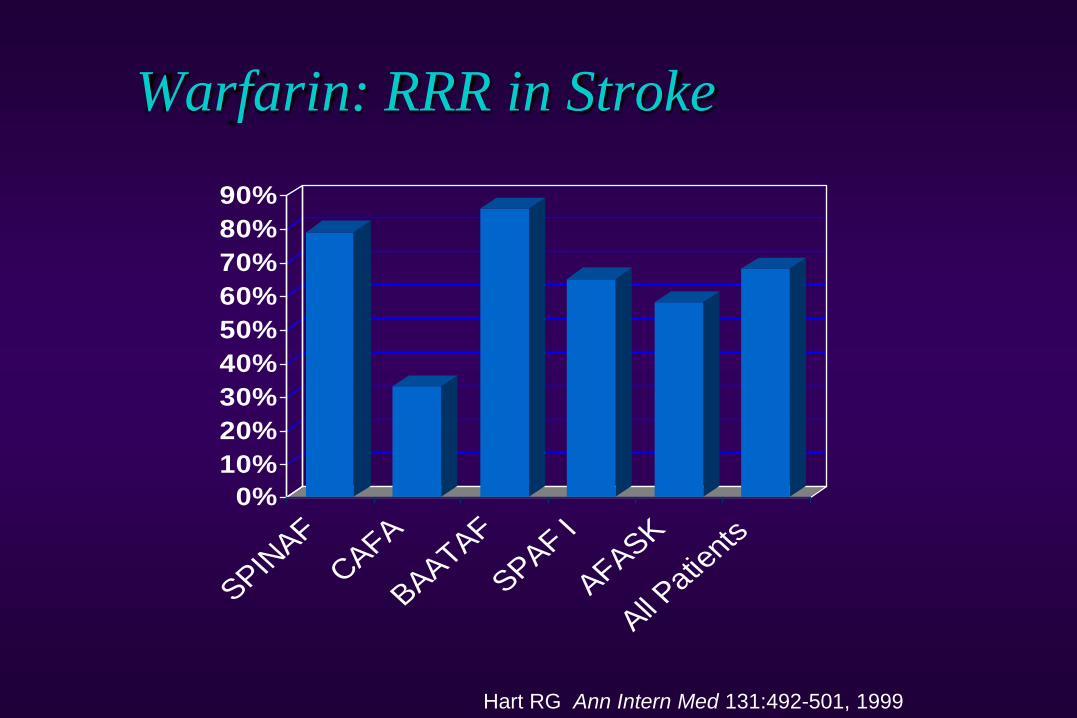
Warfarin: RRR in Stroke
Hart RG Ann Intern Med 131:492-501, 1999
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
SPINAF
CAFA
BAATAF
SPAF I
AFASK
All Patie
nts
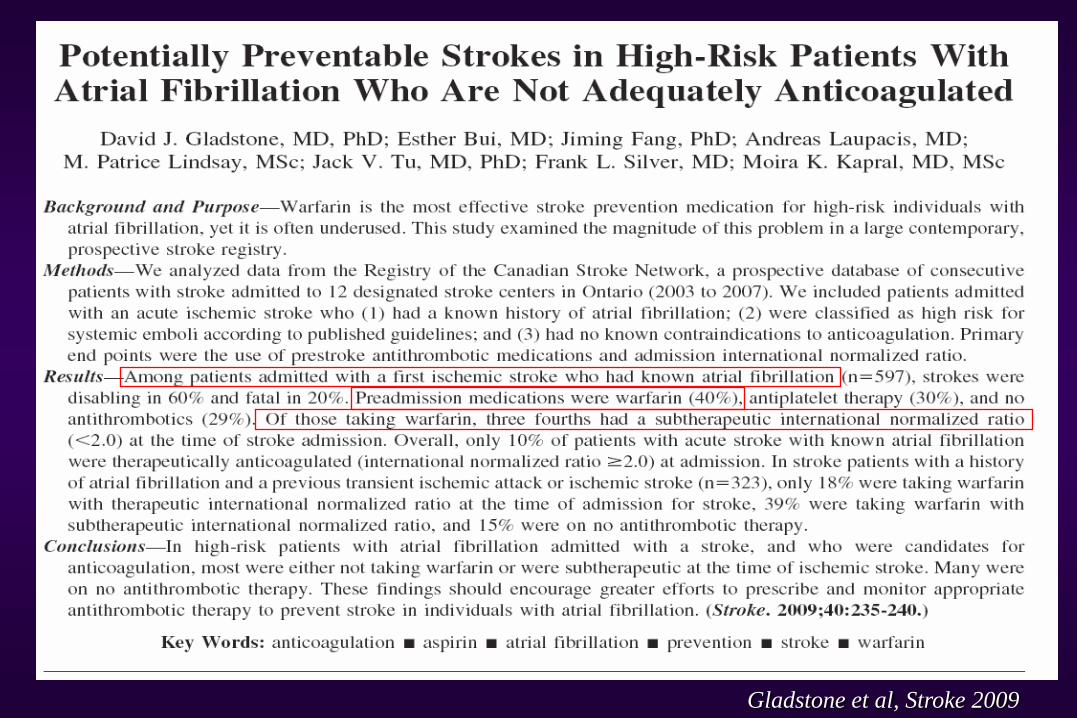
Gladstone et al, Stroke 2009
• Blood pressure: Common. >2/3 of adults >65
• The most important modifiable risk factor (2-5 x)• Ischemic, bleeding, “silent strokes”
• Contributes to:• Large-vessel atherosclerotic disease
• Small-vessel (lacunar) disease
• LV dysfunction and Afib
• Untreated HTN increases stroke risk 3-4 times. Treatment can
reduce stroke risk and fatalities ~40%.
• Most patients require 2 or more agents
• CHEP guidelines <140/90 (or if diabetes <130/80)
4) What to treat? C) Vascular risks
R.H.Swartz, University of Toronto
http://www.preventstroke.ca http://www.americanheart.org/presenter.jhtml?identifier=4704Stroke. 2006;37:577-617
• Diabetes: ~2x increased risk of stroke. Highly
correlated w/ HTN, high cholesterol, weight and
sedentary lifestyles. Target HbA1c <0.07. Treatment
reduces microvascular complications > macrovascular.
• Cholesterol: 2x increased risk of stroke. Risk for
CAD (which independently also increases stroke risk).
SPARCL (NNT = 50)
4) What to treat? C) Vascular risks
R.H.Swartz, University of Torontohttp://www.preventstroke.ca
http://www.americanheart.org/presenter.jhtml?identifier=4704
Stroke. 2006;37:577-617
R.H.Swartz, University of Toronto
• Smoking:
• 2 – 6 x risk (2x with second hand smoke only);
normalizes >5 yrs, independent of age
• one-time advice from physician results in 2% of
smokers quitting for >1 yr
• Weight loss, exercise, abdominal obesity: 2-6x
increased stroke risk with obesity. Treatments: low-
calorie, low-fat, low-sodium diet, 20-30 minutes of
moderate exercise most days
http://www.preventstroke.ca
4) What to treat? C) Vascular risks
R.H.Swartz, University of Toronto
• Anti-platelets (Aspirin (ASA), Clopidogrel (Plavix),
ASA/ER-dipyridimol (Aggrenox)):
• Low-dose ASA 1o prevention in people at risk
• increases GI bleed & hemorrhagic stroke risk.
• 75–160 mg daily as effective as higher doses.
http://www.americanheart.org/presenter.jhtml?identifier=4704
Stroke. 2006;37:577-617
4) What to treat? C) Vascular risks
R.H.Swartz, University of Toronto
• Deciding between anti-platelets?!
• CAPRIE (ASA vs. Plavix), CURE (Plavix/ASA vs
placebo/ASA post-ACS), ESPS2 and ESPRIT (ASA
plus ER dipyridamole vs. ASA)
• MATCH (Plavix vs. ASA/plavix): bleeding higher w/
combined ASA/Plavix (risk increases with long-term
use)
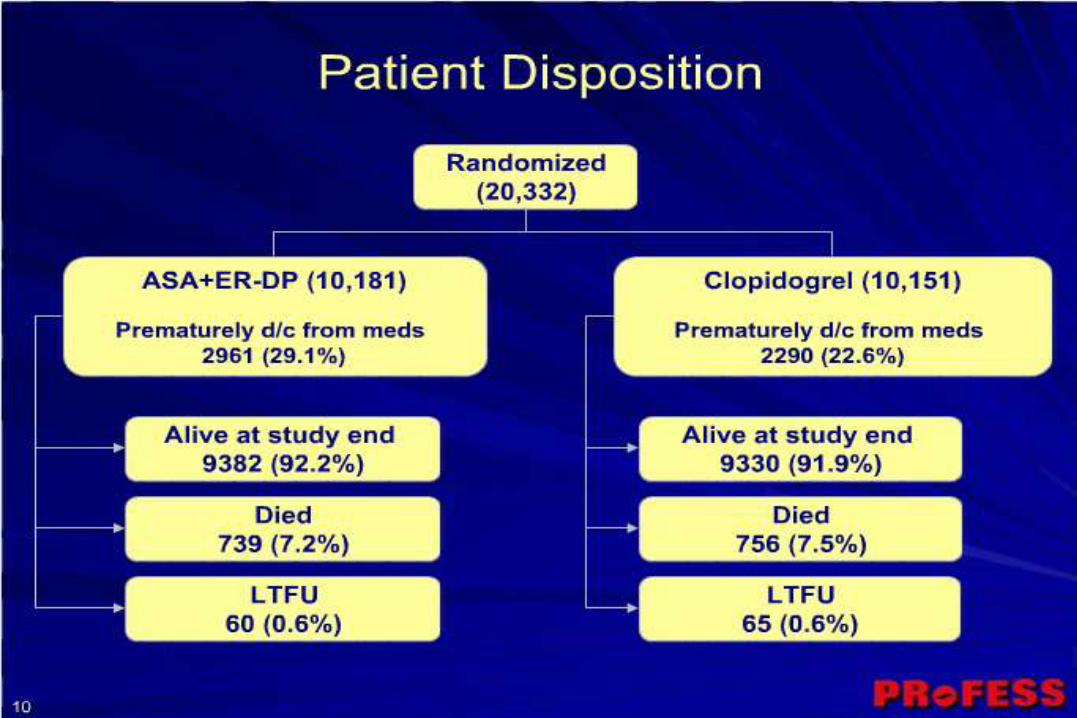
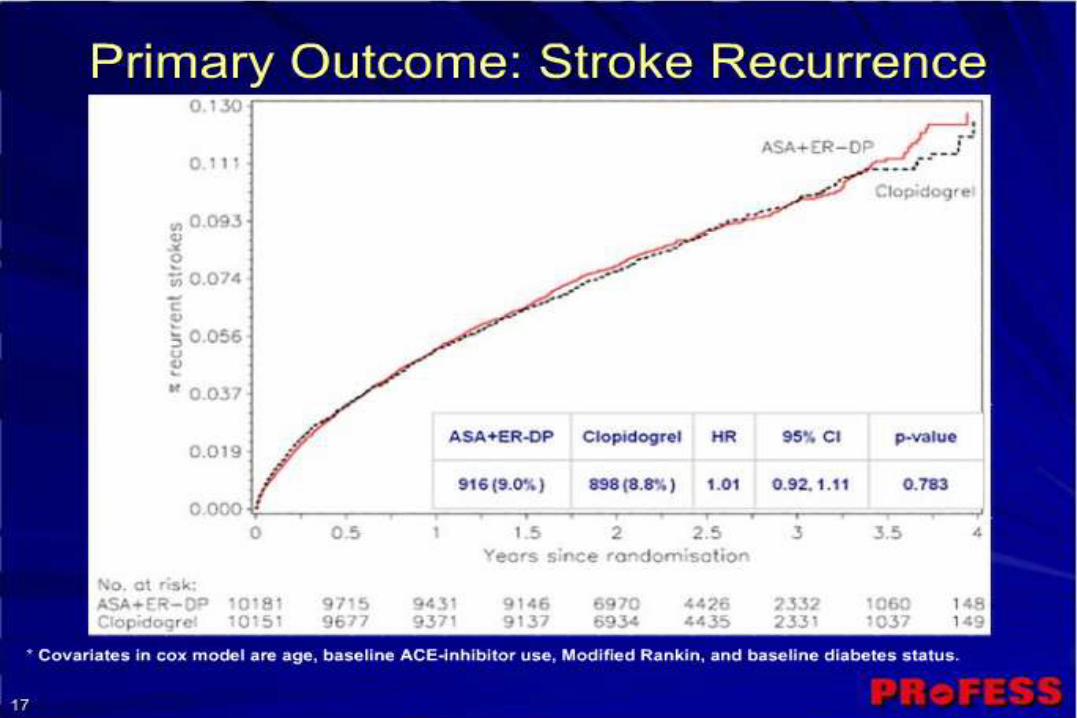
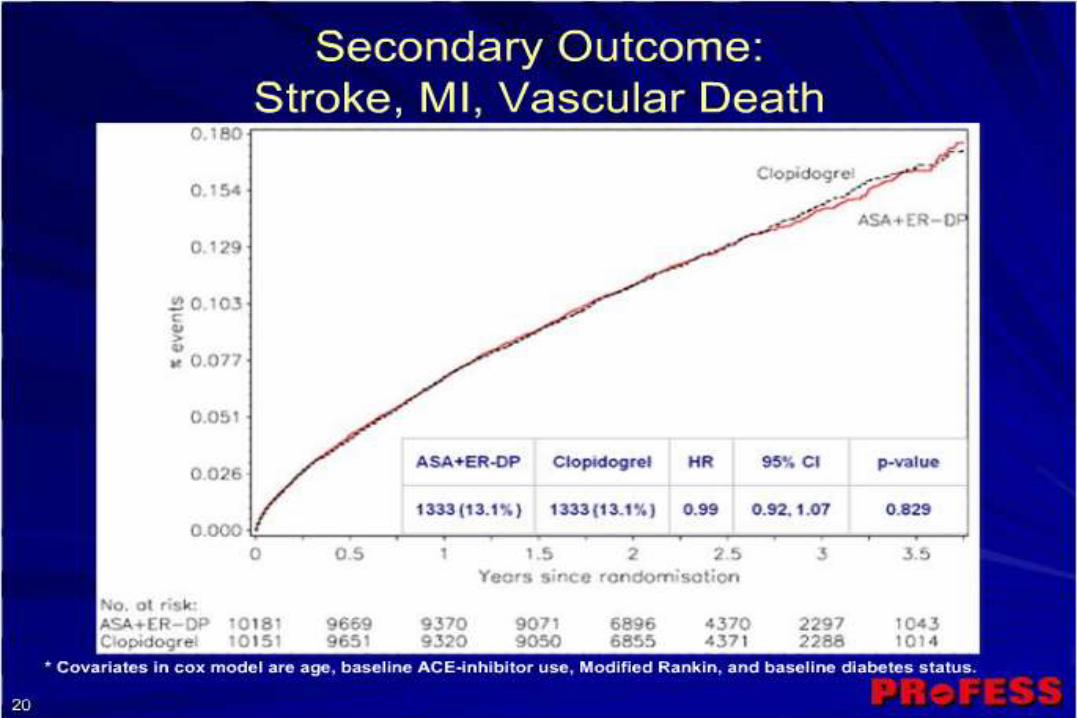
• PROFESS: no decisions between Plavix and Aggrenox
http://www.americanheart.org/presenter.jhtml?identifier=4704
Stroke. 2006;37:577-617
4) What to treat? C) Vascular risks
Stroke Prevention
R.H.Swartz, University of Toronto
• Smoking cessation:
• 2 – 6 x increased risk (2x with second hand smoke);
normalizes 5 yrs after quitting, independent of age
• one-time advice from physician results in 2% of
smokers quitting for >1 yr
• Weight loss, exercise, abdominal obesity: 2-6x
increased stroke risk with obesity. Treatments: low-
calorie, low-fat, low-sodium diet, 20-30 minutes of
moderate exercise most days
http://www.preventstroke.ca
Stroke Prevention
R.H.Swartz, University of Toronto
• We will “cure” more people by aggressively
managing risk factors than we will EVER cure
with tPA.
1) Look at the intracranial vessels: atherosclerosis,
moya-moya, inflammatory diseases
2) Look at the neck: Carotid stenosis, dissections…
3) Look at the heart: Atrial fibrillation (+/- valve etc.)
4) Look at the blood: Platelet, APLA etc.
5) Look at the patient: risk factor modification
(hypertension, high cholesterol, diabetes, smoking,
drinking, diet/exercise, social situation)
Secondary Prevention: What to treat?
R.H.Swartz, University of Toronto
Summary: Stroke Prevention
• Strokes are common and serious
• We can identify high risk patients
• We have effective stroke prevention therapies
• But…current management is often suboptimal
• Primary prevention: do the things we should do anyway
• Secondary prevention:
• Look at the brain vessels, neck, heart, blood and patient
• Treat TIA’s early and aggressively
• Expedite surgery for symptomatic carotid artery disease
• Anticoagulate patients with atrial fibrillation
• Anti-platelets and other risk reduction for everyone else!