Embed Size (px)
Citation preview
Sepsis Response Bag
Sepsis Response Bag Introduction,John Burke,
Critical Care Outreach,Royal Glamorgan Hospital,
Cwm Taf LHB.

Sepsis
A Massive ProblemHigh Mortality.40% Severe Sepsis.50% Septic Shock.Biggest Cause of Maternal Death.
High Costs Associated.Big Use of ITU Resources.
Timely Intervention is Paramount.Unsure of real numbers affected.

Drivers of Change
Saving 1000 Live +
Rapid Response To Acute Illness Learning Set. (RRAILS)
National Institute for Clinical Excellence (NICE 50)
Centre for Maternal and Child Enquiries, (CMACE)
Our will to succeed !

Tools
Survive Sepsis CampaignSepsis SixSepsis/Severe Sepsis PathwayNEWS chartsClinical Accumen and Experience
Sepsis Response Bag.
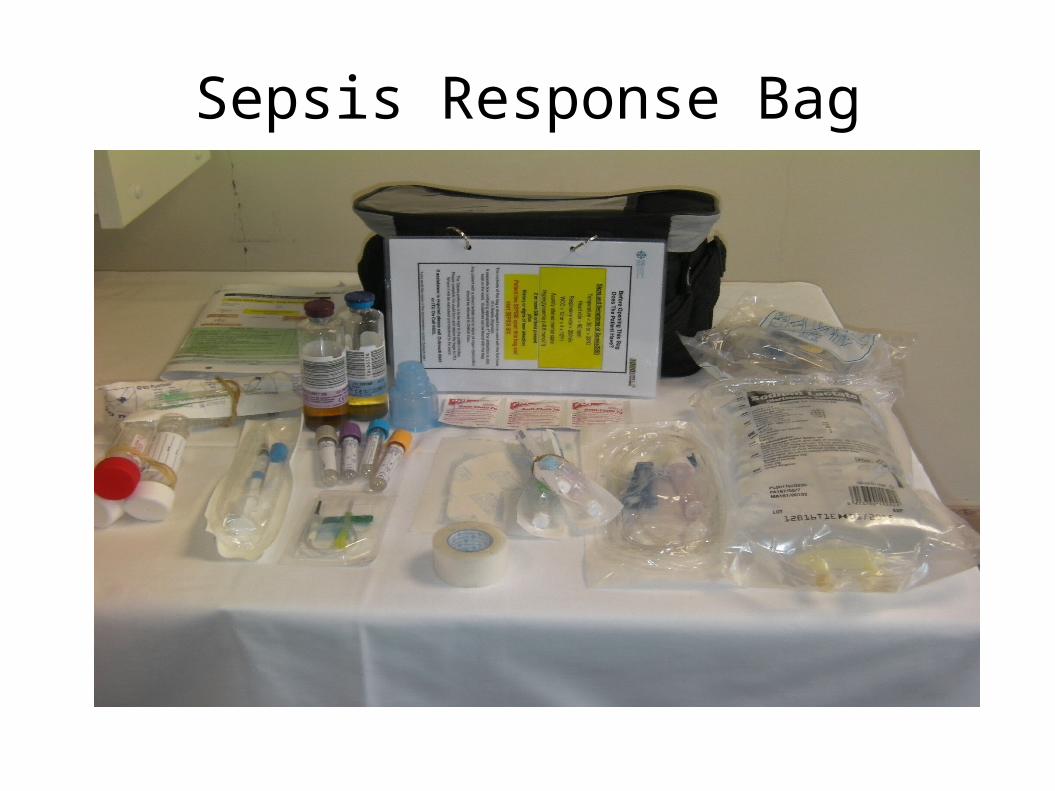
Sepsis Response Bag

A Simple Solution ?
One Stop Answer.
Proven Research Based Response
Low Cost.
Saves Time.
IVABs stored on each ward.

Problems Encountered
Senior Nurses, Outside of Critical Care Working Group.
Microbiology.
Resuscitation Dept.
Senior Medics.
Directorate Lead Nurse.

Problems Solved
NEWS Training Sessions
Nurse/Student Training Sessions
Outreach Teaching Slot.
Junior Doctors Training Sessions.
Rapid Roll Out To All Wards.
Sepsis Screening Tool Card and Posters.

Buy In.
400 Nurses and Students
50 Medics
Maternity and Obs
•Work shared with the Maternity Collective.
•New Work on Obstetric Sepsis Six plus 2.
•Keen to move forward and work with Outreach.

Audit and Assessment
4 Stranded Assessment:
Sepsis Document» 1 hour goals met ?
Bag Equipment» What was used ?
User Questionaire» What did people think ?
Patient follow up, Day 0,1, 7 and past 24hrs,» IVABs and Microbiology review» Mortality/Survival Data

Preliminary Results. Wards
15 bags opened, (10 by Outreach.)All 15 fullfilled criteria.9 Pt fullfilled criteria within previous 24 hrs.50% received IVABs with in 1 hour.Reluctance to change IVABs without Microbiology
agreement.Questionable 1 hours targets met.
2 Pt repeat bags.
1 ITU Admission.

Preliminary Results A+E/MCDU
Initially No Sepsis Pt Identified ! Why ?
8 Pt identified and put on Sepsis proforma.
2 achieved 1 hour goal2 incomplete 1 sepsis form missing
1 Pt admitted to ITU with no proforma.

Initial Feed Back
Bags are usefull !Primarily Blood bottles, cultures, butterfly and hub
and paperwork used.
Equipment to add in.
Probably do save time.
ConclusionMore Work To Be Done.
Continued Sepsis Education and Awareness
Continued Monitoring of Sepsis Pts.
Aim Training at Juniors and New Staff.
Data base to be started.
Data Mine Outreach Previous Audit for Comparison
“Be Aware of Sepsis, Beware Sepsis”
Continued Thanks
Andrew HermanDr Tamas Szakmany
Dr Chris SubbeDr Ron Danials
Chris Hancock RRAILS