Embed Size (px)
Citation preview

etiiwmniCniEwD9aaptE
em
Ea
RA
The Journal of Emergency Medicine, Vol. 35, No. 3, pp. 287–292, 2008Copyright © 2008 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/08 $–see front matter
doi:10.1016/j.jemermed.2007.08.071
Selected Topics:Emergency Radiology
THE ROLE OF CT PERFUSION IMAGING IN ACUTE STROKE DIAGNOSIS:A LARGE SINGLE-CENTER EXPERIENCE
Ansaar T. Rai, MD,* Jeffrey S. Carpenter, MD,* James A. Peykanu, MD,† Teppe Popovich, MD,*Gerald R. Hobbs, PHD,‡ and Jack E. Riggs, MD§
*Department of Radiology, †Department of Psychiatry, ‡Department of Community Medicine, and §Department of Neurology,West Virginia University Health Sciences Center, Morgantown, West Virginia
Reprint Address: Ansaar T. Rai, MD, Department of Radiology, P.O. Box 9235, West Virginia University Health Sciences Center,
Morgantown, WV 26506-9235am
a(cabfiissd
asficnjra
cim
Abstract—The objective of this study was to determinehe utility of computed tomography perfusion (CTP) scansn diagnosing acute ischemic stroke (AIS). CTP abnormal-ties in two contiguous supratentorial levels were correlatedith diffusion weighted image (DWI) abnormalities onagnetic resonance imaging (the standard for stroke diag-
osis) performed within 1 week in 422 suspected acuteschemic strokes. Of 157 AIS confirmed by DWI, 78 showedTP abnormalities (sensitivity 49.7%). All of these exami-ations were performed with a mean of 35 min from the
nitial emergency department neurological examination.xcluding small non-vascular territory strokes left 77 AISith a total volume of infarcted tissue of more than 5 cc byWI. Of these, 71 showed CTP abnormalities (sensitivity2.2%). Of the 265 patients without AIS, none showed CTPbnormalities (specificity 100%). CTP is a rapid, readilyvailable and effective method of diagnosing AIS in clinicalractice, particularly the major intracranial vessel strokeshat result in a more devastating outcome. © 2008lsevier Inc.
Keywords—acute stroke; perfusion; CT; computed to-ography
INTRODUCTION
mergency physicians are frontline doctors in the battlegainst stroke. In a disease process as dynamic and evolving
ECEIVED: 1 October 2006; FINAL SUBMISSION RECEIVED: 5
CCEPTED: 10 August 2007287
s an acute stroke, accurate initial evaluation and manage-ent by these physicians is crucial.Significant limitations exist in the clinical accuracy
nd reliability of recognizing acute ischemic strokeAIS) (1–4). Currently, 1–2% of all stroke patients re-eive acute thrombolytic therapy, with considerable vari-tion among physicians (5–7). Administration of throm-olytics in the face of an uncertain diagnosis and concernor hemorrhage is one of the most important factors citedn a low treatment rate for acute stroke (7,8). The Amer-can Academy of Emergency Medicine, in its positiontatement on the use of intravenous thrombolytics fortroke, correctly identifies the risks of such use withoutiagnostic certainty or definite supportive evidence.
Ancillary diagnostic modalities are inconsistently avail-ble for diagnosing acute ischemic stroke. Currently, diffu-ion weighted images (DWI) and apparent diffusion coef-cient maps on magnetic resonance imaging (MRI) areonsidered the most reliable imaging tests for stroke diag-osis, against which other neuroimaging modalities areudged (9–11). However, limited availability and lack ofound-the-clock coverage in most hospitals limit its utilitys a primary diagnostic tool for stroke.
Because effective therapeutic interventions are time-ritical, any method that enhances the accuracy, reliabil-ty, and speed in the diagnosis of AIS is important. Theost widely used radiological modality in the evaluation
2007;
July
omoasIhmupm
D
UrupBtCsnsatDwatgetb
lccsM
I
Cr(ptMaS(arflgf
I
ToimFpvsd
Fte
288 A. T. Rai et al.
f acute stroke syndromes is non-contrast computed to-ography (CT). Although very useful in excluding hem-
rrhage, non-contrast CT, which alone has been used inll initial studies on thrombolytic therapy in AIS, is notensitive in recognizing early signs of ischemia (12,13).n recent studies, computed tomography perfusion (CTP)as been shown to be an accurate and reproducibleethod of assessing AIS (14–17). Our experience in
tilizing CTP in the assessment for AIS in over 400atients in routine clinical practice at a single academicedical center is described.
MATERIALS AND METHODS
esign
nder an institutional review board-approved protocol, aetrospective analysis was performed of all patients whonderwent CTP as part of our routine evaluation for sus-ected stroke at Ruby Memorial Hospital at the Robert C.yrd Health Sciences Center of West Virginia University, a
ertiary care referral center. From April 2001 to April 2005,TP was performed on 867 patients admitted for suspected
troke. Patients in whom intracerebral hemorrhage wasoted on initial unenhanced CT scan did not have a CTPtudy as part of our routine acute stroke evaluation. Theverage time to obtain the CT scans was 35 min from theime of initial neurological evaluation in the Emergencyepartment. Only patients who had a follow-up MRI scanithin 1 week were included in this analysis. Because
lmost all of the perfusion CT images had been obtained inhe supratentorial brain, generally at the level of the basalanglia, patients with posterior fossa stroke (n � 48) werexcluded. Additionally, patients treated with thrombolyticherapy (n � 67) to prevent confounding the comparisonetween CTP and MRI-DWI, and patients with technically
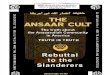
igure 1. CT perfusion parameters: Perfusion parameters at
hese are mean transit time (MTT), cerebral blood flow (CBF), andntire left middle cerebral artery distribution is obvious with increimited or unsatisfactory CTP studies (n � 32) were ex-luded. Accordingly, 422 patients were included in thisomparison analysis of CTP abnormalities seen at admis-ion with subsequent DWI abnormalities seen on follow-upRI scan.
mage Acquisition
TP was performed through a 2-cm section of supratento-ial brain consisting of two adjacent 1-cm thick slicesLightspeed; GE, Milwaukee, WI, USA). Gantry tilt waserformed parallel to the anterior cranial fossa at the level ofhe basal ganglia. Intravenous contrast (Optiray 320,
allinckrodt Inc., St. Louis, MO) was administered in anntecubital vein at a rate of 4 cc/s for a total of 50 cc.equential scanning, performed at the rate of two rotations/s1 image/rotation) for 50 s, yielded 100 images (50 im-ges/slice). From these source images, perfusion mapseflecting the mean transit time (MTT), cerebral bloodow (CBF), and cerebral blood volume (CBV) wereenerated. The follow-up MRI-DWI sequences were per-ormed using a volumetric acquisition (10 mm thick, no gap).
mage Processing
he source CTP images were retrospectively re-processedn a workstation (ADW 4.0_06.11; GE) using special-zed analysis software (CT perfusion-2, 2.6.6i; GE). CTPaps were generated evaluating MTT, CBF, and CBV.or each patient, a total of six perfusion maps wererocessed (3 parameters/slice) (Figure 1). For DWI, theolumetric diffusion data were reformatted to match thelab of brain interrogated by CT perfusion. This wasone by visually matching ventricular and brain con-
vel in the supratentorial brain are shown. From left to right
one le cerebral blood volume (CBV). A large infarct involving theased MTT and decreased CBF and CBV.

tmvvoavlbd
I
IMoCDcp
mpTpwcpA�cmait
D
Ti
Fwtac inimum( iffusio
CT Perfusion Imaging in Acute Stroke Diagnosis 289
ours. Two slices (each 1 cm thick) were generated toatch the perfusion levels (Figure 2). For DWI, the total
olume of diffusion abnormality, termed the “infarctolume,” was determined using histogram analysis basedn pixel intensity threshold after removing regions ofrtifactually increased signal that predominantly in-olved the inferior frontal and the anterior temporalobes; this yielded an infarct volume in cubic centimetersased on the total diffusion MRI abnormality in threeimensions (Figure 3).
mage Analysis
mage analysis comparing the CTP parameters and theRI-DWI (Figure 4) was performed by two neuroradi-
logists. The first neuroradiologist evaluated only theTP images and the second evaluated only the MRI-WI scans. The two neuroradiologists were blinded to
linical presentation and to each other’s assessment. For
igure 2. Image preparation for perfusion-diffusion analysis. (hite lines representing the two levels of perfusion imaging. (
o the area imaged on CTP. (C) A CT cerebral blood flow mamirror image ROI in the contralateral hemisphere. Area
ontralateral ROI and the average blood flow with its mD) Follow-up MRI shows a region of interest outlining the d
erfusion parameters, a region of interest (ROI) was M
anually drawn using a freehand select tool around anyerfusion abnormality on each of the three parameters.he absolute perfusion value and the relative percentageerfusion as compared to the contralateral hemisphere,hich was used as a reference, were calculated. The
hanges in the perfusion parameters were quantified as aercentage of the contralateral unaffected hemisphere.n MTT � 100% was abnormal. A CBF or CBV100% was abnormal. The mean time to perform and
omplete the stroke CT scan, including CTP, was 35in. Although CTP maps were retrospectively re-cre-
ted, the CTP scans and radiological interpretation weremmediately available to the treating physicians at theime of their initial performance.
ata Analysis
he sensitivity and specificity of CTP parameters in detect-ng AIS, as defined by DWI abnormality on follow-up
teral scout X-ray image for the CTP study shows two parallelcorresponding level of the diffusion slice on MRI is matchedan ROI drawn around the area of decreased blood flow andormality in mm2, the percentage of CBF compared to the
and maximum values are displayed below the image.n abnormality.
A) A laB) Thep withof abn
RI, were calculated.

OnstdM1tnbsa4(7ise
Mvtaiv7C87
Lsmwmt
F( the tol
FmdCp
290 A. T. Rai et al.
RESULTS
f the 422 patients who had a follow-up MRI and wereot excluded for the reasons indicated, AIS was demon-trated by DWI abnormality on MRI in 157 patients. Ofhe 265 patients who did not have AIS by DWI, noneemonstrated an abnormality on their CTP parametersTT, CBV, or CBF. Hence, the specificity of CTP was
00% for AIS; there were no false-positive studies. Ofhe 157 patients who did have AIS by DWI, MTT wasormal in both CTP slices in 79, CBV was normal inoth CTP slices in 90, and CBF was normal in both CTPlices in 79 patients. Hence, utilizing two CTP slices, anbnormal MTT was present in 78 of 157 AIS (sensitivity9.7%), an abnormal CBV was present in 67 of 157 AISsensitivity 42.7%), and an abnormal CBF was present in8 of 157 AIS (sensitivity 49.7%). Recognizing the lim-tation of utilizing only two CTP slices (a small ischemictroke might not be included in either of the two slicesxamined), AIS with a volume of 5 cc or greater on
igure 3. Infarct volume measurement using image-intensshown as a pale green ROI at right) was utilized to calculateeft (as area under the curve).
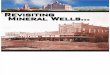
igure 4. Comparison of CT perfusion maps with correspondaps of MTT, CBF, and CBV (from left to right) show a larg
istribution secondary to a left MCA thrombus. The perfusio
T scan. The final infarct on the DWI sequence (last image), shownerfusion abnormality.RI-DWI were also counted and analyzed separately. Aolume of 5 cc as a cut-off was used because we foundhat all strokes secondary to a major vessel occlusion had
volume � 5 cc and all small non-vascular territorynfarcts had volumes � 5 cc. There were 77 AIS witholume � 5 cc. An abnormal MTT was present in 71 of7 of these larger AIS (sensitivity 92.2%), an abnormalBV was present in 64 of 77 of these AIS (sensitivity3.1%), and an abnormal CBF was present in 71 of these7 AIS (sensitivity 92.2%).
DISCUSSION
ike any therapeutic intervention, stroke treatmenthould be based on selecting patients who will deriveaximum benefit from treatment and excluding those inhom such treatment can be detrimental or futile. Theinimum requirement of any diagnostic test for stroke is
o at least identify the large vessel infarcts (such as those
sitive histogram analysis. A shaded diffusion abnormalitytal infarct volume, measured at 99.38 cc in the graph on the
ce-matched diffusion image on MRI. The three perfusion CTfusion abnormality involving the left middle cerebral arteryrmalities were evident despite a normal non-contrast head
ity-sen
ing slie per
n abno
as a large bright area, corresponds to and matches the CT
siecfteottwrpirllmml
mtasCcCarcc
ot8titpntstitcsun
hnw
eTatcj
TtospScf
Tibd
1
CT Perfusion Imaging in Acute Stroke Diagnosis 291
econdary to middle cerebral artery occlusion) that resultn the most devastating outcomes. In our study, wexcluded patients who received any therapy to preventonfounding the comparison between CTP and MRIrom the effects on final infarct size due to thrombolyticherapy, either intravenous or endovascular. The groupxcluded due to treatment did not differ in demographicsr presentation compared to the non-treated group. Also,he number of patients excluded due to thrombolyticreatment was small enough, compared to all the patientsho underwent CTP, so as not to confound or impact the
esults of the rest of the study. Our results show thaterfusion CT has a very high sensitivity for detectingnfarcts due to a major vessel occlusion. This sensitivityeaches 92% by excluding small non-vascular territory,acunar or white matter infarcts that cause relatively mildong-term deficits. The larger severe strokes involve the
iddle cerebral artery or the internal carotid artery ter-inus and can have the maximum benefit from revascu-
arization (18–20).This study demonstrates that CTP is an effective
ethod of recognizing ischemic stroke in clinical prac-ice, particularly the more serious ones. As CT softwarend computing speed improvements occur and moreections of brain can be rapidly imaged, the sensitivity ofTP in the recognition of AIS should reasonably in-rease. In this regard, we are now currently performingTP in eight slices of brain instead of two in the samemount of time. Our experience in using CTP in theoutine evaluation for AIS suggests that CTP may be-ome the diagnostic study of choice to support the initiallinical evaluation of suspect AIS patients.
Lastly, CT evaluation for stroke has logistical advantagever MRI due to its increased availability and shorter scanimes (21). We performed an emergent stroke CT scan in67 patients. This is the largest number of such examina-ions reported from a single center. Among the patientsncluded in our study who suffered a stroke, the averageime to obtain the stroke CT scan including all three com-onents was 35 min from the initial Emergency Departmenteurological evaluation. Again, such scan times have yeto be rivaled by another modality. The performance ofimultaneous CT angiogram to localize an offendinghrombus not only adds to its diagnostic power but alsos useful in planning an endovascular intervention. Withhe advent of telemedicine, data from a stroke CT scanan be transferred across networks. Teleradiology fortroke shows encouraging preliminary results, but is stillnderutilized (22–24). It may, however, allow commu-ity hospitals to treat stroke (25).
A hospital and emergency department where compre-ensive services are available can potentially serve as theexus of a “tele-stroke network” in triaging patients. This
ill increase the confidence of the referring hospitals andmergency physicians in handling these complex cases.he supportive diagnostic tests such as CT perfusion andngiography have been available and studied for someime now. The next step is their possible widespreadlinical implementation, which may allow for more ob-ective and patient-specific treatment.
LIMITATIONS
he retrospective nature of the study is its major limita-ion. Additionally, the two perfusion imaging levels werebtained in the supratentorial brain. Posterior fossatrokes were thus excluded from the study and the role oferfusion imaging in these strokes could not be assessed.imilarly, the patients receiving any treatment were ex-luded and the reversibility or irreversibility of the per-usion abnormalities was not addressed.
CONCLUSION
he utility of CT perfusion in stroke diagnosis, as well asts logistical feasibility, make it a diagnostic tool that cane potentially incorporated in stroke triage and treatmentecisions.
REFERENCES
1. Goldstein LB, Simel DL. Is this patient having a stroke? JAMA2005;293:2391–402.
2. Goldstein LB. Improving the clinical diagnosis of stroke. Stroke2006;37:754–5.
3. Hand PJ, Kwan J, Lindley RI, et al. Distinguishing between strokeand mimic at the bedside, the brain attack study. Stroke 2006;37:769–75.
4. Hand PJ, Haisma JA, Kwan J, et al. Interobserver agreement forthe bedside clinical assessment of suspected stroke. Stroke 2006;37:776–80.
5. Kaste M. Approval of alteplase in Europe: will it change strokemanagement? Lancet Neurol 2003;2:207–8.
6. Kaste M, Fogelholm R, Rissanen A. Economic burden of strokeand the evaluation of new therapies. Public Health 1998;112:103–12.
7. Chan YF, Kwiatkowski TG, Rella JG, Rennie WP, Kwon RK,Silverman RA. Tissue plasminogen activator for acute ischemicstroke: a New York City emergency medicine perspective. J EmergMed 2005;29:405–8.
8. Brown DL, Barsan WG, Lisabeth LD, Gallery ME, MorgensternLB. Survey of emergency physicians about recombinant tissueplasminogen activator for acute ischemic stroke. Ann Emerg Med2005;46:56–60.
9. Na DG, Thijs VN, Albers GW, Moseley ME, Marks MP. Diffusion-weighted MR imaging in acute ischemia: value of apparent diffu-sion coefficient and signal intensity thresholds in predicting tissueat risk and final infarct size. AJNR Am J Neuroradiol 2004;25:1331–6.
0. Chong J, Lu D, Aragao F, et al. Diffusion-weighted MR of acute
cerebral infarction: comparison of data processing methods. AJNRAm J Neuroradiol 1998;19:1733–9.
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
292 A. T. Rai et al.
1. Chen PE, Simon JE, Hill MD, et al. Acute ischemic stroke:accuracy of diffusion-weighted MR imaging—effects of b valueand cerebrospinal fluid suppression. Radiology 2006;238:232–9.
2. von Kummer R, Nolte PN, Schnittger H, et al. Detectability ofcerebral hemisphere ischaemic infarcts by CT within 6 h of stroke.Neuroradiology 1995;38:31–3.
3. Patel SC, Levine SR, Tilley BC, et al. Lack of clinical significanceof early ischemic changes on computed tomography in acutestroke. JAMA 2001;286:2830–8.
4. Wintermark M, Thiran J-P, Maeder P, et al. Simultaneous measure-ment of regional cerebral blood flow by perfusion CT and stable xe-non CT: a validation study. AJNR Am J Neuroradiol 2001;22:905–14.
5. Gillard JH, Antoun NM, Burnet NG, et al. Reproducibility ofquantitative CT perfusion imaging. Br J Radiol 2001;74:552–5.
6. Wintermark M, Fischbein NJ, Smith WS, et al. Accuracy ofdynamic perfusion CT with deconvolution in detecting acute hemi-spheric stroke. AJNR Am J Neuroradiol 2005;26:104–12.
7. Maruya J, Yamamoto K, Ozawa T, et al. Simultaneous multi-section perfusion CT and CT angiography for the assessment ofacute ischemic stroke. Acta Neurochir (Wien) 2005;147:383–92.
8. Paciaroni M, Arnold P, Van Melle G, Bogousslavsky J. Severedisability at hospital discharge in ischemic stroke survivors. Eur
Neurol 2000;43:30–4.9. Lee BI, Nam HS, Heo JH, Kim DI. Yonsei stroke registry. Anal-ysis of 1,000 patients with acute cerebral infarctions. CerebrovascDis 2001;12:145–51.
0. Arnold M, Nedeltchev K, Mattle HP, et al. Intra-arterial thrombol-ysis in 24 consecutive patients with internal carotid artery t occlu-sions. J Neurol Neurosurg Psychiatry 2003;74:739–42.
1. A systems approach to immediate evaluation and management ofhyperacute stroke. Experience at eight centers and implications forcommunity practice and patient care. The National Institute ofNeurological Disorders and Stroke (NINDS) rt-PA Stroke StudyGroup. Stroke 1997;28:1530–40.
2. Wang S, Gross H, Lee SB, et al. Remote evaluation of acuteischemic stroke in rural community hospitals in Georgia. Stroke2004;35:1763–8.
3. Johnston KC, Worrall BB. Teleradiology Assessment of Comput-erized Tomographs Online Reliability Study (TRACTORS) foracute stroke evaluation. Telemed J E Health 2003;9:227–33.
4. Misra UK, Kalita J, Mishra SK, Yadav RK. Telemedicine inneurology: Underutilized potential. Neurol India 2005;53:27–31.
5. Schwamm LH, Rosenthal ES, Hirshberg A, et al. Virtual telestrokesupport for the emergency department evaluation of acute stroke.
Acad Emerg Med 2004;11:1193–7.
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具