Embed Size (px)
Citation preview

OTOLOGY
Sequence of vestibular deficits in patients with noise-inducedhearing loss
Chia-Chen Tseng • Yi-Ho Young
Received: 3 March 2012 / Accepted: 2 November 2012 / Published online: 10 November 2012
� Springer-Verlag Berlin Heidelberg 2012
Abstract This study utilized audiometry, and cervical
vestibular-evoked myogenic potential (cVEMP), ocular
VEMP (oVEMP) and caloric tests to investigate the
sequence of vestibular deficits in patients with noise-induced
hearing loss (NIHL). Thirty patients with NIHL underwent
an inner ear test battery. Another 30 normal controls with
age- and sex-matched were included for comparison. The
abnormal percentages of the audiometry, and cVEMP,
oVEMP and caloric tests were 100, 70, 57 and 33 % in NIHL
patients, which showed significant differences from 13, 13, 7
and 3 % in normal controls, respectively. A significantly
decreasing trend among the four tests, with the sequence of
damage from the cochlea, followed by the saccule, utricle,
and semicircular canals was noted in NIHL patients, but not
in normal controls. In conclusion, the decreasing order of
abnormal percentages in the function of the cochlea, saccule,
utricle and semicircular canals after chronic noise exposure
further supports that the pars inferior (cochlea and saccule) is
more vulnerable to noise exposure than the pars superior
(utricle and semicircular canals).
Keywords Cervical vestibular-evoked myogenic
potential � Inner ear monitoring system � Noise-induced
hearing loss � Ocular vestibular-evoked myogenic potential
Introduction
Extreme noise is a well known cause of cochlear damage
leading to temporary or permanent hearing loss [1].
Conversely, vestibular damage by noise has less been
investigated [2], possibly because vestibular deficits often
subside via central compensation. Occasionally, some
individuals experience vertigo or imbalance when exposed
to intense impulse noise. This condition, known as the
Tullio phenomenon, arises from vestibular activation in
response to acoustic stimulation, especially when the lab-
yrinth is opened, such as in the case of superior canal
dehiscence [3]. In addition to semicircular canal damage,
transmission of impulse noise from a gunshot may cause
the otoconia to detach from the otolithic organs, resulting
in paroxysmal vertigo after repeated exposure [4].
Acoustic trauma such as saccular damage from chronic
exposure to very high intensity noise can cause abnormal
vestibular-evoked myogenic potentials (VEMPs) [5]. In
guinea pigs, the recovery of VEMP from damage by short-
term noise exposure occurs before the hearing threshold is
restored [6]. Thus, noise exposure can cause the saccule to
exhibit temporary or permanent functional loss resembling
hearing threshold shifts. However, whether noise affects
the utricular macula remains unexplored.
Recently, VEMP can also be recorded from extraocular
muscles, termed ‘‘ocular’’ VEMP (oVEMP), which is
thought to arise from the otolithic macula, via superior
vestibular nerve, along the crossed vestibulo-ocular reflex
(VOR), and recorded on the extraocular muscles [7, 8].
Therefore, VEMPs recorded from the neck muscles via
sacculo-collic reflex are now termed ‘‘cervical’’ VEMPs
(cVEMPs). Through bone-conducted vibration (BCV)
stimuli, Yang et al. [9] have recently established an animal
model of oVEMP in guinea pigs, which sets the stage for
investigating the pathophysiology of utricular disorders.
Thus, the inner ear function can be completely evaluated
via an inner ear test battery including audiometry, and
cVEMP, oVEMP, and caloric tests. This study used the
C.-C. Tseng � Y.-H. Young (&)
Department of Otolaryngology, National Taiwan University
Hospital, 1, Chang-Te St., Taipei, Taiwan
e-mail: [email protected]
123
Eur Arch Otorhinolaryngol (2013) 270:2021–2026
DOI 10.1007/s00405-012-2270-6

inner ear test battery to investigate the vestibular deficits in
patients with noise-induced hearing loss (NIHL).
Subjects and methods
Subjects
A total of 30 patients with NIHL (26 males and 4 females,
aged 22–64 years, mean 48 years) were enrolled in this
study. The diagnostic criteria of NIHL were based on
American College of Occupational and Environmental
Medicine (ACOEM) guidelines [10]. Briefly, the principal
characteristics of NIHL are as follows:
1. Sensorineural hearing loss affects hair cells in the inner
ear.
2. Usually, symmetrical bilateral hearing loss.
3. Initially, ‘‘notching’’ of the audiogram at 3, 4 or 6 kHz,
with recovery at 8 kHz.
4. Usually, low-tone limits are approximately 40 dBHL,
and high-tone limits are approximately 75 dBHL.
5. Hearing loss reaches maximal after approximately
10–15 years of exposure.
6. No significant further progression of hearing loss
occurs after termination of noise exposure.
7. Continuous noise exposure is more damaging than
interrupted noise exposure.
Excluding criteria consisted of subjects with previous ear
disorders, systemic diseases, aged [65 years, receiving
ototoxic reagents, and lacking notched audiogram. The
occupational environments for the participants included steel
factory in seven, construction in six, electronics plant in four,
telecom industry in three, textile factory in two, commercial
ship in two, railway in two, wood shop in two and others in
two. The years of work history in these 30 NIHL patients
were 1–19 years in 10 patients, 20–29 years in 9 patients, and
[30 years in 11 patients. All patients received otoscopy first,
followed by audiometry, caloric, oVEMP and cVEMP tests.
Another 30 normal controls (26 males and 4 females,
aged 24–64 years, mean 48 years) without noise exposure
were tested in the same paradigm for comparison.
Caloric test
Bithermal caloric test was conducted with electronystag-
mographic (ENG) recordings (Nagashima, OK-5, Tokyo,
Japan). Canal paresis was defined as a greater than 25 %
difference between maximum slow phase velocity mea-
surements for each ear, when compared with the sum of
slow phase velocities from each ear. If cold water failed to
elicit caloric response, the subject underwent ice water
(0 �C, 10 mL) caloric test.
oVEMP test
The subject was in a sitting position. Surface potentials,
predominantly electromyographic (EMG) activities, were
recorded (Smart EP 3.90, Intelligent Hearing Systems,
Miami, FL, USA). Two active electrodes were placed around
1 cm below the center of the two lower eyelids. The other
two reference electrodes were positioned about 1–2 cm
below the active ones, and one ground electrode was placed
on the sternum. During recording, the subject was instructed
to look upward at a small fixed target[2 m from the eyes,
with a vertical visual angle of approximately 30� above
horizontal. The EMG signals were amplified and bandpass
filtered between 1 and 1,000 Hz. The input signal was a half
cycle 500 Hz sine wave, driven by a custom amplifier. The
drive voltage was adjusted and fixed to produce a peak force
of 15 N, about 128 dB force level (FL) from the vibrator, as
measured by an artificial mastoid (model 4930, Bruel &
Kjaer P/L, Denmark). Notably, the reference levels for air
and bone-conducted sound (0 dB) are defined differently.
For sound in air, 0 dB sound pressure level (SPL) is defined
as a pressure (20 lP), for bone conduction 0 dB SPL is
defined as a force (1 lN) [11]. The operator held the vibrator
by hand and delivered a repeatable tap with little pressure on
the subject’s skull at Fz, with the stimulation rate of 5/s. The
duration of analysis of each response was 50 ms, and 30
responses were averaged for each run [12].
The initial negative-positive biphasic waveform com-
prised peaks nI and pI. Consecutive runs were performed to
confirm the reproducibility of peaks nI and pI, and oVEMPs
were then deemed to be present. Conversely, oVEMPs were
deemed to be absent when the biphasic waveform was not
reproducible. At our laboratory, the norm for the latency of
peak nI was 11.4 ± 0.8 ms. Those with the nI latency
[13.0 ms were defined as delayed response. The asymmetry
ratio (%) was defined as the difference of the amplitude
nI–pI on each ear divided by the sum of amplitude nI–pI of
both ears, that is, (larger amplitude-smaller amplitude/larger
amplitude ? smaller amplitude) 9 100. Those with asym-
metry ratio[40 % were interpreted as reduced responses.
cVEMP test
Each subject was in a supine position. Two active elec-
trodes were placed on the upper half of the sternocleido-
mastoid (SCM) muscles; one reference electrode was
positioned on the suprasternal notch, and a ground elec-
trode was situated on the forehead. The acquisition settings
were similar to oVEMP test, except that the vibrator
delivered a repeatable tap on the subject’s head at inion.
The reason for using BCV tapping to elicit cVEMPs is that
the BCV stimuli evoke neural responses similar to those
evoked by ACS stimuli. Most, but not all, otolithic
2022 Eur Arch Otorhinolaryngol (2013) 270:2021–2026
123

irregular neurons activated by ACS stimulation can also be
activated by BCV stimulation [13]. Thus, substituting BCV
mode for ACS mode to elicit both oVEMPs and cVEMPs,
especially in ‘‘mass detection’’, may increase the simplic-
ity, speed and convenience of VEMP testing.
To measure background muscle activity, subjects were
given feedback of the level of EMG activity in their SCM
muscles during data collection and were required to keep a
background muscle activity of at least [50 lV. The sub-
jects elevated their heads during testing. A total of 50
responses were averaged and recorded bilaterally.
The first positive and second negative polarities of
biphasic waveform were termed waves p13 and n23,
respectively. Consecutive runs were performed to confirm
the reproducibility of peaks p13 and n23, and cVEMP
responses were termed present. The latencies of p13, n23,
and amplitude p13–n23 were measured. At our laboratory,
the norm for the latency of p13 was 14.4 ± 1.3 ms, and we
defined when the latency of peak p13 exceeding 17.0 ms as
delayed cVEMPs. In addition, those with asymmetry ratio
[33 % were defined as reduced response.
Statistical methods
Comparison of the mean hearing levels of each frequency
between the two groups was conducted by unpaired t test.
The abnormal rates of each test between two groups were
compared by Fisher’s exact test. The abnormal percentages
in the inner ear test battery were compared with Cochrane
Q test. A difference of p \ 0.05 is considered significant.
This study was approved by the institutional review board,
and each subject signed the informed consent to participate.
Results
NIHL group
Clinical manifestation consisted of hearing loss in all
30 NIHL patients, followed by tinnitus in 19 (63 %),
rotational vertigo in 14 (47 %), nausea/vomiting in 13
(43 %), headache in 10 (33 %) and aural fullness in four
patients (13 %).
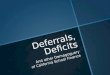
Audiometry revealed bilateral sensorineural hearing loss
in all patients (100 %). The mean hearing thresholds of
each frequency from 250 to 8,000 Hz are shown on
Table 1. There were no significant side-differences in
terms of mean hearing threshold of each frequency
(p [ 0.05, paired t test). The mean hearing threshold of
4,000 Hz revealed the worst hearing threshold compared
with that of other frequencies regardless of whether the
right or left ear was analyzed (p \ 0.01, paired t test),
leading to a 4-kHz-notched audiogram (Fig. 1). The latter
may help to exclude the possibility of Meniere’s disease,
although Meniere’s disease has its diagnostic criteria pro-
posed by American Academy of Otolaryngology, Head and
Neck Surgery in 1995 [14].
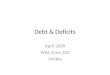
The cVEMP test displayed normal responses in 30 ears
and abnormal responses in 30 ears (50 %), consisting of
reduced responses in 2 ears, delayed responses in 6 ears,
and absent response in 22 ears (Fig. 2). The oVEMP test
showed normal responses in 40 ears and abnormal
responses in 20 ears (33 %), including reduced and absent
responses in 9 and 11 ears, respectively (Fig. 2). The
caloric test demonstrated normal responses in 45 ears and
abnormal responses in 15 ears (25 %), including absent
response in 1 ear and canal paresis in 14 ears.
To compare the inner ear deficits, a damaged ear on
either side was considered abnormal. Thus, the percentages
of abnormalities observed in the audiometry, cVEMP,
oVEMP, and caloric tests of the 30 NIHL patients were
100, 70, 57 and 33 %, respectively, revealing a signifi-
cantly decreasing trend among the four tests (p \ 0.001,
Cochrane Q test, Table 2).
Control group
The mean hearing thresholds of each frequency from 250 to
8,000 Hz in the control group were demonstrated in Table 1.
Compared with NIHL group, significant differences existed
Table 1 Comparison of mean hearing thresholds in noise-induced hearing loss (NIHL) patients versus normal controls
Group n 250 Hz 500 Hz 1,000 Hz 2,000 Hz 4,000 Hz 8,000 Hz
R ear
NIHL 30 12 ± 9 15 ± 10 20 ± 13 22 ± 15 44 ± 18 33 ± 20
Control 30 14 ± 6 14 ± 6 15 ± 8 14 ± 8 17 ± 8 20 ± 12
p value NS NS NS \0.05 \0.01 \0.01
L ear
NIHL 30 12 ± 7 16 ± 7 18 ± 9 19 ± 12 42 ± 15 29 ± 14
Control 30 13 ± 6 14 ± 7 15 ± 8 15 ± 8 16 ± 8 21 ± 14
p value NS NS NS \0.05 \0.01 \0.01
Data are expressed as mean ± SD dBHL, p value: unpaired t test
Eur Arch Otorhinolaryngol (2013) 270:2021–2026 2023
123

in the mean hearing thresholds at the frequencies of 2,000,
4,000 and 8,000 Hz regardless of right or left ear was ana-
lyzed (p \ 0.05, unpaired t test, Table 1; Fig. 1).
Hearing loss is defined positive when the hearing
threshold of any frequency is [25 dBHL. Accordingly, 4
(13 %) of the 30 normal controls had hearing loss. The
percentages of abnormalities in audiometry, and cVEMP,
oVEMP and caloric tests in 30 normal controls were 13,
13, 7 and 3 %, respectively, which differed significantly
when compared with those of the NIHL group (p \ 0.001,
Table 2). Unlike NIHL group, no significantly decreasing
trend among the four tests was observed in the control
group (p [ 0.05, Cochrane Q test, Table 2).
Discussion
The mechanism of NIHL can be classified into two major
categories: direct mechanical trauma and metabolic change
to the cochlea [1]. When the noise intensity is [140 dB,
e.g., the noise produced by an explosion, NIHL results
from mechanical trauma alone. In contrast, workplace
noise damaging the cochlea is mainly due to metabolic
stress [15], leading to the production of reactive oxygen
species (ROS), reactive nitrogen species (RNS) and other
free radical molecules in the cochlea. These ROS are quite
capable of inducing cochlear damage as well as loss of
function by destroying DNA and cell membranes, which
Fig. 1 The mean hearing thresholds from 30 NIHL patients (solid circle) versus 30 normal controls (hollow circle). A 4-kHz-notched audiogram
is observed in NIHL patients, but not in normal controls
Fig. 2 Clear oVEMPs and cVEMPs are observed in a normal control (male, 38 years), while clear oVEMPs but absent cVEMPs are noted in a
NIHL patient (male, 48 years)
2024 Eur Arch Otorhinolaryngol (2013) 270:2021–2026
123

up-regulates apoptotic cell death genes [16]. For the ves-
tibular part, the saccule in lower species such as amphib-
ians and fish acts as an acoustic receptor. Hence, loud noise
damaging the hair cells of cochlea may also affect the
saccular macula [6]. Animal studies of guinea pigs exposed
to high level noise shows that the pars inferior (cochlea and
saccule) is the most susceptible to damage whereas the pars
superior (semicircular canals and utricle) remains intact
[17].
The saccular neurons have a strong projection to neck
muscles and a weak projection to the oculomotor system,
while neural connections in the sacculo-ocular system are
relatively weak compared with neural connections in the
utriculo-ocular and sacculo-collic reflexes [13]. Thus,
based on the hypothesis of ‘‘efferent specificity’’ proposed
by Curthoys [8], oVEMPs by bone-conducted vibration
primarily originate from the utricular macula, whereas
cVEMPs originate from the saccular macula. Thereby, all
the inner ear end organs can be completely evaluated via
audiometry, and cVEMP, oVEMP, and caloric tests. In this
study, high abnormal rates in hearing (100 %) and cVEMP
(70 %) tests, and low abnormal rates in oVEMP (57 %)
and caloric (33 %) tests in NIHL patients, further support
that the pars inferior (cochlea and saccule) is more vul-
nerable to noise exposure than the pars superior (utricle and
semicircular canals), compatible with the animal experi-
ment [17].
As the superior vestibular nerve innervates the lateral
and superior semicircular canals, utricular macula, and the
‘‘hook’’ region of the saccular macula; while the inferior
vestibular nerve supplies the posterior semicircular canal
and the elongated ‘‘shank’’ region of the saccular macula,
one may argue that saccular lesion may cause abnormal
responses in both oVEMP and cVEMP tests. Likewise, the
BCV mode may activate the utricular afferents leading to
increased cVEMP amplitude. Nevertheless, this possibility
can be neglected since the contribution of utricular affer-
ents to the SCM muscles and that of saccular afferents to
the extraocular muscles are limited [13].
Morphologically, the cochlear and vestibular receptors
have a similar embryologic origin and share a common
basic structure, namely, a hair cell synapsing with a pri-
mary sensory neuron. However, the vulnerability of the
pars superior differs from that of the pars inferior, probably
due to the existence of membrane limitans.
The membrane limitans, first described by De Burlet
[18] in 1920, serves as a barrier between the pars superior
and pars inferior, protecting the pars superior against
mechanical trauma from fluid pressure. In addition, this
membrane may also prevent or delay toxic substances from
pars inferior to pars superior [19].
In addition to noise effect, aging process may play
another role for causing vestibular deficit, since the ves-
tibular system deteriorates with age. Thus, comparison of
NIHL patients from normal controls was conducted. The
percentages of abnormalities in audiometry, cVEMP,
oVEMP and caloric tests in normal controls were 13, 13, 7
and 3 %, which were significantly less than 100, 70, 57 and
33 % in NIHL group, respectively (Table 2), indicating
that aging effect does not provide a major role in causing
vestibular deficits in NIHL patients.
Further, loss of the hair cell population in the crista
ampullaris (40 %), saccular macula (24 %) and utricular
macula (21 %) were noted in subjects with increasing age
after 40 years [20]. Restated, the cristae showed a more
pronounced degeneration than the maculae, while both
utricular and saccular maculae exhibited the same degree
of degeneration. In contrast, the declining sequence of the
saccule, utricle and semicircular canals in NIHL patients is
opposed from that in aging process, further indicates that
vestibular deficit in NIHL patients is mostly due to chronic
noise exposure. Moreover, aging process is usually a
bilateral phenomenon, while some cases of NIHL showed
asymmetrical audiovestibular deficits, probably because of
the asymmetric sources of noise related to the victim’s
position in a factory [10].
Okuno and Sando [21] studied 22 temporal bones of
Meniere’s disease and reported that next to the cochlea
(100 %), the saccule (77 %) is the second most frequent
site for hydrops formation. Conversely, hydrops are less
common in the utricle (50 %) and semicircular canals
(27 %). Notably, the decreasing order of abnormal per-
centages in the function of the cochlea, saccule, utricle and
semicircular canals after chronic noise exposure mimics
the declining sequence of hydrops formation in the tem-
poral bones and physiological testing [22], which further
suggests that the endolymphatic hydrops can be induced by
noise exposure, as evidenced in animal experiments [23].
Table 2 Comparison of inner ear deficits in noise-induced hearing
loss (NIHL) patients versus normal controls
NIHL patients Normal controls p value
Case no. 30 30
Gender (M/F) 26/4 26/4
Age (Years) 48 ± 10 48 ± 12 0.928a
Abnormal rates in
Audiometry 30/30 (100 %) 4/30 (13 %) \0.001c
cVEMP test 21/30 (70 %) 4/30 (13 %) \0.001c
oVEMP test 17/30 (57 %) 2/30 (7 %) \0.001c
Caloric test 10/30 (33 %) 1/30 (3 %) \0.001c
p value \0.001b [0.05b
a Non-paired t testb Cochrane Q testc Fisher’s exact test
Eur Arch Otorhinolaryngol (2013) 270:2021–2026 2025
123

Based on the clinical and pathological results, Schukn-
echt and Gulya [24] developed a classification of the
endolymphatic hydrops including embryopathic, inflam-
matory, traumatic, and idiopathic types. The pathogenesis
of post-traumatic endolymphatic hydrops is attributable to
the pressure striking force causing direct injury to the
labyrinthine membranous duct [25]. This kind of hydrops
may not progress, and subside or arrest in a short period of
time after injury. Conversely, an idiopathic endolymphatic
hydrops i.e., Meniere’s disease may present repeated pro-
gressive dilatation and rupture of the endolymphatic duct.
Conclusion
The decreasing order of abnormal percentages in the
function of the cochlea, saccule, utricle and semicircular
canals after chronic noise exposure further supports that the
pars inferior (cochlea and saccule) is more vulnerable to
noise exposure than the pars superior (utricle and semi-
circular canals).
Acknowledgments Grant no. NSC 99-2314-B002-049-MY3 from
National Science Council, Taipei, Taiwan.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Lim DJ (1986) Effects of noise and ototoxic drugs at the cellular
level in the cochlea; a review. Am J Otolaryngol 7:73–99
2. Shupak A, Bar-El E, Podoshin L, Spitzer O, Gordon CR,
Ben-David J (1994) Vestibular findings associated with chronic
noise induced hearing impairment. Acta Otolaryngol 114:579–585
3. Halmagyi GM, Curthoys IS, Colebatch JG, Aw ST (2005)
Vestibular responses to sound. Ann NY Acad Sci 1039:54–67
4. Bruno E, Napolitano B, Di Girolamo S, de Padova A,
Alessandrini M (2007) Paroxysmal positional vertigo in skeet
shooters and hunters. Eur Arch Otorhinolaryngol 264:381–383
5. Wang YP, Young YH (2007) Vestibular evoked myogenic
potentials in chronic noise-induced hearing loss. Otolaryngol
Head Neck Surg 137:607–611
6. Hsu WC, Wang JD, Lue JH, Day AS, Young YH (2008) Physi-
ological and morphological assessment of the saccule in guinea
pigs after noise exposure. Arch Otolaryngol Head Neck Surg
134:1099–1106
7. Rosengren SM, Todd NP, Colebatch JG (2005) Vestibular-
evoked extraocular potentials produced by stimulation with bone-
conducted sound. Clin Neurophysiol 116:1938–1948
8. Curthoys IS (2010) A critical review of the neurophysiological
evidence underlying clinical vestibular testing using sound,
vibration and galvanic stimuli. Clin Neurophysiol 121:132–144
9. Yang TH, Liu SH, Wang SJ, Young YH (2010) An animal model
of ocular vestibular-evoked myogenic potential in guinea pig.
Exp Brain Res 205:145–152
10. ACOEM Noise and Hearing Conservation Committee (2003)
ACOEM evidence-based statement: noise-induced hearing loss.
J Occup Environ Med 45(6):579–581
11. Welgampola MS, Rosengren SM, Halmagyi GM, Colebatch JG
(2003) Vestibular activation by bone conducted sound. J Neurol
Neurosurg Psychiatry 74:771–778
12. Su CH, Young YH (2011) Differentiating between cerebellar and
brainstem lesions with ocular vestibular-evoked myogenic
potential test. Eur Arch Otorhinolaryngol 268:923–930
13. Curthoys IS (2012) The interpretation of clinical tests of
peripheral vestibular function. Laryngoscope 122:1342–1352
14. (1995) Committee on hearing and equilibrium guideline for the
diagnosis and evaluation of therapy in Meniere’s disease. Oto-
laryngol Head Neck Surg 113(3):181–185
15. Kopke RD, Coleman JK, Liu J, Campbell KC, Riffenburgh RH
(2002) Enhancing intrinsic cochlear stress defenses to reduce
noise-induced hearing loss. Laryngoscope 112:1515–1532
16. Henderson D, Bielefeld EC, Harris KC, Hu BH (2006) The role
of oxidative stress in noise-induced hearing loss. Ear Hear 27(1):
1–19
17. McCabe BF, Lawrence M (1958) The effects of intense sound on
the non-auditory labyrinth. Acta Otolaryngol 49:147–157
18. De Burlet HM (1920) Der perilymphatische Baum des Meer-
schweinchenohres. Anat Anz 53:302–315
19. Hara M, Kimura RS (1993) Morphology of the membrane limi-
tans. Ann Otol Rhinol Laryngol 102:625–630
20. Rosenhall U (1973) Degenerative patterns in the aging human
vestibular neuroepithelia. Acta Otolaryngol 76:208–220
21. Okuno T, Sando I (1987) Localization, frequency and severity of
endolymphatic hydrops and the pathology of the labyrinthine
membrane in Meniere’s disease. Ann Otol Rhinol Laryngol
96:438–445
22. Huang CH, Wang SJ, Young YH (2011) Localization and prev-
alence of hydrops formation in Meniere’s disease using a test
battery. Audiol Neurotol 16:41–48
23. Kumagami H (1992) Endolymphatic hydrops induced by noise
exposure. Auris Nasus Larynx 19:95–104
24. Schuknecht HF, Gulya AJ (1983) Endolymphatic hydrops: an
overview and classification. Ann Otol Rhinol Laryngol 106
(suppl):1–20
25. Shea JJ Jr, Ge X, Orchik DJ (1995) Traumatic endolymphatic
hydrops. Am J Otol 16:235–240
2026 Eur Arch Otorhinolaryngol (2013) 270:2021–2026
123