Embed Size (px)
Citation preview

Sepsis: Three phases crucial for
clinicians to consider
Didier Payen MD, Ph D
INSERM 1160 Univ Paris 7 Diderot



The W-shaped mortality curve seen in the 1918 influenza pandemic curves for incidence of clinical illness vs. fatality rate markedly differ Same age-dependent mortality pattern is seen for TB, pneumococcal infection, trauma, Yellow fever, malaria, streptococcal Toxic shock, etc.
What accounts for this difference? Fedson D. Antiviral Research 2013; 99,(3), 417- 435


The reaction to the sepsis-induced stress…

Sepsis a complex Puzzle
outcome Anti infl cytokines
Physiol
Status
Type of infection
circulatory & metabolic consequences
Iatrogenic
complications
Economical
aspects
Genetic Time course of the Disease
Pro infl cytokines
Strategy for care
Hormonal patterns

Medzhitov et al. Science 2012; 355:936-41
• “Threat” vs. non-threat • Tolerating pathogens • Limiting host response
• Stress hormones • Anti-inflammatory actions • Pro-resolving actions

Medzhitov et al. Science
2012; 355:936-41
Organ-specific
tolerance capacity
to pathogen-
induced or
immune-induced
pathology
1o research question: 1) Can we promote immune
tolerance or pathogen tolerance at the right time in vulnerable patients


1994 Matzinger: Danger model
Response to non physiologic Cell death
Tolerance # Autoimmunité
Pathogen pathway PAMPs or MAMPs
“stranger model”
Infection and sepsis
Cell and tissue lesions DAMPs
“danger model”
infection, trauma, postop, burns


Phase 1 Phase 2 Phase 3

Phase 1

The host response to sepsis
Days
Pro
-in
fla
mm
ato
ry
resp
on
se
s
An
ti-i
nfl
am
ma
tory
resp
on
se
s
Excessive inflammation causing collateral damage (tissue injury)
Immune suppression resulting in enhanced susceptibility for nosocomial pathogens

NEJM 2013; 369: 840
The Host Response to Sepsis

The Host Response to Sepsis

Drug RCT’s (number)
Odds ratio (survival)
Corticosteroids high dose Corticosteroids low dose
5 9
0.91 (0.31-1.25) 0.80 (0.40-1.37)
IL-1 receptor antagonist 3 1.18 (0.97-1.44)
PAF antagonists 7 1.10 (0.93-1.30)
Prostaglandin antagonists 3 1.22 (0.78-1.58)
Bradykinin antagonists 2 0.91 (0.65-1.27)
Immunoglobulins 17 1.47 (0.55-6.25)
Anti-inflammatory strategies in sepsis trials
Adapted from: Leentjens J et al. AJRCCM 2013; 187: 1287

Qui P et al. Crit Care Med 2013; 41: 2419
Anti-TNF trials

The Host Response to Sepsis

The Host Response to Sepsis

0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Surv
ival
Study Day
Log-rank test P value: 0.5789
Hazard ratio (95% CI): 1.05 (0.88, 1.26)
Placebo
Eritoran
Placebo Censored
Eritoran Censored
ACCESS trial: TLR4/MD2 inhibition in severe sepsis
28-day mortality
28.1%
26.9%

The Host Response to Sepsis
Activated Protein C Antithrombin
Tissue factor pathway inhibitor
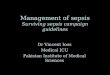
Ranieri et al NEJM 2012
PROWESS-SHOCK (NEJM 2012)
Percent in study hospital 28d:
DrotAA 305 (49%)
Placebo 279 (43%)

The Host Response to Sepsis
Urgent need for biomarkers that reflect the predominant type of the host response to sepsis in an individual patient.
Aid in identification of patients that might benefit from a specific intervention.
Aid in titrating the intervention and monitoring the response.
Rapid: “point-of-care”.

Phase 2

Phase 1 Phase 2 Phase 3

Loss of delayed type hypersensitivity response to common recall antigens
Apoptosis-induced depletion of immune effector cells, loss of CD4, CD8, B, and dendritic cells Reactivation of latent viruses (CMV; herpes virus in roughly 25–35% of patients
with sepsis)
autopsy most patients admitted to ICUs for treatment of sepsis had unresolved septic foci at post mortem, patients
unable to eradicate invading pathogens and were more susceptible to nosocomial organisms, or both Blood studies from patients with and without sepsis show decreased production of proinflammatory cytokines, decreased monocyte HLA-DR expression,
increased numbers of regulatory T cells (Treg Fox P3), increased production of PD-1 or PD-L1
Clinical or laboratory evidence for sepsis being an immunosuppressive disorder


Patients with a slope of log(mHLA-DR) <0.06 (poor recovery of HLA-
DR expression) had a higher risk of secondary infection than the group with slope >0.06.
Cumulative incidences of secondary infections after 7 days:
Crit Care Med 2009; 37: 2746–2752
283 patients

(Crit Care Med 2009; 37: 2746–2752)

Venet et al. Crit Care Med 2013; 41(1):111-119
T cell repertoire rapidly decreases in sepsis

Is this immunodepression also observed in tissue
infiltrating immune cells?

splenocytes from sepsis patients had highly
significant functional impairments as evidenced
by major reductions in cytokine secretion.
Multiple inhibitory mechanisms were identified,
dominance of inhibitory over activating receptors, expansion of suppressive cell types,
and induction of inhibitory ligands on both APCs and tissue parenchymal cells.
Both pro- and anti-inflammatory cytokines were impaired.
Cytokine production at 22 hours in sepsis patients was comparable
with controls, some patients, defective cytokine secretion
may be reversible if cells are removed from the sepsis milieu.

Sepsis Profound Loss of CD4 and CD8 Cells
the loss of CD 4 T cells mimics HIV in severity in ineffective adaptive immunity
Non- septic Septic
Boomer, Chang, Takasu, et. al Journal of the American Med. Association (JAMA) 306:2594 2011

Can we treat it? Does it change outcome?

39 2013
PMN, Mono phagocytose mHLA-DR TNF
Fct Mono Phagocytose
Prolif. Tcell IFN Anti-apoptose PD-1, molec adhesion Treg Diversité récepteurs TCR

interferon
0
5000
10000
15000
20000
25000
30000
35000
Day3 Day6 Day7
Day9 Day11
Day12 Day13
Day15 Day17
discharge
BAL pseudomonas aeru 109 +++ +++ + 0 0
2603 570
mH
LA-D
R (
AB
/C)
Days after ICU admission (post cardiac arrest)
Lukaszewicz et al.Crit Care Med 2009; 37: 2746–2752
Nl

IL-7 restores INF- γ in septic patients
Elispot for IFN-γ: PBMC from whole blood
from septic patients and incubated overnight
in wells with anti-CD3/anti-CD28 to stimulate
T cells. Half of the wells had IL-7 and
have did not.
The amount of IFN-γ produced is indicated by
the red color. IL-7 containing wells
produced much more IFN-γ compared to
non-IL-7 treated wells.
From Monneret et al J Immunol 2012

Can we restore immune tranquility to our
septic patients? Yes we can, but its going to be complicated

February 2013
Immunostimulation therapy in sepsis: a new approach

Phase 3

Is it relevant for the clinician?
D0: Oesophagectomy
D8: severe SIRS WCk from 6 400 to 64 600 BAL: 102 Citrobacter, ECBU (-), HC (-), HC sur PAC (-), Plèvres (-) OGDF: No fistulae TDM IV opacifié: NO leak, NO mediastinitis
D1 Early post-operative period -Hypoxemia with pleural effusion chest drainage -CCVasc collaps responding to fluid challenge -Acute Kidney Injury AKIN3
D11: M O S F
GB: 223 000 98% PMNs (Chronic ttmt fro ITP with GFactor) BC+ : multiple bateria Serratia et Citrobacter, Tracheal asp >10 7 Citrobacter, OGDF & TDM no fistulae AB: 3 molecules (Cefotax; linezolid; Imipenem)

(x 10
0
50
100
150
200
250
300
350
400
450
3rd/4th -07
6th 7th 8th 9th 10th
SOFA
P/F ratio
creatinine (mm/l)
WBC (n x 103 /ml)
PMNs (n x 103 /ml)
Hydrea 1 dose
NE 1.6 0.8 0 0
Day +6
Controlling immuno-inflammation improved
In OFailures:
1- Cvasc (stop NE) 2- Lung (increase P/F ratio) 3- AKI stabilisation (creat)
Let’s see the results of immune monitoring….

0
100
200
300
400
500
600
700
800
900
1000
ROS PRODUCTION (AUC) HEALTHY MRS G 7/7 MRS G 11/7 MRS G16/7
ROS production by PMNs
Hydrea 1 dose
ROS production measured in 10 min in our lab (patent) by luminescence
Quantitative value
28383 22262
35032
23017
34016 31757
53850
80094
HEALTHY MRS G 7/7 MRS G 11/7 MRS G16/7
Phenotyping CD11b
Immune phenotype CD11b Immune phenotype CD11b
Hydrea 1 dose Phenotyping of the immune cells Using flowcytometry (5 colors) Timing 1 hr Quantitative results
PMNs CD11b decreased with Hydrea ttmt… not in monocytes

To conclude:
• At least 3 phases different mechanisms; different cause of mortality
• Phase 1 Acute phase of cellular activation + mediators tissue lesions
• Phase 2 Rapidly induced Post Agressive Immuno Depressing (PAID) Syndrome
• Phase 3 Revovery phase: relatively unknown continues to increase mortality along time.
• All these phases require different markers to diagnose the phase, the intensity and the risk of mortality
• Until now, RCTs had mainly concerned the Phase 1, Phase 2 is on going with immuno-stimulation


TCR CD28
ICOS
CTLA4 PD1
BTLA
T cell Early co-
stimulatory
signals
B7-
H2
CD80
CD86
B7.1/2
CD80CD86 PD-
L1 HVEM
MHCII
APCs, DCs, B cells
monocyte/macrophages
Signal 1
Signal 2
The CD 28 family of T
cell antigens
Epitope
groove

TCR CD28
ICOS
CTLA4 PD1
BTLA
T cell Early co-
stimulatory
signals
Late co-
inhibitory
signals
B7-
H2
CD80
CD86
CD80CD86 PD-
L1 HVEM
MHCII
APC, monocyte/macrophage, some
epithelial and endothelial cells

Sepsis - induced effector cell apoptosis in spleen tissue
Boomer, J. S. et al. JAMA 2011;306:2594-2605

Anti-PD-1 aB improves survival S/P CLP (given 24, 48 hr)
Brahmamdam P et al. J Leukoc Biol 2010;88:233
Similar results in PD-1 KO mice
PD-1 expression impairs bacterial
clearance

Spite, M. and Sherhan Circ Res 2010;107:1170-1184
Proresolving actions of lipoxins, resolvins, and protectins

two important questions: First , despite more than a decade of work on the basic science of
innate immunity and the pathogenesis of sepsis, why has no potential target been translated into a new treatment?
Second, how many more such trials of sepsis need to fail before we call a moratorium and consider a completely different approach?
Studies of sepsis are hampered by the absence of reliable biomarkers to select patients for study. The consequent heterogeneity in the study population is one of the main reasons why achievement of a discernable signal has been so difficult
Hypothesis: modification of an aberrant immune response will limit organ damage.

A genomic storm: Refining the immune, inflammatory paradigm in trauma

The facts…

Cell energetic failure

energy consuming functions of immune cells
• Synthesis of macromolecule & ion transport; O2 is mainly used by mitochondria, non-mitochondrial O2 consumption is negligible
Stop these Functions
When energy fails

It cannot result from tissue hypoxia!!!!

If this immunosupression exists, how can we detect and measure its intensity?

Mechanisms Features of sepsis-induced immune alterations Endotoxin tolerance ↓ pro-inflammatory ↑ anti-inflammatory cytokine
production ↓ Ag presentation capacity
Apoptosis ↓ cell number Cell anergy
Energetic failure Cell anergy Apoptosis Mitochondrial dysfunction
Anti-inflammatory mediators
↓ activating co-receptor expressions ↑ inhibitory co-receptor expressions Cell anergy Endotoxin tolerance
Epigenetic regulation ↓ pro-inflammatory gene expressions Cellular reprogramming
Central and endocrine Regulations
↓ pro-inflammatory cytokine production
From Venet F, Lukaszewicz AC, Payen D, Hotchkiss R, Monneret G (Curr Op Immunol 2013)

Key Concept in Sepsis
Sepsis is a race to the death between the pathogen and the host immune system and one way in which the pathogen wins is by incapacitating key aspects of innate and adaptive immunity.

In conclusion • Sepsis is more complex than a word
• At least 2 phases: • Acute (2 to 3 days)
• Post acute immunodepression • What are the relative contributions of co-morbidities
vs inflammation?
• Immunodepression is always present: • Adaptative? • Should we treat it? Who? When? How?
• Markers are needed for making decision and are ready to be used…
• Several drugs are potentially useful: trial are on going…

In conclusion • Sepsis is more complex than a word
• What are the relative contributions of co-morbidities vs inflammation?
• Immunodepression is always present: • Adaptative?
• Should we treat it? Who? When? How?
• Markers are needed for making decision and are ready to be used…
• Several drugs are potentially useful: trial are on going…

Drug RCT’s (number)
Odds ratio (survival)
Corticosteroids high dose Corticosteroids low dose
5 9
0.91 (0.31-1.25) 0.80 (0.40-1.37)
IL-1 receptor antagonist 3 1.18 (0.97-1.44)
PAF antagonists 7 1.10 (0.93-1.30)
Prostaglandin antagonists 3 1.22 (0.78-1.58)
Bradykinin antagonists 2 0.91 (0.65-1.27)
Immunoglobulins 17 1.47 (0.55-6.25)
Anti-inflammatory strategies in sepsis trials
Adapted from: Leentjens J et al. AJRCCM 2013; 187: 1287

Another caveat affecting treatment selection is timing Patients rapidly transition from the initial cytokine storm to a predominant immunosuppressed state as sepsis persists. shift to an immunosuppressed state occurs for many reasons: massive sepsis-induced death of immune cells, development of T cell exhaustion, generation of T regulatory myeloid-derived suppressor cells.

Host can protect himself from infectious disease
using 3 distinct mechanisms:
Avoidance Resistance Tolerance
Tolerance reduces both tissue damage by
Pathogen and immunopathology The term tolerance used in this context is not to be confused with immunological tolerance,which is defined as unresponsiveness to self antigens

Miscell.
N=43
Neuro
N=85
PostOp
N=16
Trauma
N=20
Hemor.
N=29
SAPS II
Early
mHLA-DR
(< D3)
Sepsis
N=90
*
*

Biomarker guided therapy


Immunotherapy of sepsis.

Neutrophils Versus Staphylococcus aureus: A Biological Tug of War∗ Andras N. Spaan, Bas G.J. Surewaard, Reindert Nijland, and Jos A.G. van Strijp Annu. Rev. Microbiol. 2013. 67:629–50

Neutrophils Versus Staphylococcus aureus: A Biological Tug of War∗ Andras N. Spaan, Bas G.J. Surewaard, Reindert Nijland, and Jos A.G. van Strijp
Annu. Rev. Microbiol. 2013. 67:629–50
Evasion of neutrophil extravasation, activation, and neutrophil attack. (a) Mechanisms by which Staphylococcus
aureus subverts neutrophil extravasation. (b) Neutrophil attack and evasion of
activation. Red boxes represent an antagonizing protein of S. aureus, and green boxes represent a protease of S. aureus.

Neutrophils Versus Staphylococcus aureus: A Biological Tug of War∗ Andras N. Spaan, Bas G.J. Surewaard, Reindert Nijland, and Jos A.G. van Strijp
Annu. Rev. Microbiol. 2013. 67:629–50
Schematic representation of the mechanisms utilized by Staphylococcus aureus to avoid killing inside neutrophils or by neutrophil extracellular traps (NETs). Staphyloxanthin provides an antioxidant shield, and catalase detoxi es hydrogen peroxide. Resistance to cationic antimicrobial peptides (AMPs) is mediated by positive-charge modi cations of the cel

Clinical evidence of immunodepression

Loss of delayed type hypersensitivity response to common recall antigens
Apoptosis-induced depletion of immune effector cells, loss of CD4, CD8, B, and dendritic cells Reactivation of latent viruses (CMV; herpes virus in roughly 25–35% of patients with sepsis)
autopsy most patients admitted to ICUs for treatment of sepsis had unresolved septic foci at post mortem, patients unable to eradicate invading pathogens and were more susceptible to nosocomial organisms, or both Blood studies from patients with and without sepsis show decreased production of proinflammatory cytokines, decreased monocyte HLA-DR expression,
increased numbers of regulatory T cells (Treg Fox P3), increased production of PD-1 or PD-L1
Clinical or laboratory evidence for sepsis being an immunosuppressive disorder

interferon
0
5000
10000
15000
20000
25000
30000
35000
Day3 Day6 Day7
Day9 Day11
Day12 Day13
Day15 Day17
discharge
BAL pseudomonas aeru 109 +++ +++ + 0 0
2603 570
mH
LA-D
R (
AB
/C)
Days after ICU admission (post cardiac arrest)
Lukaszewicz et al.Crit Care Med 2009; 37: 2746–2752
Nl

The Lymphopenia of sepsis (apoptosis and
extravascular distribution)
Monneret et al. Mol Med 2008;14(1-2):64


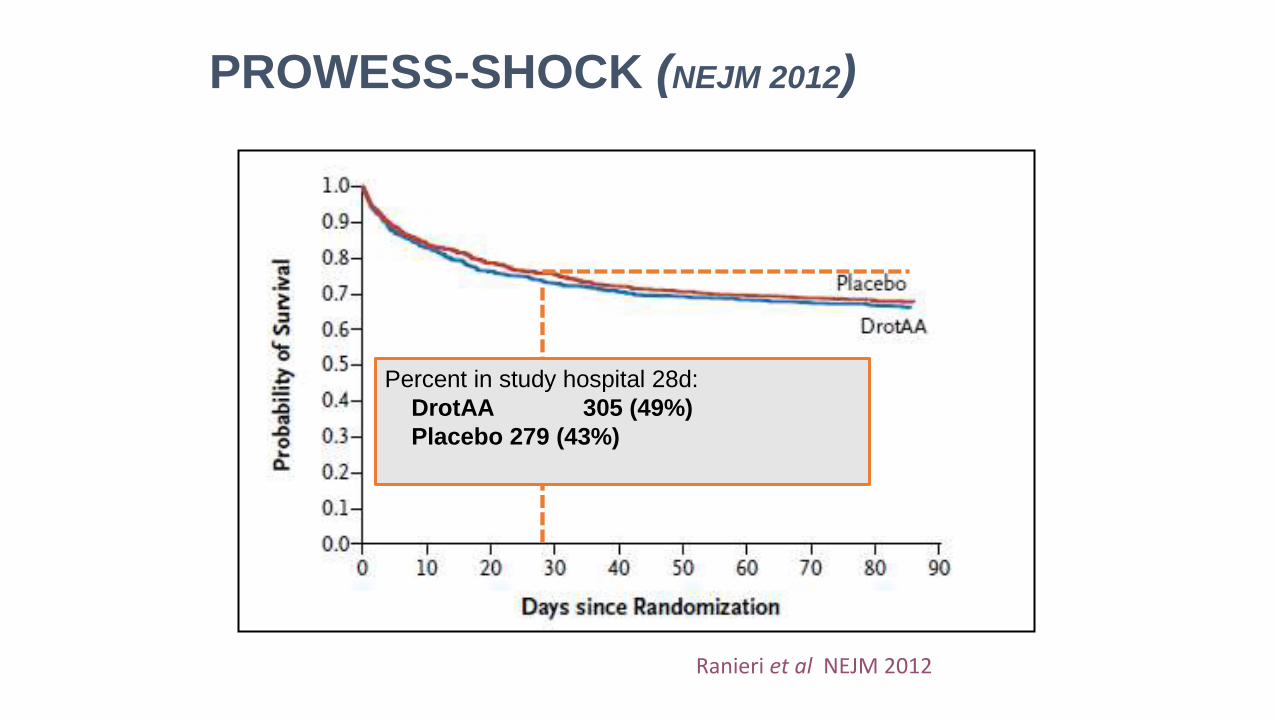
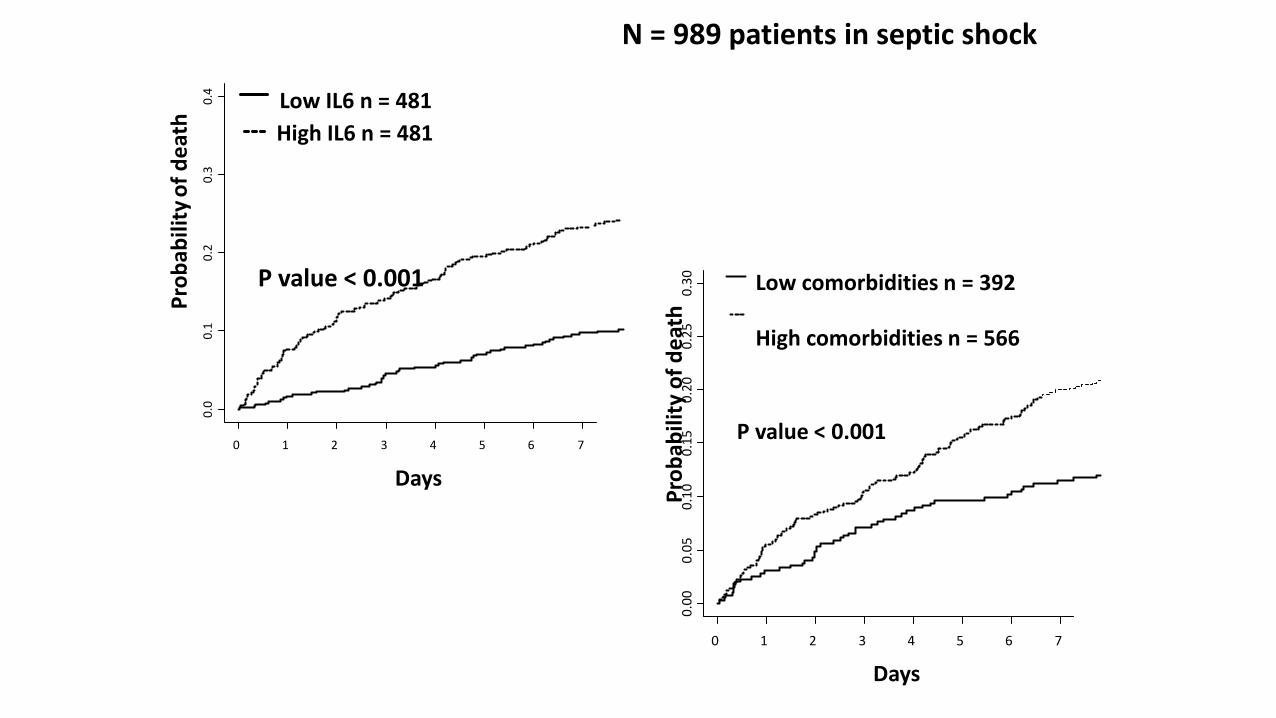
This concept obtained from a training cohort (202 pts) was tested in large testing cohort N = 989 SS patients from Prowess data base

0 5 10 15 20 25
0.0
0
.1
0.2
0
.3
0.4
0
.5
0.6
Days
Pro
ba
bil
ity o
f d
ea
th
Low Il6/Low comorbidities n=167
Low IL6/High comorbidities n=297
High Il6/Low comorbidities n=215
High IL6/High comorbidities n=253
P value < 0.001
N = 989 patients in septic shock

87
“Frapper fort et
frapper vite”
Hit hard and fast
-Paul Erlich, address to
the 17th International
Congress of Medicine,
1913

88
Kumar et al: The median time to effective/appropriate antimicrobial therapy was 6
hours and that for every hour delay over the first 6 hours, the projected mortality
increased by 7.6%. (Crit Care Med 2006)


Figure 3 - Kaplan Meier Curves for time to reversal of shock in (a) ACTH nonresponders (b) ACTH
responders and (c) all patients
placebo
steroid
P value for log rank test: <0.001
0
0.25
0.50
0.75
1.00
0 5 10 15 20 25 30
day
(c) All patients
P value for log rank test: 0.038 0
0.25
0.50
0.75
1.00
0 5 10 15 20 25 3
0
placebo
steroid
(a) ACTH non-responders (b) ACTH responders
P value for log rank test: <0.001 0
0.25
0.50
0.75
1.00
0 5 10 15 20 25 30
placebo
steroid

(b) ACTH responders
P value for log rank test: 0.937 0
0.25
0.50
0.75
1.00
0 5 10 15 20 25 30
placebo
steroid
P value for log rank test: 0.850 0
0.25
0.50
0.75
1.00
0 5 10 15 20 25 30
(a) ACTH non-responders
placebo
steroid
P value for log rank test: 0.813
0
0.25
0.50
0.75
1.00
0 5 10 15 20 25 30
day
(c) All patients
placebo
steroid
Figure 2 - Kaplan Meier Curves for 28 day all-cause mortality in (a) ACTH nonresponders (b) ACTH responders and
(c) all patients

blood cultures before antibiotic therapy (1C)
Early quantitative resuscitation of the septic patient during the first 6 h after recognition (1C)
administration of broad-spectrum antimicrobials therapy within 1 h of the recognition of septic shock (1B)
Initial fluid resuscitation with crystalloid (1B) ; consideration of the addition of albumin in patients who continue to require substantial amounts of crystalloid to maintain adequate
mean arterial pressure (2C); the avoidance of hetastarch formulations (1B); achieve a
minimum of 30 mL/kg of crystalloids

norepinephrine as the first-choice vasopressor to maintain mean arterial pressure ≥ 65 mmHg (1B);
epinephrine when an additional agent is needed to maintain adequate
blood pressure (2B); dopamine is not recommended except in highly selected circumstances
Dobutamine infusion administered or added to vasopressor in the presence of (a) myocardial dysfunction (elevated cardiac filling pressures and low cardiac output) (b) ongoing signs of hypoperfusion despite achieving adequate intravascular volume and adequate mean arterial pressure (1C);
avoiding use of intravenous hydrocortisone in adult septic shock patients if adequate fluid
resuscitation and vasopressor therapy are able to restore hemodynamic stability (2C)
hemoglobin target of 7–9 g/dL

a protocolized approach to blood glucose management commencing insulin dosing when two consecutive blood glucose levels are >180 mg/dL, targeting an upper blood glucose B180 mg/dL (1A);
equivalency of continuous venovenous hemofiltration or intermittent hemodialysis (2B);
use of stress ulcer prophylaxis to prevent upper gastrointestinal bleeding in patients with bleeding risk factors (1B);
oral or enteral (if necessary) feedings, as tolerated, rather than either complete fasting or provision of only intravenous glucose within the first 48 h after a diagnosis of severe sepsis/septic shock (2C);
Although a significant number of aspects of care have relatively weak support, evidence-based recommendations regarding the acute management of sepsis and septic shock are the foundation of improved outcomes for this important group of critically ill patients


Difficult to reverse but good reserve
Easy to reverse But high co-morbidity in elderly…
Comorbidity
AGE Comorbidity
Seve
rity
Sco
re
AGRESSION
Severe Injury + good tissue reserve Moderate injury + high Co-morbidity Similar severity score
Severity is characterized by scores…
Outcome may depend on injury but also
on constitutive factors… Threshold for ICU transfer or Trial enrollment

Death rate may vary along time…
What is related to acute inflammation?
What is related to comorbidity?
0 1 2 3 4 5 6 7
0.0
0
.1
0.2
0
.3
0.4
Days
Pro
bab
ility
of
de
ath
Low IL6 n = 481
High IL6 n = 481
P value < 0.001
N = 989 patients in septic shock
0 1 2 3 4 5 6 7
0.0
0
0.0
5
0.1
0
0.1
5
0.2
0
0.2
5
0.3
0
Days P
rob
abili
ty o
f d
eat
h Low comorbidities n = 392
High comorbidities n = 566
P value < 0.001

10 15 20 25
0.0
0
0.0
5
0.1
0
0.1
5
0.2
0
0.2
5
0.3
0
Days
Pro
bab
ility
of
de
ath
Low IL6 n = 434
High IL6 n = 369
P value = 0.96
7
N = 989 patients in septic shock After Day 7
10
15 20 25
0.0
0
0.0
5
0.1
0
0.1
5
0.2
0
0.2
5
0.3
0
Days P
rob
abili
ty o
f d
eat
h
Low comorbidities n = 347
High comorbidities n = 453
P value < 0.001
7

0 5 10 15 20 25
0.0
0
.1
0.2
0
.3
0.4
0
.5
0.6
Days
Pro
ba
bil
ity o
f d
ea
th
Low Il6/Low comorbidities n=167
Low IL6/High comorbidities n=297
High Il6/Low comorbidities n=215
High IL6/High comorbidities n=253
P value < 0.001
N = 989 patients in septic shock

Yende et al. AJRCCM 2014


Show an increasing nonheritable
influence on many variables with age, suggest
strongly that many if not most of the less
heritable traits that we measure here in our
mostly adult population may be much more heritable if measured in young children.


Tolsma et al.Chest 2014
Multivariate analysis Death at D28
HR 95% CI P-value

Galbois et al. Crit Care Med 2014



Infections + Systemic inflammation
Remove of bacteria or bacterial products
Neutralyze antigenes
Immune interventions
AB early given Remove nidus
Toraymixin Plasmapheresis
Anti TLR4 SuperAG antagonist
Thrombomoduline Lactoferrine AB anti TNF Boost of immuno adaptative phase (IL-7)
the worldwide sepsis market was valued at
$5 billion in 2010 and is expected to
grow by 50% over the next five years.

Damaged-associated molecular patterns
- Necrotic cells DAMPs
- Criteria for DAMPs
- Alone should induce biological response without contamination (PAMPs = 0)
- Being efficient at physiol [ ]
- Their blockade inhibates their action

Survivors of hospitalization for community-acquired pneumonia are at increased risk
of cardiovascular events, repeated infections, and death in the following months.
But the cause is unknown…Early and long-lasting mechanisms?

Jonathan Cohen, Nature 2002
Fluid is given for filling Cvasc system improving circulation induce « shear stress »
But it is also diluting factors diluting cells changing the physical environment The QS might be: ARE THESE FLUID NEUTRAL FOR CELL PHENOTYPE?

Neutrophil crawling. Neutrophils usually transmigrate at endothelial cell–cell junctions, to which they actively crawl
Migrating neutrophils
actively choose sites of transmigration.

Neutrophil transmigration.
In order to leave the vasculature, neutrophils must first cross the endothelium,
which takes 2–5 minutes, and then the basement membrane, which takes longer (5–15 minutes
Requires integrins and CAMs (ICAM1, ICAM2 and vascular cell adhesion protein 1 (VCAM1))
as well as different junctional proteins, including platelet/endothelial cell adhesion
molecule 1 (PECAM1;
Neutrophils harbour specific groups of proteases — such as MMPs (for example, MMP9)
or serine proteases (for example, neutrophil elastase) — that have enzymatic activity against ECM molecules.
Although it is tempting to conclude that the neutrophil ‘cuts’ its way through the
basement membrane, to date neither genetic nor pharmacologic inhibition has conclusively demonstrated this.

Impact of the tissue on neutrophil recruitment
These resident cells are alerted by PAMPs and/or DAMPs11 that trigger PRRs, such as
TLRs, NOD-like receptors (NLRs), C-type lectin receptors (CLRs) and RIG-I-like receptors (RLRs).
A recent study has shown the interplay between infection and sterile inflammation by the
expression of macrophage-inducible C-type lectin (MINCLE; also known as CLEC4E) in response to LPS (of bacterial origin), which then binds SIN3-associated polypeptide p130 (SAP130) released from dead cells (sterile stimulus), initiating neutrophil recruitment into damaged tissue.
iNKT cells can produce pro-inflammatory or anti-inflammatory stimuli depending on the
nature of the stimulus they receive iNKT cells were shown to limit neutrophil recruitment to liver and, as such, prevent subsequent neutrophil-mediated damage of this organ.
Is it then possible for a neutrophil to distinguish between infectious and sterile inflammation?
Neutrophils seem to be strongly attracted to either type of inflammation; different neutrophil types (pro-inflammatory versus pro-resolving) might be recruited.

Crit Care Med 2006

• LPS complex has at least 3 components:
CD14, TLR4, and MD-2.
• TLR4 interacts with CD14. Another
protein MD-2 is required for TLR4-
mediated recognition of LPS
• TLR4 and MD-2 are constitutively
associated with each other, CD14 is
presumably recruited after binding LPS
• Very limited informations about allelic
variants of human toll genes and impact on
susceptibility to infection
The signalisation

• PAMP = pathogen-associated molecular pattern
• Proteins from pathogens are processed in the lysosomes to generate antigenic peptides, which form a complex with MHC class II on the surface of MQ, recognized by T cell receptors
ANTIGENE PRESENTING CELLS

Cell death and inflammation. - Necrotic cell death DAMPs receptors on
leukocytes + prod of pro-inflam cytokines (IL-1).
- Other molecules proteases; hydrolases act on EC
components + mediators (complement
fragments) or DAMPs prod of pro-inflam
cytokines by host cells.
- Pro-inflam mediators local vascular
endothelium ‘leaky’, attracts neutrophils and
monocytes/macrophages soluble (antibody)
and cellular defences in the tissue



alterations in microcirculatory flow hTransit Time for cells
trigger an oxidative Outburst in a paracrine fashion cell cycle arrest TIMP-2; IGFBP-7

PROWESS-SHOCK
Percent in study hospital
@ 28d:
DrotAA 305
(49%)
Placebo 279
(43%)
Ranieri et al NEJM 2012

Payen et al, Crit Care Med 2009 Vol. 37, No. 3
Comparison: conventional therapy vs conventional therapy + CVVH (25ml/kg/h)
Inclusion within 24 hours after meeting the inclusion criteria • Conventional treatment: treatment decided by the physician in charge
• HF treatment: CVVH started within 24 hrs for at least 96 hrs
Primary end point: reduction of number and duration of sepsis-induced organ failure at day 14
Secondary end point:
mortality at day 14;
withdrawal of catecholamines infusion and
length of mechanical ventilation

Primary end point
Evolution of SOFA score in the 2 groups:
SOFA was compared to Day 0. A positive value indicates a maintenance
or a deterioration
Log Rank test: Chi2 : 8.73; p<0.003 HF group
CT group

Payen et al, Crit Care Med 2009 Vol. 37, No. 3

What means heterogeneity?
related to « physiological reserve »
related to immune status
related to site of infection
related to the type of bacteria
related to delay for treatment
related to genetic susceptibility
others…

Anti TLR4 – Anti EDTX



2013
Expression of CD11b/CD18 ROS (Bedside?)
Tissue damage

Biomarker guided therapy quick test