-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
1/143
Cardiovascular system &
dental considerations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
2/143
ContentsIntroduction
Anatomy & physiology
Examination of CVS
Questionnare
ECG & JVP
Infective endocarditis
Rheumatic fever
Hypertension
Ischaemic heart disease
Anticoagulation therapy and dental care
Acute coronary syndromes
Congenital heart diseases
Valvular heart diseases
Cardiac Arrhythmias
Heart failure
Conclusion
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
3/143
IntroductionCardiovascular diseases (CVD) are very common in
India , though more
frequent and severe in the later stages of life, can also affect
young
individuals.
They have high mortality rate and the associated morbidity
affects all walksof life impacting the quality of life .
A thorough knowledge of CVD is necessary because of its
implications in
dentistry and also the initial measures to be taken by the
dentists in case of
certain emergency conditions can be life saving.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
4/143
Anatomy & physiology
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
5/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
6/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
7/143
Clinical examinationof CVS
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
8/143
QuestionnareHave you experienced chest pain or shortness of
breath
The quality of chest discomfort should be determined by asking
the patient
to describe the nature of the episode and the usual radiation
pattern
associated with it .
An unpleasant sensation , squeezing , pressing ,strangling ,
constricting ,
bursting and burning .
Clenching of the fist in front of the chest while describing the
sensation is a
very strong indication of an ischemic origin of the pain (Levine
sign )
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
9/143
Where does the pain ,hurt or radiate
Anginal pain is usually substernal , across both sides of the
chest . Pain may
radiate to various regions. Common sites of radiation of
ischemic chest pain
include the neck and jaw , the upper epigastric region (stomach
) , intracapsular
( between shoulder blades ), to the left arm .
If the pain or discomfort is localized , the origin is not
usually ischemic
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
10/143
Have you experienced swollen ankles or shortness of breath
Bilateral swelling of the legs ,is a common feature of chronic
CVDs
Shortness of breath is a major symptom of CVDs . Dyspnea may
vary in severity
from an uncomfortable awareness of breathing to a frightening
sensation offighting for breath
Questions regarding exertional dysapnea, orthopnea , paroxysmal
nocturnal
dyspnea should be asked .
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
11/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
12/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
13/143
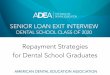
3 distinct waves are produced
during cardiac cycle
P wavecaused by atrial
depolarization
QRS complexcaused by
ventricular depolarization
T waveresults from ventricular
repolarization
ECG
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
14/143
ECG interpretationP waves are absent in atrial fibrillation and
before ventricular premature beats.
Normally, all P waves are followed by QRS complexes but in third
degree A-V
block, P waves do not bear any relation to QRS complexes.
Morphology and duration of P waves are important to determine
left and
right atrial hypertrophy.
A tall P wave >2.5 mm in amplitude (P pulmonale) seen in
right atrial
enlargement.
A wide P wave >0.1 seconds (P mitrale) seen in left atrial
enlargement
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
15/143
The P-R interval (normally 0.12-0.20 seconds) reflects
intra-atrial, AV nodal
and His-Purkinje conduction. It is the interval between the
beginning of P wave
and the beginning of QRS complex.
The QRS complex, has a normal duration of 0,04-0.10 seconds.
Abnormal Q
waves are present in myocardial infarction.
Wide and bizarre QRS complexes are seen in ventricular ectopics,
ventricular
tachycardia and supraventricular tachycardia with aberrant
conduction.
Increase in the height of QRS complexes indicates right or left
ventricular
hypertrophy
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
16/143
ST segment elevation or depression is seen in ischaemic heart
disease,
cardiomyopathies, myocarditis and conduction blocks. Some drugs
like digitalis
can also produce ST segment depression.
T waves represent ventricular repolarisation.InvertedT waves are
frequently seen in cases with ischaemic heart disease,
bundle branch blocks, atrial fibrillation with rapid ventricular
rate and in PS
VT due to relative coronary insufficiency.
QT interval is abnormal in hypokalemia and hypocalcaemia
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
17/143
Electrocardiography is useful in the following situations:
Effects of drugs (digitalis). Hypothermia, pericarditis.
Myocardial ischaemia and infarction.
Cardiac arrhythmias.
Conduction defects.
Chamber hypertrophy.
Electrolyte abnormalities (hypokalemia, hyperkalemia,
hypocalcaemia,
hypercalcaemia).
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
18/143
Jugular venous pulseJugular venous pulse is the oscillating top
of a height of venous blood in the
internal jugular vein which faithfully reflects the pressure and
haemodynamic
changes in the right side of heart in all phases of the cardiac
cycle.
Jugular venous pressure is expressed as the vertical distance in
centimetres
between the top of the venous column and the sternal angle,
regardless of the
body position. Normally, it is less than 3 cm. By convention,
jugular venous
pressure is measured from the sternal angle with the patient
reclining at 45.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
19/143
Central venous pressure can be accurately estimated from the
jugular venous
pressure. For this, the sternal angle is taken as the reference
point The centre
of the right atrium lies 5 cm below the sternal angle,
regardless of body
position. The central venous pressure is calculated as 5+jugular
venous
pressure in centimetres (e.g. if jugular venous pressure is 6
cm. the central
venous pressure = 5 + 6= 11 cm of blood).
Jugular venous pressure reflects the central venous pressure and
also the mean
right atrial pressure.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
20/143
The various waves on JVP reflect the phasic pressure
changes in the right atrium.
Normal JVP has three positive waves, namely, a, c andv waves,
and two negative descents namely xdescent andy descent
awave is due to right atrial contraction
Thecwave is due to bulging of the tricuspid valve into
the right atrium and impact of the adjacent carotid artery
during ventricular systole.
v wave is due to passive right atrial filling during
ventricular systole.
Thexdescent ('systolic collapse9) is due to atrialrelaxation and
downward displacement of tricuspid
valve during systole.
a They descent ('diastolic collapse') is due to opening ofthe
tricuspid valve and the rapid flow of blood into
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
21/143
Causes for raised JVP
Abnormalities in wave form
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
22/143
Infective endocarditis & subacute bacterial endocarditis
Infective endocarditis (IE) is a microbial infection of the
endothelial surface of
the heart or heart valves that most often occurs in proximity to
congenital or
acquired cardiac defects.
A clinically and pathologically similar infection that may occur
in the
endothelial lining of an artery, usually adjacent to a vascular
defect (e.g.,
coarctation of the aorta) or a prosthetic device (e.g.,
arteriovenous [AV] shunt),is calledinfective endarteritis.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
23/143
Previously, IE was classified as acute and subacute, to reflect
the rapidity of
onset and duration of symptoms prior to diagnosis.
It has now largely been replaced by a classification that is
based on the
causative microorganism (e.g., streptococcal endocarditis,
staphylococcal
endocarditis, candidal endocarditis) and the type of valve that
is infected (e.g.,
native valve endocarditis [NVE], prosthetic valve endocarditis
[PVE]). IE is
also classified according to the source of infection, that is,
whether community
acquired or hospital acquired, or whether the patient is an
intravenous drug
user.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
24/143
EtiologyA total of 80% to 90% of cases of identified IE are due
to Viridans streptococci
(alpha-hemolytic streptococci)and staphylococci. This variation
depends on the
type of valve infected (i.e., native or prosthetic), whether the
infection is
community acquired or hospital acquired (nosocomial).
The species that most commonly cause endocarditis are
Streptococcus sanguis,
Streptococcus oralis (mitis), Streptococcus salivarius,
Streptococcus mutans, and
Gemella morbillorum formerly called Streptococcus morbillorum).
Group D
streptococci, which include Streptococcus bovis and the
enterococci
(Enterococcus faecalis)
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
25/143
Other microbial agents that less commonly cause IE include the
HACEK group
(Haemophilus, Actinobacillus, Cardiobacterium, Eikenella,
Kingella),
Pseudomonas aeruginosa, Corynebacterium, pseudodiphtheriticum,
Listeria
monocytogenes, Bacteroides fragilis, and fungi.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
26/143
PATHOPHYSIOLOGY AND COMPLICATIONSThe sequence of events leading
to infection usually begins with injury or damage
to an endothelial surface, most often of a cardiac valve
leaflet. Although IE can
occur on normal endothelium, most cases begin writh a damaged
surface, usually
in proximity to an anatomic defect or prosthesis. Endothelial
damage can result
from any one of a variety of events, including the
following:
A high-velocity jet striking endothelium
Flow from a high- to a low-pressure chamberFlow across a
narrowed orifice at high velocity Fibrin and platelets then
adhere to the roughened endothelial surface and form small
clusters or masses
callednonbacterial thrombotic endocarditis (NBTE)
A similar and frequently indistinguishable condition is found in
somepatients with systemic lupus erythematosis and is called
Libman-Sacksverrucous endocarditis
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
27/143
With the occurrence of a transient bacteremia, however, bacteria
can be seeded
into and adhere to the mass. Additional platelets and fibrin are
then deposited
onto the surface of the mass, which serves to sequester and
protect the bacteria
that undergo rapid multiplication within the protection of the
vegetative mass.
Once established, the metabolic activity and cellular division
of the bacteria are
reduced, which decreases the effectiveness of antibiotics.
Bacteria are slowly and continually released from the
vegetations and shed into
the bloodstream, resulting in a continuous bacteremia; fragments
of the friable
vegetations break off and embolize. A variety of host immune
responses to
bacteria may occur. This sequence of events results in the
clinical manifestations
of IE.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
28/143
The clinical outcome of IE depends upon several factors,
including the
following:
Local destructive effects of intracardiac (valvular) lesions
Embolization of vegetative fragments to distant sites, resulting
in infarction or
infection
Hematogenous seeding of remote sites during continuous
bacteremia
Antibody response to the infecting organism with subsequent
tissue injury
caused by deposition of preformed immune complexes or
antibody/complement interaction with antigens deposited in
tissues
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
29/143
ComplicationsHeart failure that results from severe valvular
dysfunction. This most commonly
occurs as a problem with aortic valve involvement followed by
mitral and then
tricuspid valve infection.
Embolization of vegetation fragments leads to complications in
up to 35% of
cases of IE, with stroke being the most common.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
30/143
SIGNS AND SYMPTOMSThe classic findings of IE include fever,
heart murmur, and positive blood
culture, although the clinical presentation may be varied.
In many cases of IE that have been reported due to dentally
induced bacteremia,
the interval between the dental appointment and the diagnosis of
IE has been
much longer than 2 weeks (sometimes months) unlikely that the
initiating
bacteremia was associated with dental treatment.
Peripheral manifestations ofIE due to emboli and/or immunologic
responses areless frequently seen since the advent of antibiotics.
These include petechiae of
the palpebral conjunctiva, the buccal and palatal mucosa, and
extremities.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
31/143
Osler's nodes (small, tender, subcutaneous nodules that develop
in the pulp of
the digits), Janeway lesions (small, erythematous or
hemorrhagic, macular
contender lesions on the palms and soles), splinter hemorrhages
in the nail beds,
and Roth spots, retinal hemorrhages with pale centers)
Other signs include splenomegaly and clubbing of the digits.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
32/143
DUKES CRITERIAThe Duke criteria were developed and later
modified to facilitate the definitive
diagnosis of IE. This set of diagnostic criteria assesses the
presence or absence
of major and minor criteria.
MAJOR CRITERIA Positive blood cultures
Evidence of endocardial involvement (e.g., positive
echocardiography,
presence of new valvular regurgitation)
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
33/143
MINOR CRITERIA Predisposing heart condition or IV drug use
Fever
Vascular phenomena
Immunologic phenomena
Microbiologic evidence other than positive blood culture
Definitive diagnosis of IE requires the presence of two
majorcriteria, one major and three minor criteria, or five minor
criteria.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
34/143
LABORATORY FINDINGSComplete blood count with differential,
electrolytes, renal function tests,
urinalysis, chest x-ray, and electrocardiogram (ECG). Patients
with IE
frequently have a normocytic, normochromic anemia that tends to
worsen as
the disease progresses. The white blood cell count may or may
not be elevated.
Urinalysis often reveals microscopic hematuria and proteinuria.
Chest x-ray
may be abnormal with evidence of heart failure.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
35/143
ECG may show evidence of conduction block with myocardial
involvement or
infarction. Other abnormal findings may include an elevated
erythrocyte sedi-
mentation rate, increased immune globulins, circulating immune
complexes, and
positive rheumatoid factor.
Echocardiography is used to confirm the presence of vegetation
in patients
suspected of having IE; it has become a cornerstone in the
diagnostic process.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
36/143
Dental considerationsAntibiotic ProphylaxisDental treatment has
long been implicated as a significant cause of IE. It was
most often due to a bacteremia that resulted from an invasive
dental procedure,
and that through the administration of antibiotics prior to
those procedures, IE
could be prevented.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
37/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
38/143
CURRENT AMERICAN HEART ASSOCIATION RECOMMENDATIONS(2007)
AHA cites the following reasons for revision of the previous
recommendations:
IE is much more likely to result from frequent exposure to
random bacteremia
associated with daily activities than from bacteremia caused by
a dental
procedure
Prophylaxis may prevent an exceedingly small number, if any, of
cases of IE
in individuals who undergo a dental procedure
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
39/143
The risk of antibiotic-associated adverse events exceeds the
benefit, if any,
from prophylactic antibiotic therapy
Maintenance of optimal oral health and hygiene may reduce the
incidence of
bacteremia from daily activities and is more important than
prophylactic
antibiotics for reducing the risk of IE resulting from a dental
procedure
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
40/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
41/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
42/143
Special SituationsPatients Already Taking AntibioticsPatients
who are already taking penicillin or amoxicillin for eradication of
an
infection (e.g., sinus infection) or for long-term secondary
prevention of
rheumatic fever are likely to have viridans group streptococci
that are relatively
resistant to penicillin or amoxicillin.
Clindamycin, azithromycin, or clarithromycin should be selected
for prophylaxis
if treatment is immediately necessary. Because of cross
resistance with
cephalosporins, this class of antibiotics should be avoided. An
alternative
approach is to wait for at least 10 days after completion of
antibiotic therapy
before administering prophylactic antibiotics. In this case, the
usual regimen can
be used.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
43/143
Patients Who Undergo Cardiac Surgery.It is recommended that a
preoperative dental evaluation be performed and
necessary dental treatment provided whenever possible prior to
cardiac valve
surgery or replacement or repair of congenital heart
disease.
Prolonged Dental Appointment.The length of a dental appointment
in relation to the effective plasma
concentration of an administered antibiotic is not addressed in
these
recommendations.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
44/143
With amoxicillin, which has a half-life of approximately 80
minutes, the
average peak plasma concentration of 4 (mg/mL is reached about 2
hours after
oral administration of a 250-mg dose. Most of the
penicillin-sensitive viridans
group streptococci have an MIC requirement of 0.2 mg/mL. Thus, a
2-g dose of
amoxicillin would produce an acceptable MIC for at least 6
hours. If a
procedure lasts longer than 6 hours, it may be prudent to
administer an
additional 2-g dose.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
45/143
Other ConsiderationsNo evidence suggests that coronary artery
bypass graft surgery is associated
with long-term risk for infection; thus, antibiotic prophylaxis
is not
recommended for these individuals. Patients who have had a heart
transplant
are at increased risk for acquired valvular dysfunction,
especially during
episodes of rejection. Endocarditis that occurs in this instance
is associated with
a high risk of adverse outcome; therefore, patients with
mechanical or tissue
prosthetic valves will often be taking long-term anticoagulant
medication (e.g.,
warfarin) to prevent valve-associated thrombosis. These patients
are at risk for
excessive bleeding during and after surgical procedures.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
46/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
47/143
Rheumatic feverRheumatic fever is an inflammatory disease
occurring as a delayed sequale to
pharyngeal infection with group A Streptococci. It primarily
involves the heart,
joints, central nervous system skin and subcutaneous
tissues.
EtiologyRheumatic fever follows an antecedent pharyngeal
infection with group A
beta hemolytic steptococci
Latent period between the pharyngeal infection and the onset of
fever 1-5weeks, with average duration being 19 days.
Fewer than 2-3% of previously healthy persons develop rheumatic
fever.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
48/143
Streptococcus-induced autoimmunity is believed to be the
mechanism resulting in
rheumatic process.
Several Streptococcal antigens have demonstrated cross
reactivity with cardiac
and other tissues.
Acute rheumatic fever is characterised by exudative and
proliferativeinflammatory lesions of the connective tissues. It
mainly involves the heart,
joints and subcutaneous tissues.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
49/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
50/143
MANAGEMENT Bedrest Antistreptococcal therapyA course of
antibiotic should be given to eradicate the streptococci, even if
the
throat culture is negative. One of the following regimens may be
used:
a. Single injection of benzathine penicillin 1.2 million units
intramuscularly.
b. Daily injection of procaine penicillin 6,00,000 units
intramuscularly for 10
days.
c. Oral erythromycin 20-40 mg/kg/day in three divided doses, in
patients who
are sensitive to penicillin.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
51/143
SalicylatesAspirin is effective in providing symptomatic
relief.
Aspirin is started at doses of 60 mg/kg/day in 6 divided doses.
Dose is increased
gradually until the drug produces either a clinical improvement
or systemic
toxicity (tinnitus, headache or hyperpnoea). This dose might go
up to 120
mg/kg/day or a maximum of 8 g/day.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
52/143
CorticosteroidsPatients who have severe carditis manifested by
congestive heart failure not
responding to aspirin.
Patients with severe arthritis whose symptoms and signs are not
adequately
suppressed by aspirin.
Prednisolone is given orally at a dose of 60-120 mg/day in four
divided doses
until the ESR is normal. It is then gradually tailed off over a
period of 2 weeks. 4
To prevent a 'post-steroid rebound' an 'overlap course of
aspirin may be added
when the steroid is being tapered off.
Aspirin is then continued for an additional 2-3 weeks
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
53/143
PreventionPrimary prevention can be summarised as accurate
diagnosis and treatment of
group A streptococcal pharyngeal infection.
An outbreak of rheumatic fever in a closed population is best
treated by mass
penicillin prophylaxis.
Rheumatic fever prophylaxis should be given to all patients who
have
experienced a documented attack of rheumatic fever.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
54/143
Duration of prophylaxis is controversial. Broad outlines
are:
Those under the age of 18 years should receive continuous
prophylaxis.
Those who are over 18 years who develop rheumatic fever without
carditis
should receive prophylaxis for a minimum period
of5years.Decisionto continue prophylaxis beyond 5 years in the
second group depends on
many variables like age of tbe patient, relative risk of
acquiring infection,
socioeconomic state, presence of rheumatic heart disease,
etc.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
55/143
4 Regimens: One of the following regimens may be used:
Intramuscularinjection of 1.2 millionunits ofbenzathine
penicillin
G every 3 weeks (most efficient regimen).
Oral penicillinV 250 mg twice a day.Sulphadiazine 1 g/day orally
as a single dose (in those allergic to
penicillins).
Erythromycin 250 mg twice a day orally (in those allergic
topenicillins and sulpha)
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
56/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
57/143
HYPERTENSIONHypertension is an abnormal elevation in arterial
pressure that can be fatal if
sustained and untreated. People with hypertension may not
display symptoms
for many years but eventually can experience symptomatic damage
to several
target organs, :ncluding kidneys, heart, brain, and eyes. In
adults, a sustained
systolic blood pressure of 140 mm Hg or greater and/or a
sustained diastolic
blood pressure of 90 mm Hg or greater is defined as
hypertension.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
58/143
The dental patient with hypertension poses several potentially
significant
management considerations.
These include
identification of disease,
monitoring stress and anxiety reduction,
prevention of drug interactions, and
awareness and management of drug adverse effects.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
59/143
EtiologyAbout 90% of patients have no identifiable cause for
their disease, which is
referred to asessential, primary, or idiopathichypertension. For
the remaining10% of patients, an underlying cause or condition may
be identified; for these
patients, the termsecondaryhypertension is applied.
The most common cause of secondary hypertension is renal
parenchymal disease,
followed by renovascular disease and various adrenal disorders
(a
pheochromocytoma of the adrenal medulla).
Lifestyle can play an important role in the severity and
progression of
hypertension; obesity, excessive alcohol intake, excessive
dietary sodium, and
physical inactivity are significant contributing factors.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
60/143
Pathophysiology and ComplicationsIn sustained essential
hypertension, the basic underlying defect is a failure in the
regulation of vascular resistance.
The pulsating force is modified by the degree of elasticity of
the walls of larger
arteries and the resistance of the arteriolar bed. Control of
vascular resistance is
multifactorial, and abnormalities may exist in one or more
areas. Mechanisms of
control include neural reflexes and ongoing maintenance of
sympathetic
vasomotor tone; neurotransmitters such as norepinephrine,
extracellular fluid,
and sodium stores; the renin-angiotensin-aldosterone pressor
system; and locally
active hormones and substances such as prostaglandins, kinins,
adenosine, and
hydrogen ions (H)
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
61/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
62/143
Signs & symptomsHypertension may remain an asymptomatic
disease for many years, with the
only sign being elevated blood pressure.
Blood pressure is measured with the use of a sphygmomanometer.
Pressure at the
peak of ventricular contraction issystolic pressure.
Diastolic pressure represents the total resting resistance in
the arterial system
after passage of the pulsating force produced by contraction of
the left
ventricle.
The difference between diastolic and systolic pressures is
calledpulse pressure.
Mean arterial pressure is roughly defined as the sum of the
diastolic pressure
plus one-third the pulse pressure.
Labile hypertension is the term that was previously used to
describe a subgroup of patients with wide variability in
blood
pressures
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
63/143
About 15% to 20% of patients with untreated stage 1 hypertension
have what
is calledwhite coat hypertension, which is defined as
persistently elevated blood
pressure only in the presence of a health care worker but not
elsewhere.
Before the age of 50, hypertension is typically characterized by
an elevation in
both diastolic and systolic pressures. Isolated diastolic
hypertension, defined as a
systolic pressure 90, is uncommon and is most
often found in younger adults.
Isolated systolic hypertension is defined as a systolic pressure
>140 and a
diastolic blood pressure
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
64/143
Alcohol and smoking should be avoided for 30mins
beforemeasurement
Allow the patient to rest
Place the sphygmomanometer cuff on right upper arm with about
3
cm of skin visible at the ante-cubital fossa , should encircle
atleast
2/3rdof the arm
Palpate radial /brachial artery
Inflate the cuff slowly to about 200-250 mm Hg or until the
pulse
is no longer palpable
Assessment of blood pressure
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
65/143
Deflate cuff slowly while listening with the stethoscope over
the brachial artery
over the skin
Record the systolic pressure as and when the first tapping sound
appears
( korotkoff sounds )
Deflate cuff further until the tapping sounds become muffled i.e
diastolic
pressure and then disappear.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
66/143
The "ideal" cuff should have a bladder length that is 80% and a
width that is at
least 40% of arm circumference (a length-to-width ratio of
2:1).
The recommended cuff sizes are:
For arm circumference of 22 to 26 cm, the cuff should be "small
adult" size:
12X22 cm
27 to 34 cm, "adult" size: 16X30 cm
35 to 44 cm, "large adult" size: 16X36 cm
45 to 52 cm, "adult thigh" size: 16X42 cm
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
67/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
68/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
69/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
70/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
71/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
72/143
DENTAL CONSIDERATIONSThe first task of the dentist is to
identify patients with hypertension, both
diagnosed and undiagnosed. A medical history, including the
diagnosis of
hypertension, how it is being treated, identification of
antihypertensive drugs,
compliance of the patient, the presence of symptoms associated
with
hypertension, and the level of stability of the disease, should
be obtained.
Patients receiving treatment for complications of hypertensive
disease, such as
congestive heart failure, cerebrovascular disease, MI, renal
disease, peripheral
vascular disease, and diabetes mellitus should be identified
.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
73/143
Blood pressure measurements should be routinely performed for
all new patients
and at recall appointments. When a patient with upper level
stage 2 blood
pressure is treated, consideration should be given to leaving
the blood pressure
cuff on the patient's arm and periodically checking pressure
during the
appointment.
The primary concern when one is providing dental treatment for a
patient with
hypertension is that during the course of treatment, the patient
might experience
an acute elevation in blood pressure that could lead to a
serious outcome such as
stroke or MI.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
74/143
This acute elevation in blood pressure could result from the
release of endogenous
catecholamines in response to stress and anxiety, from injection
of exogenous
catecholamines in the form of vasoconstrictors in the local
anesthetic, or from
absorption of a vasoconstrictor from the gingival retraction
cord.
Other concerns include potential drug interactions between the
patient's
antihypertensive medications and the drugs prescribed and oral
adverse effects
that might be caused by antihypertensive medications.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
75/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
76/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
77/143
Drug interactionsSome NSAIDS ( indomethacin , ibuprofen ,
naproxen ) can reduce the efficacy of
antihypertensive agents.
Sodium based analgesics should be avoided
Systemic corticosteroids may raise the BP and antihypertensive
treatment may
have to be adjusted .
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
78/143
Because some antihypertensive agents tend to produce orthostatic
hypotension,
sudden changes in chair position during dental treatment should
be avoided.
After patients have had time to adjust to the change in posture,
they should be
physically supported while slowly getting out of the chair and
should have
obtained good balance and stability. If they complain of
dizziness or
lightheadedness, they should sit back down until they recover
equilibrium.
References
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
79/143
Burketsoral medicine 10th& 11thedition.
Essentials of medical physiology 3rdedition. Sembulingam.
Davidsonsprinciples & practice of medicine 20thedition.
Current medical diagnosis & treatment. Lange 2004
Dental management of medically compromised patients. 7th
edition. Little
Medicine prep manual for undergraduates 3rd edition George
mathew
Ischemic Heart Disease
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
80/143
Is an inflammatory disease affecting the large and medium sized
arteries of
heart resulting in inadequate or decreased coronary blood flow
.
Symptomatic coronary atherosclerotic heart disease is referred
to as coronary
heart disease.
Atherosclerosis & hypertension are the major contributory
factors .
Atherosclerosis is the thickening of the intimal layer of the
arterial wall caused
ne accumulation of lipid plaques. The atherosclerotic process
results in a
narrowed arterial lumen with dimmer blood flow and oxygen
supply.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
81/143
In the later stages , the atherosclerotic plaque ruptures and
exposes the arterial
blood to the plaque contents and stimulates the formation of
haemostatic plug .
This occlusive thrombus may cause myocardial infaction.
Atherosclerosis is the most common underlying cause of not only
coronary an
disease (angina and myocardial infarction [MI]) but :
cerebrovascular disease
(stroke) and peripheral artery disease (intermittent
claudication).
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
82/143
Coronary obstruction/Cardiac pain/Cardiac Ischemia lesion
II) Occlusion
Obstruction:Impediment.Stenosis Narrowingof blood vesslePain
:Angina Pectoris Cardiac lesionsIschemia fibrosis.
Occlusion:Closed vesselPain :InfarctPain
Cardiac lesionsInfarct (necrosis).
I) Obstruction Narrowlumen
Closureof thelumen
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
83/143
Risk factors
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
84/143
Male gender, older age, a family history of cardiovascular
disease,
hyperlipidemia, hypertension, cigarette smoking, physical
inactivity, obesity,
insulin resistance and diabetes mellitus, mental stress, and
depression. In
addition to these conventional risk factors, markers of
inflammation such as C-
reactive protein, homocysteine, fibrinogen, and lipoprotein(a)
have been found
to be associated with atherosclerosis.
Between the ages of 35 and 44 years, the risk is 5 times greater
for men than for
women.
Studies have confirmed that individuals with parents or siblings
affected bycoronary atherosclerotic heart disease have a greater
risk of developing the diseaseat a younger age than do those
without such a history. This risk may be as highas 5 times
greater.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
85/143
ANGINA PECTORIS
Defined as a temporary inability of the coronary arteries to
supply the
myocardium with sufficient amount of circulated blood
Due to imbalance between myocardium oxygen requirement and
oxygen supply.
Angina is a Latin word describing a spasmodic , cramp like
,choking feeling or
suffocation & pectoris meaning chest.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
86/143
DurationStable Chronic , classic , exertional 1-15mins Due to
obstruction of
coronaries by atheroma.
Variant
angina
prinzmetal or atypical or
vasopastic
at rest or Odd times
such as night
Variable
due to Spasm of coronaries.
Unstable Preinfarction ,crescendo At rest or very lowlevels of
exertion ,any
factors .
Upto 30 mins
Due to spasm and partialobstruction of coronaries.
Variants of angina
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
87/143
The atypical attack of classic angina usually follows physical
exertion or
emotion stress . The patient is seized with a viselike crushing
pain in the
substernal region .
The pain radiates characteristically to the left shoulder and
down the arm to the
4th and 5th finger tips , but it may radiate to other areas ,
including the neck
region and even the jaws .
Jaw pain has been reported to occur in the absence of precordial
or substernal
pain . This crushing pain lasts a few seconds to minutes, seldom
longer .
Diagnosis
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
88/143
ElectrocardiographyECG is normal in these pts at rest and in
between
attacks . Evidence, is demonstration of reversible ST segment
depression or
elevation ,with or without T wave inversion during attack of
pain .
Exercise testingtreadmill testing or bicycle ergometry .
Myocardial perfusion scanning using radioactive thallium
Echocardiography
Coronary arteriography , provides detailed information about the
extent and
site of coronary artery stenosis.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
89/143
Dental considerations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
90/143
Acute anginal attack may occur as a result of the stress
associated with dental
services , particularly extractions .
It is speculated that because of the over lapping of the 5th
cranial nerve , 3rd
cervical nerve and 1st thoracic nerve cardiac pain may be
transmitted to the jaw
and interpreted as dental pain .
Anginal jaw pain is characterized by its extreme severity , its
onset associated
with exertion and its disappearance with rest .these
characteristics serve to
differentiate it from the usual pain of dental origin .
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
91/143
MYOCARDIAL INFARCTIONSynonymscoronary occlusion and heart attack
.
MI is a clinical syndrome caused by a deficient coronary
arterial blood supply to
a region of myocardium that results in cellular death and
necrosis . The
syndrome is usually characterized by severe and prolonged
substernal pain
similar to , but more intense and of longer duration than , that
of angina
pectoris
Anginal attack lasting longer than 30mins is considered by
definition to be a
MI
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
92/143
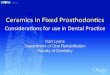
MI Types
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
93/143
MI - Types
Transmural
Full thickness
Superimposed thrombus in
atherosclerosis
Focal damage
Sub-endocardial
Inner 1/3 to half of ventricular
wall
Decreased circulating bloodvolume( shock, Hypotension,
Lysed thrombus)
Circumferential
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
94/143
Symptoms
Pain severe & intolerable , prolonged 30 mins , crushing ,
choking ,
retrosternal , radiates to left arm , hand epigastrium shoulders
neck and jaws
Nausea and vomiting weakness , dizziness palpitations ,cold
perspiration
Signsrestlessness , acute distress
Skincool ,pale ,moist
Heart ratebradycardia later tachycardia
Investigations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
95/143
ECGuseful in conforming the diagnosis
ST segment elevation
Appearance of pathologic Q waves i.e initial negative
deflections .
Detectable by changes in S-T segment of ECG
Myocardial infarction(MI) is diagnosed by high
levels of creatine phosphate (CPK) & lactate
dehydrogenase (LDH)
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
96/143
Plasma enzymes1 . Creatine kinase (CK)More specific and starts
to rise at 4-6 hrs , reaches
peak 12 hrs , falls back to normal in 48-72 hrs
2. aspartate aminotransferase (AST)
Lactate dehydrogenase (LDH)
Myoglobin
Troponins (I and T )
Dental considerations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
97/143
Prevention
Identification of the at-risk patient permits modification in
dental care that , in
most instances will prevent the development of chest pain
Elimination of stress ( emotional and physical ) is primary
preventive measure .
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
98/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
99/143
Studies have indicated the influence of circadian variation on
the triggering
of acute coronary events , occur between 6 am and noon . It has
been
proposed that sympathetic nervous system activation and an
increased
coagulative state may be precipitating factors
Therefore , dental care for highrisk pts might ideally be
provided in the late
morning or the early afternoon .
Consultation with the patients primary physicians or
cardiologists prior to
dental therapy is recommended.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
100/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
101/143
Anticoagulation therapy and dental care
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
102/143
Patients with CAD may require the use of aspirin or other
antiplatelet drug , such as clopidogrel .
The combination of acetylsalicylic acid and clopidogrel is
usually
continued for a minimum period of 4 weeks after stent
placement
and 3-6 months after drugeluting stents
The most common antiplatelet drug is aspirin , which is used
chronically in low doses to prevent CVD . Aspirin
irreversiblydecreases platelet aggregation and pts will take
between 81-325 mg
/day
Data that address the risk of bleeding from dental extractions
in pts who
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
103/143
Data that address the risk of bleeding from dental extractions
in pts who
use antiplatelet agents are limited
although a bleeding time test is often recommended to evaluate
the
qualitative defect in platelets
If emergency surgery needs to be performed and there is concern
about
aspirin therapy , 1-desamino8D- arginine vasopressin(DDAVP)
can
be instituted to improve hemostatis
DDAVP isadministered parenterally at 0.3g/kg , maximum dose
20-24gwithin 1 hour of surgery
A nasal spray containing 1.5 mg DDAVP per mm can be given in a
dose of
300 mg /kg
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
104/143
Studies suggest that there is no need to discontinue or alter
anticoagulation
therapy prior to routine oral surgical procedures for patients
taking
antiplatelet medications other than aspirin
There seems to be a consensus that the risk to the patient (
thromboembolism)
if these drugs are discontinued , which far exceeds the problem
of prolonged
bleeding
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
105/143
The most commonly used antithrombin medications are the
dicumarols (
e.g.warfarin) , which inhibit the biosynthesis of vitamin K
dependent
coagulation proteins ( factors II, prothrombin , VII ,IX and
X)
The full therapeutic effect of warfarin is reached after 4872
hrs and lasts
for 3672 hrs if the drug is discontinued
The efficacy of warfarin therapy is monitored by INR and in the
range of 2-
3.5 is considered as adequate .
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
106/143
There is minimal indication for discontinuation of
anticoagulation therapy ,
before minor oral surgical procedures when pts INR is
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
107/143
3) warfarin therapy is discontinued and the patient is placed on
an alternative
anticoagulation therapy
Advantagepts risk for developing thromboembolic events is
minimized by
comparision with the 2ndprotocol .
Unfractionated heparin is used for bridging the warfarin free
period and
vitamin K is administrated . Heparin is continued ,
approximately to about
6hrs before surgery and is reinstituted after surgery with in
combinationwoth oral anticoagulants until desirable INR has been
achieved .
The advantage of using heparin are its short half life of 4-6
hrs and the
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
108/143
availability of antidote , protamine sulfate .
Patient can also self administer a subcutaneous injection of low
molecular
weight heparin on an outpatient basis.
Recent guidelines from AHA suggests that there is no requirement
of
antibiotic prophylaxis for dental procedures in pts after
coronary stent
placement , unless the pt presents with an acute odontogenic
pain .
risk of bleeding in highly invasive dental procedures is small
and bleeding
is relatively easy to manage , antiplatelet therapy should never
be
discontinued for elective dental procedures.
Acute coronary syndromes
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
109/143
The sudden rupture of an atherosclerotic plaque ,with ensuing
intracoronary
thrombus formation that acutely reduces coronary blood flow ,
causes ACS
ACSs represent a continuous spectrum of disease ranging from
unstable
angina , nonST elevation MI to acute ST elevation MI (STEMI)
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
110/143
The diagnosis of an ACS is usually made on the basis of
clinical
data .the patients history suggests a change in anginal pattern
at
rest
Acutely ,the ECG is important to risk stratify the patient and
to
make decisions regarding treatment
Resting ST segment depression or T wave inversions in the
distribution of an epicardial coronary artery often
accompanyunstable angina , STsegment elevation is the hallmark of
an acute
MI
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
111/143
Step -1 termination of the dental procedure
Step 2 : P (position ) the anginal patient is consciuos and
usually
apprehensive . The pt is allowed to position themselves in the
most
comfortable manner . Commonly sitting or standing upright . The
supine
position is rarely preferred .
Step 3 :A-B-C ( AIRWAY BREATHING CIRCULATION) or basic
life support (BLS)
Step -4 : D (definitive care )
4aadministration of vasodilator and oxygen
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
112/143
If the patient experiences an anginal attack while in the dental
chair ,
a nitroglycerine tablet should be placed immediately under the
tongue
or the patient should inhale amyl nitrate . These medications
are not
useful in patients known to be having a myocardial
infraction.
In patients with known anginal pectoris , either classic or
variant ,
relatively short acting antianginal drugs such as sublingual
isosorbide
nitrate tablets are recommended prophylactically before
initiating
dental therapy or a particularly stressful phase of dental
therapy .
Recognize the problem ( chest pain or dysapnea)Emergency
management
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
113/143
Discontinue dental treatment
Activate office emergency kit
Pposition . Commonly sitting or standing upright . The supine
position is
rarely preferred
A-B-C ( AIRWAYBREATHINGCIRCULATION) or basic lifesupport
(BLS)
Ddefinitive management
History of angina
present
Administer
vasodilators and
O2
If pain resolves consider
further dental
modifications , monitor
vital signs and
treatment
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
114/143
In the dental office , the use of nitrolingual spray is
preferred to the
sublingual tablets because of the relative insability of the
tablets
One or two metered sprays are recommended intially with no more
than 3
metered doses within a 15 min period , whereas sublingual
nitoglycerine
tablets are recommended at 0.3 0.6 mg every 5 mins as needed
with no more
than 3 tablets every 15 mins
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
115/143
Nitroglycerine normally reduces or eliminates anginal
discomfort
dramatically within 2 4 mins ,commonly seen side effects are
fullness or
pounding in the head,flushing,tachycardia and possible
hypotension .
Represents a contraindication to nitroglycerine
administration
Congenital heart diseases
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
116/143
Are the common heart disease among children , present in 1% of
live
births
Cyanotic
transposition of great vessels , tetralogy of
FallotAcyanotic
Atrial and ventricular septal defect , pantent ductus
arteiosus,
soarctation of aorta ,pulmonary and aortic stenosis , mitral
valve
prolapse
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
117/143
Dental considerations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
118/143
Antimicrobial prophylaxis
Dental bacteria may cause cerebral abscess
Bleeding tendencies due to platelet dysfunction and excessive
fibrinolytic
activity .
Gingival retraction cord containing epinephrine
Valvular heart disease
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
119/143
Mitral valve disease - mitral valve prolapse(MVP) ,
mitral regurgitation (MR) , mitral stenosis (MS )
Aortic valve diseasesAR and AS
Prosthetic heart valves currently most widely used is the
bileaflettilting disk valves
Bioprosthetic valves - heterografts made from porcine or bovine
tisssue
or the homografts from preserved human aortic valves.
Patients with mechanical valves are on chronic anticoagulation
therapy
and are at an increased risk of IE
DENTAL CONSIDERATIONS
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
120/143
According to AHA 2007 , antimicrobial prophylaxis is now
recommended
only for people defined as being in higher risk for a poor
outcome
Prophylaxis is recommended because endothelialization of
prosthetic material
occurs within 6 months after the procedure.
Pacemakers
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
121/143
These are small implanted electronic devices that stimulates the
heart to beat
and pace the heart rate when it is too slow
Bipolar , implanted transvenously in the subclavian or cephalic
vein and
typically located in right ventricle .
Dental apparatus with no known effect on cardiac pacemakers
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
122/143
Electric toothbrushes
Electronic apex locators
Piezoelectric ultrasonic scalers
Dental apparatus with likely effects on cardiac pacemakers
Electronic dental analgesia units
Electrosurgical units
MRI units
TENS units
Ultrasonic instruments
Cardiac Arrhythmias
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
123/143
Refers to any variation in the normal heartbeat, and includes
disturbances of
rhythm, rate, or the conduction pattern of the heart. Cardiac
arrhythmias are
present in a significant percentage of the population, many of
whom will seek
dental treatment. Most arrhythmias are of little concern to the
patient or die
dentist; however, some can produce symptoms, and a few may be
life
threatening.
Th l f i l d l i i i f
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
124/143
The normal pattern of sequential depolarization consists of
(1) sinoatrial (SA) node
(2) atrioventricular (AV) node
(3) bundle of His
(4) right and left bundle branches
(5) subendocardial Purkinje network.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
125/143
Normal cardiac function depends on cellular automaticity
(impulse forrnation),
conductivity, excitability, and contractiiity. Disorders in
automaticity and
conductivity form the basis of the vast majority of cardiac
arrhythmias.
Disorders of conductivity (block or delay) paradoxically may
lead to rapid
cardiac rhythm.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
126/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
127/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
128/143
Investigations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
129/143
The electrocardiogram (ECG) is the primary tool used in the
identification
and diagnosis of cardiac arrhythmias. Additional tests that may
be used
include exercise or stress testing, long-term or ambulatory ECG
(Holter)
recording, baroreceptor reflex sensitivity testing, body surface
mapping, and
upright tilt-table testing. Electrode catheter techniques allow
for
intracavitary recordings of the specialized conducting systems,
which aid
greatly in the diagnosis of arrhythmias.20
Drugs in arrhythmias
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
130/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
131/143
Dental considerations
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
132/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
133/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
134/143
Heart failureh d f f h d l d h
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
135/143
HF represents the end stage of many of the cardiovascular
diseases. The
American College of Cardiology/ American Heart Association 2005
Guideline
Update for the Diagnosis and Management of Chronic Heart Failure
in the
Adult1 defines HF as a complex clinical syndrome that may result
from any
structural or functional cardiac disorder that impairs the
ability of the
ventricle to fill with or eject blood. Patients with untreated
or poorly
managed HF are at high risk during dental treatment for
complications such
as cardiac arrest, cerebrovascular accident, and myocardial
infarction.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
136/143
When right-sided ventricular enlargement occurs as the result of
a lung
disorder (e.g., emphysema), pulmonary hypertension is produced;
this
condition is calledcorpulmonale
.
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
137/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
138/143
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
139/143
Conclusion
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
140/143
Referencesk l d th & th d
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
141/143
Burketsoral medicine 10th& 11thedition
Davidsonsprinciples & practice of medicine 20thedition.
Current medical diagnosis & treatment. Lange 2004
Dental management of medically compromised patients. 7th
edition. Little
Medicine prep manual for undergraduates 3rd edition George
mathew
Referencesk l di i th & th di i
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
142/143
Burketsoral medicine 10th& 11thedition.
Essentials of medical physiology 3rdedition. Sembulingam.
Davidsonsprinciples & practice of medicine 20thedition.
Current medical diagnosis & treatment. Lange 2004
Dental management of medically compromised patients. 7th
edition. Little
Medicine prep manual for undergraduates 3rd edition George
mathew
-
7/27/2019 Sem 11 Cardiovascular System & Dental
Considerations
143/143