Embed Size (px)
Citation preview

SR
R
*‡
P
BbnoirrDr(bDmitstsvaA�algtrpoits
TacflaatpflTts
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:729 –735
erious Adverse Events With Infliximab: Analysis of Spontaneouslyeported Adverse Events
ICHARD A. HANSEN,* GERALD GARTLEHNER,‡ GREGORY E. POWELL,§ and ROBERT S. SANDLER¶
Center for Pharmaceutical Outcomes and Policy, Division of Pharmaceutical Outcomes and Policy, School of Pharmacy, University of North Carolina at Chapel Hill;University of North Carolina–Cecil G. Sheps Center for Health Services Research§GlaxoSmithKline-Safety Evaluation and Risk Management, Global Clinical Safety &
harmacovigilance, Research Triangle Park, North Carolina; and ¶University of North Carolina–School of Medicine, Chapel Hill, North Carolinardwlstflsspeaaa3
edirtuncophaaaz
sEBimSM
ackground & Aims: Serious adverse events such asowel obstruction, heart failure, infection, lymphoma, andeuropathy have been reported with infliximab. The aimsf this study were to explore adverse event signals with
nfliximab by using a long period of post-marketing expe-ience, stratifying by indication. Methods: The relativeeporting of infliximab adverse events to the U.S. Food andrug Administration (FDA) was assessed with the public
elease version of the adverse event reporting systemAERS) database from 1968 to third quarter 2005. On theasis of a systematic review of adverse events, Medicalictionary for Regulatory Activities (MedDRA) terms wereapped to predefined categories of adverse events, includ-
ng death, heart failure, hepatitis, infection, infusion reac-ion, lymphoma, myelosuppression, neuropathy, and ob-truction. Disproportionality analysis was used to calculatehe empiric Bayes geometric mean (EBGM) and corre-ponding 90% confidence intervals (EB05, EB95) for ad-erse event categories. Results: Infliximab was identifieds the suspect medication in 18,220 reports in the FDAERS database. We identified a signal for lymphoma (EB05
6.9), neuropathy (EB05 � 3.8), infection (EB05 � 2.9),nd bowel obstruction (EB05 � 2.8). The signal for granu-omatous infections was stronger than the signal for non-ranulomatous infections (EB05 � 12.6 and 2.4, respec-ively). The signals for bowel obstruction and infusioneaction were specific to patients with IBD; this suggestsotential confounding by indication, especially for bowelbstruction. Conclusions: In light of this additional ev-
dence of risk of lymphoma, neuropathy, and granuloma-ous infections, clinicians should stress this risk in thehared decision-making process.
argeted immune modulators, commonly referred to asbiologic response modifiers or simply biologics, are a rel-
tively new category of medication used in the treatment ofertain types of immunologic and inflammatory diseases. In-iximab, the first of the biologics approved by the U.S. Foodnd Drug Administration (FDA), is a chimeric (mouse/human)nti–tumor necrosis factor (TNF)–� antibody that binds bothhe circulating and transmembrane forms of TNF-�, therebyreventing binding with the receptor.1,2 Infliximab is approvedor the treatment of rheumatoid arthritis, ankylosing spondy-itis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis.he general efficacy of infliximab has been well-established for
hese conditions; effect sizes are large and consistent across
tudies.The benefits of infliximab do not come without potentialisks. Infusion reactions, abdominal pain, nausea, headache,iarrhea, and infections are the most common adverse eventsith infliximab reported in clinical trials.3 Evidence in regard to
ong-term, rare, but serious adverse events is sparser. In aystematic review of potential harms with biologic agents,3
here was a potential increase in risk of serious infection, heartailure, demyelination, autoimmunity, bowel obstruction, andymphoma. These data were derived from a number of differentources, including clinical trials, observational studies, andpontaneous post-marketing adverse event reports. A recentlyublished systematic review and meta-analysis added to thevidence for malignancy and serious infection. On the basis of
pooled analysis of placebo-controlled trials of adalimumabnd infliximab,4 the pooled odds ratio for malignancy was 3.3nd for serious infection was 2.0 during a treatment period of–12 months.
The purpose of this study was to further explore adversevent signals with infliximab. We used published evidence toefine, a priori, specific adverse events of concern with inflix-
mab.3 We also searched for adverse event signals not previouslyeported. Our analysis focused on infliximab because at theime it was the only biologic product on the market labeled forse in IBD. We included a broad spectrum of bowel-related andon-bowel–related conditions in our analysis to avoid potentialonfounding by indication. This is especially important becausef an increased risk of infection and certain malignancies inatients with rheumatoid arthritis.5–7 Although other studiesave documented adverse events with infliximab, our analysis isn important contribution because it uses the most recentlyvailable FDA adverse event reporting system (AERS) databasend targets major events by using an a priori defined categori-ation system.
Abbreviations used in this paper: AERS, adverse event reportingystem; CI, confidence interval; EBGM, empiric Bayes geometric mean;B05, empiric Bayes lower 90% confidence bound; EB95, empiricayes upper 90% confidence bound; FDA, U.S. Food and Drug Admin-
stration; MedDRA, Medical Dictionary for Regulatory Activities; MGPS,ulti-item gamma poisson shrinker; SRS, Spontaneous Reporting
ystem; TNF, tumor necrosis factor; WebVDME, Web Visual Dataining Environment.
© 2007 by the AGA Institute1542-3565/07/$32.00
doi:10.1016/j.cgh.2007.02.016

eAptpdrrasmbptpmhi
boeimbnemtnncitmcidie
saErmddwtrtt9tlbn
eMtTtcfievigrsc
DIqiedthiarea
ddw((i31nwifauWsn2n
E32as
730 HANSEN ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 5, No. 6
MethodsWe assessed the relative reporting of infliximab adverse
vents to the FDA by using the public release version of theERS database. AERS is a post-marketing safety database com-osed of spontaneous adverse event reports to the FDA’s Spon-aneous Reporting System (SRS) before October 1997 and re-orts to AERS from November 1997 to present. The AERSatabase includes post-marketing adverse events spontaneouslyeported from U.S. sources, serious and unlabeled spontaneouseports from non-U.S. sources, and serious, unlabeled, andttributable post-marketing clinical trial reports from allources. AERS receives reports from 2 principal sources; phar-
aceutical companies are required to report events that haveeen spontaneously reported to the company, and health careroviders and consumers can submit adverse event reports tohe FDA’s MedWatch program.8 As of December 2004, theublic release version of AERS contained approximately 2.6illion reports9 involving more than 2000 drugs. More than
alf of reports in AERS were reported after 1997, with approx-mately 90% reported since 1990.9
Disproportionality analysis was used to assess associationsetween infliximab and adverse events. This method comparesbserved adverse event counts to the count that would bexpected if occurrence of drugs and events in reporting werendependent. The expected adverse event count is derived by
ultiplying the sum of the number of reports that mentionoth the drug of interest and the event of interest and theumber of reports that mention the drug of interest but not thevent of interest by the sum of the number of reports thatention both the drug of interest and the event of interest and
he number of reports that mention the event of interest butot the drug of interest and dividing this number by the totalumber of reports. Taking the ratio of the observed to expectedount reflects a relative rate of reporting. We used the multi-tem gamma poisson shrinker (MGPS)10,11 to smooth the rela-ive rate value. The MGPS is an empirical Bayes data mining
ethod that uses data on all drugs and events in a database toompute relative reporting frequencies. To prevent confound-ng of drug-event associations and associations due to patientemographics or secular characteristics, MGPS internally strat-
fies on age, gender, and year of report and then computes anstimate of the relative rate.
The estimate of relative rate obtained with MGPS is thetatistic known as the empiric Bayes geometric mean (EBGM)nd corresponding 2-sided 90% confidence interval (CI) (EB05,B95). The EBGM values represent adjusted relative reportingates (observed/expected) after Bayesian shrinkage is applied to
inimize the variability that occurs in large, sparsely populatedatabases. An EBGM value of 5 is interpreted to mean that arug-event pair has been reported 5 times as frequently asould be expected if reports involving the drug and reports of
he event were independent (ie, no association). A high relativeeporting rate does not necessarily indicate a high incidence ofhe event or suggest a causal relationship between the drug andhe event. For purposes of signal detection, we applied a lower0% confidence bound (ie, EB05) �2 as a signal threshold. Thishreshold ensures with a high degree of confidence that regard-ess of the number of reports, a particular drug event pair iseing reported at least twice as often as it would be if there were
o association between the drug and the event.12 fBefore the analysis, we conducted a systematic review of adversevents with infliximab3 and mapped adverse event terms from the
edical Dictionary for Regulatory Activities (MedDRA) that wehought represented previously reported infliximab adverse events.his resulted in 8 general event categories of interest (Supplemen-
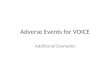
ary Table 1; see supplementary material online at www.ghjournal.org). For some categories such as infection, we chose tourther stratify the data because there were many heterogeneousnfections with signals. On the basis of the hypothesis that TNF isssential for granuloma formation and maintenance13–15 and pre-ious evidence documenting an increased risk of granulomatousnfections,16 we categorized infections as granulomatous and non-ranulomatous (Supplementary Table 2; see supplementary mate-ial online at www.cghjournal.org). We also looked at pathogen-pecific infections (Table 1) by mapping MedDRA terms to 26ommon pathogens.
The data mining methods were run by using Web Visualata Mining Environment (WebVDME) (Lincoln Technologies,
nc, Waltham, MA) for the period of 1968 through the thirduarter of 2005. Adverse event reports dating back to 1968 were
ncluded, even though infliximab was not yet on the market, tostablish the rate of reporting assuming events were indepen-ent from infliximab. We included all adverse events for whichhe reporter identified infliximab as suspect. Because infliximabas a number of indications (ie, rheumatoid arthritis, ankylos-
ng spondylitis, psoriatic arthritis, Crohn’s disease, and ulcer-tive colitis) and the condition being treated could be related toeported events, we stratified our analysis by condition. Wevaluated reports for IBD–Crohn’s disease or ulcerative colitis–nd other inflammatory conditions separately.
ResultsInfliximab appeared in 18,619 reports in the FDA AERS
atabase as a suspect or concomitant medication. Limiting theatabase to reports that identified infliximab as suspect only,e identified 18,220 reports. Of these reports, 2457 cases
13.5%) reported multiple suspect medications, and 15,76386.5%) cases reported infliximab as the only suspect drug; wencluded all of these reports in our analysis. Nearly 20% (N �378) of reports were for patients with IBD, roughly 55% (N �0,127) were for non-IBD indications, and 25% (N � 4715) didot identify an indication. Reports generally were for adults andere more common for women than men, with most reports
nvolving patients 46 –75 years of age. Although a denominatoror the distribution of infliximab use by gender and age is notvailable, previous reports suggest no differences in infliximabsers by gender and a general trend of decreasing use with age.17
ith unmapped MedDRA terms, initial inspection revealed thetrongest signals for histoplasmosis (EB05 � 23.9), dissemi-ated tuberculosis (EB05 � 23.5), listerial meningitis (EB05 �2.3), disseminated histoplasmosis (EB05 � 21.3), and lymphode tuberculosis (EB05 � 19.8).
For the mapped events of interest, we identified a signal (ie,B05 � 2) for lymphoma (EB05 � 6.9), neuropathy (EB05 �.8), infection (EB05 � 2.9), and bowel obstruction (EB05 �.8) (Figure 1). The signal for lymphoma was relatively strongnd consistent for IBD and non-IBD groups. The bowel ob-truction and infusion reaction signals were specific to reports
or IBD. A signal was not detected for the relationship between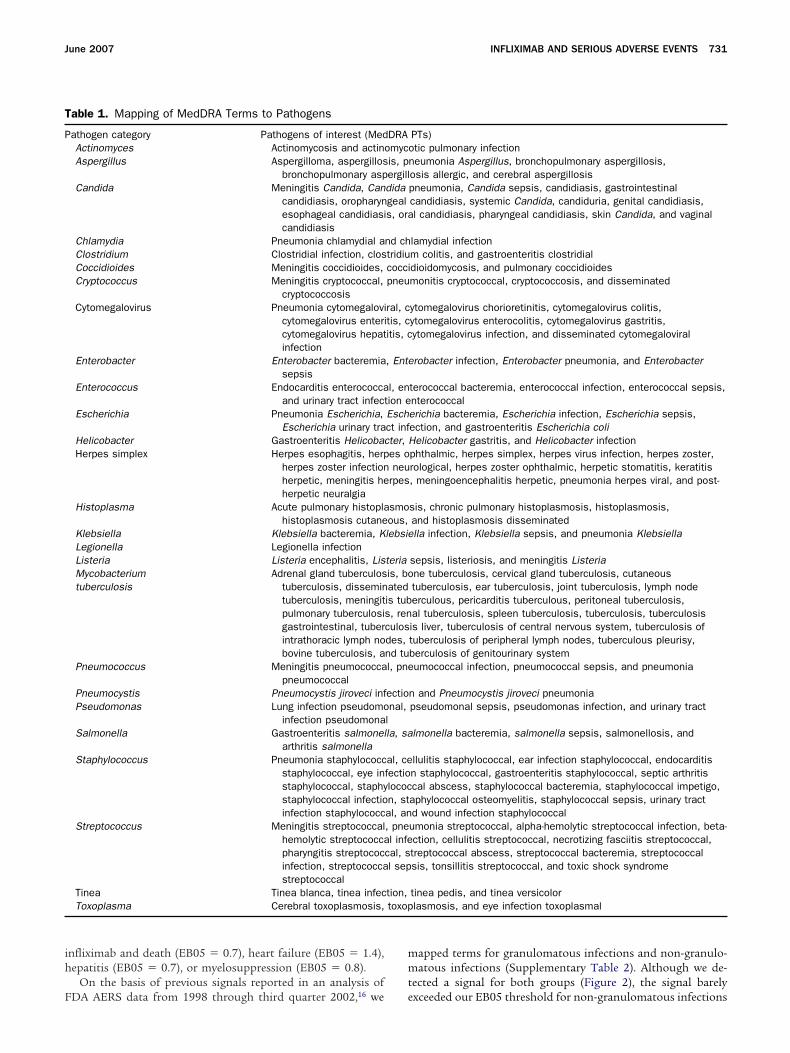
ih
F
mmt
T
P
toxop
June 2007 INFLIXIMAB AND SERIOUS ADVERSE EVENTS 731
nfliximab and death (EB05 � 0.7), heart failure (EB05 � 1.4),epatitis (EB05 � 0.7), or myelosuppression (EB05 � 0.8).
On the basis of previous signals reported in an analysis of
able 1. Mapping of MedDRA Terms to Pathogens
athogen category Pathogens of interest (MedActinomyces Actinomycosis and actinAspergillus Aspergilloma, aspergillos
bronchopulmonary aspCandida Meningitis Candida, Can
candidiasis, oropharynesophageal candidiasicandidiasis
Chlamydia Pneumonia chlamydial aClostridium Clostridial infection, closCoccidioides Meningitis coccidioides,Cryptococcus Meningitis cryptococcal,
cryptococcosisCytomegalovirus Pneumonia cytomegalovi
cytomegalovirus entericytomegalovirus hepatinfection
Enterobacter Enterobacter bacteremiasepsis
Enterococcus Endocarditis enterococcaand urinary tract infect
Escherichia Pneumonia Escherichia,Escherichia urinary tra
Helicobacter Gastroenteritis HelicobacHerpes simplex Herpes esophagitis, herp
herpes zoster infectionherpetic, meningitis heherpetic neuralgia
Histoplasma Acute pulmonary histoplahistoplasmosis cutane
Klebsiella Klebsiella bacteremia, KLegionella Legionella infectionListeria Listeria encephalitis, LisMycobacteriumtuberculosis
Adrenal gland tuberculostuberculosis, dissemintuberculosis, meningitpulmonary tuberculosigastrointestinal, tuberintrathoracic lymph nobovine tuberculosis, a
Pneumococcus Meningitis pneumococcapneumococcal
Pneumocystis Pneumocystis jiroveci infPseudomonas Lung infection pseudomo
infection pseudomonaSalmonella Gastroenteritis salmonel
arthritis salmonellaStaphylococcus Pneumonia staphylococc
staphylococcal, eye instaphylococcal, staphystaphylococcal infectioinfection staphylococc
Streptococcus Meningitis streptococcalhemolytic streptococcapharyngitis streptococinfection, streptococcastreptococcal
Tinea Tinea blanca, tinea infecToxoplasma Cerebral toxoplasmosis,
DA AERS data from 1998 through third quarter 2002,16 we e
apped terms for granulomatous infections and non-granulo-atous infections (Supplementary Table 2). Although we de-
ected a signal for both groups (Figure 2), the signal barely
PTs)otic pulmonary infectionneumonia Aspergillus, bronchopulmonary aspergillosis,osis allergic, and cerebral aspergillosispneumonia, Candida sepsis, candidiasis, gastrointestinalcandidiasis, systemic Candida, candiduria, genital candidiasis,l candidiasis, pharyngeal candidiasis, skin Candida, and vaginal
lamydial infectionm colitis, and gastroenteritis clostridialdioidomycosis, and pulmonary coccidioidesmonitis cryptococcal, cryptococcosis, and disseminated
ytomegalovirus chorioretinitis, cytomegalovirus colitis,ytomegalovirus enterocolitis, cytomegalovirus gastritis,ytomegalovirus infection, and disseminated cytomegaloviral
robacter infection, Enterobacter pneumonia, and Enterobacter
terococcal bacteremia, enterococcal infection, enterococcal sepsis,nterococcalerichia bacteremia, Escherichia infection, Escherichia sepsis,ection, and gastroenteritis Escherichia coliHelicobacter gastritis, and Helicobacter infectionphthalmic, herpes simplex, herpes virus infection, herpes zoster,rological, herpes zoster ophthalmic, herpetic stomatitis, keratitis, meningoencephalitis herpetic, pneumonia herpes viral, and post-
sis, chronic pulmonary histoplasmosis, histoplasmosis,and histoplasmosis disseminatedlla infection, Klebsiella sepsis, and pneumonia Klebsiella
sepsis, listeriosis, and meningitis Listeriane tuberculosis, cervical gland tuberculosis, cutaneoustuberculosis, ear tuberculosis, joint tuberculosis, lymph nodeerculous, pericarditis tuberculous, peritoneal tuberculosis,al tuberculosis, spleen tuberculosis, tuberculosis, tuberculosisis liver, tuberculosis of central nervous system, tuberculosis oftuberculosis of peripheral lymph nodes, tuberculous pleurisy,berculosis of genitourinary systemumococcal infection, pneumococcal sepsis, and pneumonia
n and Pneumocystis jiroveci pneumoniapseudomonal sepsis, pseudomonas infection, and urinary tract
lmonella bacteremia, salmonella sepsis, salmonellosis, and
llulitis staphylococcal, ear infection staphylococcal, endocarditisn staphylococcal, gastroenteritis staphylococcal, septic arthritiscal abscess, staphylococcal bacteremia, staphylococcal impetigo,aphylococcal osteomyelitis, staphylococcal sepsis, urinary tractd wound infection staphylococcalumonia streptococcal, alpha-hemolytic streptococcal infection, beta-ction, cellulitis streptococcal, necrotizing fasciitis streptococcal,treptococcal abscess, streptococcal bacteremia, streptococcalsis, tonsillitis streptococcal, and toxic shock syndrome
tinea pedis, and tinea versicolorlasmosis, and eye infection toxoplasmal
DRAomycis, pergilldidageals, ora
nd chtridiucoccipneu
ral, ctis, citis, c
, Ente
l, enion eEschct infter,es oneu
rpes
smoous,lebsie
teriais, boatedis tubs, renculosdes,nd tul, pne
ectional,
lla, sa
al, cefectiolococn, stal, an, pnel infe
cal, sl sep
tion,
xceeded our EB05 threshold for non-granulomatous infections
(ft
lA�E(2rP(
(tlOsLtpca
d
Ft
Ftl
Fs9
732 HANSEN ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 5, No. 6
EB05 � 2.4). Conversely, we detected a relatively strong signalor granulomatous infections (EB05 � 12.6) that was consis-ent for IBD and non-IBD groups.
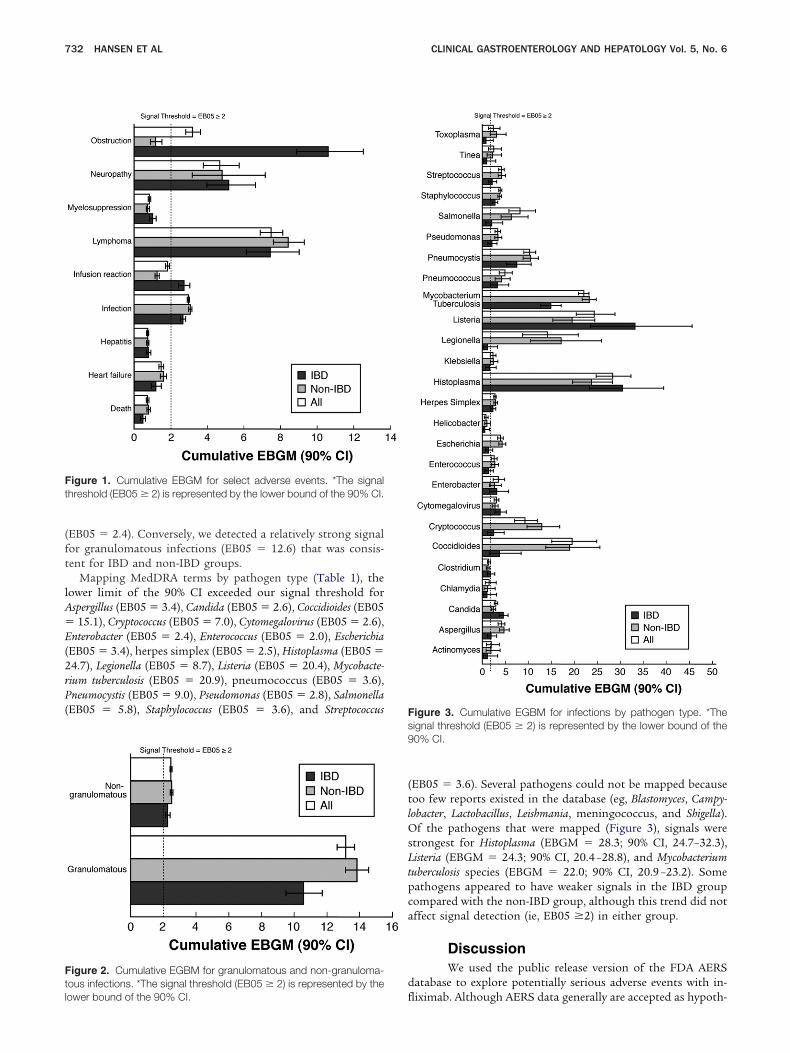
Mapping MedDRA terms by pathogen type (Table 1), theower limit of the 90% CI exceeded our signal threshold forspergillus (EB05 � 3.4), Candida (EB05 � 2.6), Coccidioides (EB0515.1), Cryptococcus (EB05 � 7.0), Cytomegalovirus (EB05 � 2.6),
nterobacter (EB05 � 2.4), Enterococcus (EB05 � 2.0), EscherichiaEB05 � 3.4), herpes simplex (EB05 � 2.5), Histoplasma (EB05 �4.7), Legionella (EB05 � 8.7), Listeria (EB05 � 20.4), Mycobacte-ium tuberculosis (EB05 � 20.9), pneumococcus (EB05 � 3.6),neumocystis (EB05 � 9.0), Pseudomonas (EB05 � 2.8), Salmonella
EB05 � 5.8), Staphylococcus (EB05 � 3.6), and Streptococcus
igure 1. Cumulative EBGM for select adverse events. *The signalhreshold (EB05 � 2) is represented by the lower bound of the 90% CI.
igure 2. Cumulative EGBM for granulomatous and non-granuloma-ous infections. *The signal threshold (EB05 � 2) is represented by the
flower bound of the 90% CI.
EB05 � 3.6). Several pathogens could not be mapped becauseoo few reports existed in the database (eg, Blastomyces, Campy-obacter, Lactobacillus, Leishmania, meningococcus, and Shigella).
f the pathogens that were mapped (Figure 3), signals weretrongest for Histoplasma (EBGM � 28.3; 90% CI, 24.7–32.3),isteria (EBGM � 24.3; 90% CI, 20.4 –28.8), and Mycobacterium
uberculosis species (EBGM � 22.0; 90% CI, 20.9 –23.2). Someathogens appeared to have weaker signals in the IBD groupompared with the non-IBD group, although this trend did notffect signal detection (ie, EB05 �2) in either group.
DiscussionWe used the public release version of the FDA AERS
atabase to explore potentially serious adverse events with in-
igure 3. Cumulative EGBM for infections by pathogen type. *Theignal threshold (EB05 � 2) is represented by the lower bound of the0% CI.
iximab. Although AERS data generally are accepted as hypoth-

ewbnrpil
rrgafbtBilstredobibar
ampyiwiofapipftrrgivsftor1y
rf
cr(rbptthedtwpi
ipvrao
fiufetimcrpt
bwprylDdosvlida
tItTiwai
June 2007 INFLIXIMAB AND SERIOUS ADVERSE EVENTS 733
sis generating and do not demonstrate causal relationships,9
e used the data as a mechanism to refine existing hypothesesy looking at a priori– defined adverse events. Our analysis doesot demonstrate causality, but it helps to focus on more nar-owly defined groups of adverse events in a systematic way. Inart, our analysis validates the AERS methodology by confirm-
ng the relative rate of adverse events previously reported in theiterature.
On the basis of these spontaneously generated adverse eventeports, we confirmed relatively strong signals for previouslyeported adverse events including lymphoma, neuropathy, andranulomatous infections. Signals were relatively consistentcross inflammatory bowel and other indications, although weound indication-related differences for adverse events likeowel obstruction, infusion reactions, and infections with cer-ain pathogen types (eg, Coccidioides, Cryptococcus, and Legionella).owel obstruction might be an example of confounding by
ndication. Individuals with symptoms of obstruction wereikely treated for these symptoms with infliximab. When theyubsequently obstructed, the event could have been attributedo infliximab. For the case of infusion reactions, indication-elated differences might be explained by other factors. Forxample, in Crohn’s disease infliximab was approved as a singleose, which likely means there was more episodic use than inther conditions. This pattern of administration is thought toe �immunogenic” and could partially explain differences in
nfusion reactions. Alternatively, infusion reactions might haveeen more widely discussed in the gastroenterology literature,nd thus gastroenterologists might have been more likely toeport infusion reactions.
Our analysis of FDA AERS data indicated that lymphomand serious infections were reported at least 6.9 and 2.9 timesore often, respectively, with infliximab than would be ex-
ected. Previous meta-analysis, observational studies, and anal-sis of spontaneous adverse event reports have also reported anncreased risk of lymphoma4,18,19 and serious infections4,16,20 –27
ith infliximab. In a prospective cohort study, the standardizedncidence ratio for lymphoma, a measure reflecting the numberf cases observed over the total number of cases expected, wasound to be 2.6 among patients taking infliximab.19 A 2002nalysis of FDA AERS data estimated the incidence of lym-homa to be 6.6 per 100,000.18 In a meta-analysis of data from
nfliximab and adalimumab placebo-controlled trials, theooled odds ratio for malignancy was 3.3 (95% CI, 1.2–9.1) andor serious infection was 2.0 (95% CI, 1.3–3.1).4 This is consis-ent with the German Biologics Register,27 which showed aelative risk of 3.0 (95% CI, 1.8 –5.1) for serious infections. Theisk of infection has been documented for opportunistic patho-ens like Mycobacterium tuberculosis,22,23 histoplasmosis,24 coccid-oidomycosis,21 listeriosis,25 and Candida.23 Our analysis pro-ides additional, up-to-date evidence supporting the risk ofuch infections, demonstrating relatively strong signal scoresor these pathogens as well as Pneumocystis, Legionella, and Cryp-ococcus. In addition, we were able to confirm the increased riskf granulomatous infections documented by Wallis et al.16 Theelative reporting rate of granulomatous infections was nearly3 times greater than the expected reporting rate in our anal-sis.
Evidence from randomized, controlled trials and databaseeviews has suggested the potential for increased risk of heart
ailure28,29 and neuropathy.30 Although we identified an in- treased risk of neuropathy (EB05 � 3.8), the relative rate ofeporting of heart failure did not exceed our signal thresholdEB05 � 1.4). In this analysis, we mapped 17 MedDRA termsepresenting heart failure to a single term (Supplementary Ta-le 1). The practice of combining terms, in general, might beroblematic because the relative reporting rate might decline ifhe wrong terms are combined.9 To explore the potential forhis, we evaluated EBGM values for individual terms mapped toeart failure. No EB05 value for an individual MedDRA termxceeded our signal threshold of 2.0, although EBGM valuesid range from 0.3–1.9, and the upper confidence bound forerms such as ventricular dysfunction and cardiac failure congestiveas greater than 2.0. Regardless, this does not provide a com-elling signal for an increased risk of heart failure with inflix-
mab.We included the MedDRA terms for death and sudden death
n our analysis and did not identify a signal. However, thesearticular terms might be challenging. In many cases, death isiewed as an outcome rather than an adverse event. As such, theate of reporting of death or sudden death might be lower thanctual rates, which could contribute to the low signal scores webserved.
An analysis of adverse events on infliximab is of interestor several reasons. First, at the time of this analysis, inflix-mab was the only biologic product on the market labeled forse in IBD. By including both IBD and non-IBD indications
or the use of the drug, we could potentially tease out adversevents (like bowel obstruction) that were a consequence ofhe disease rather than the treatment. This is especiallymportant because rheumatoid arthritis, regardless of treat-
ent, has been linked to an increased risk of infection andertain malignancies. Given the similarity of adverse eventeporting for IBD and non-IBD indications, our analysisrovides some support for an effect of the drug, rather thanhe disease being treated.
We focused exclusively on infliximab rather than on alliologics. We also chose not to include other drugs that likelyould be used for IBD and non-IBD conditions because com-aring the magnitude of signals for multiple drugs is notecommended with this methodology.9 Although previous anal-ses have done this,16 we chose not to include additional bio-ogics because of the temptation to compare signal scores.
ifferences in the magnitude of signal scores do not implyifferences in risk with different drugs because the spontane-usly reported events are biased in ways that cannot be mea-ured or controlled.9 In general, the MedWatch system relies onoluntary reporting of adverse events, and underreporting isikely.31 Therefore, it lacks an adequate denominator to drawnferences about causation and the comparative risks of anyrugs. Our analysis is limited to infliximab, and generalizationsbout biologics should not be made.
The present analysis was limited to events that were reportedo the FDA in patients treated with infliximab. Patients withBD are often treated with drug combinations, and the signalhat we observed could be due to concomitant therapy. In theREAT study,32 more than 3000 patients treated with inflix-
mab were compared with a similar number of patients whoere not treated with infliximab. In multivariate analyses theuthors reported that the risk factors for serious infectionsncluded prednisone use, narcotic analgesic use, and moderate
o severe disease but not infliximab. The results raise the pos-
smflstsamcdo
emArpcrrmcmobaa
ripmsevssshHtasebtctisvr
egywcc
no
1
1
1
1
1
1
1
1
1
734 HANSEN ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 5, No. 6
ibility that other therapy (eg, prednisone) or severe diseaseight confound the association that we observed between in-
iximab and serious infections. The results from the TREATtudy are at odds with systematic reviews.3 Generally speaking,he very high signals that we observed for certain infectionsuch as histoplasmosis are not likely to be due to confounding,lthough they could be due to biases in reporting. Histoplas-osis, for example, is listed on the label for infliximab, which
ould influence reporting. Heart failure, liver injury, and bloodyscrasias are also listed on the label but were not observed inur study.
Although this analysis focuses on potentially serious adversevents with infliximab and raises concern, risk of such eventsust be viewed in light of the significant benefits of this drug.recent decision analysis suggested that despite an increased
isk of important adverse events, the substantial clinical im-rovement and fewer surgeries associated with infliximab in-reased quality-adjusted life-years for users.33 Even though aisk of events exists, serious adverse events are still relativelyare. In Crohn’s disease, infliximab has demonstrated an esti-
ated 2-fold to 3-fold increase in the number of respondersompared with placebo.3 Patients requiring aggressive treat-ent with infliximab might be willing to accept the higher risk
f serious adverse events because of the high likelihood ofenefits. Patients should be properly informed of potential risksnd allowed to decide what level of risk they are willing toccept in light of clinical efficacy.
Disproportionality analysis is limited in that it provides theelative rate of reporting of adverse events in the post-market-ng setting rather than the incidence of adverse events. Dispro-ortionality analyses are poor surrogates for controlled epide-iologic studies.34 –37 They can be used as a method to explore
ignals, as we have done here, but they should not be viewed asstablishing causal relationships. Future studies should seek toalidate the hypotheses generated by disproportionality analy-es by reviewing individual cases behind signals or using causaltudy designs (eg, case-control study) to test hypotheses. Onetrong point of our analysis compared with other studies thatave used the FDA AERS data is the timeliness of the data.owever, as a result of data entry delays, some reports spanning
he first 6 –9 months of 2005 might not be included in ournalysis. In addition, the FDA gives data entry priority toerious, unlabeled events, which could lead to potential under-stimation of the risk of some events. Because the AERS data-ase relies on self-reports, the reporting rates can fluctuate overime and are sensitive to publicity, marketing, and liabilityoncerns.38 Differences in the rate of reporting (or recording inhe database) for specific drugs or events are known to benfluenced by product age, targeted surveillance, selective pre-cribing, stimulated reporting, or source of reporting (eg, U.S.s foreign reports). These differences might have influenced theesults of our analysis.9
We found the relative rate of reporting of serious adversevents with infliximab such as lymphoma, neuropathy, andranulomatous infections to be consistent with previous anal-ses. Still, this potential risk needs to be studied further withell-conducted epidemiologic studies. In the meantime, clini-
ians should discuss potential risks with patients in light of
linical efficacy.Supplementary DataNote: To access the supplementary material accompa-
ying this article, visit the online version of Clinical Gastroenter-logy and Hepatology at www.cghjournal.org.
References
1. Knight DM, Trinh H, Le J, et al. Construction and initial charac-terization of a mouse-human chimeric anti-TNF antibody. MolImmunol 1993;30:1443–1453.
2. Scallon BJ, Moore MA, Trinh H, et al. Chimeric anti-TNF-alphamonoclonal antibody cA2 binds recombinant transmembraneTNF-alpha and activates immune effector functions. Cytokine1995;7:251–259.
3. Gartlehner G, Hansen RA, Thieda P, et al. Drug class review ontargeted immune modulators. Chapel Hill, NC: RTI-UNC Evidence-based Practice Center, 2005: Available at: http://www.ohsu.edu/drugeffectiveness/reports/final.cfm. Accessed: October 18,2006.
4. Bongartz T, Sutton AJ, Sweeting MJ, et al. Anti-TNF antibodytherapy in rheumatoid arthritis and the risk of serious infectionsand malignancies: systematic review and meta-analysis of rareharmful effects in randomized controlled trials. JAMA 2006;295:2275–2285.
5. Doran MF, Crowson CS, Pond GR, et al. Frequency of infection inpatients with rheumatoid arthritis compared with controls: a pop-ulation-based study. Arthritis Rheum 2002;46:2287–2293.
6. Mellemkjaer L, Linet MS, Gridley G, et al. Rheumatoid arthritisand cancer risk. Eur J Cancer 1996;32A:1753–1757.
7. Thomas E, Brewster DH, Black RJ, et al. Risk of malignancyamong patients with rheumatic conditions. Int J Cancer 2000;88:497–502.
8. Ahmad SR. Adverse drug event monitoring at the Food and DrugAdministration. J Gen Intern Med 2003;18:57–60.
9. Almenoff J, Tonning JM, Gould AL, et al. Perspectives on the useof data mining in pharmaco-vigilance. Drug Saf 2005;28:981–1007.
0. DuMouchel WPD. Bayesian data mining in large frequency tables,with an application to the FDA Spontaneous Reporting System.The American Statistician 1999;53:177–202.
1. DuMouchel WPD. Empirical Bayes screening for multi-item asso-ciations: Seventh ACM SigKDD International Conference onKnowledge Discovery and Data Mining. San Francisco: ACMPress, 2001.
2. Szarfman A, Machado SG, O’Neill RT. Use of screening algo-rithms and computer systems to efficiently signal higher-than-expected combinations of drugs and events in the US FDA’sspontaneous reports database. Drug Saf 2002;25:381–392.
3. Roach DR, Bean AG, Demangel C, et al. TNF regulates chemokineinduction essential for cell recruitment, granuloma formation,and clearance of mycobacterial infection. J Immunol 2002;168:4620–4627.
4. Kindler V, Sappino AP, Grau GE, et al. The inducing role of tumornecrosis factor in the development of bactericidal granulomasduring BCG infection. Cell 1989;56:731–740.
5. Allendoerfer R, Deepe GS Jr. Regulation of infection with His-toplasma capsulatum by TNFR1 and -2. J Immunol 2000;165:2657–2664.
6. Wallis RS, Broder MS, Wong JY, et al. Granulomatous infectiousdiseases associated with tumor necrosis factor antagonists. ClinInfect Dis 2004;38:1261–1265.
7. Hilsden RJ, Verhoef MJ, Best A, et al. A national survey on thepatterns of treatment of inflammatory bowel disease in Canada.BMC Gastroenterol 2003;3:10.
8. Brown SL, Greene MH, Gershon SK, et al. Tumor necrosis factor
antagonist therapy and lymphoma development: twenty-six cases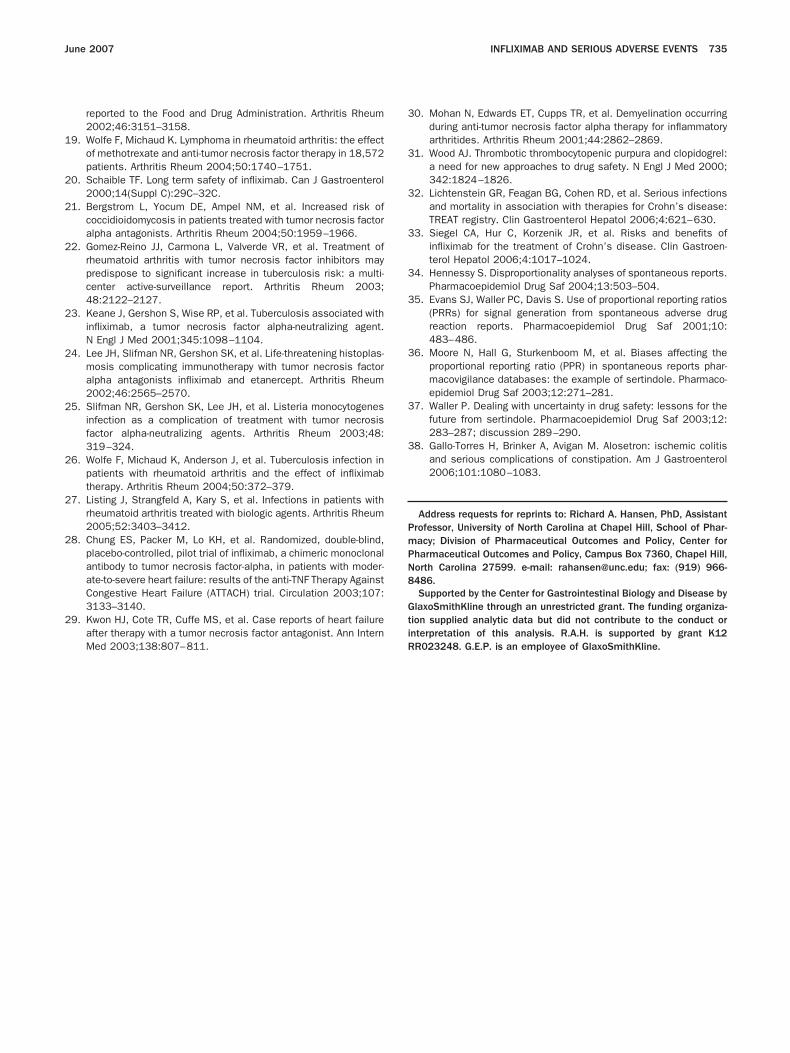
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
PmPN8
Gti
June 2007 INFLIXIMAB AND SERIOUS ADVERSE EVENTS 735
reported to the Food and Drug Administration. Arthritis Rheum2002;46:3151–3158.
9. Wolfe F, Michaud K. Lymphoma in rheumatoid arthritis: the effectof methotrexate and anti-tumor necrosis factor therapy in 18,572patients. Arthritis Rheum 2004;50:1740–1751.
0. Schaible TF. Long term safety of infliximab. Can J Gastroenterol2000;14(Suppl C):29C–32C.
1. Bergstrom L, Yocum DE, Ampel NM, et al. Increased risk ofcoccidioidomycosis in patients treated with tumor necrosis factoralpha antagonists. Arthritis Rheum 2004;50:1959–1966.
2. Gomez-Reino JJ, Carmona L, Valverde VR, et al. Treatment ofrheumatoid arthritis with tumor necrosis factor inhibitors maypredispose to significant increase in tuberculosis risk: a multi-center active-surveillance report. Arthritis Rheum 2003;48:2122–2127.
3. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated withinfliximab, a tumor necrosis factor alpha-neutralizing agent.N Engl J Med 2001;345:1098–1104.
4. Lee JH, Slifman NR, Gershon SK, et al. Life-threatening histoplas-mosis complicating immunotherapy with tumor necrosis factoralpha antagonists infliximab and etanercept. Arthritis Rheum2002;46:2565–2570.
5. Slifman NR, Gershon SK, Lee JH, et al. Listeria monocytogenesinfection as a complication of treatment with tumor necrosisfactor alpha-neutralizing agents. Arthritis Rheum 2003;48:319–324.
6. Wolfe F, Michaud K, Anderson J, et al. Tuberculosis infection inpatients with rheumatoid arthritis and the effect of infliximabtherapy. Arthritis Rheum 2004;50:372–379.
7. Listing J, Strangfeld A, Kary S, et al. Infections in patients withrheumatoid arthritis treated with biologic agents. Arthritis Rheum2005;52:3403–3412.
8. Chung ES, Packer M, Lo KH, et al. Randomized, double-blind,placebo-controlled, pilot trial of infliximab, a chimeric monoclonalantibody to tumor necrosis factor-alpha, in patients with moder-ate-to-severe heart failure: results of the anti-TNF Therapy AgainstCongestive Heart Failure (ATTACH) trial. Circulation 2003;107:3133–3140.
9. Kwon HJ, Cote TR, Cuffe MS, et al. Case reports of heart failureafter therapy with a tumor necrosis factor antagonist. Ann Intern
Med 2003;138:807–811. R0. Mohan N, Edwards ET, Cupps TR, et al. Demyelination occurringduring anti-tumor necrosis factor alpha therapy for inflammatoryarthritides. Arthritis Rheum 2001;44:2862–2869.
1. Wood AJ. Thrombotic thrombocytopenic purpura and clopidogrel:a need for new approaches to drug safety. N Engl J Med 2000;342:1824–1826.
2. Lichtenstein GR, Feagan BG, Cohen RD, et al. Serious infectionsand mortality in association with therapies for Crohn’s disease:TREAT registry. Clin Gastroenterol Hepatol 2006;4:621–630.
3. Siegel CA, Hur C, Korzenik JR, et al. Risks and benefits ofinfliximab for the treatment of Crohn’s disease. Clin Gastroen-terol Hepatol 2006;4:1017–1024.
4. Hennessy S. Disproportionality analyses of spontaneous reports.Pharmacoepidemiol Drug Saf 2004;13:503–504.
5. Evans SJ, Waller PC, Davis S. Use of proportional reporting ratios(PRRs) for signal generation from spontaneous adverse drugreaction reports. Pharmacoepidemiol Drug Saf 2001;10:483–486.
6. Moore N, Hall G, Sturkenboom M, et al. Biases affecting theproportional reporting ratio (PPR) in spontaneous reports phar-macovigilance databases: the example of sertindole. Pharmaco-epidemiol Drug Saf 2003;12:271–281.
7. Waller P. Dealing with uncertainty in drug safety: lessons for thefuture from sertindole. Pharmacoepidemiol Drug Saf 2003;12:283–287; discussion 289–290.
8. Gallo-Torres H, Brinker A, Avigan M. Alosetron: ischemic colitisand serious complications of constipation. Am J Gastroenterol2006;101:1080–1083.
Address requests for reprints to: Richard A. Hansen, PhD, Assistantrofessor, University of North Carolina at Chapel Hill, School of Phar-acy; Division of Pharmaceutical Outcomes and Policy, Center forharmaceutical Outcomes and Policy, Campus Box 7360, Chapel Hill,orth Carolina 27599. e-mail: [email protected]; fax: (919) 966-486.Supported by the Center for Gastrointestinal Biology and Disease by
laxoSmithKline through an unrestricted grant. The funding organiza-ion supplied analytic data but did not contribute to the conduct ornterpretation of this analysis. R.A.H. is supported by grant K12
R023248. G.E.P. is an employee of GlaxoSmithKline.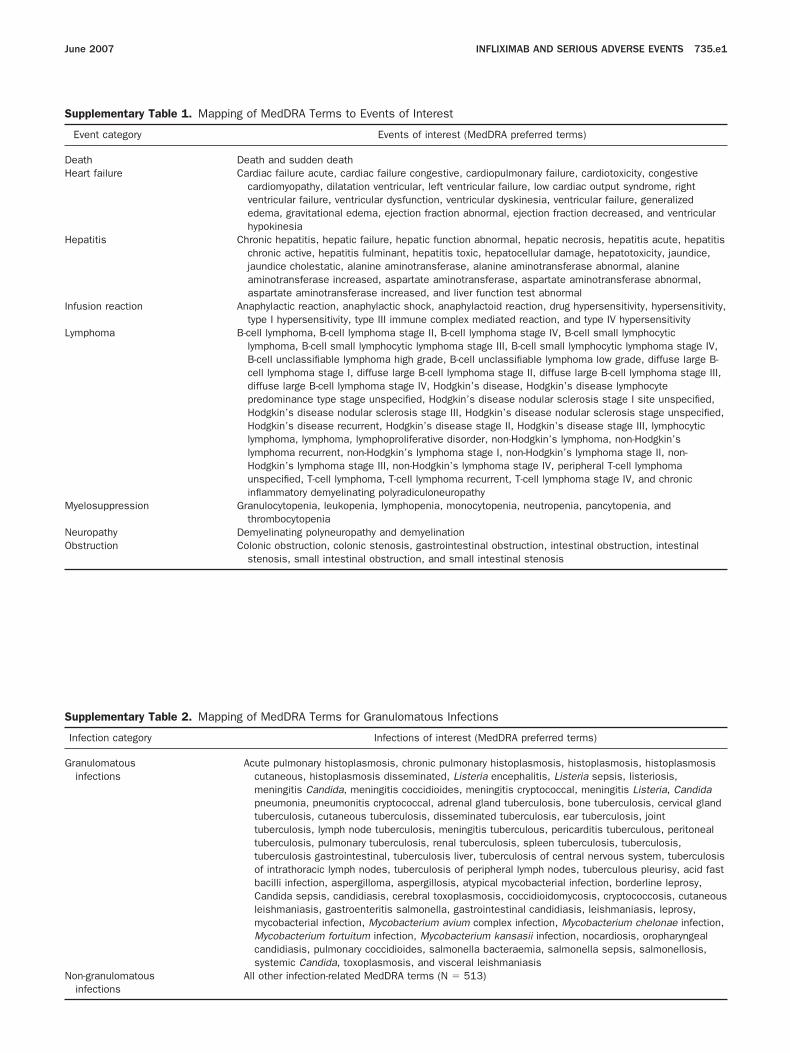
S
DH
H
I
L
M
NO
truction, and small intestinal stenosis
S
G
N
June 2007 INFLIXIMAB AND SERIOUS ADVERSE EVENTS 735.e1
upplementary Table 1. Mapping of MedDRA Terms to Even
Event category Ev
eath Death and sudden deatheart failure Cardiac failure acute, cardiac fa
cardiomyopathy, dilatation venventricular failure, ventricularedema, gravitational edema,hypokinesia
epatitis Chronic hepatitis, hepatic failurechronic active, hepatitis fulmijaundice cholestatic, alanineaminotransferase increased,aspartate aminotransferase in
nfusion reaction Anaphylactic reaction, anaphylactype I hypersensitivity, type III
ymphoma B-cell lymphoma, B-cell lymphomlymphoma, B-cell small lymphB-cell unclassifiable lymphomcell lymphoma stage I, diffusediffuse large B-cell lymphomapredominance type stage unsHodgkin’s disease nodular scHodgkin’s disease recurrent,lymphoma, lymphoma, lympholymphoma recurrent, non-HodHodgkin’s lymphoma stage IIIunspecified, T-cell lymphoma,inflammatory demyelinating po
yelosuppression Granulocytopenia, leukopenia, lythrombocytopenia
europathy Demyelinating polyneuropathy abstruction Colonic obstruction, colonic sten
stenosis, small intestinal obs
upplementary Table 2. Mapping of MedDRA Terms for Gran
Infection category Inf
ranulomatousinfections
Acute pulmonary histoplasmoscutaneous, histoplasmosis dmeningitis Candida, meningipneumonia, pneumonitis crytuberculosis, cutaneous tubtuberculosis, lymph node tubtuberculosis, pulmonary tubetuberculosis gastrointestinalof intrathoracic lymph nodesbacilli infection, aspergillomCandida sepsis, candidiasisleishmaniasis, gastroenteritmycobacterial infection, MycMycobacterium fortuitum infcandidiasis, pulmonary coccsystemic Candida, toxoplasm
on-granulomatous All other infection-related MedD
ts of Interest
ents of interest (MedDRA preferred terms)
ilure congestive, cardiopulmonary failure, cardiotoxicity, congestivetricular, left ventricular failure, low cardiac output syndrome, rightdysfunction, ventricular dyskinesia, ventricular failure, generalizedejection fraction abnormal, ejection fraction decreased, and ventricular
, hepatic function abnormal, hepatic necrosis, hepatitis acute, hepatitisnant, hepatitis toxic, hepatocellular damage, hepatotoxicity, jaundice,aminotransferase, alanine aminotransferase abnormal, alanineaspartate aminotransferase, aspartate aminotransferase abnormal,creased, and liver function test abnormaltic shock, anaphylactoid reaction, drug hypersensitivity, hypersensitivity,immune complex mediated reaction, and type IV hypersensitivitya stage II, B-cell lymphoma stage IV, B-cell small lymphocytic
ocytic lymphoma stage III, B-cell small lymphocytic lymphoma stage IV,a high grade, B-cell unclassifiable lymphoma low grade, diffuse large B-
large B-cell lymphoma stage II, diffuse large B-cell lymphoma stage III,stage IV, Hodgkin’s disease, Hodgkin’s disease lymphocytepecified, Hodgkin’s disease nodular sclerosis stage I site unspecified,lerosis stage III, Hodgkin’s disease nodular sclerosis stage unspecified,Hodgkin’s disease stage II, Hodgkin’s disease stage III, lymphocyticproliferative disorder, non-Hodgkin’s lymphoma, non-Hodgkin’s
gkin’s lymphoma stage I, non-Hodgkin’s lymphoma stage II, non-, non-Hodgkin’s lymphoma stage IV, peripheral T-cell lymphomaT-cell lymphoma recurrent, T-cell lymphoma stage IV, and chroniclyradiculoneuropathymphopenia, monocytopenia, neutropenia, pancytopenia, and
nd demyelinationosis, gastrointestinal obstruction, intestinal obstruction, intestinal
ulomatous Infections
ections of interest (MedDRA preferred terms)
is, chronic pulmonary histoplasmosis, histoplasmosis, histoplasmosisisseminated, Listeria encephalitis, Listeria sepsis, listeriosis,tis coccidioides, meningitis cryptococcal, meningitis Listeria, Candidaptococcal, adrenal gland tuberculosis, bone tuberculosis, cervical glanderculosis, disseminated tuberculosis, ear tuberculosis, jointerculosis, meningitis tuberculous, pericarditis tuberculous, peritonealrculosis, renal tuberculosis, spleen tuberculosis, tuberculosis,, tuberculosis liver, tuberculosis of central nervous system, tuberculosis, tuberculosis of peripheral lymph nodes, tuberculous pleurisy, acid fasta, aspergillosis, atypical mycobacterial infection, borderline leprosy,, cerebral toxoplasmosis, coccidioidomycosis, cryptococcosis, cutaneousis salmonella, gastrointestinal candidiasis, leishmaniasis, leprosy,obacterium avium complex infection, Mycobacterium chelonae infection,ection, Mycobacterium kansasii infection, nocardiosis, oropharyngealidioides, salmonella bacteraemia, salmonella sepsis, salmonellosis,osis, and visceral leishmaniasisRA terms (N � 513)
infections