Embed Size (px)
Citation preview
Section 2 Tissue and
Cellular Damage
1. Degenerations
Definition: When cellular injury is sublethal and sustained, cells and tissues tend to accumulate substances in abnormal quantities. These materials may be endogenous or exogenous.
Location: Intracellular and/or Extracellular
Nature: Normal substances:Normal substances: increase Exogenous materials:Exogenous materials: appearance
(1) Intracellular edema (cloudy swelling)
Definition: Accumulation of watery fluid in cells.
Morphologic change: Gross features:Gross features: cloudy swelling
Light microscopic features( LM):Light microscopic features( LM): Parenchymal cells swollen.
Early stages:Early stages: granularity degeneration——a fine granularity like ground-glass in the cytoplasm.
Later stages:Later stages: hydropic degeneration——clear vacuoles in the cytoplasm Progressive dilatation of the swollen cell
E.M. features:E.M. features: watery fluid in the dilated mitochondria and endoplasmic reticulum.
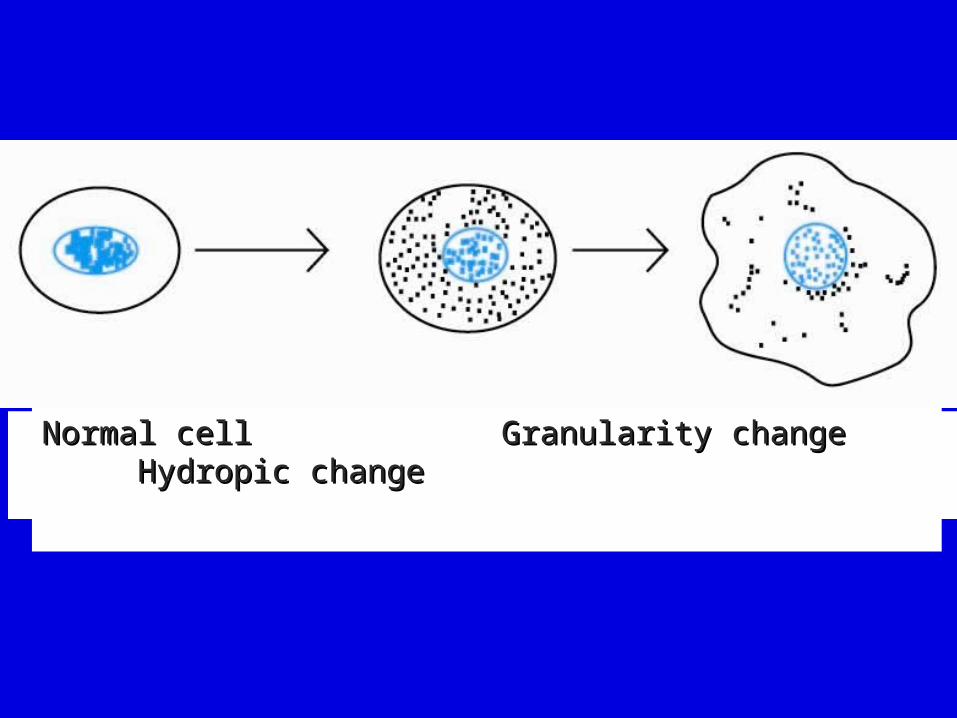
Normal cell Granularity change Hydropic Normal cell Granularity change Hydropic changechange
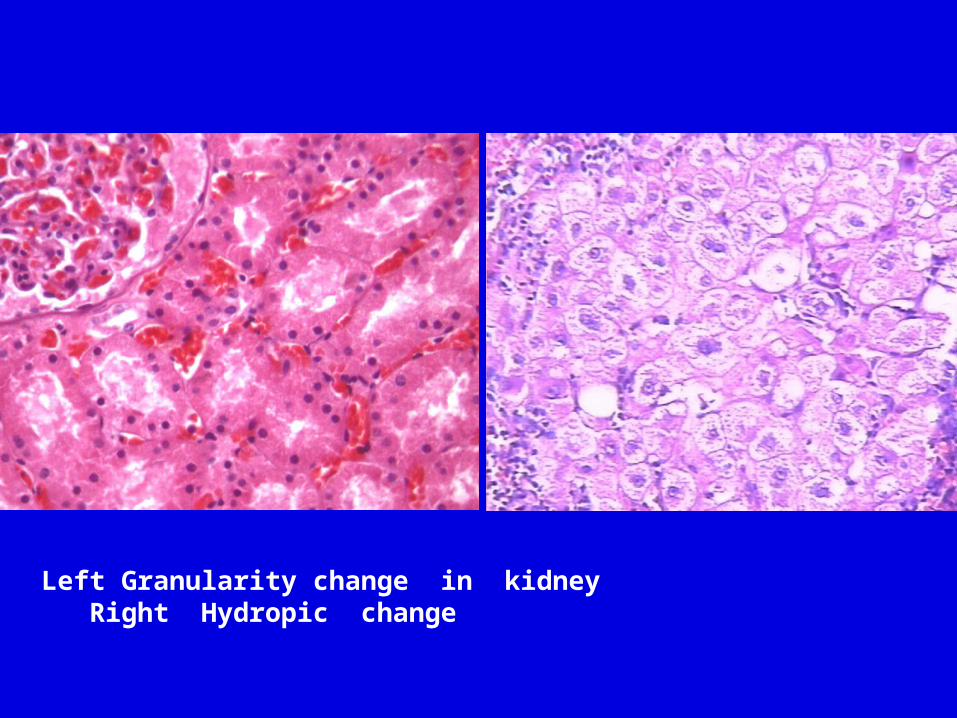
Left Granularity change in kidney Right Hydropic change
Mechanism:
Lack of oxygen Toxic Osmotic effect
Damage to mitochondria or its enzymatic pathways. The diminished formation of ATP affects all the energy requiring reaction in the cell but in particular leads to failure of the sodium pump. Sodium ions enter the cell in exchange for potassium and as the former have a larger hydration shell, there is a net influx of water.
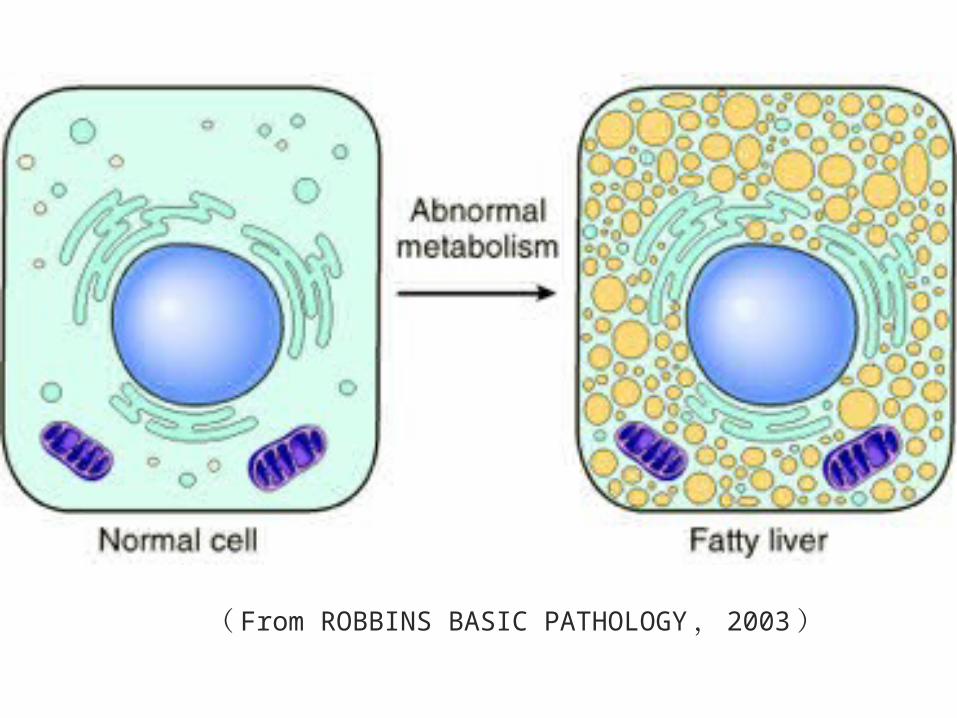
(2) Fatty change:
Definition: There is the accumulation of fat in non-fatty cells. Morphologic change:
Gross features:Gross features: The organ enlarges and becomes yellow, soft, and greasy.
LM:LM: An Fatty change appears as clear vacuoles within parenchymal cells.
Liver:Liver: Since this organ plays a central role in fat metabolism, the accumulation of fat in toxic conditions can be very considerable, fatty distribution varies with the cause, e. g. :
Poison, Toxins:Poison, Toxins: alcohol, infections, organic solvents etc. fat is found nearest the afferent blood supply (portal venue and hepatic arteriole).

Fatty change of liver
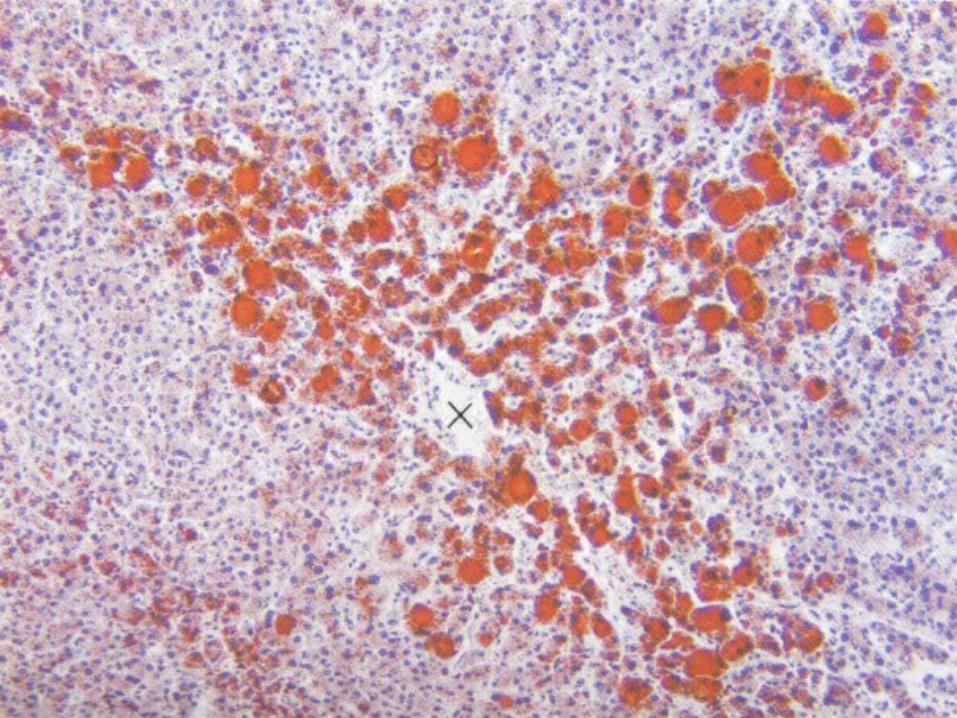
Left: Gross photograph .Center:Left: Gross photograph .Center: HE Stain. Right: Oil Red-O Stain . HE Stain. Right: Oil Red-O Stain .
( offered by Prof.Orr )
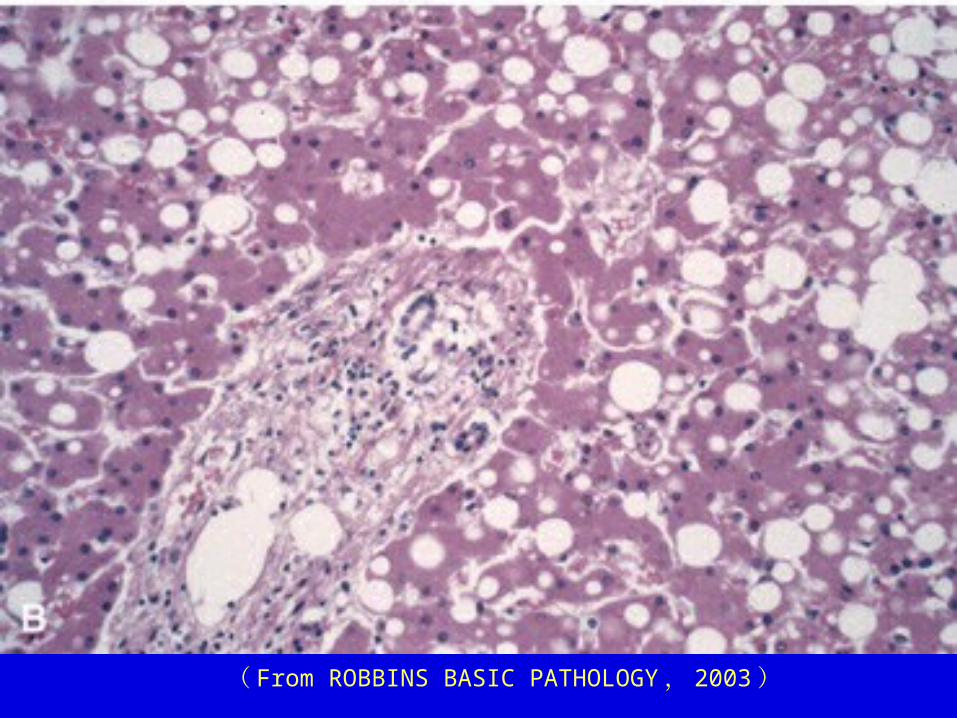
( From ROBBINS BASIC PATHOLOGY , 2003 )
Confirmation
Fresh frozen section Special stain Sudan Ⅲ : orange red
Osmic acid: black
Heart:Heart: It occurs in two patterns, in one,
prolonged moderate hypoxia, such as that produced by profound anemia, causes intracellular deposits of fat, which create grossly apparent bands of yellowed myocardium alterations with bands of darker, red-brown, uninvolved myocardium (tigered effect). In the other pattern of fatty change produced by more profound hypoxia or diphtheritic myocarditis, the myocardial cells are uniformly affected.
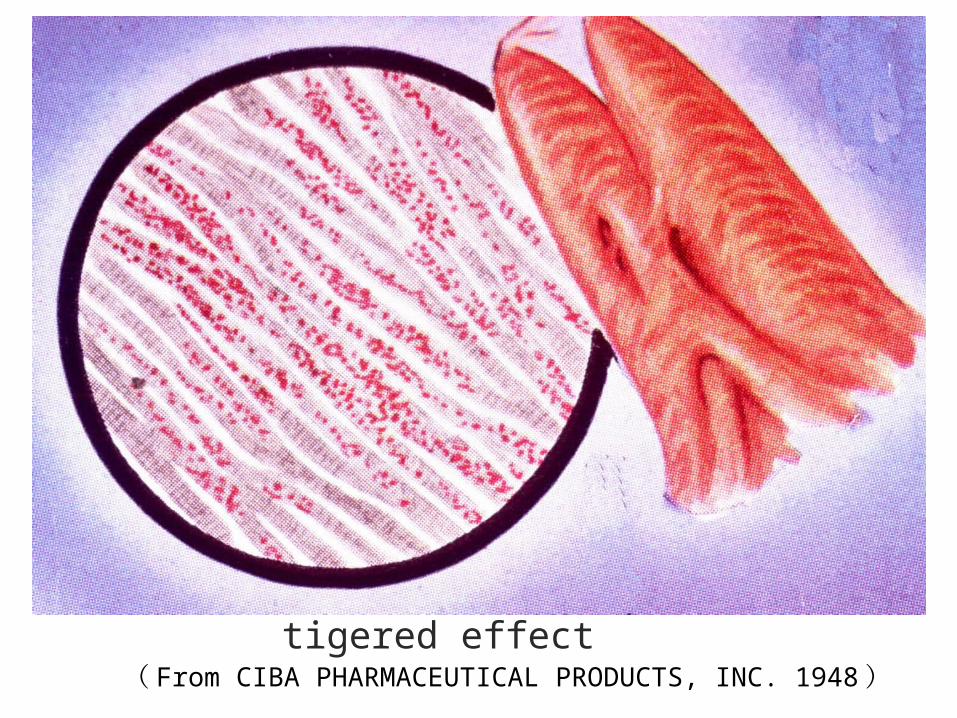
tigered effectProf. ( From CIBA PHARMACEUTICAL PRODUCTS, INC. 1948 ) Orr
Kidney:Kidney:
In most cases fatty change is confined to the epithelium of the convoluted tubules, but in severe poisoning it may affect all structures including the glomerule.
Causes: Poisons. e. g. carbon tetrachloride,
phosphorus (liver) Chronic alcoholism (liver) Infections Congestive cardiac failure Severe anaemia Ischaemia Diabetes mellitus Malnutrition and wasting disease.
Mechanism:
Impaired metabolism of fat
Excessive triglyceride into the cell.
Slide 2.9
( From ROBBINS BASIC PATHOLOGY , 2003 )
(3) Hyaline change:
Definition:Definition: Not a distinct chemical entity. Various histological or cytological alterations characterized by homogeneous, glasslike appearance in hematoxylin and eosin-stained sections.
Types:Types:
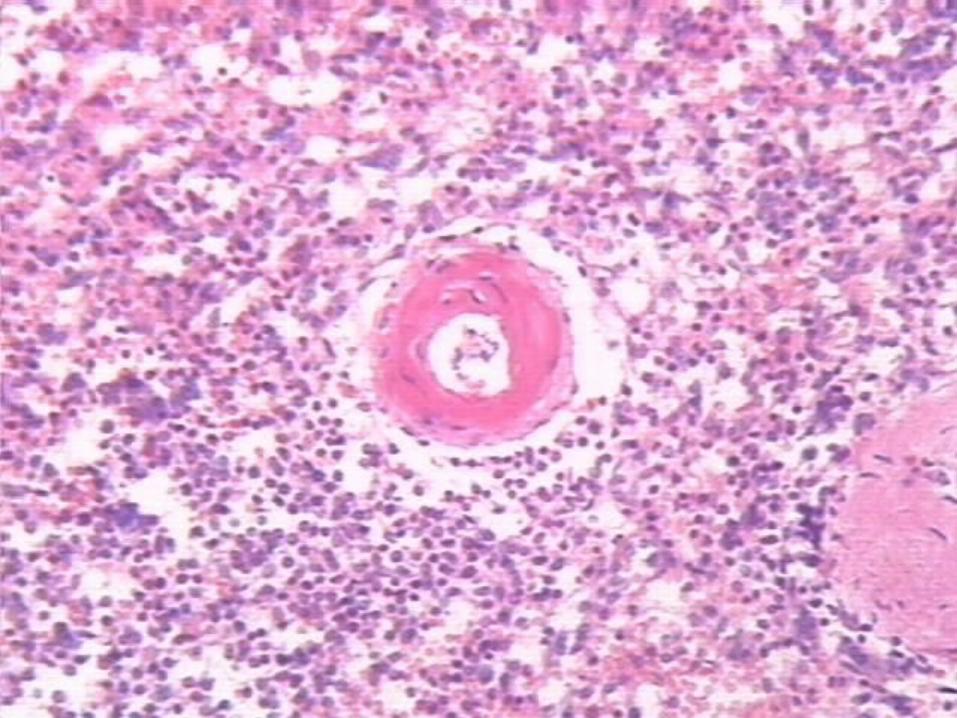
①① arterioles hyalin hyalin
In long-standing hypertension and diabetes mellitus, the walls of arterioles, especially in the kidney, become hyalinized, owing to extravasated plasma protein and deposition of basement membrane material.
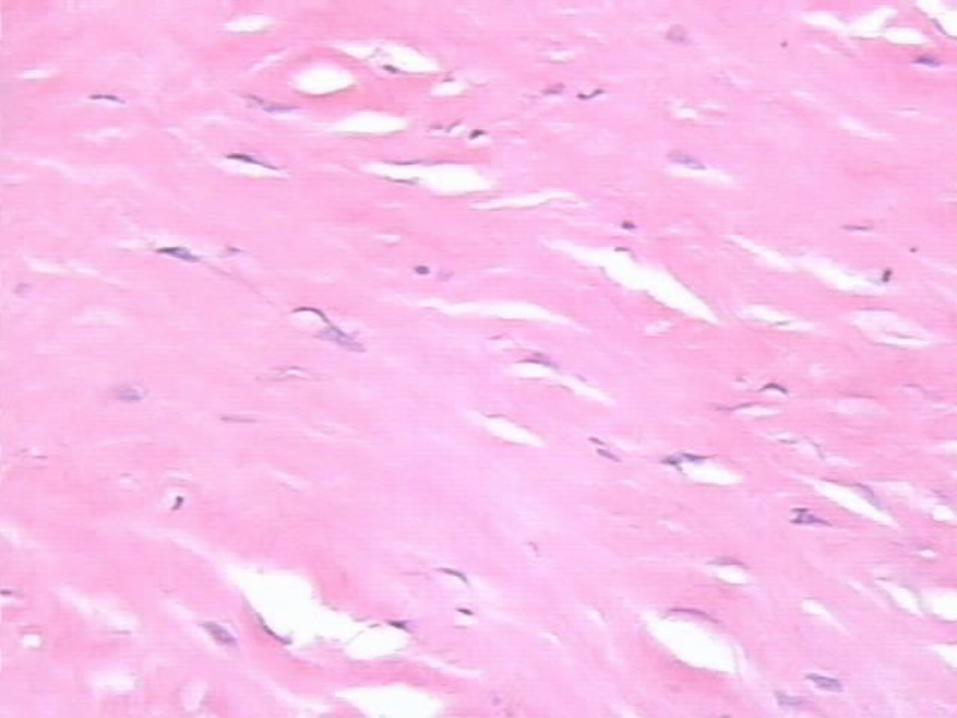
② Collagenous fibrous tissue hyalin in old scars may appear
hyalinized, but the physiochemical mechanism underlying this change is not clear.
With H. E. stains, the protein amyloid also has a hyaline appearance.
Intracellular hyaline:Intracellular hyaline:
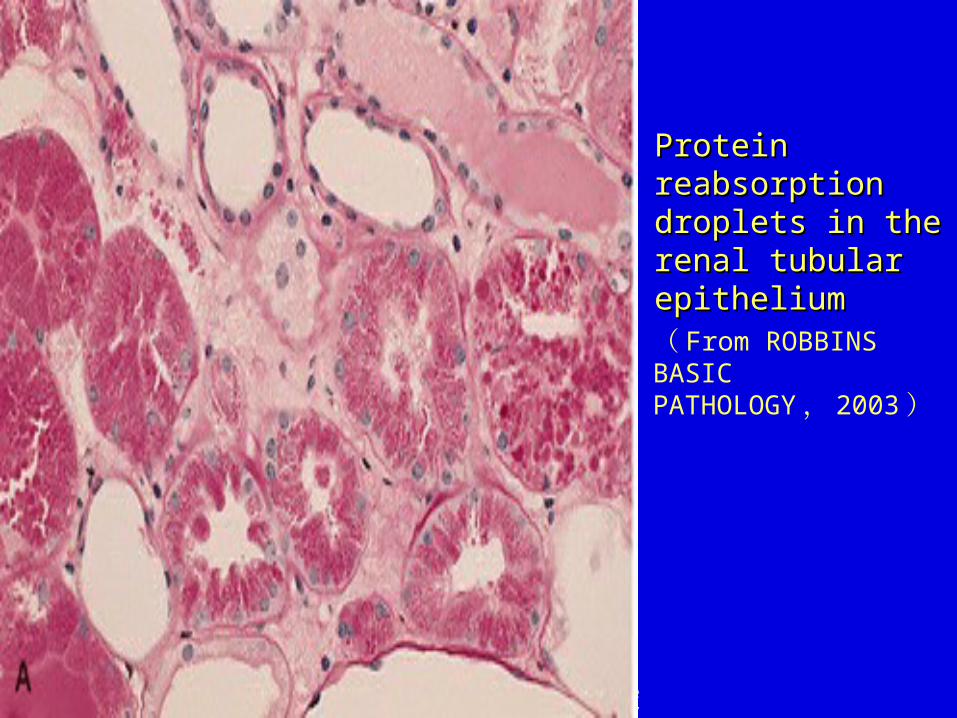
Restorative droplets:Restorative droplets: Renal tubules with phagolysosomes filled with plasma protein during proteinuria.
Mallory alcoholic bodies:Mallory alcoholic bodies: liver cytoplasmic aggregates of fragmented fine filaments and tubules, derived from hepatocyte cytoskeleton.
Russell bodies Russell bodies
W.B. Saunders Company items and derived items Copyright (c) 1999 by W.B. Saunders Company
Protein Protein reabsorption reabsorption droplets in the droplets in the renal tubular renal tubular epitheliumepithelium( From ROBBINS BASIC PATHOLOGY , 2003 )
(4) (4) Mucoid degeneration:Mucoid degeneration:
Definition:Definition: Change characterized by accumulation of mucin in intracellular or extracellular loci.
Types:Types: Epithelial: Mucin is composed of sialomucin plus neutral mucopolysaccharide. May accumulate in intracellular or extracellular (if secreted) locations.
Connective tissue:Connective tissue: Mucin is predominantly acid mucopolysaccharide, sulfated or carboxylated.
Mechanisms of accumulation:Mechanisms of accumulation:
Acute injury:Acute injury: Inflammation (as common cold ) causes hypersecretion by epithelium.
Late injury, repair:Late injury, repair: Overproduction by fibroblasts as in atherosclerosis, cardiac “myxoma”.
Neoplasia:Neoplasia: lack of access to duct results in intracellular (signet ring) or extracellular accumulation when cancer secretes much mucin (colloid carcinoma, cystadenoma of ovary).
Endocrine:Endocrine: Thyroid hypofunction produces increase in mucopolysaccharide in dermis (myxedema).
(5) (5) Amyloid degenerationAmyloid degeneration
General features:General features: a ‘waxy substance’ (amyloid substance) composed essentially of an abnormal protein is deposited in the extracellular tissue, particularly around the supporting fibres of blood vessels and basement membranes.
Detection:Detection:
Post-mortem organs:
Amyloid: deep brown
Lugol’s iodine Normal tissue: yellow
Biopsy materials:
Amyloid: red and specific apple LM: Congo red green fluorescence in polarized
light. Normal tissue: pale pink or yellow: No fluorescence.
EM: specific appearance: closely packed interlacing fibrils 70 to 100 A0 in diameter.
Nature of amyloid:
Chemical: protein:protein: variable. related to acute phase
reactive protein, which appears in the serum in many inflammatory conditions or derived from fragments of immunoglobulin molecules (particularly lambda light chains).
Carbohydrate:Carbohydrate: a glycosaminoglycan (e. g. heparin sulphate)——this give the iodine stain.
Physical:Physical: the fibrils are organized uniquely——β-pleated.
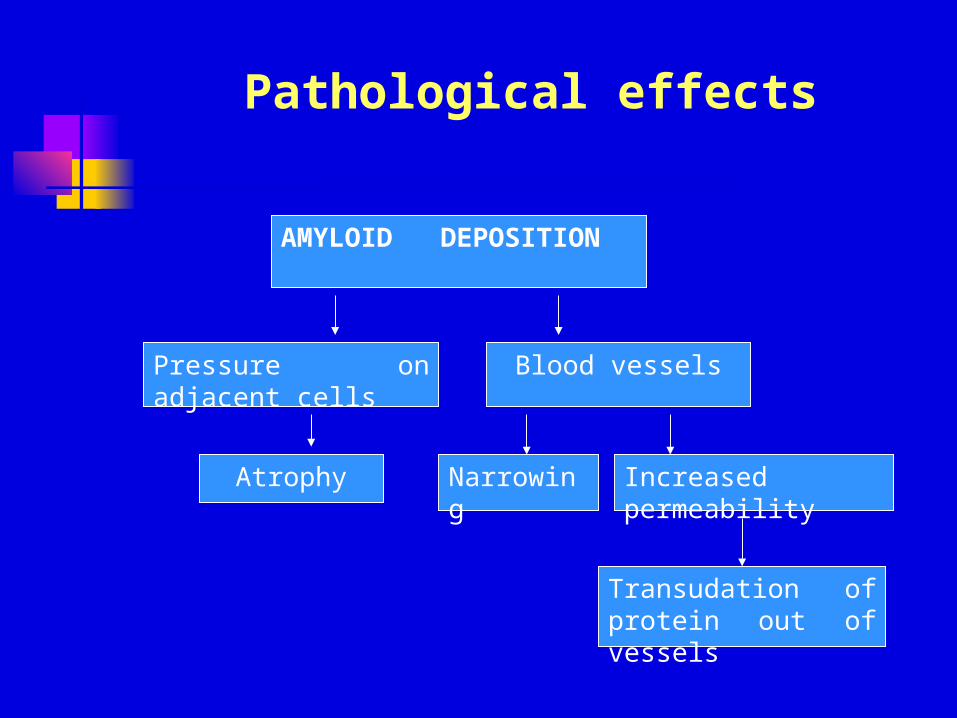
Pathological effects
AMYLOID DEPOSITION
Pressure on adjacent cells Blood vessels
Atrophy Narrowing Increased permeability
Transudation of protein out of vessels
Amyloidogenic proteins and polypeptides may also occur in other circumstances, e. g. in tumors of endocrine glands producing polypeptide hormones and in cases of rare familial amyloidosis.
In old age, minor deposits of amyloid may occur in the heart and brain; the amyloidogenic protein in these cases is related to prealbumin.
Types:Types:
Primary:Primary: without know cause
Secondary:Secondary: i. e. associated with chronic inflammatory diseases such as tuberculosis, osteomyelitis, rheumatoid arthritis.
Systemic:Systemic:
Localized:Localized:
(6) (6) Pathologic Pathologic calcificationcalcification
Definition:Definition: Abnormal deposits of calcium salts occur in any tissues except bones and teeth.
Type:Type:
①① Dystrophic calcification:Dystrophic calcification: Local deposits of calcium may occur in:
Necrotic tissue which is not absorbed.
Tissues undergoing slow degeneration. The mechanism may be as follows:
alteration of enzymes or PH.

( From ROBBINS BASIC PATHOLOGY , 2003 )
View looking down onto the unopened aortic View looking down onto the unopened aortic valve in a heart with calcific aortic stenosis.valve in a heart with calcific aortic stenosis.
②② Metastatic calcification:Metastatic calcification:
This alteration may occur in normal tissues whenever there is hypercalcemia. The causes of hypercalcemia include hyper Para thyroidism, vitamin D intoxication, systemic sarcoidosis, hyperthyroidism Addison’s disease.
Metastasis calcification may occur widely throughout the body but principally affects the interstitial tissues of the blood vessels, kidneys, lungs, and gastric mucosa
(7) Pigments:
exogenous
Pigments are colored substances
endogenous
①① HemosiderinHemosiderin Local breakdown of red cells in
tissues, e. g. in internal haemorrhage.
Extravasated red cells
Phagocytosis of red cells by macrophages
Haemosiderin (yellow)(Prussian Blue reaction)
Iron free pigments
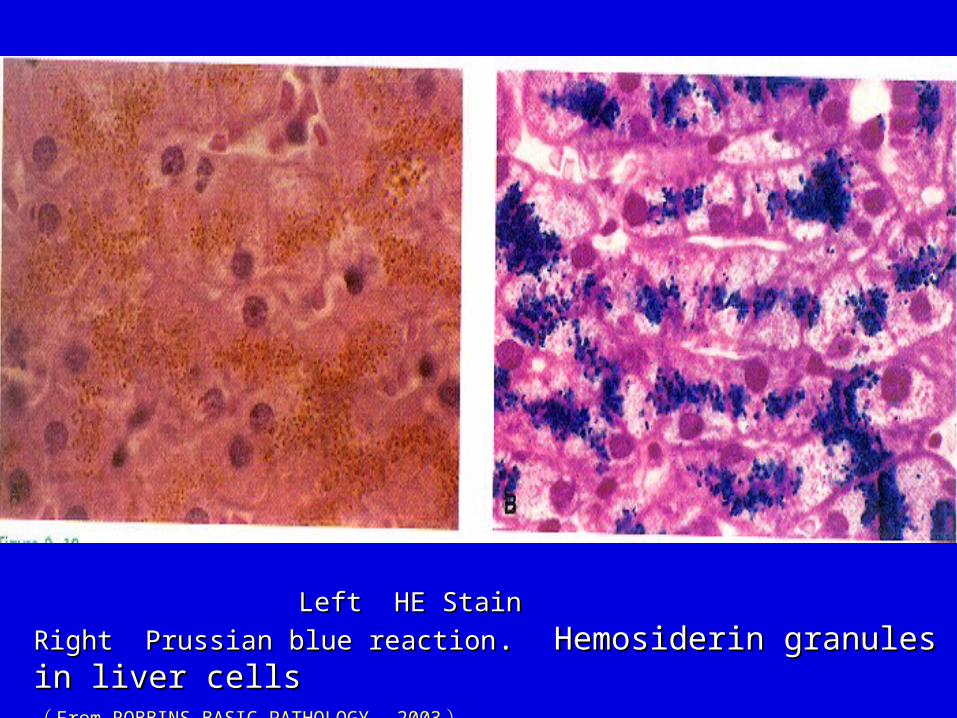
Left HE Stain Right Prussian blue Left HE Stain Right Prussian blue
reactionreaction. Hemosiderin granules in liver cells . Hemosiderin granules in liver cells ( From ROBBINS BASIC PATHOLOGY , 2003 )
②② Bilirubin:Bilirubin: When the bilirubin content of
the serum rises above 34μmol/L, jaundice appears.
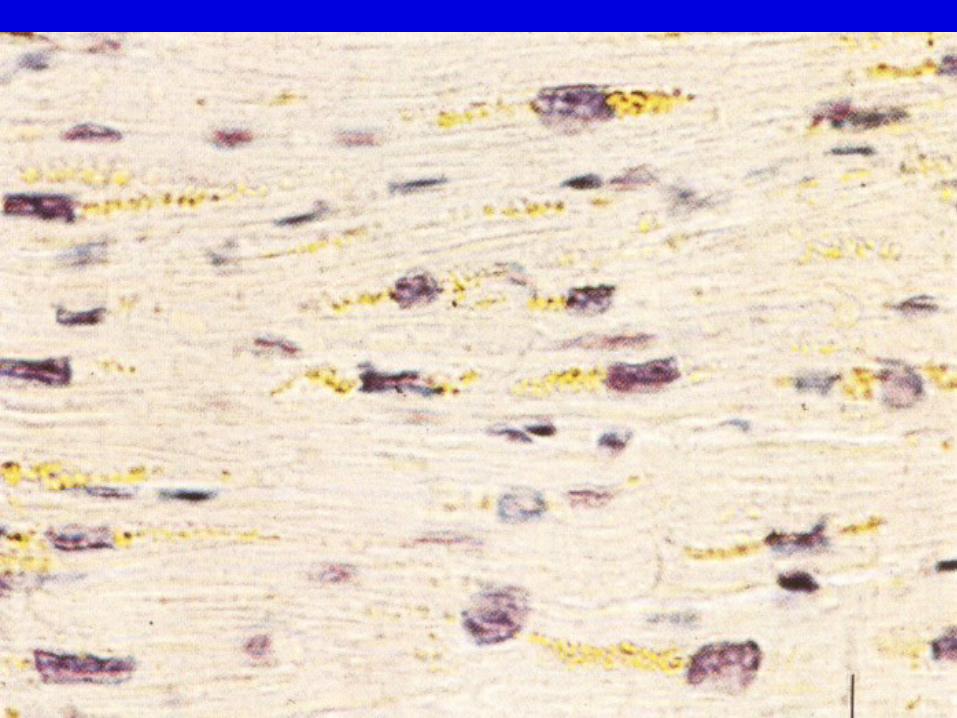
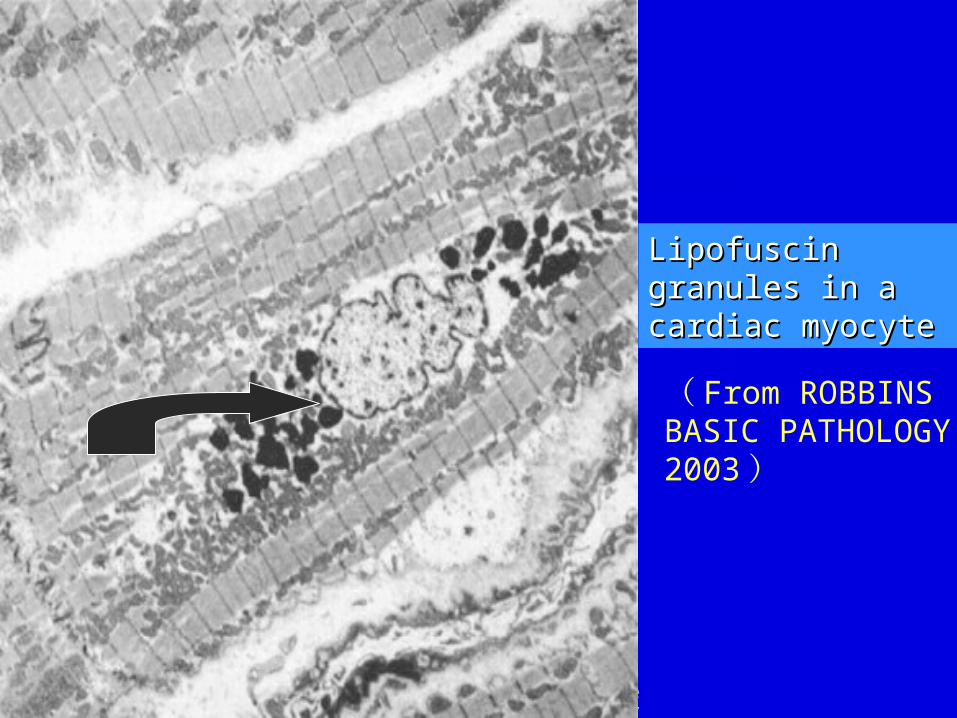
③ Lipofuscin This is a yellowish brown pigment
having high lipid content, often found in the atrophied cell or old age. It is particularly common in the heart muscle, and the term “brown atrophy” is often applied. It is also found in liver cells, testes and nerve cells.
W.B. Saunders Company items and derived items Copyright (c) 1999 by W.B. Saunders Company
Lipofuscin Lipofuscin granules in a granules in a cardiac myocyte cardiac myocyte
( From ROBBINS BASIC PATHOLOGY ,2003 )
④ Melanin
Melanin is a normal pigment found in the form of fine brown granules in the skin, choroids of the eye, adrenal medulla.
Local melanin pigmentation e. g. pigmented nevus, melanoma.
Generalized melanin pigmentation e. g. Addison’s disease.
⑤ Dust