Embed Size (px)
Citation preview

Injury, Int. J. Care Injured 33 (2002) 635–638
Case report
Self inflicted neck injury with an electric drill
D. Barnes∗, F. Clark, P. Baguley, N. Brady37 St David’s Grove, Ingleby Barwick, Stockton-on Tees TS17 5HE, UK
Accepted 30 August 2001
1. Introduction
Although penetrating injuries to the neck are increasinglycommonplace the literature only describes one other sui-cide attempt by electric drill [1]. We report the subsequentmanagement of this patient and emphasise the need for ad-equate cervical spine stabilisation in high-energy trauma tothe neck.
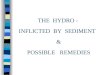
Fig. 1. Sagital T2-weighted MRI scan showing intramedullary high signal at C6 consistent with cord contusion/evolving myelomalcia. Note, the increasedsignal in the C6 vertebral body consistent with marrow oedema along the course of the drill.
∗ Corresponding author.E-mail address: [email protected] (D. Barnes).
2. Case report
A 45-year-old man was brought by ambulance to the Ac-cident and Emergency fully conscious, shocked, with a par-tially compromised airway and obvious neurological deficitafter repeatedly drilling his neck. Full cervical immobilisa-tion was already in place and the man underwent a surgicaltracheotomy under local anaesthetic to secure the airway.
0020-1383/02/$ – see front matter © 2002 Elsevier Science Ltd. All rights reserved.PII: S0020-1383(01)00170-X

636 D. Barnes et al. / Injury, Int. J. Care Injured 33 (2002) 635–638
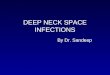
Fig. 2. (a) Axial CT on a bone winding algorithm showing the drill path through the right half of the body of C6 extending to the lamina with boreshards within the spinal cord. (b) A second path is shown on the left side 4 mm lower down on C6. Note, the bilateral facet subluxation. (c) A thirdpath on the left side is shown transversing the foramen transversarium.

D. Barnes et al. / Injury, Int. J. Care Injured 33 (2002) 635–638 637
Fig. 2. (Continued ).
He was sedated, ventilated and an MRI scan was per-formed, which showed extensive soft tissue damage withoedema around the spinal cord at C6/17 (Fig. 1). He wastransferred to the nearest neurosurgical centre where CTscan (Fig. 2a–c) showed that the cervical fracture wasunstable and raised the likelihood of vertebral artery dam-age. Angiography confirmed the presence of complete leftvertebral artery occlusion (Fig. 3). The possibility of oe-sophageal injury combined with the amount of necrotictissue led to a substantial risk of infection. The neck wastherefore not fixed internally but following a repeat MRIscan halo traction was applied and sedation could bediscontinued.
His wound (which essentially was a third degree burnsecondary to the friction of the drill bit and chuck) was ex-plored. This showed at least three distinct pathways includ-ing one passing through the cricothyroid membrane into thesubglottis and another just missing the great vessels on theright.
Once debrided the defect was then closed by a PectoralisMajor myocutaneous rotational flap to the neck and skingrafting.
Oesophageal injury was excluded with a barium swal-low once the man was awake. Neurological deficit includedsubstantial weakness of his right leg with decreased ex-tension of both arms, which improved over the followingweeks.
3. Discussion
ATLS protocol teaches us that airway and cervical spinecontrol go hand in hand. On arrival of the paramedics, thegentleman’s airway was documented as being partially ob-structed, the extensive soft tissue swelling leading to upperairway compromise. However in-drawing of air throughone of the drill holes led to adequate oxygenation, he hadunwittingly performed his own cricothyroidotomy. It isfortunate that cervical spine immobilisation was instigatedimmediately as his fractured cervical spine was unstable,however the need for cervical collars in penetrating in-juries is controversial with some authors suggesting thatlife-threatening injuries may be masked by the stabilisationdevice [2]. Inline manual stabilisation of the neck and logrolling allows full examination of the neck if there is apenetrating wound. The cervical collar also provides a di-rect means of applying pressure to a bleeding area whilstallowing immobilisation for transport.
Finally, case reports describe fatal outcomes from bi-lateral or dominant vertebral artery occlusion followingcervical spine trauma [3]. Angiography is therefore nec-essary to identify occult vascular injuries, contra lateralpatency and if necessary to embolise the vessel [4]. He wasextremely lucky therefore that the heat of the drill cau-terised his artery hence saving him from considerable bloodloss.

638 D. Barnes et al. / Injury, Int. J. Care Injured 33 (2002) 635–638
Fig. 3. Left vertebral artery injection at angiography. Early arterial phase shows occlusion of the vertebral artery at the level of the C6 foramentransversarium.
References
[1] Navarro JA, Mir Marin MA, Aso Escario J, Chastellano Arroys M.A report of a suicide by means of an electric drill. Acta Med LegSoc (Leige) 1989;39(2):247–9.
[2] Barkana Y, Stein M, Scope A, Maor R, Abramovich Y,Friedman Z, Knoller N. Prehospital stabilisation of the cervicalspine for penetrating injuries of the neck—is it necessary?
Surgeon general headquarters, Medical Corps, Israel DefenceForces.
[3] Wirbel R, Pistorius G, Braun C, Eichler, Mutschler W. Bilateralvertebral artery lesion after dislocating cervical spine trauma. A casereport. J Trauma 1996; 40 (2):261–5
[4] Golueke P, Sclafani S, Phillips T, Goldstein A, Scalea T, DuncanA. Vertebral artery injury-diagnosis and management. J Trauma1987;27(7):774–81.










![[Originalgröße] Kopie von March • 25 • 2019N.U. Auditorium ... · Taekwondo, Kung Fu, Ninja Uniforms FT- 0109 TAEKWONDO Uniform 100% Cotton Drill, V-Neck White, Elastic Waist](https://img.pdfslide.net/doc/110x75/5f623a05467ccb2d9e163446/originalgre-kopie-von-march-a-25-a-2019nu-auditorium-taekwondo.jpg)