Embed Size (px)
Citation preview

REVIEW Open Access
Self-determination theory: its application tohealth behavior and complementarity withmotivational interviewingHeather Patrick1* and Geoffrey C Williams2
Abstract
Mounting evidence implicates health behaviors (e.g., nutrition, physical activity, tobacco abstinence) in varioushealth outcomes. As the science of behavior change has emerged, increasing emphasis has been placed on theuse of theory in developing and testing interventions. Self-determination theory (SDT)-a theoretical perspective-andmotivational interviewing (MI)-a set of clinical techniques-have both been used in health behavior interventioncontexts. Although developed for somewhat different purposes and in relatively different domains, there is a gooddeal of conceptual overlap between SDT and MI. Accordingly, SDT may offer the theoretical backing thathistorically has been missing from MI, and MI may offer SDT some specific direction with respect to particularclinical techniques that have not been fully borne out within the confines of health related applications of SDT.Research is needed to empirically test the overlap and distinctions between SDT and MI and to determine theextent to which these two perspectives can be combined or co-exist as somewhat distinct approaches.
Self-Determination Theory: Its Application toHealth Behavior and Complementarity withMotivational InterviewingAn impressive body of research has provided convincingevidence for the pivotal role of behavior in well-being,and morbidity and mortality, as well as health care costs[1]. Indeed, some estimates indicate that nearly 3/4 ofall health care costs are attributable to chronic diseasesresulting from health behaviors such as tobacco use andexposure, poor diet, and physical inactivity [2]. Otherresearch has shown that adherence to five key lifestylebehaviors (eliminating tobacco exposure, body massindex (BMI) < 25, engaging in 30 minutes of physicalactivity or more per day, consuming alcohol in modera-tion, and eating a healthy diet) reduced coronary eventsby 62% over 16 years in a cohort of 42,000 US adultmen. Further, men who adopted at least two of thesebehaviors had 27% lower risk for cardiovascular eventscompared to those who did not [3]. Lifestyle behaviorsaccount for some 40% of mortality in industrializedcountries and have been implicated in up to 2/3 of all
cancers [4] as well as the onset and management of obe-sity, diabetes, cardiovascular disease, heart attacks, andstroke. Given the importance of health behaviors towell-being, health outcomes, and disease processes,developing a rigorous science of health behavior, itschange and maintenance is critical to prolonging bothlength and quality of life.In recent years, the science of health behavior change
has increasingly emphasized theory- based approachesto intervention. The use of theory to inform and testinterventions is important both for expanding basicscience and for developing interventions that have real-world practical utility. From the perspective of basicscience, theories must be tested in multiple domainsand through multiple methods to refine and expandthem appropriately. Further, the use of theory is impor-tant to applications in health behavior change and main-tenance because theories often inform us on howinterventions work by identifying underlying mechan-isms, thus providing more proximal targets of interven-tion (i.e., mediators and moderators of interventioneffects). Mediators may help to clarify the processes bywhich an intervention is efficacious and may be usefulin circumstances when an intervention has either adirect or an indirect effect on the primary outcome. For
* Correspondence: [email protected] of Cancer Control and Population Sciences National CancerInstitute 6130 Executive Boulevard Rockville, MD 20852-7335 USAFull list of author information is available at the end of the article
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
© 2012 Patrick and Williams; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.

example, an intervention may have no direct effect on aparticular behavioral outcome but may indirectlyimprove the outcome via its effect on a psychosocialvariable such as self-efficacy or motivation. Thus, inter-ventionists may refine interventions to specifically targetthese intervening variables yielding more efficient inter-ventions. In other circumstances, an intervention maydirectly impact a behavioral outcome, and mediatorsmay elucidate the mechanisms through which an inter-vention functions and the sequence by which behaviorchange occurs. In this way, change in a mediator maybe an important outcome in and of itself whereby inter-ventionists and practitioners can gage whether an inter-vention is functioning in predicted ways prior to theassessment of the behavioral outcome at the end of anintervention (or other follow-up period). Moderatorsmay help to clarify for whom and under what circum-stances an intervention is efficacious (e.g., an interven-tion is particularly effective for a particularsociodemographic subgroup). Thus, interventions maytarget the populations for whom they are most effica-cious and effective and/or be tailored to become moreeffective for other populations. Theory can also lead toparadigm shifts in how change and its maintenance aremeasured and how treatment outcomes are assessed.While a theory’s parsimony, applicability to a range ofbehaviors and outcomes, and capacity to be refined andexpanded are all important to basic science, good the-ories must also be practical. That is, theories must berigorous not only from a scientific standpoint but alsofrom a practical standpoint. To the extent that theoriesare consistent with clinical guidelines and tenets of clini-cal practice (e.g., medical professionalism, principles ofbiomedical ethics), they are better suited to not onlyscientific but also practical discourse.The late 1970s and early 1980s saw the emergence of
a key theory (i.e., self-determination theory; SDT) andclinical style (motivational interviewing; MI) that havebeen used to understand and intervene with healthbehavior. Although these efforts were spear-headed bytwo different groups and, to some extent, for two differ-ent purposes, today the parallels between SDT as a the-ory and MI as a style of clinical practice-as they applyto health behavior-are becoming increasingly clear [5-8].These parallels have been further clarified as SDTresearchers have developed efficacious clinical interven-tions based on SDT and MI techniques that facilitatehealth behavior change through change in the SDTmediators of autonomous self-regulation and perceivedcompetence [e.g., [9-12]]. In addition, MI has movedtoward a formal statement of theory in a recent publica-tion [13]. Together, these events suggest that the synth-esis of SDT (and its mediators) with MI techniques maybe a potent combination that can contribute to the field
of health behavior change. MI’s movement toward astatement of theory also allows a closer comparison ofcommon theoretical underpinnings between SDT andMI. We also offer discussion of some potential differ-ences between MI and SDT not discussed previously.The purpose of this piece is to discuss self-determina-tion theory and the more practical aspects of its applica-tion to health behavior in both research and clinicalcontexts and to further explore potential conceptualoverlaps and distinctions between SDT and MI.
Self-Determination TheorySelf-determination theory (SDT [14,15]) is a general the-ory of human motivation that emphasizes the extent towhich behaviors are relatively autonomous (i.e., theextent to which behaviors originate from the self) versusrelatively controlled (i.e., the extent to which behaviorsare pressured or coerced by intrapsychic or interperso-nal forces). SDT defines motivation as psychologicalenergy directed at a particular goal. Many theories ofhuman behavior account for the direction of behavior,but fail to account for how that behavior is energized[14]. SDT has thus emphasized the importance of moti-vational quality in addition to its quantity. It has alsooffered a particularly comprehensive approach to study-ing health behavior via its conceptualization and mea-surement of autonomy, perceived competence,relatedness to others, and its emphasis on the role ofthe social context in supporting or thwarting optimalmotivation.The Motivation ContinuumTraditionally, theories of motivation have made a dis-tinction between intrinsic and extrinsic motivations.Intrinsic motivation is characterized by engaging inbehaviors for their own sake, while extrinsic motivationis characterized by engaging in behaviors for someseparable outcome, whether this comes in the form oftangible rewards, social acceptance, proving somethingto oneself, or maintaining consistency between one’svalues and one’s behaviors. Given these definitions,many behaviors-particularly those relevant to healthpromotion (e.g., making dietary changes), disease pre-vention (e.g., screenings such as colonoscopy), and dis-ease management (e.g., taking medications)-are likelyextrinsic in nature [e.g., [16,17]]. However, not allextrinsic motivations are equivalent. Ryan and Connell[18] proposed a motivational continuum within SDT tobetter characterize the extent to which extrinsic motiva-tions are relatively more or less internalized.SDT uses the term “internalization” to describe the
process by which behaviors become relatively moreautonomously regulated or valued over time. Autono-mous self-regulation is particularly important for healthbehavior because the more autonomously-regulated an
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 2 of 12

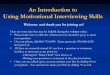
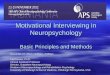
individual is toward a given behavior, the greater effort,engagement, persistence, and stability the individual islikely to evidence in that behavior [19]. According toSDT, the least internalized form of regulation is externaland reflects engaging in behaviors to gain some rewardor avoid some negative contingency. So, for example,someone may stop smoking because his surgeon willnot perform needed coronary artery bypass surgeryunless he stops smoking first, or because he wants the$800 his employer is offering to smokers for stopping.Introjected regulation involves engaging in behavior outof some sense of guilt or obligation or out of a need toprove something to oneself or others (i.e., enhance self-worth). Thus, a person may stop smoking because shewould feel guilty about the emotional and financial tur-moil her family would have to face if she were to have aprolonged illness and early death. The next most inter-nalized form of regulation (i.e., the first level of autono-mous regulation) is called identified in which case aperson engages in a behavior because it is important tothem. For example, someone may stop smoking becausehe personally believes it is an important goal to accom-plish. Finally, the most internalized form of extrinsicmotivation is integrated. Integrated regulations aremotives for behaviors that are important to the person,and they are engaged because they are also consistentwith one’s other goals and values. So, someone maystop smoking because she values her health, and quit-ting smoking is consistent with her other goals in life (e.g., maintaining a regular exercise routine, living longerto enjoy her family). Figure 1 provides a visual represen-tation of the continuum of extrinsic motivation. It isworth noting that, while described here as discrete,exclusive forms of motivation and self-regulation, it isquite common-particularly in health behavior-for
different forms of regulation to coexist for the samebehavior and to vacillate over time and across contexts.For example, someone may exercise because he valueshis health (identified regulation) but also because, as ahealth behavior researcher, he would feel guilty if he didnot engage in the behavior he prescribes to patients, cli-ents, or intervention study participants (introjectedregulation).Need Support: The Social Context and the MotivationContinuumOne of the defining features of SDT is its treatment ofboth the person (i.e., personality) and the situation (i.e.,the social context) in motivated behavior. That is, at apersonality level, individuals may orient to their sur-roundings in relatively more or less autonomous waysand thus their behaviors may be, on average, relativelymore or less autonomously regulated. However, person-ality does not tell the full story. Indeed, the social con-text may support or thwart autonomous self-regulationand the process of internalization in any given domain.According to SDT, the extent to which one experiencesneed support from various contexts (e.g., doctor-patientinteractions) is largely predictive of how autonomously-regulated one is likely to be for prescribed behaviors.SDT has identified three psychological needs critical
to supporting the process of internalization and thedevelopment of optimal motivation and personal well-being. The need for autonomy reflects the need to feelchoiceful and volitional, as the originator of one’sactions. Competence involves the need to feel capable ofachieving desired outcomes, conceptually similar to self-efficacy in social cognitive theory. Finally, relatednessreflects the need to feel close to and understood byimportant others. When people experience the satisfac-tion of these needs in a given context, they are more
Type of Regulation
Definition
Health Behavior Example
External
Regulation
Introjected
Regulation
Identified
Regulation
Integrated
Regulation
Behaving to gain somereward or avoid somenegative contingency
Behaving out of a senseof guilt or obligation or aneed to prove something
Behaving because of theimportance one ascribesto the behavior
Behaving because thebehavior is consistentwith other goals & values
Losing weight to get aprize and/or recognitionin a competition
Losing weight becauseone feels that obesity is acharacter flaw
Losing weight because ahealthy weight is animportant goal to accomplish
Losing weight because it isconsistent with other healthgoals (e.g., lower cholesterol)
Figure 1 The Extrinsic Motivation Continuum.
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 3 of 12

likely to be autonomously self-regulated around thebehaviors relevant to that context. Thus, to the extentthat a patient feels his needs for autonomy, competence,and relatedness are supported in a discussion with hisprimary care doctor about, for example, modifying hisdiet to include more fruits and vegetables, the patient islikely to feel more autonomously self-regulated (i.e.,more identified or integrated) around this recommendedhealth behavior change.Given the importance of need support in facilitating
internalization, SDT has offered suggestions for specificbehavioral strategies that may support one or more ofthese needs. For example, autonomy supportive beha-viors include eliciting and acknowledging patients’ per-spectives and emotions before makingrecommendations; supporting patients’ choices andinitiatives; providing a rationale for advice given; provid-ing a menu of effective (i.e., evidence-based) options forchange; minimizing control and judgment; and explor-ing how relevant health behaviors relate to patients’aspirations in life. For example, a practitioner workingwith a patient on tobacco cessation may support thepatient’s autonomy by asking the patient to expresswhat the patient thinks it would be like to deal withstressful situations without smoking (i.e., by eliciting thepatient’s perspectives and emotions). Competence sup-port involves being positive that patients can succeed;reframing past failures as short successes; providingaccurate effectance feedback in a non-judgmental man-ner; identifying barriers; skills building and problem sol-ving; and developing a plan that is appropriatelychallenging to patients’ skill and experience level. Com-petence support may be particularly relevant in the con-text of failure. For example, a patient may have gonetwo weeks without smoking but started smoking after aparticularly stressful event at work. The practitionercould support the patient’s need for competence byfocusing on the accomplishment of being smoke-free fortwo weeks and discussing with the patient the importantgains that were made in that (e.g., knowing that quittingfor 2 weeks is possible; learning more about triggers forsmoking, etc.). Both theoretical conjecture and somerecent empirical evidence in applications of SDT tohealth suggest that authentic perceived competencedoes not emerge without the person feeling fully voli-tional (i.e., autonomously regulated [20]). Thus, support-ing patient autonomy by ensuring that patients are fullyvolitional or willing to consider change is also relevantto supporting competence. Finally, relatedness supportincludes providing unconditional positive regard (parti-cularly in the face of failure to achieve desired goals),being empathic with patients’ concerns, and providing aconsistently warm interpersonal environment. Thus, apractitioner may support a patient’s need for relatedness
by expressing understanding about how difficult makinga behavior change like quitting smoking can be andreflecting the patient’s concerns about failure. Supportfor all three needs requires that clinicians are activelyengaged with their clients, and that they take a client-centered approach to the interaction. For example, eli-citing and acknowledging the client’s perspective startswith active listening and includes reflections (e.g., briefsummaries of the thoughts, emotions, and plans the cli-ent has about the health issue being addressed). Typi-cally perceived need support from health carepractitioners has been measured with the Health CareClimate Questionnaire, (HCCQ [21-23]).The concept of need support is one factor that makes
SDT particularly amenable to health contexts as it isconsistent with biomedical ethics [24], law and medicine[25], medical professionalism [26], and informed deci-sion making [27,28]. Respect for patient autonomy is anintegral part of all health care interventions. Biomedicalethics has elevated respect for autonomy to one of threehighest- priority outcomes of all healthcare encounters,equivalent to those of enhancing patient welfare andimproving social justice (e.g., eliminating discrimina-tion). Thus, SDT’s emphasis on supporting basic psy-chological needs, particularly individuals’ need forautonomy, is consistent with these more general princi-ples of patient care, making its practical utility in clinicaland healthcare contexts paramount. These general prin-ciples of patient care also suggest that measuring auton-omy and its change is important-if not essential-fortranslational research, as all clinical interventions areobligated to respect autonomy regardless of the theoreti-cal frame it is based upon, or the outcome it is intendedto change. Biomedical ethics establishes that respect forautonomy and autonomous self-regulation is an impor-tant health outcome in and of itself. This topic isaddressed further by Vansteenkiste and Williams, thisissue.AspirationsAs described above, SDT has focused on the role of per-sonality-level (i.e., motivational orientations) anddomain-specific (i.e., self-regulation) forms of motiva-tion, and has emphasized the importance of the socialcontext in supporting or thwarting the process of inter-nalization. SDT has also addressed the role of valuesand aspirations in goal pursuits [29,30]. Specifically,SDT has distinguished aspirations that are extrinsicfrom those that are intrinsic. Extrinsic aspirations reflectgoals that are relatively external to the self and includewealth, fame, and image. Intrinsic aspirations reflectgoals that are more internal to the self and includemeaningful relationships, personal growth, communitycontributions, and, importantly, health. Research onaspirations within the SDT framework has focused
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 4 of 12

largely on the extent to which people value intrinsicrelative to extrinsic aspirations. When individuals placeprimary emphasis on extrinsic aspirations, they evidencelower levels of autonomy and relatedness as well aspoorer physical and mental well-being and greaterhealth risk behaviors. In contrast, placing strongeremphasis on intrinsic aspirations has been associatedwith a variety of positive outcomes including greaterautonomy and vitality [29-32]. Recent interventionsapplying SDT to healthcare contexts have placed anemphasis on exploring patients’ aspirations as a meansof aligning the patient’s broader life goals with goals forhealth behavior change. A newly-emerging body ofresearch is also examining the internalization of aspira-tions over time (i.e., the extent to which individualsbegin to shift focus from placing stronger emphasis onextrinsic aspirations to intrinsic aspirations [33]) and therole of aspirations in the context of health behaviorchange interventions. Indeed, recent analyses from theSmokers’ Health Study (described below) indicated thatan SDT-based intervention helped to sustain intrinsicaspirations at 12 months post-intervention. Further,intrinsic aspirations demonstrated both a mediating anda moderating effect on the intervention such that (a) anSDT-based intervention facilitated a maintained increasein the importance of intrinsic aspirations for healthwhich in turn predicted better tobacco cessation out-comes at 18 months post-intervention; and (b) the SDT-based intervention was particularly effective in promot-ing long-term tobacco cessation amongst those whoplaced greater importance on health aspirations [34].
From Basic Science to Application: SDT and HealthUnlike MI, which was developed in the context of healthbehavior change (i.e., problem drinking [35]), SDT wasdeveloped in the context of basic social science (i.e., the-ory development and testing [14,36,37]). Much of theearly work on SDT focused on the undermining effectsof rewards on intrinsic motivation [e.g., [38-40]], andthe first applications of SDT were geared toward under-standing these processes in education [e.g., [41-43]].Over the past 10-15 years, a growing body of researchhas emerged testing the applicability of SDT to healthcontexts including the healthcare environment, healthbehavior change, and interventions. Together, the find-ings from these studies have demonstrated the role ofneed support and autonomous self-regulation in a vari-ety of mental and physical health outcomes includingdepression, anxiety, somatization, quality of life, tobaccocessation, physical activity, weight loss, diabetes manage-ment, dental health, and medication adherence [20].Below we summarize a few of these studies to highlightthe breadth and depth of findings applying SDT tohealth.
Just as MI arose as a behavior therapy for problemdrinking, one of SDT’s first forays into health behaviorapplication involved a study of individuals mandated toan 8-week alcohol treatment program [44]. Primary out-comes were attendance during the program and clini-cians’ ratings of patient involvement in treatment.Results revealed that individuals who had more autono-mous self-regulation for alcohol treatment evidencedgreater treatment attendance, program completion, andclinician-rated treatment involvement.Williams and colleagues [22] studied individuals
enrolled in a weight loss program for morbidly obesepatients. The 26-week program involved a very low-cal-orie liquid diet for the first 13 weeks, with normal foodsintroduced gradually over the final 13 weeks of treat-ment. Treatment also included once weekly group ses-sions with 12-15 individuals to discuss feelings andchallenges through the weight loss process, facilitatepeer support, and provide techniques for self-monitoringdiet, physical activity, and weight. Primary outcomeswere program attendance and BMI change. Findingsdemonstrated that those with greater autonomous self-regulation for the weight loss program had better pro-gram attendance and greater reductions in BMI. Impor-tantly, autonomous self-regulation for treatmentpredicted long-term BMI change more than one yearafter the end of treatment. Further, this study demon-strated a direct link between patients’ perceptions ofneed support from treatment providers and (1) autono-mous self-regulation for treatment mid-way through theintervention, (2) program attendance, and (3) BMIchange (post-intervention and at long-term follow-up).Autonomous self- regulation for treatment mid-waythrough the intervention was shown to mediate theassociation between perceived need support and treat-ment outcomes, providing the first empirical evidencefor the SDT model of health behavior change wherebythe social context (i.e., need support) predicts motiva-tion (i.e., autonomous self-regulation) which, in turn,predicts health behavior and/or health outcomes.SDT has also been applied to the study of adherence
to long-term and complex medication routines. In anobservational study of 126 patients taking 1 of 30 differ-ent medications for more than two months (mean > 6years), adherence over a 2-week period was stronglyrelated to patients’ autonomous self-regulation for tak-ing that medication, as assessed at the beginning of thestudy. Importantly, patients’ perceptions of need supportfrom their healthcare providers also predicted autono-mous self-regulation for medication-taking and for med-ication adherence [23]. Similar results were found in astudy of 201 HIV+ patients on highly active anti-retro-viral therapies (HAART). HAART medications regimensare particularly complex as they involve taking 3-4
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 5 of 12

medications several times each day. This study alsoincluded perceived competence for medication-takingand demonstrated an expanded model whereby per-ceived need support from health care providers pre-dicted autonomous self-regulation for medication-takingwhich, in turn, predicted perceived competence for tak-ing the medication. Perceived competence was a stron-ger and more proximal predictor of medicationadherence [45]. This model was replicated in a study ofmedication use in a large closed health care systemamong more than 2,000 patients with diabetes, and themotivation variables prospectively predicted medicationuse, glycemic control and healthier cholesterol [46]. Inother research, to the extent that patients with diabetesperceived their health-care provider to be need-suppor-tive, they experienced greater autonomous self-regula-tion which, in turn, predicted perceived competence forboth maintaining a healthy diet and exercising regularly.Perceived need support at Time 1 predicted lower bloodglucose levels over 12 months both directly and indir-ectly through the links between perceived need support,autonomous self-regulation, and perceived competence[47]. Thus, autonomous self-regulation and perceivedcompetence for the prescribed behavior seem to play animportant role in behavior and health outcomes, andpractitioners play an important role in facilitating thesemotivational variables.Recently, researchers have begun developing interven-
tions based on the tenets of SDT and the empirical sup-port for the SDT process model of health behaviorchange from observational research. Here we describe afew of these interventions. Others are discussed else-where in this issue. Some of the earliest developmentsof SDT-based interventions involved tobacco cessation.In one study, 316 patients who smoked were recruitedto have a discussion with their physician about theirsmoking behavior [21]. Physicians were randomlyassigned to work with each patient in either a need-sup-portive or need- thwarting manner (i.e., randomizationwas at the level of patient) and to use the National Can-cer Institute’s 4As model for smoking cessation. Theneed-supportive condition was characterized by elicitingand acknowledging the patient’s perspective, providing arationale for advice given, and minimizing control, whileavoiding judgment. The need-thwarting condition wascharacterized by the physician dominating the conversa-tion, minimizing patient choice, and instructing thepatient on what he or she should do, with no rationaleor reflection. Patient involvement in the discussion wasassessed by independent raters, based on audio tapes ofthe doctor-patient interaction. Patient smoking statuswas assessed at 6 months, 12 months, and 30 monthspost-discussion. Results revealed that observed physicianinteraction style indirectly predicted patient smoking
status through its direct influence on patient involve-ment-a hallmark of autonomous self-regulation. Thisintervention is particularly important because it speaksdirectly to the practical utility of SDT as it was con-ducted in the real-world setting of a community-basedphysician group with physicians and their patients, withwhom they had had ongoing relationships.In the Smokers’ Health Study, participants were 1,006
smokers who smoked at least five cigarettes per day andhad smoked at least 100 cigarettes in their lifetime.Slightly more than half of the participants did not wantto try to stop smoking at the time they enrolled in thestudy. Participants were randomly assigned to either anintensive treatment or community care control. Inten-sive treatment consisted of four contacts over sixmonths. Practitioners were trained to interact with par-ticipants based on the Public Health Service Guidelineintensive tobacco dependence treatment [48] in anSDT-consistent manner, which included: providing needsupport, including supporting the participant’s decisionabout whether to stop or continue smoking; providinginformation about nicotine, tobacco dependence, andtips for successful quitting; exploring barriers and howsmoking related to their values; using shared decision-making to develop a plan; problem-solving and skills-building; and access to pharmacotherapy. The commu-nity care condition consisted of provision of currentpamphlets on stopping smoking and encouragement todiscuss smoking with one’s physician and was consistentwith what was typically prescribed for tobacco cessationin the community at the time [49].Results demonstrated support for the SDT process
model whereby greater perceived need support fromone’s health care providers (including study practi-tioners) predicted greater increases in autonomous self-regulation and perceived competence for stoppingsmoking from baseline to the end of the intervention.Greater increases in autonomous self-regulation andperceived competence for stopping smoking predictedbetter tobacco abstinence 12 months after the end ofthe intervention, both in terms of 7-day point preva-lence and prolonged abstinence. It is worth noting thatautonomous self-regulation influenced tobacco absti-nence indirectly through its impact on use of smokingcessation medications. This model was invariant acrossthe intervention and community care groups, suggestingthat internalization is at least, in part, a naturally-occur-ring process. However, it is important to note that thosein the intervention group, compared to those in com-munity care, evidenced greater perceived need support,greater changes in autonomous self-regulation and per-ceived competence for stopping smoking, greater medi-cation usage, and higher abstinence rates. Thus,although the process of internalization appears to be a
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 6 of 12

process that occurs naturally in the course of behaviorchange, this study demonstrated that the process can beaccelerated through a need-supportive, SDT-based inter-vention [12]. Importantly, tobacco abstinence was main-tained 24 months post-intervention more so for those inthe intervention group compared to community care[50]. Thus, there is some initial evidence that SDT-based interventions not only facilitate health behaviorchange, but, importantly its maintenance. Further,change in autonomous self-regulation during treatmentdirectly predicted 7-day abstinence 24 months post-intervention and indirectly predicted change in pro-longed abstinence 24 months post- intervention. Thissuggests that the change in autonomy during treatmentcontinued to motivate new efforts at abstinence wellafter the intervention was over.SDT-based interventions have also been developed for
dental behaviors and oral health [10]. Participants were86 individuals in a dental clinic randomly assigned toeither the SDT intervention or a usual care controlgroup. All participants completed baseline question-naires to assess autonomous self- regulation and per-ceived competence for dental care and were providedwith a routine dental cleaning. One month following thedental cleaning, participants in the intervention groupparticipated in a 60- minute informational session aboutdental health conducted by a dental hygienist. Theinformational session was designed to be consistent withthe principles of SDT including acknowledging patientperspectives and feelings about dental health concerns,providing a rationale for dental prophylaxis, and provid-ing choices and options for preventive behaviors thatpatients could choose to adopt. The dental hygienistalso provided competence-support for intervention par-ticipants by demonstrating proper brushing and flossingtechniques, allowing participants to practice these dentalhealth behaviors, and conveying confidence in partici-pants’ ability to maintain these behaviors over time. Sixmonths after the routine dental cleaning, all participantsreturned for an assessment of their oral health (plaqueand gingivitis) and to complete follow-up questionnairesassessing autonomous self-regulation and perceivedcompetence for dental care, self-reported dental beha-viors, and attitudes and affect toward dental care. Com-pared to those in the usual care control, those in theSDT intervention group evidenced greater increases inautonomous self-regulation and perceived competencefor dental care, decreases in plaque and gingivitis, betterself-reported dental behaviors, and more positive atti-tudes and affect toward dental care. Importantly, furthersupport for the SDT process model of health behaviorchange was provided by this study on dental health. Per-ceived need support of dental health providers predictedgreater increases in autonomous self-regulation and
perceived competence for dental care, which in turnpredicted better dental health behaviors and outcomes(i.e., plaque, gingivitis).In addition to these interventions developed for
tobacco cessation and oral health, there has been aflurry of recent research activities involving SDT-basedinterventions for weight loss, physical activity, and diet-ary change. Although previous research has examinedSDT variables in the context of traditional medicalweight loss interventions [22], this recent research activ-ity has used the tenets of SDT to inform the develop-ment of interventions for weight loss, physical activity,and diet. For example, in a study of patients in a com-munity-based primary care practice, participants whoworked with an SDT-trained physical activity counselorexperienced greater need support in the health care cli-mate which predicted greater increases in autonomousself-regulation for physical activity and, in turn,increases in perceived competence for physical activity.Both autonomous self-regulation and perceived compe-tence for physical activity predicted greater increases inphysical activity behavior [9]. In a one- year, SDT-basedintensive behavioral intervention for weight loss amongoverweight and obese women, weight loss was greaterfor women in the intervention compared to the controlat the end of the intervention and at 1 year post-inter-vention [11,51]. The intervention explicitly targetedincreasing exercise autonomous self-regulation andintrinsic motivation, namely enjoyment of physical activ-ity. The effect of the intervention on autonomous self-regulation was notable because it was large, it was sus-tained over one year, and it mediated the effect of theintervention on physical activity at 1 and 2 years [52].Further evidence from this study has suggested a “moti-vational spill-over” whereby autonomous self-regulationfor exercise predicted later autonomous self-regulationfor healthy eating over one year [53]. Thus, facilitatingautonomous self-regulation in one health domain mayincrease autonomous self-regulation in other, relateddomains. Additional details on each of these studies-andother related studies-are provided elsewhere in thisissue.Considered together, these randomized controlled
trials demonstrate that SDT based interventions effectchange in several health behaviors that are maintainedafter a free choice period (tobacco abstinence, physicalactivity, dental health, and weight loss). These tests ofSDT interventions demonstrate mediation by key SDTconstructs, thus linking SDT with these interventions’effect on important health behaviors through change inautonomous self-regulation and perceived competence.These studies conducted by several investigators in dif-ferent countries (all western cultures) support a causalrole of change in autonomous self-regulation, and
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 7 of 12

perceived competence in the process of health behaviorchange.
SDT and MI: Overlap and DistinctionsWhile SDT and MI have developed independently andhave been utilized by relatively independent sets ofresearchers, recent attention has been given to the com-plementarity of these perspectives [e.g., [5,6]], includingthe MI-SDT Satellite Meeting held in Sintra, followingthe 2009 Annual Meeting of the International Societyfor Behavioral Nutrition and Physical Activity. It isworth noting that, in this section, we are consideringthe similarities and distinctions between SDT and MIthrough the lens of SDT researchers. Thus, it is possible(indeed, likely!) that those who view these two perspec-tives through the MI lens may see somewhat differentsimilarities and distinctions [cf 7]. We hope that thepoints outlined below will facilitate further discussion,debate, and, perhaps most importantly, empirical inves-tigation about how these two perspectives may comple-ment and enhance each other and the science of healthbehavior more broadly.Miller [54] has described MI as being based on con-
cepts such as causal attributions, cognitive dissonance,and self-efficacy-all of which are grounded in social psy-chological theories and various social cognitiveapproaches. However, MI has been criticized for beinglargely atheoretical [55]. This lack of an organizing theo-retical framework precludes explanations for how andwhy MI can be effective [56-58], although recent effortshave been made toward the development of an emer-gent theory of MI [13]. This is perhaps the most notabledistinction between MI and SDT: SDT is a theory, whileMI is a set of techniques (for further discussion of thisdistinction, see [8]). And although an advantage to SDTis that it offers a theoretical basis from which to under-stand the mechanisms through which SDT-based inter-ventions are efficacious, a challenge to SDT researchershas been to translate theoretical concepts of need-sup-portive contexts into clinical techniques used in inter-ventions. Thus, because of the consistency between MItechniques and SDT need support, many SDT-basedinterventions have been informed by MI techniques [e.g., [12,19]]. Importantly, SDT and MI have both drawnon Rogerian perspectives (e.g., unconditional positiveregard, and patient centeredness [59,60]) and thus manyof the underlying assumptions of both approaches aresimilar.One of the areas in which much debate has ensued
between SDT and MI researchers is around the area ofdirectiveness. Although Miller and Rollnick [61] defineMI as both client-centered and directive, MI is also veryclear that attempts to directly persuade a client are inef-fective in dealing with the client’s ambivalence because
such persuasive attempts inherently “take sides” in theambivalence. In contrast, SDT has maintained, in thepractice of healthcare interventions, that patient auton-omy may be supported, in part, by making explicitrecommendations about health and well-being (cf 12,49). Further, in medical contexts in particular, explicitrecommendations are often an expected component ofinteractions between practitioners and patients, and apractitioners’ refusal to provide such direction-in addi-tion to its potential for being unethical-does not supportthe patient ’s psychological needs. To illustrate, if apatient asks for a recommendation about treatment fora heart attack, the patient would likely feel a high levelof control (e.g., thwarting of need for autonomy) andabandonment (thwarting of need for relatedness), forthe doctor to insist the patient choose the treatmentwithout a recommendation. Within SDT, recommenda-tions must be given after eliciting and acknowledgingclient perspectives, non-coercively and in an autonomy-supportive way. When provided in this manner, therecommendation is more likely to be experienced by thepatient as being informational, as opposed to coercive,and thus supports the patient in making the decisionhimself or herself (e.g., “I believe that stopping smokingis the best thing for your health, but only you candecide if you are going to smoke or not. The choice isultimately yours, and I am here to support you in what-ever decision you make.”). More recent formulations ofMI have allowed for medical practitioners to makerecommendations when patients specifically ask foradvice and have encouraged directiveness in the case ofprovoking change talk [13]. It is also possible that, aswith the case of intrinsic motivation (described below),these two perspectives have defined “directive” in some-what different ways.Another distinction between MI and SDT is around
the use of the term “intrinsic motivation.” MI maintainsthat a primary goal of the techniques employed in MIinterventions is to enhance intrinsic motivation [e.g.,[61]]. However, SDT and other motivational theories [e.g., [62,63]] have defined intrinsic motivation as engagingin an activity for its own sake, because it is inherentlyenjoyable, satisfying or challenging. Given this definition,it seems likely that, rather than enhancing intrinsicmotivation, MI techniques facilitate the process of inter-nalization of extrinsic motivations (see [6] for a moredetailed discussion of this point). This issue is largelyone of semantics and may be one area in which SDTmay serve to refine and enhance MI.Despite these differences, there is actually a good deal
of conceptual overlap and similarity between SDT andMI. Perhaps most noteworthy is that both SDT and MIstart with the same basic assumption: That humans arenaturally oriented toward growth, health and well-being.
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 8 of 12

Additionally, both identify and work with-rather thanattempt to combat-patient’s ambivalence toward change.Further, MI techniques are at least partially consistentwith SDT’s notion of need support. Although tradition-ally, SDT has spoken primarily to the issue of autonomysupport, the way in which perceptions of autonomy sup-port have traditionally been measured (i.e., HCCQ [e.g.,[17,21,22]]) and the nature of SDT-based interventionsreally address all three psychological needs. Indeed, per-ceived competence is facilitated by autonomous self-reg-ulation, which arises out of need-supportive contexts [e.g., [20]]. Once individuals have a high willingness to act,they are more likely to learn new knowledge and applynew strategies that result in greater perceived compe-tence. SDT predicts that perceived competence alone isnot sufficient to motivate behavior; it must be accompa-nied by autonomy. This is in contradistinction to SocialCognitive Theory [64] which places nearly exclusiveemphasis on self-efficacy.As mentioned previously, MI techniques have
informed some of the SDT interventions to date [e.g.,[9,11,12]]. These SDT-based interventions are discussedin greater detail elsewhere in this issue [cf 64]. MI ori-ginally identified four key principles consistent with thepractice of MI techniques: use of an empathic interper-sonal style, development of discrepancy, rolling withresistance, and supporting self- efficacy for change[62,65]. More recent conceptualizations of MI applica-tions to health care contexts have used somewhat differ-ent terminology, though the spirit of MI remains muchthe same [66]. Here we provide a brief overview of thecurrent conceptualization of MI’s four guiding principles(RULE = Resist the righting reflex, Understand andexplore the patient’s motivations, Listen to the patientempathically, Empower the patient) and three core com-munication skills (ask, listen, inform). We also discusshow these elements of MI are consistent with the sup-port of psychological needs identified by SDT and thus,may support the process of internalization more broadly.MI recognizes the natural tendency for those in the
helping professions-particularly those in health care set-tings-to want to try to “fix” whatever is wrong with theirpatients or clients. However, MI also notes that resis-tance can arise when patients feel that their practitioneris trying to convince them of a particular course ofaction. This may be particularly pronounced in situa-tions in which the individual feels ambivalent aboutchange. Thus, it is critical that practitioners resist therighting reflex and instead allow clients to explore bothsides of their ambivalence so that, in the end, the clientis the one giving voice to reasons for change [66]. Thisguiding principle is similar to what SDT describes asminimizing control and remaining nonjudgmental. Thismay support clients’ needs for both autonomy and
relatedness by allowing patients the freedom to explorereasons for or against change (autonomy) in a non-judg-mental context (relatedness).Like SDT, from the perspective of MI, it is critical for
patients to experience themselves as the originators oftheir actions toward behavior change. Thus, practi-tioners need to understand and explore the patient’smotivations. This includes exploring how the patientviews their current behavior and situation, concernsabout change, and other goals and values [66]. Thisguiding principle of MI is consistent with SDT auton-omy support, particularly eliciting and acknowledgingclient perspectives and emotions, supporting clientinitiative, and assessing values.One of the defining features of MI is its emphasis on
listening to the patient empathically. Thus, MI placesimportance on listening over informing on the part ofpractitioners, and an empathic interpersonal style,including an authentic interest in understanding the cli-ent [61,65,66]. According to MI, the client must feelpersonally accepted and valued before behavior changeis possible. Listening to a patient empathically likelysupports the client’s need for relatedness and reflectsthat both MI and SDT emerged from the Rogerianschool of thought, which promotes unconditional posi-tive regard and patient centeredness as paramount tothe therapeutic relationship [60]. Finally, the fourthguiding principle of MI-empower the patient - involvessupporting self-efficacy for change. This technique likelyprimarily supports clients’ need for competence byenhancing their confidence in being able to make pro-gress toward positive change and to cope with chal-lenges and barriers as they arise.In addition to these four guiding principles, MI
researchers have also articulated three core communica-tion skills that provide practical utility to these princi-ples. These communication skills include asking,listening, and informing. The purpose of asking is to eli-cit the client’s perspective so that the practitionerunderstands where the patient is coming from and howthe patient approaches the possibility of behaviorchange. Listening is an active process whereby the prac-titioner “checks in” with the client to ensure that he orshe has an accurate understanding of client’s perspec-tive, motivations, and struggles through the process ofbehavior change. Finally, informing is the primary meansby which practitioners convey knowledge to a clientabout their health condition, the behavior changesnecessary to monitor or improve the health condition,and treatment options that may be available.
Directions for the FutureAlthough SDT and MI originally began on two distinctpaths, it seems clear from this special issue, the meeting
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 9 of 12

in Sintra, and previous publications elsewhere [e.g.,[5,6,67,68]] that there is now a critical mass of research-ers engaged in dialogue about the similarities and dis-tinctions between SDT and MI. However, it isimportant that this endeavor not stagnate with discus-sion and debate. Indeed, the next steps in this processof bringing together this theory and these clinical tech-niques must be borne out empirically. SDT has not yetidentified the critical components for supporting psy-chological needs and facilitating autonomous self-regula-tion and perceived competence in health behaviorinterventions. MI techniques and their assessments maybe useful additions to current SDT interventions ininforming this empirical avenue.Some MI interventions have included SDT measures
[e.g., [69,70]], and this is an important step towardempirically testing the similarities between the twoapproaches. However, to date, results on whether MIinterventions facilitate change in autonomous self-regu-lation, in particular, have been somewhat mixed, thoughsome research has found that autonomous self-regula-tion mediates the association between MI interventionand treatment outcome [71]. Additional research isneeded to identify which principles of MI operate onneed support and the process of internalization. Further,current measures from SDT may need to be refined tobetter capture all three dimensions of perceived needsupport and to more accurately assess fluctuations inautonomous self-regulation and perceived competencein the initial stages of behavior change as well as beha-vior maintenance. In addition, assessment techniques,advanced analytic methods (growth curve analysis andlatent trajectory modeling) and the use of internet tech-nology and mobile devices in ecological momentarysampling may also improve researchers’ ability to detectchanges in motivation in response to provision of speci-fic components of need support.Finally, future research in which MI and SDT-based
interventions are directly compared are needed to (1)more clearly elucidate the extent to which SDT canexplain how and why MI interventions effect behavior,(2) identify aspects of SDT-based interventions that aresimilar to and distinct from MI (e.g., MI coding of SDTinterventions and vice versa), (3) determine if MI inter-ventions facilitate change in both autonomous self-regu-lation and perceived competence and support the needfor relatedness, and (4) better clarify how bothapproaches can be used in concert to yield the mostpositive results. These empirical endeavors require notonly a bridging of ideas but, perhaps more importantly,the convergence of a multi-conceptual team with repre-sentation from both SDT and MI camps to refine MItechniques, to improve SDT applications to health beha-vior, and to further expand our understanding of these
approaches and how they serve to facilitate the initiationand maintenance of health behavior change.Miller and Rose [13] recently published a statement
on a theory for MI. Although SDT was not mentioneddirectly in that publication, SDT researchers mayfacilitate linking SDT to MI through empirical studyof how eliciting change talk is experienced by clients(i.e., as relatively more or less need-supportive) andthe extent to which change talk reflects a shift inpatients’ perceived locus of causality and/or change inautonomous self-regulation. From the SDT perspec-tive, change talk is a reflection of the client or patientshifting from a voice of external locus of causality tointernal -literally reflecting “real time” internalization.However, it is not clear that this is precisely how MIviews change talk. Miller and Rose [13] and othershave placed strong emphasis on practitioners activelypromoting and eliciting change talk. This may besomewhat inconsistent with SDT. The aggressive pushtoward change talk may reflect an underlying assump-tion that the person is better off changing (when infact this may not be their goal). Pushing change talkmay be experienced as coercive and judgmental, andthus is not need-supportive. Self-determination theor-ists will also need to carefully consider whether MI’sstatement of theory is consistent with SDT. Particu-larly important for SDT theorists and researchers willbe the resolution of issues such as MI’s conceptualiza-tion of intrinsic motivation, the role of directiveness,and the issue of development of discrepancy. Thoughthe latter is not explicitly listed in current conceptua-lizations of MI ’s guiding principles, the extent towhich development of discrepancy is key to the execu-tion of MI interventions may be important particularlywith respect to whether this aspect of MI supports orthwarts need satisfaction.
ConclusionsBy bringing together the strengths of both approaches,we may be better equipped to develop efficacious inter-ventions that yield positive results for health, healthbehavior, and well-being not only amongst the highlymotivated participant pool willing to enroll in clinicaltrials but also among more general patient populationswith whom practitioners interact on a daily basis. Onlyby facilitating the development of practical interventionswith long-lasting effects will we succeed in improvinglength and quality of life through lifestyle change. Theopportunity at hand may be to identify SDT and MI ascomplementary approaches. Collaborative effortsbetween complementary approaches will foster thedevelopment of a rigorous science of health behaviorchange that is equipped to tackle these issues in the realworld of health care practice.
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 10 of 12

Author details1Division of Cancer Control and Population Sciences National CancerInstitute 6130 Executive Boulevard Rockville, MD 20852-7335 USA.2Department of Medicine and of Clinical and Social Psychology University ofRochester 46 Prince Street Rochester, NY 14607 USA.
Authors’ contributionsHP and GWC discussed the format and scope of the manuscript. HP wrotethe initial draft of the manuscript, and GWC contributed to the writing ofthe manuscript. All authors read and approved the final manuscript.
Competing interestsThe authors declare that they have no competing interests.
Received: 14 July 2010 Accepted: 2 March 2012Published: 2 March 2012
References1. Schroeder SA: We can do better-Improving the health of the American
people. New England Journal of Medicine 2007, 357:1221-1228.2. Woolf SH: The power of prevention and what it requires. Journal of the
American Medical Association 2008, 299:2437-2439.3. Chiuve SE, McCullough ML, Sacks FM, Rimm EB: Healthy lifestyle factors in
the primary prevention of coronary heart disease among men: Benefitsamong users and nonusers of lipid lowering and anti hypertensivemedications. Circulation 2006, 114(2):160-167.
4. Kushi LH, Byers T, Doyle C, Bandera EV, McCullough M, Gansler T,Andrews KS, Thun MJ, American Cancer Society: American Cancer SocietyGuidelines on nutrition and physical activity for cancer prevention:Reducing the risk of cancer with healthy food choices and physicalactivity. CA: A Cancer Journal for Clinicians 2006, 56:254-281.
5. Markland D, Ryan RM, Tobin VJ, Rollnick S: Motivational interviewing andself-determination theory. Journal of Social and Clinical Psychology 2005,24:811-831.
6. Vansteenkiste M, Sheldon KM: There’s nothing more practical than a goodtheory: Integrating motivational interviewing and self-determinationtheory. British Journal of Clinical Psychology 2006, 45:63-82.
7. Resnicow K, McMaster F: Motivational interviewing: Moving from why tohow with autonomy support. International Journal of Behavioral Nutritionand Physical Activity 2011, this issue.
8. Vansteenkiste M, & Williams GC: Self-determination theory andmotivational interviewing as examples of development from a meta-theory (top-down) vs. from clinical experience up (bottom-up):Implications for theory development, research and clinical practice andinterventions. International Journal of Behavioral Nutrition and PhysicalActivity 2011, this issue.
9. Fortier MS, Sweet SN, O’Sullivan TL, Williams GC: A self-determinationprocess model of physical activity adoption in the context of arandomized controlled trial. Psychology of Sport and Exercise 2007,8:741-757.
10. Münster Halvari AE, Halvari H: Motivational predictors of change in oralhealth: An experimental test of self-determination theory. Motivation andEmotion 2006, 30:294-305.
11. Silva MN, Markland D, Minderico CS, Vieira PN, Castro MM, Coutinho SR,Santos TC, Matos MG, Teixeira PJ: A randomized controlled trial toevaluate self-determination theory for exercise adherence and weightcontrol: rationale and intervention description. BMC Public Health 2008,8:234.
12. Williams GC, McGregor H, Sharp D, Levesque CS, Kouides RW, Ryan RM,Deci EL: Testing a self- determination theory intervention for motivatingtobacco cessation: Supporting autonomy and competence in a clinicaltrial. Health Psychology 2006, 25:91-101.
13. Miller WR, Rose GS: Toward a Theory of Motivational Interviewing.American Psychologist 2009, 64:27-537.
14. Deci EL, Ryan RM: Intrinsic motivation and self-determination in humanbehavior New York: Plenum Publishing Co.; 1985.
15. Deci EL, Ryan RM: The ‘what’ and ‘why’ of goal pursuits: Human needsand the self-determination of behavior. Psychological Inquiry 2000,11:227-268.
16. Ryan RM: Psychological needs and the facilitation of integrativeprocesses. Journal of Personality 1995, 63:397-427.
17. Williams GC, Deci EL, Ryan RM: Building health-care partnerships bysupporting autonomy: Promoting maintained behavior change andpositive health outcomes. In Partnerships in healthcare: Transformingrelational process. Edited by: Suchman AL, Hinton-Walker P, Botelho R.Rochester, NY: University Of Rochester Press; 1998:67-87.
18. Ryan RM, Connell JP: Perceived locus of causality and internalization:Examining reasons for acting in two domains. Journal of Personality andSocial Psychology 1989, 57:749-761.
19. Ryan RM, Deci EL: Self-determination theory and the facilitation ofintrinsic motivation, social development, and well-being. AmericanPsychologist 2000, 55:68-78.
20. Ryan RM, Patrick H, Deci EL, Williams GC: Facilitating health behaviourchange and its maintenance: Interventions based on self-determinationtheory. The European Health Psychologist 2008, 10:2-5.
21. Williams GC, Deci EL: Activating patients for smoking cessation throughphysician autonomy support. Medical Care 2001, 39:813-823.
22. Williams GC, Grow VM, Freedman ZR, Ryan RM, Deci EL: Motivationalpredictors of weight loss and weight-loss maintenance. Journal ofPersonality and Social Psychology 1996, 70:115-126.
23. Williams GC, Rodin GC, Ryan RM, Grolnick WS, Deci EL: Autonomousregulation and adherence to long-term medical regimens in adultoutpatients. Health Psychology 1998, 17:269-276.
24. Beauchamp TL, Childress JF: Principles of biomedical ethics NewYork, NY:Oxford University Press; 2001.
25. Schneider K: Existential processes. In Handbook of experientialpsychotherapy. Edited by: Greenberg L, Watson J, Lietaer G. New York:Guilford; 1998:103-120.
26. European Federation of Internal Medicine ABIM Foundation: MedicalProfessionalism in the new millennium: A physician charter. Annals ofInternal Medicine 2002, 136:243-246.
27. Woolf SH, Chan ECY, Harris R, Sheridan SL, Braddock CH, Kaplan RM, Krist A,O’Connor AM, Tunis S: Promoting informed choice: Transforming healthcare to dispense knowledge for decision making. Annals of InternalMedicine 2005, 143(4):293-300.
28. Braddock CH, Edwards KA, Hasenberg NM, Laidley TL, Levinson W:Informed decision making in outpatient practice: Time to get back tobasics. Journal of the American Medical Association 1999, 282(24):2313-2320.
29. Kasser T, Ryan RM: A dark side of the american dream: Correlates offinancial success as a central life aspiration. Journal of Personality andSocial Psychology 1995, 65:410-422.
30. Kasser T, Ryan RM: Further examining the american dream: Differentialcorrelates of intrinsic and extrinsic goals. Personality and Social PsychologyBulletin 1996, 22:280-287.
31. Grouzet FM, Kasser T, Ahuvia A, Dols JMF, Kim Y, Lau S, Ryan RM,Saunders S, Schmuck P, Sheldon KM: The structure of goals across 15cultures. Journal of Personality and Social Psychology 2005, 89:800-816.
32. Williams GC, Cox EM, Hedberg V, Deci EL: Extrinsic life goals and healthrisk behaviors in adolescents. Journal of Applied Social Psychology 2000,30:1756-1771.
33. Weinstein N, Przybylski AK, Ryan RM: Can nature make us more caring?effects of immersion in nature on intrinsic aspirations and generosity.Personality and Social Psychology Bulletin 2009, 35:1315-1329.
34. Niemiec CP, Ryan RM, Deci EL, Williams GC: Aspiring to physical health:The role of aspirations for physical health in facilitating long-termtobacco abstinence. Patient Education and Counseling 2009, 74:250-257.
35. Miller WR, Taylor CA, West JC: Focused versus broad spectrum behaviortherapy for problem drinkers. Journal of Consulting and Clinical Psychology1980, 48:590-591.
36. Deci EL: The psychology of self-determination Lexington, MA: D. C. Heath(Lexington Books); 1980.
37. Deci EL, Koestner R, Ryan RM: The undermining effect is a reality after all:Extrinsic rewards, task interest, and self-determination. PsychologicalBulletin 1999, 125:692-700.
38. Deci EL: Effects of externally mediated rewards on intrinsic motivation.Journal of Personality and Social Psychology 1971, 18:105-115.
39. Deci EL: Intrinsic motivation, extrinsic reinforcement, and inequity.Journal of Personality and Social Psychology 1972, 22:113-120.
40. Deci EL, Ryan RM: The empirical exploration of intrinsic motivationalprocesses. In Advances in experimental social psychology. Edited by:Berkowitz L. New York: Academic Press; 1980:39-80.
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 11 of 12

41. Flink C, Boggiano AK, Barrett M: Controlling teaching strategies:Undermining children’s self- determination and performance. Journal ofPersonality and Social Psychology 1990, 59(5):916-924.
42. Skinner EA, Belmont MJ: Motivation in the classroom: Reciprocal effectsof teacher behavior and student engagement across the school year.Journal of Educational Psychology 1993, 85:571-581.
43. Valas H, Sovik N: Variables affecting students’ intrinsic motivation forschool mathematics: Two empirical studies based on Deci and Ryan’stheory of motivation. Learning and Instruction 1994, 3:281-298.
44. Ryan RM, Plant RW, O’Malley S: Initial motivations for alcohol treatment:Relations with patient characteristics, treatment involvement anddropout. Addictive Behaviors 1995, 20:279-297.
45. Kennedy S, Goggin K, Nollen N: Adherence to HIV medications: Utility ofthe theory of self- determination. Cognitive Therapy and Research 2004,28(5):611-628.
46. Williams GC, Patrick H, Niemiec CP, Williams LK, Devine G, Lafata JE,Heisler M, Tunceli K, Pladevall M: Reducing the health risks of diabetes:How self-determination theory may help improve medication adherenceand quality of life. Diabetes Educator 2009, 35:484-492.
47. Williams GC, Freedman ZR, Deci EL: Supporting autonomy to motivateglucose control in patients with diabetes. Diabetes Care 1998,21:1644-1651.
48. Fiore MC, Bailey WC, Cohen SJ, Dorfman SF, Goldstein MG, Gritz ER,Heyman RB, Jaén CR, Kottke TE, Lando HA, Mecklenburg RE, Mullen PD,Nett LM, Robinson L, Stitzer ML, Tommasello AC, Villejo L, Wewers ME:Treating Tobacco Use and Dependence Rockville, MD: U.S. Department ofHealth and Human Services. Public Health Service; 2000, Clinical PracticeGuideline.
49. Williams GC, McGregor H, Sharp D, Kouides RW, Levesque CS, Ryan RM,Deci EL: A self- determination multiple risk intervention trial to improvesmokers’ health. Journal of General Internal Medicine 2006, 21:1288-1294.
50. Williams GC, Niemiec CP, Patrick H, Ryan RM, Deci EL: The importance ofsupporting autonomy and perceived competence in facilitating long-term tobacco abstinence. Annals of Behavioral Medicine 2009, 37(3):315.
51. Teixeira PJ, Silva MN, Coutinho SR, Palmeira AL, Mata J, Vieira PN,Carraça EV, Santos TC, Sardinha LB: Mediators of weight loss and weightloss maintenance in middle-aged women. Obesity 2009, 281:1-11.
52. Silva MN, Markland D, Vieira PN, Coutinho SR, Carraça EV, Palmeira AL,Minderico CS, Matos MG, Sardinha LB, Teixeira PJ: Helping OverweightWomen Become More Active: Need Support and MotivationalRegulations for Different Forms of Physical Activity. Psychology of Sportand Exercise 2010, 11:591-601.
53. Mata J, Silva MN, Vieira Pn N, Carraca EV, Andrade AM, Coutinho SR,Sardinha LB, Teixeira PJ: Motivational “spill-over” during weight control:Increased self-determination and exercise intrinsic motivation predicteating self-regulation. Health Psychology 2009, 28:709-716.
54. Miller WR: Motivational interviewing with problem drinkers. BehavioralPsychotherapy 1983, 11:147-172.
55. Draycott S, Dabbs A: Cognitive dissonance 1: An overview of theliterature and its integration into theory and practice in clinicalpsychology. British Journal of Clinical Psychology 1998, 37:341-353.
56. Miller WR: Motivational interviewing: III. On the ethics of motivationalintervention. Behavioural and Cognitive Psychotherapy 1994, 22:111-123.
57. Miller WR: Motivational interviewing: Research, practice, and puzzles.Addictive Behaviors 1996, 21:835-842.
58. In Enhancing motivation for change in substance abuse treatment. Editedby: Miller WR. Rockville, MD: Center for Substance Abuse Treatment; 1999:,Treatment Improvement Protocol (TIP) Series, No. 35.
59. Patterson TG, Joseph S: Development of a self-report measure ofunconditional positive self- regard. Psychol Psychotherapy 2007, 79:557-70.
60. Rogers C: On Becoming a Person: A Therapist’s View of PsychotherapyLondon: Constable; 1961.
61. Miller WR, Rollnick S: Motivational Interviewing. 2 edition. New York: TheGuilford Press; 2002.
62. Csikszentmihalyi M: Finding flow: The psychology of engagement witheveryday life Basic Books; 1997.
63. Lepper MR, Green D, Nisbett R: Undermining children’s intrinsic interestwith extrinsic rewards: A test of the overjustification hypothesis. Journalof Personality and Social Psychology 1973, 28:129-137.
64. Bandura A: Perceived self-efficacy in the exercise of personal agency.Psychologist 1989, 2:411-24.
65. Miller WR, Rollnick S: Motivational interviewing: Preparing people tochange addictive behavior. New York: Guilford Press; 1991.
66. Rollnick S, Miller WR, Butler CC: Motivational Interviewing in Health Care:Helping Patients Change Behavior The Guilford Press. New York, New York;2008.
67. Foote J, DeLuca A, Magura S, Warner A, Grand A, Rosenblum A, Stahl S: Agroup motivational treatment for chemical dependency. Journal ofSubstance Abuse Treatment 1999, 17:181-192.
68. Ginsburg JI, Mann RE, Rotgers F, Weekes JR: Motivational interviewingwith criminal justice populations. In Motivational Interviewing. Edited by:Miller WR, Rollnick S. New York: The Guilford Press; 2002:333-346.
69. Resnicow K, Jackson A, Blissett D: Results of the Health Body HealthySpirit Trial. Health Psychology 2005, 24:339-348.
70. Rubak S, Sandbaek A, Lauritzen T, Borch-Johnsen K, Christensen B: Generalpractitioners trained in motivational interviewing can positively affectthe attitude to behaviour change in people with type 2 diabetes. Oneyear follow-up of an RCT, ADDITION Denmark. Scandinavian Journal ofPrimary Health Care 2009, 27(3):172-179.
71. Fuemmeler BF, Mâsse LC, Yaroch AL, Resnicow K, Campbell MK, Carr C,Wang T, Williams A: Psychosocial mediation of fruit and vegetableconsumption in the body and soul effectiveness trial. Health Psychology2006, 25:474-483.
doi:10.1186/1479-5868-9-18Cite this article as: Patrick and Williams: Self-determination theory: itsapplication to health behavior and complementarity with motivationalinterviewing. International Journal of Behavioral Nutrition and PhysicalActivity 2012 9:18.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Patrick and Williams International Journal of Behavioral Nutrition and Physical Activity 2012, 9:18http://www.ijbnpa.org/content/9/1/18
Page 12 of 12