Embed Size (px)
Citation preview

NATURE MEDICINE • VOLUME 9 • NUMBER 1 • JANUARY 2003 19
NEWS & VIEWS
The main function of the heart is toprovide adequate delivery of oxygen
to meet the metabolic demands of thebody under conditions of normal andincreased workload. Although the per-formance of the heart is well maintainedover a wide range of physiological stres-sors, increased biomechanical stressfrom either exercise or disease can drivemorphological changes in the heartmuscle, known as cardiachypertrophy. Cardiac hy-pertrophy is an increasein mass of the heart dueprimarily to an increase incell size, which under cer-tain conditions progressesinto heart failure. Themolecular and cellularmechanisms that are atthe base of the pathologi-cal transition from cardiachypertrophy to cardiacfailure have been the sub-ject of intense investiga-tion for over a halfcentury. In this issue,Brancaccio et al.1 addressthe fundamental questionof how biomechanicalstress translates into bio-chemical changes inside aheart muscle cell. Theyshow that the integrin-bound protein melusinacts as a biomechanicalsensor, and that it is pro-tective against the adverseeffects of pressure over-load.
Pressure-overload–in-duced cardiac hypertro-phy, such as that causedby chronic hypertension,is triggered by two majortypes of input that resultin an enlarged muscle: (1) mechanicalstress and (2) neural and humoral fac-tors that activate growth factor receptortyrosine kinases (RTKs), cytokine recep-tors and G-protein-coupled receptors2
(GPCRs), particularly those that coupleto the Gq class of heterotrimeric gua-nine-nucleotide binding regulatory pro-teins (G proteins)3. Signals originatingfrom all of these pathways converge in-
tracellularly and result in altered geneexpression and protein synthesis thatlead to an enlarged heart.
Although many of the factors that ini-tiate GPCR-mediated hypertrophy havebeen studied extensively, the role of bio-
mechanical sensor molecules in cardiachypertrophy is less understood.Transduction of mechanical stress intobiochemical signals is largely mediatedby a group of cell surface receptors calledintegrins, which link the extracellularmatrix (ECM) to the cellular cytoskele-ton, thus providing physical integrationbetween the outside and the inside of thecell. Activation of integrins by different
ligands in the ECM (for example, colla-gen, fibronectin and laminin) initiatessignaling in multiple intracellular path-ways through integrin-bound proteinsthat regulate gene expression, cell growthand survival4,5. One of the candidate pro-teins to act as a biomechanical sensor inthis pathway is melusin, which interactswith the cytosolic domain of integrinand is expressed exclusively in skeletal
and cardiac muscle5.In this new report1, the
authors examined therole of melusin in the de-velopment of cardiac hy-pertrophy in response totwo different models.Mice that are geneticallydeficient for the melusingene were exposed to ei-ther biomechanical stressthrough physical con-striction of the aorta7, orhormonally induced car-diac hypertrophy throughactivation of Gq-coupledreceptors at doses that donot induce elevation inblood pressure. The mostimportant finding of thisstudy is that melusin wascritical only for the devel-opment of biomechani-cally induced cardiachypertrophy, whereas itwas not involved in hor-monally induced hyper-trophy or in normal heartfunction and develop-ment. Moreover, mice thatwere melusin-deficient de-veloped heart failure in re-sponse to biomechanicalpressure overload. The au-thors further identified arole for melusin in the ac-
tivation of a specific signaling pathwayinvolved in mediating the hypertrophicresponse. Together their data indicatethat the actions of melusin are restrictedto integrin-mediated signaling pathwaysactivated by mechanically induced pres-sure overload.
A long-standing controversy has cen-tered on whether the development ofcardiac hypertrophy is protective
Sensing heart stressHeart failure and pathological overgrowth of the heart often occur hand in hand. New data on a biomechanical
sensor challenge the viewpoint that cardiac hypertrophy causes heart failure (pages 68–75).
LIZA BARKI-HARRINGTON &HOWARD A. ROCKMAN
CytokinesRTKs
GPCRs
Pressure overload
Integrins
α β
Melusin
Hypertrophy
Heart failure No heart failure
Gαq
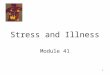
Fig. 1 Signaling pathways in the development of cardiac hypertrophy in re-sponse to pressure overload. Pressure overload initiates signaling in multiplepathways that result in cardiac hypertrophy. Melusin is a biomechanical trans-ducer that is selectively involved in integrin-mediated hypertrophy, and is pro-tective against the development of heart failure. In contrast, activation of othersignaling pathways that also lead to cardiac hypertrophy, such as Gq-coupled re-ceptors, is deleterious and often progresses to heart failure. Progression to heartfailure is unlikely to be related to the development of hypertrophy, but rather islikely to be related to the intricate balance between the activation of protectiveand deleterious signaling pathways.
Kim
ber
ly H
omer
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

20 NATURE MEDICINE • VOLUME 9 • NUMBER 1 • JANUARY 2003
NEWS & VIEWS
against the deterioration into heart fail-ure. The long-held view has been thatcardiac hypertrophy in response topathological overload serves to restoreheart muscle stress back to normal andcounteracts the progressive deteriora-tion of cardiac function. However, re-cent studies have demonstrated thatcardiac hypertrophy is not critical forthe prevention of cardiac deterioration.Rather it is the chronic activation ofGq-coupled receptors and other signal-ing pathways that is harmful8,9. Giventhe observation that the lack ofmelusin prevents the development ofcardiac hypertrophy and promotesheart failure, Brancaccio et al. deducethat hypertrophy prevents the deterio-ration in cardiac function. While theirdata are certainly intriguing, we offer adifferent interpretation of it. In ouropinion, progression to cardiac failuredoes not depend on the phenotype ofhypertrophy, but rather is related to theintricate balance between the activa-tion of protective and deleterious sig-naling pathways. In this regard, thenovel contribution of Brancaccio et al.lies in the identification of a moleculethat is involved in a hypertrophic sig-naling pathway and is also protective
against the development of heart fail-ure. In contrast, the activation of Gq-coupled receptor signaling pathways,which also culminates in the same phe-notype of cardiac hypertrophy, is dele-terious and often progresses to cardiacenlargement and heart failure9,10. It isnot the hypertrophy per se that deter-mines a detrimental outcome, butrather the different signaling pathwaysthat are activated in response to thechronic overload state of the heart.Indeed, a recent study supports thefinding of a protective role for integrinsagainst the development of pressure-overload–induced heart failure4.
The identification of the precise inter-section between the integrin–melusinpathway and other signaling pathwayswill be of great importance in under-standing the complexity of the hyper-trophic response that leads to heartfailure. Further investigation will likelyprovide the exact molecular mecha-nisms involved in pressure-overload–in-duced cardiac hypertrophy and perhapslead to novel therapeutic opportunitiesfor the treatment of this deadly disease.
1. Brancaccio, M. et al. Melusin, a muscle-specific in-tegrin β1-interacting protein, is required to pre-vent cardiac failure in response to chronic
pressure overload. Nature Med. 9, 68–75 (2003).2. Molkentin, J.D. & Dorn, I.G., 2nd. Cytoplasmic
signaling pathways that regulate cardiac hyper-trophy. Annu. Rev. Physiol. 63, 391–426 (2001).
3. Akhter, S.A. et al. Targeting the receptor-Gq in-terface to inhibit in vivo pressure overload my-ocardial hypertrophy. Science 280, 574–577(1998).
4. Shai, S.Y. et al. Cardiac myocyte-specific excisionof the β1 integrin gene results in myocardial fi-brosis and cardiac failure. Circ. Res. 90, 458–464(2002).
5. Giancotti, F.G. & Ruoslahti, E. Integrin signaling.Science 285, 1028–1032 (1999).
6. Brancaccio, M. et al. Melusin is a new muscle-spe-cific interactor for β(1) integrin cytoplasmic do-main. J. Biol. Chem. 274, 29282–29288 (1999).
7. Rockman, H.A. et al. Segregation of atrial-specificand inducible expression of an atrial natriureticfactor transgene in an in vivo murine model ofcardiac hypertrophy. Proc. Natl. Acad. Sci. USA88, 8277–8281 (1991).
8. Rockman, H.A., Koch, W.J. & Lefkowitz, R.J.Seven-transmembrane-spanning receptors andheart function. Nature 415, 206–212 (2002).
9. Esposito, G. et al. Genetic alterations that inhibitin vivo pressure-overload hypertrophy preventcardiac dysfunction despite increased wall stress.Circulation 105, 85–92 (2002).
10. Adams, J.W. et al. Enhanced Gαq signaling: Acommon pathway mediates cardiac hypertrophyand apoptotic heart failure. Proc. Natl. Acad. Sci.USA 95, 10140–10145 (1998).
Department of Medicine, Cell Biology, and GeneticsDuke University Medical CenterDurham, North Carolina, USAEmail: [email protected]
Protein-based agents that block the ac-tion of cytokines have substantially im-
proved treatment for patients withautoimmune diseases over the last fiveyears. Diseases such as rheumatoid arthri-tis, psoriasis and Crohn’s inflammatorybowel disease are now routinely treatedwith agents such as neutralizing mono-clonal antibodies to tumor necrosis factor(TNF; Remicade, also known as inflix-imab). Other agents include receptors toTNF (Enbrel or etanercept) and the inter-leukin-1 receptor antagonist (IL-1Ra;Kineret or anakinra). These specific anti-cytokine–based therapies can reduce in-flammation and joint destruction inrheumatoid arthritis, are being used inover 250,000 patients and have validatedthe importance of IL-1 and TNF in inflam-matory diseases. But the current repertoireof agents has some drawbacks—chiefamong them is the relatively short half-life, which necessitates frequent injections
or intravenous infusions. Fully humanagents with high affinities and long bio-logical half-lives would provide improvedtherapeutic options.
To that end, Economides et al. have de-veloped novel ‘cytokine traps’1 which takeadvantage of the way that cytokines bindto the extracellular domains of their cellsurface receptors. In general, cytokinessuch as IL-1, IL-4 or IL-18 first bind to asingle surface receptor protein chain witha relatively low affinity. But this bindingdoes not result in signal transduction; in-stead, binding results in recruitment of asecond, usually structurally distinct pro-tein chain. It is this new complex of thecytokine bound to the two receptor chainsthat initiates the signal (Fig. 1). The cy-tokine binds to the two-chain complexconsiderably more tightly than that to the
first protein chain due to two distinctbinding domains on the cytokine, whicheach bind to the separate chains2. The nat-urally occurring IL-1Ra lacks the secondbinding domain and does not recruit thesecond chain in the receptor complex.
The cytokine trap takes advantage of thetwo separate receptor chains, which to-gether provide high-affinity binding. Thecytokine trap provides both receptorchains in a dimeric configuration that re-sembles the two chains of extracellular cellsurface receptor. The trap is, however, dif-ferent in that each arm of the dimericstructure is identical and contains do-mains of both receptor chains. The twochains of the trap are linked by fusion ofthe complement binding domain of IgG1.As such, the structure is not natural, but iscomposed of solely natural proteins. Thestructures are stable, bind cytokines withhigh affinity and have the potential tosupplant current therapies.
Setting the cytokine trap for autoimmunityAgents that block the action of specific cytokines have changed the lives of many patients with rheumatoid arthritis
and other autoimmune disorders. But frequent self-injections or injections by a physician during a clinic visit arerequired. Now a new class of anti-cytokine that may bypass such problems appears on the horizon (pages 47–52).
CHARLES A. DINARELLO
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine





![Compressed sensing and applications in positioning, audio …users.ics.forth.gr/~tsakalid/PAPERS/VALENCIA_Talk_2011... · 2015. 12. 19. · Compressed Sensing [Donoho06][Tao06] Heart](https://img.pdfslide.net/doc/110x75/60e01b5e56d1544b94735e13/compressed-sensing-and-applications-in-positioning-audio-usersicsforthgrtsakalidpapersvalenciatalk2011.jpg)