Embed Size (px)
Citation preview

Self-Change: Common Pathway to Recovery
From Alcohol and Drug Problems
Linda C. Sobell, Ph.D., [email protected]
Scotland’s Future ForumFresh Perspective on
Alcohol and DrugsDecember 6, 2007

• Briefly look at where addictions field was 35 years ago and highlight selected major changes with respect to providing treatment services
• Look at prevalence and process of self-change and its implications for clinical treatment
• Present results from a large scale community mail in intervention designed to promote self-change
• Consider public health and policy implications of this work
• Questions after talk relating to Scotland’s Future Forum
Objectives

Addictions Field Circa 1970• Research scare; most knowledge
derived from folk science• Very few treatment programs; inpatient norm• Treatment services then and now PRIMARILY
for severely dependent substance abusers• Abstinence ONLY goal!• Motivation something clients brought to
treatment; if not, not ready to change• Gambling not an addiction under study• Nicotine dependence not diagnosis until DSM
III• Dominant treatment approaches: AA and 28-
day Minnesota Model

• Concept of continuum did not exist: Everyone viewed and treated as severely dependent
• Cognitive-behavioural treatments for substance abusers nonexistent
• Brief treatments and self-change were considered as heresy
• Terms like problem drinker and harm reduction not in our vocabulary
• Addictions problems viewed as progressive and irreversible; and
• Recovery only possible through treatment or traditional self-help groups
35 Years Ago Addictions Field Looked Very Different

Recovery Only Possible Through
Treatment
• Robert Dupont, 1993, "Addiction is not self–curing. Left alone addiction only gets worse, leading to total degradation, to prison, and ultimately to death.”
• V. E. Johnson,1980, "Alcoholism is a fatal disease, 100% fatal. We estimate that 10% of drinkers in America will become alcoholic, and that these people will not be able to stop drinking by themselves. They are forced to seek help; and when they don’t, they perish miserably.”
• Hazelden, 2003, “Untreated addiction will ultimately kill you.”

Where We Are Today
• All treatments look very similar; consequently, field seen as at impasse• Instead of continuing to look at effective treatments NEED to
• Look at the change process in general • Take broad perspective on change process
• Looking ONLY at clinical cases obscures big picture • To complete the picture, field needs to understand process of SELF-CHANGE and its implication for treatment

Why Study the Self-Change Process?
• “Addiction looks very different if you study it in general populations compared to treated cases”
Robins 1993• “If you only study the tip of the iceberg your view of
the disorder will be very biased.” Cahalan, 1987• “We cannot understand the natural history of
alcoholism by only studying clinic populations.” Vaillant & Milofsky 1984
• “Way ahead in alcoholism treatment research should embrace study of ‘natural forces’ that can then be captured and exploited by planned interventions.” Orford & Edwards 1977

Natural Recovery Studies Not New• 1814: Dr. Benjamin Rush, signer of
Declaration of Independence, described several cases of natural recoveries from alcohol problems
• Early Classic Pioneering Studies (‘60s-’70s): Winick, Vaillant, Tuchfeld, Rozien, Fillmore
• Vietnam Veterans’ Study: one of largest natural recovery studies (Robins)
• Different Types of Natural Recovery Studies
• Longitudinal studies • Population surveys• Convenience samples

Review of Studies of Natural Recovery From Alcohol and Drug Problems(Sobell, et al., Addictions, 2000, pp.749-764; recent update Carballo et al, 2007)
• 1960s-1997: 38 studies met inclusion criteria• # Respondents: Mean = 141; Median = 43• Advertisements = 40%; Females = 30% • Mean recovery = 6.3 yrs; Mean problem =
10.9 yrs• Problem Type: Alcohol, 75%; Heroin, 22.5%;
Cocaine, 7.5%; Marijuana, 2.5% • Recovery Status: Low-risk Drinking = 40.3%;
Limited Drug Use = 11.5%• 1999-2005: 22 studies met inclusion criteria

Self-Change Well Recognized Phenomenon Outside of Addictions Field
• Most psychological problems never discussed with mental heath professionals; rather shared with ‘natural helpers’ who have no training (Toro, 1986)
• More Americans try to change health behaviours through self-help than all other forms of professional programs (Davison et al, 2000)
• Natural recovery rule rather than exception for problem gambling (Slutske et al., 2003)
• Persistent stuttering not intractable — improvement occurs without professional help--most learned to self-manage their disorder (Finn, in press)
• 25% of people successfully lose weight and 83% do so on own (Consumer Reports, 2002)

Major Findings From Self-Change Studies
• Today there are over 60 studies of the self-change process in the addiction field
• Self-change is very enduring: Almost all recoveries > 1 year and 50% > 5 years
• Vast majority of moderate drinking recoveries occur outside of treatment programs
• While multiple pathways to recovery (e.g., treatment, self-help), predominant pathway is self-change

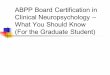
Individuals Who Have Recovered from Alcohol Dependence
For At Least 1 Year (N = 4,422)
Ever treated
26%
Never treated
74%
Majority Recovered Without Treatment
Dawson et al., (2005) Recovery from DSM-IV alcohol dependence:
US, 2001-2002. Addiction. 100(3):281-92

• Three quarters of those who were previously alcohol dependent, recovered on their own; that is, without treatment
• 21% of of those who changed without treatment did so for 5 or more years
• 18% were low risk drinkers

How Does Self-Change Occur?
What are the clinical implications?
Next Step

Major Processes Associated with Self-Change and Clinical Implications
• Cognitive Appraisal of Risky Behaviours
• Affect-Related Statements• Behavioural Monitoring and
Actions Statements• Supportive Statements from
Others

Cognitive Appraisal of Risky behaviours
• Over 2/3’s of respondents’ reported evaluating costs and benefits of their behaviour; at some point they say reported seeing that the negatives outweighed the positives and then the scale tipped in favor of changes
• Clinical Implication: Incorporate Decisional Balancing Exercises into clinical interventions as they appear to accelerate the self-change process

Decisional Balance Exercise Helps to Address Ambivalence and
Helps to Increases Motivation to Change
Benefits of Changing Costs of Changing
Benefits of Not Changing Costs of Not Changing

2nd Process Linked to Self-Change Affect-Related Statements
It is not just the rationality that drives the change process,
rather its the emotional quality or affective context of
reasons for change

Reasons for Quitting Smoking Emotional Content Differs
Imminent Consequential Threats Health insult; spot on lung; spouse died of smoking illness
PotentialInformationalThreatsSmoking causes cancer, stroke, decreaseslife expectancy

Imminent Consequential Threats
Used Past Month* Pregnant Not Preg
Illicit Drug Use * 4.3% 10.4%
Cigarettes 18.0% 30.7%
Alcohol: use * 9.8% 53.0%
Alcohol: binge days * 4.1% 23.2%
Alcohol: heavy use
*Significant
0.7% 4.3%
SAMSA, 2002/2003; women ages 15-44.

#3: Behavioural Monitoring and Actions Statements
• Respondents report engaging in self-regulatory process
• Gave themselves feedback to enact those changes
• Similar to motivational interventions where self-monitoring and advice/feedback routinely used to help clients evaluate their behaviour with intent of motivating them to change

#4: Supportive Statements From Others
• Support from others reported important to self-change process
• Parallels treatment studies where positive outcomes associated with positive social support
• Clinical implication: Successful interventions need to consider social support for clients

What Do We
Know Today?
20072007

Self-Change: 2007• Major route to recovery for multiple health and
mental health behaviours Cigarettes, Alcohol, Drugs, Gambling, Obesity,
Stuttering, Juvenile Delinquency, Mental Health Problems
• Vast numbers of people do not enter treatment; overwhelming reason relates to stigma of being labeled (e.g., stutter, alcoholic, addict, obese)
• Better understanding of what drives and maintains change process (e.g., decisional balance; cognitive appraisal)
• Identifying mechanisms of change has major implications for treatment and prevention

What is Happening to the Masses?*
• In 2003 ONLY 8% in US who met criteria for Substance Use Disorder received any services in past year
• And of those, 50% did not complete treatment!
• For the 92% who received no services, ONLY 5% reported needing treatment
**SAMSA (2004). Results from the 2003
National Survey on Drug Use and Health.

Taking the Treatment to the Masses
• Considerable evidence shows TREATED alcohol abusers represent but a fraction of those whose alcohol/drug causes them problems
• Only small percentage who have alcohol/drug problems cross the clinical threshold
• Why won’t they come for treatment?• Vast majority say STIGMA associated with
being labeled “alcoholic” or “drug addict”• Alternative: Use community mail-in
intervention to reduce alcohol/drug problems• Most of us don’t know self-change is possible!

% Who Know Someone Who Had Resolved an Alcohol Problem on Their Own
53.20%
37.80%
29.70%25.70%
13.80%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Per
cent
Self-Changersn=109
Alcohol AbusersUnresolved
Untreated n=45
Alcohol Abusersin Treatment
n=195
Significant Othersof Self-Changers
n=108
GeneralPopulation No
Alcohol Problemn=435

Perceived Optimism for Self-Change:
Treatment Not Needed
49.2%43.8%
32.5% 32.3% 31.6%
18.0%13.5%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Pe
rce
nt
Tobacco(n=458)
Cannabis(n=375)
Gambling(n=400)
Medication(n=402)
Alcohol(n=452)
Cocaine(n=376)
Heroin(n=375)

% Who Know Someone Who Had Alcohol,
Tobacco, or Cocaine Problem90.2%
82.00%
34.10%
82.6%
54.60%
48.40%
85.0%
31.90%
44.20%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Pe
rce
nt
(515
/571
)
(469
/572
)
(194
/56)
(347
/408
)
(423
/512
)
(79/
248)(2
54/4
65)
(38/
86)
(92/
190)
Cig Alc Coc Cig Alc CocCig Alc Coc
Ever Have Problem Dealt With Problem Resolved On Own

Attracting the MassesWhat a Message Says
is Critical!• Unwanted messages evoke resistance
and produce counter arguments
• For example, when high risk drinkers told they are “alcoholic,” they start thinking of reasons why they are not
• To attract intended target audience messages need to be carefully crafted

Studies of the self-change process suggest it is important to………
• Avoid labels (e.g., alcoholic, addict)
• Promising confidentiality
• Send message that many people DO RECOVER ON THEIR OWN
• Offer interventions outside of clinical settings
Use Evidence Based Message to Attract Those Who Do Not
Seek Treatment

1 year Empirically Crafted Message1 year Empirically Crafted MessageAttracted Close to 2,500 CallsAttracted Close to 2,500 Calls
NIAAA Funded StudyNIAAA Funded Study

Promoting Self-ChangeCommunity Mail Out Intervention
• People responded to ads
• Screened for eligibility: No past history of treatment/help for alcohol problems
• Assessment materials mailed out
• Respondents completed assessments at home
• Respondents mail their completed questionnaires to PO box
• Study materials sent to respondents based on their group assignment
• 12 month mail follow-up

Response to Empirically Crafted Advertisements# of respondents 2,434
# (%) met screening criteria and sent assessment materials
1,756 (72.1%)
# (%) returned assessment, met criteria, in study
825 (47.0%)

Promoting Self-Change: Community Intervention for
825 Problem Drinkers
Experimental Group
Control GroupReceived 2 Alcohol Education Pamphlets
and Drinking Guidelines Available in
the Community
Randomly Assigned

Control GroupReceived 2 Alcohol Education/Drinking Guideline
Pamphlets Available in the Community

Promoting Self-Change: Community Intervention for 825
Problem Drinkers
Experimental Group Motivationally
Enhancing Personalized Feedback
Control Group
Randomly Assigned

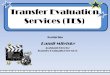
Where Does Your Drinking Fit In? Personalized Feedback
Weekly alcohol consumption Health risks AUDIT score & problem level Self-confidence profile How much is too much? What do you do next?
Experimental Group:Experimental Group: Answers to assessment Answers to assessment materials used to prepare advice feedback materialsmaterials used to prepare advice feedback materials

Where Does Your Drinking Fit In?Personal Feedback for _______
7-16 Drinks7%
17+ Drinks6%
1-6 Drinks46%
0 Drinks41%
QuickTime™ and a decompressor
are needed to see this picture.
You reported drinking an average of43 drinks per week

Where Does Your Drinking Fit In?Personal Feedback for _______
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0-17 18-39 > 39
Average number of drinks per week
QuickTime™ and a decompressor
are needed to see this picture.
You reported drinking an average of43 drinks per week

Demographic Variables (N = 825)
Male 67.7%
Employed (full or self) 60.2%
Married or widowed 63.5%
Completed high school 85.5%
Completed some university 30.8%
White collar 62.1%
White (ethnicity) 94.4%
Mean age (years) 47.5

Alcohol Variables (N = 825)
Mean yrs drinking problem 11.4
Mean arrests 0.5
Mean hospitalizations 0.1
Mean AUDIT score (0-40) 20.2
% days drinking past year 77.7%
Mean drinks/drinking days 6.0

Promoting Self-Change Mail Intervention
Results• Several drinking and non-drinking
variables examined
• No significant differences between the two interventions
• Both groups produced significant drinking related changes 1 year pre- to 1-year post intervention

What Happened? 1 Year Pre-Post Intervention
• 15% reduction number of drinking days
• 18% reduction number of drinks per drinking day
• 28% reduction mean drinks per per week
Significant Decreases

If Motivational Materials Had No Value Beyond the Two Informational
Pamphlets, What Caused Participants to Change
Their Drinking?

What Precipitated the Change in Both Groups?
• Seeing ad increased motivation to change, thus facilitating change
• Brief telephone screening triggered self-evaluation process leading to change
• Completing in-depth assessment materials (2-3 hours)
• All of the above • None of the above

Answer
• For all major drinking measures, significant reductions occurred between seeing ads and calling, but before receiving assessment materials
• Ads, like brief interventions, appear to catalyzed respondents’ motivation and commitment to change
• Similar to trigger events or tipping point in natural recovery studies
Responding to AdsResponding to Ads

First Contact: Respondents Asked Why They Responded To Ad
Ad Title: “Thinking of Changing Your Drinking 29%
Statement: “75% of people changed on their own” 27%
“Wanted to change on their own” or “Didn’t want to come to treatment”
25%

Fig. 1: Mean Days Drinking/Week
5.41 5.254.66 4.54 4.49
0
1
2
3
4
5
6
Pre 1-11 Pre 1 Ad Assess Post 12
Fig. 2: Mean Drinks/Drinking Day
5.74 5.8
4.45 4.584.31
0
1
2
3
4
5
6
7
Pre 1-11 Pre 1 Ad Assess Post 12
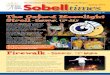
Fig. 3: Mean Drinks/Week
30.23 29.82
22.36 21.71 21.03
0
5
10
15
20
25
30
35
Pre-1 11 Pre 1 Ad Assess Post 12
Fig. 4: % Days Drinking 5 or More Drinks
43.74 43.03
30.98 29.93 28.31
0
10
20
30
40
50
Pre 1-11 Pre 1 Ad Assess Post 12
P< .05P< .001
P< .05
P< .001
P< .001
P< .05
P< .001

Future Research Directions
• Clinical trials MUST examine and control for Mechanisms of Change beyond treatment effects—ads, assessments, talking with screener, online material
• Use time course analysis to examine changes at critical hypothesized time junctures using sensitive measure of change (e.g., daily drinking)

Where Do Mail Interventions Fit in Overall System of Health Care With Finite Number of Resources?
Sensible 1st Step in Stepped Care Model of
Treatment

Stepped Care Model Services/interventions need to be
Least restrictive Least intrusive Least costly Likely to have good outcomes
Have consumer appeal

Serious relapse requires further treatment at
appropriate intensity
Negative Outcome
Matched to treatment based on research and
clinical judgment
Matched to treatment based on research and
clinical judgment
Positive
Outcome
Positive
Outcome
Positive
Outcome
Negative Outcome
Population newly entering treatmentPopulation newly
entering treatment
Treatment "A"Treatment "A"
Treatment "B"Treatment "B"
Treatment "C"Treatment "C"
Treatment "D", etc.Treatment "D", etc.
STEPPED CARESTEPPED CARE
Treatment
intensity
increases
Continued positive
outcome:
Monitor only
Continued positive
outcome:
Monitor only
Serious relapseSerious relapse
Negative Outcome

Public Health and Policy Implications of Mail Interventions
• In context of a Stepped Care Model, promoting self-change through mail-in interventions is consistent with efficient approach to health care
• As a 1st STEP, mail-in interventions are least restrictive, least intrusive, and to date have good outcomes, and CONSUMER APPEAL
• From Harm Reduction perspective, stepped care looks at incremental improvements
• When intervention does not work, step up care

Public Health and Policy Implications
• Ad was change mechanism that appeared to motivate many to change drinking
• Low cost population approaches can reach large numbers who are unwilling or not ready to access traditional health care settings
• Such interventions could be coupled with messages to seek treatment if self-change was not successful
• Interestingly, during 12 months after mail intervention some participants never previously in treatment reported stepping up own care

Post Intervention Treatment Seeking
• 28% sought some help or treatment during 1 year after intervention
• Treatment seekers significantly more impaired pre-intervention
• Added benefit of mail interventions some problem drinkers never in treatment sought additional help, stepped up their own care

Providing Interventions Outside the Clinical Arena
• Addiction field needs to respond to full range of addictive behaviours by offering multiple and varied pathways to change
• Such efforts, however, will require FIELD TO SHIFT from its longstanding clinical focus to a broader public health perspective