Embed Size (px)
Citation preview
ORIGINAL INVESTIGATION
Serotonin2A receptor blockade and clinical effectin first-episode schizophrenia patients treatedwith quetiapine
Hans Rasmussen & Bjorn H. Ebdrup & David Erritzoe & Bodil Aggernaes & Bob Oranje &
Jan Kalbitzer & Lars H. Pinborg & William F. C. Baaré & Claus Svarer &
Henrik Lublin & Gitte M. Knudsen & Birte Glenthoj
Received: 19 March 2010 /Accepted: 24 June 2010 /Published online: 8 July 2010# Springer-Verlag 2010
AbstractRationale We have previously reported decreased frontalcortical serotonin2A receptor binding in 30 antipsychoticnaïve first-episode schizophrenic patients and a relationshipbetween this binding and positive psychotic symptoms.Until now, no longitudinal studies of serotonin2A receptor
in first-episode antipsychotic-naïve schizophrenia patientshave reported on the relationship between serotonin2Areceptor occupancy and treatment effect after sustainedtreatment with a specific atypical antipsychotic compound.Objectives Here, we measured serotonin2A receptor occu-pancy with [18F]altanserin PET in 15 first-episodeantipsychotic-naïve schizophrenia patients before and after6 months of quetiapine treatment. Moreover, we investi-gated possible relationships between clinical efficacy, oraldose, and plasma levels of quetiapineResults Significant nonlinear relationships were foundbetween serotonin2A receptor occupancy, quetiapinedose, and plasma concentration. There was a modesteffect on positive symptoms up until a serotonin2Areceptor occupancy level of approximately 60%. Areceptor occupancy level between 60% and 70%appeared to exert the optimal serotonin2A receptorrelated treatment effect on positive symptoms whereasno additional serotonin2A receptor associated treatmenteffect was obtained above a receptor occupancy of 70%.Conclusions Taken together, the data point to a thera-peutic role of the serotonin2A receptor in the treatmentof subgroups of patients with schizophrenia. Specifically,the study indicates a serotonin2A receptor associatedtherapeutic window on positive symptoms in respondingpatients in the range between 60% and 70% occupancyin antipsychotic-naïve first-episode schizophrenia. Wespeculate that non-responding patients need higherdopamine D2 receptor blockade. Future studies withconcurrent measurement of interactions with the dopaminesystem are, however, warranted to clarify this.
Keywords Schizophrenia . First-episode . PET. 5-HT2A.
Quetiapine . Receptor occupancy
H. Rasmussen (*) : B. H. Ebdrup : B. Aggernaes :B. Oranje :H. Lublin : B. GlenthojCenter for Neuropsychiatric Schizophrenia Research,Faculty of Health Sciences, Psychiatric Center Glostrup,Copenhagen University Hospital Glostrup,Copenhagen DK-2600, Denmarke-mail: [email protected]
H. Rasmussen :B. H. Ebdrup :B. Aggernaes : B. Oranje :H. Lublin : B. GlenthojCenter for Clinical Intervention and NeuropsychiatricSchizophrenia Research, Faculty of Health Sciences,Psychiatric Center Glostrup,Copenhagen University Hospital Glostrup,Copenhagen DK-2600, Denmark
H. Rasmussen :D. Erritzoe : J. Kalbitzer : L. H. Pinborg :C. Svarer :G. M. KnudsenNeurobiology Research Unit and Center for Integrated MolecularBrain Imaging, Faculty of Health Sciences,Copenhagen University Hospital Rigshospitalet,Copenhagen, Denmark
B. H. Ebdrup :W. F. C. BaaréDanish Centre for Magnetic Resonance Imaging,University Hospital Hvidovre,Copenhagen, Denmark
W. F. C. BaaréCenter for Integrated Molecular Brain Imaging, Faculty of HealthSciences, Copenhagen University Hospital Rigshospitalet,Copenhagen, Denmark
Psychopharmacology (2011) 213:583–592DOI 10.1007/s00213-010-1941-5

Introduction
Increasing evidence points towards a role of the seroto-nin2A receptor in schizophrenia. Eleven out of 15published post-mortem studies report that serotonin2Areceptor binding is decreased in cortical, and especiallyfrontal cortical brain regions (see (Rasmussen et al. 2010)for references), although these reports are primarily basedon chronically ill, medicated patients, and the techniquesused to analyze post-mortem tissue differed between studies(Dean et al. 2008).
However, these findings are supported in vivo by ourrecent PET study in 30 first-episode antipsychotic-naïveschizophrenia patients, reporting decreased serotonin2Areceptor binding in the frontal cortex and a relation betweendecreased binding and positive psychotic symptoms in themale patients (Rasmussen et al. 2010). Furthermore, clinicaltrials with MDL-100907, a drug with highly specificserotonin2A receptor antagonism, have indicated antipsy-chotic effects (de Paulis 2001; Snigdha et al. 2010).Likewise the inverse agonist, pimavanserin, which current-ly is in clinical development reduces hallucinations anddelusions in patients with Parkinson's disease supportingthe hypothesis that blocking serotonin2A receptors is aneffective means of diminishing positive symptoms in thiscondition (Meltzer et al. 2010).
Indirect support for the involvement of the serotonin2Areceptors in schizophrenia comes from the associationbetween the receptor affinity profile and the clinicalcharacteristics of second generation antipsychotic drugs(SGAs). In contrast to first-generation antipsychotic drugs,that primarily are dopamine D2 receptor antagonists,most SGAs have higher affinity to serotonin2A receptorsthan to D2 receptors (Farde et al. 1995). Moreover, theserotonin2A receptor is the major site of action ofhallucinogens (Nichols 2004). Furthermore, an associationbetween polymorphisms in the promoter and codingregions of the serotonin2A receptor gene and the responseto treatment with clozapine has been reported (Arranz et al.1998). Among the SGAs, both clozapine and quetiapine arecharacterized by a moderate affinity for the serotonin2Areceptor combined with a loose binding (a fast koff) and alow affinity for dopamine D2 receptors (Kapur and Seeman2001; Kessler et al. 2006). However, according to clinicalguidelines, clozapine is not recommended as a first choicein first-episode schizophrenia (Kerwin 2007).
The relationships between serotonin2A receptor block-ade, oral dose, plasma quetiapine concentrations andtreatment effect are unclear. In recent studies, with atreatment period of 6 weeks or less, no clear associationbetween quetiapine plasma concentration and clinicalresponse was found, and no optimal therapeutic range forquetiapine was identified (Fabre et al. 1995; Small et al.
1997). Measurements of plasma quetiapine concentrations,oral dose and clinical response have generally beeninconclusive, for a review see (Mauri et al. 2007).However, in 12 chronic schizophrenic patients, a [18F]setoperone PET study founda curvilinear hyperbolic rela-tion between serotonin2A receptor blockade and plasmaquetiapine concentration. Moreover, a quetiapine dosebetween 300 and 600 mg/day resulted in a serotonin2Areceptor blockade between 57% and 78% (Kapur et al.2000).
Previous treatment studies with antipsychotic drugs thatantagonize the serotonin2A receptor have shown a para-doxical down-regulation of the receptor, both in vivo and invitro (Dean 2003; Gray and Roth 2001). As such, thismight have influenced the results of previous studies ofserotonin2A receptors since they included patients whowere chronically ill and previously medicated with bothtypical and atypical compounds before their shift toquetiapine (Gefvert et al. 1998, 2001; Kapur et al. 2000).Furthermore, the tracers [18F]setoperone and [11C]N-meth-ylspiperone that were used in these studies (Gefvert et al.1998, 2001; Kapur et al. 2000) are limited by theirrelatively poor selectivity for the serotonin2A receptors. Incomparison [18F]altanserin has a 200–500-fold seroto-nin2A/D2 receptor selectivity (Kristiansen et al. 2005; Tanet al. 1999) making it eight to 50 times more selective forthe serotonin2A receptor than [18F]setoperone (Lewis et al.1999). In addition, the affinity of [18F]altanserin for theserotonin2A receptor is at least 20-fold higher than forother serotonin receptor subtypes (Tan et al. 1999). Wehave previously demonstrated that [18F]altanserin PET witha bolus infusion design is a highly reproducible and reliablemethod for quantification of serotonin2A receptors(Haugbol et al. 2007).
Results of previous studies reporting no difference inserotonin2A receptor binding between patients with schizo-phrenia and healthy controls (Lewis et al. 1999; Okubo et al.2000; Trichard et al. 1998; Verhoeff et al. 2000) mighttherefore have been due to a poor selectivity of theradiotracers that have been used and the relatively smallsample sizes of the studies (Haugbol et al. 2007; Rasmussenet al. 2010).
In this study, we included first-episode antipsychotic-naïve patients who were examined with the highlyserotonin2A receptor selective radioligand [18F]altanserin.We examined the relation between serotonin2A receptorblockade and clinical effect after 6 months of sustainedtreatment with quetiapine. Furthermore, we investigatedwhether cerebral serotonin2A receptor blockade was relatedto plasma levels of quetiapine, dose, and clinical effect.Based on our baseline findings, we expected to find arelationship between serotonin2A receptor blockade andtreatment effect on positive symptoms.
584 Psychopharmacology (2011) 213:583–592

Methods and materials
The study was approved by the Ethics Committee ofCopenhagen and Frederiksberg ((KF)11-061/03, (KF)12291906 and (KF) 11-323091). After complete descriptionof the study to the subjects, written informed consent wasobtained.
Participants
Fifteen patients participated in this study. Initially, thirtyantipsychotic-naïve patients (23 males) diagnosed withschizophrenia according to both ICD-10 and DSM-IV wererecruited after voluntary first-time referral to a psychiatricunit of one of the affiliated university hospitals in theCapital Region of Copenhagen. The patients were identicalto those included in our previously published PET study oncerebral serotonin2A receptor binding in the antipsychotic-naïve state (Rasmussen et al. 2010).
The schizophrenia diagnoses were verified by meansof the Schedules for Clinical Assessment in Neuropsy-chiatry (SCAN 2.1) interview (Wing et al. 1990). Noneof the patients had a history of significant head injury ornon-psychiatric disorder. All patients had normal neuro-logical and physical examinations, and structural magneticresonance imaging (MRI) brain scans were withoutabnormalities.
In the 6-month period between baseline and follow-up,12 patients dropped out. Reasons for attrition were:clinically inadequate effect (n=2), intolerable side-effects(sedation, weight gain, rise in liver enzymes; n=4),pregnancy (n=2), or refusal to participate at follow-up(n=4). Moreover, after the baseline examinations, threepatients had explicitly stated that they were not willing toundergo treatment with quetiapine. As a result, 15 patients(ten males, mean age: 28.9 years, SD=5.4) completed thestudy (see Table 1).
Of the 15 patients participating in the follow-upassessment, four patients were diagnosed as having ahistory of substance abuse according to DSM-IV: alcoholabuse, in sustained full remission (n=2); cannabis abuse,sustained full remission (n=1), other abuse, sustained fullremission and other abuse, early partial remission (n=1).The diagnosis ‘other abuse’ covered mixed cannabis andalcohol abuse. During the treatment period, none of the 15patients had any substance abuse as determined by regularclinical contacts, and all patients had a negative urinescreening for substance intake prior to the PET scans. Twopatients were treated with the selective serotonin reuptakeinhibitors (SSRIs) fluoxetine (n=1) and citalopram (n=1) instable doses (40 mg/day for both compounds), throughoutthe investigation period. Thirteen patients had no lifetimehistory of antidepressant exposure.
Experimental design
All 15 subjects were tested twice: once at baseline and onceafter a period of as close to 6 months as possible (mean=6.8 months, SD=0.9). During the follow-up period, patientswere treated with quetiapine (once daily) in flexible dosesaccording to their clinical condition (mean dose, 383±145 mg per day or 5.2±2.2 mg/kg bodyweight per day), seeTable 1. Concomitant treatment with benzodiazepines wasallowed on an ‘if needed basis’, except on the test days.Nine patients were smokers. Smoking was not allowed upuntil 2 h before the PET radioligand administration.
While at baseline, patients had never been exposed toantipsychotic treatment, at follow-up patients received theirusual daily quetiapine dose 165 min prior to the PET scan.The tmax of quetiapine is between 1 and 2 h withconsiderable interindividual variability in plasma concen-tration (DeVane and Nemeroff 2001). Two previous PETstudies of quetiapine determined a transiently high D2
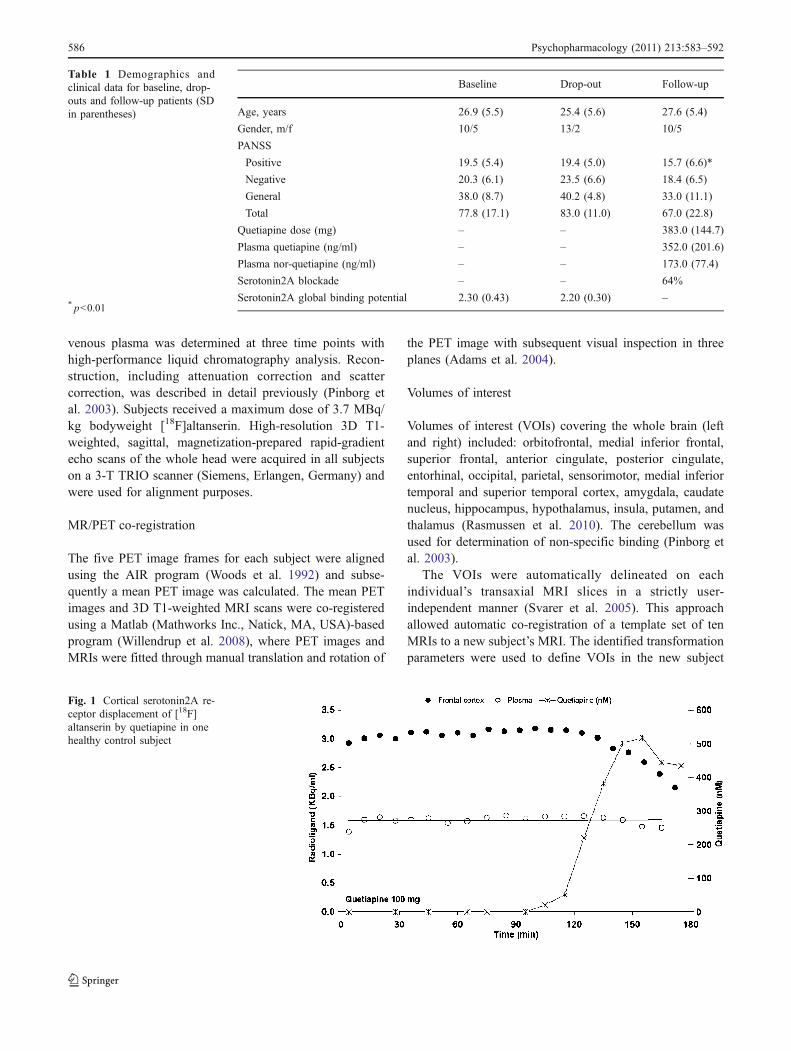
receptor blockade 2 h post dose (Kapur et al. 2000;Tauscher-Wisniewski et al. 2002). A more prolongedblockade has been reported for serotonin2A receptor(blockade half life 53–64 h) as compared to D2R (8–10 h;Gefvert et al. 1998). In the present study, patients werescanned for 40 min 165 min post dose. The period of165 min was chosen because it was the intention to scan ata time point when plasma level of quetiapine was relativelystable and with a low interindividual variability (DeVaneand Nemeroff 2001). Furthermore, 165 min correspond to ahigh level of altanserin displacement by quetiapine asestablished by a pilot study in a healthy individual (seeFig. 1).
Psychopathological ratings
Symptom severity was assessed at the time of both PETscans by trained raters using the Positive and NegativeSyndrome Scale (PANSS; Kay et al. 1987). An intra-classcorrelation coefficient of 0.92 was achieved (Rasmussen etal. 2010).
Imaging
The serotonin2A receptor binding was imaged with [18F]altanserin according to a method described previously(Pinborg et al. 2003). In short: after bolus infusion of thetracer, emission scans (five frames of 8 min each) wereacquired in tracer steady-state conditions with an 18-ringGE-Advance tomograph (GE, Milwaukee, Wisconsin)operating in three-dimensional acquisition mode. The totalaxial field of view was 15.2 cm with an approximate in-plane resolution of 6 mm. After 2 h, when steady state hadbeen obtained, the fraction of unmetabolized tracer in
Psychopharmacology (2011) 213:583–592 585
venous plasma was determined at three time points withhigh-performance liquid chromatography analysis. Recon-struction, including attenuation correction and scattercorrection, was described in detail previously (Pinborg etal. 2003). Subjects received a maximum dose of 3.7 MBq/kg bodyweight [18F]altanserin. High-resolution 3D T1-weighted, sagittal, magnetization-prepared rapid-gradientecho scans of the whole head were acquired in all subjectson a 3-T TRIO scanner (Siemens, Erlangen, Germany) andwere used for alignment purposes.
MR/PET co-registration
The five PET image frames for each subject were alignedusing the AIR program (Woods et al. 1992) and subse-quently a mean PET image was calculated. The mean PETimages and 3D T1-weighted MRI scans were co-registeredusing a Matlab (Mathworks Inc., Natick, MA, USA)-basedprogram (Willendrup et al. 2008), where PET images andMRIs were fitted through manual translation and rotation of
the PET image with subsequent visual inspection in threeplanes (Adams et al. 2004).
Volumes of interest
Volumes of interest (VOIs) covering the whole brain (leftand right) included: orbitofrontal, medial inferior frontal,superior frontal, anterior cingulate, posterior cingulate,entorhinal, occipital, parietal, sensorimotor, medial inferiortemporal and superior temporal cortex, amygdala, caudatenucleus, hippocampus, hypothalamus, insula, putamen, andthalamus (Rasmussen et al. 2010). The cerebellum wasused for determination of non-specific binding (Pinborg etal. 2003).
The VOIs were automatically delineated on eachindividual’s transaxial MRI slices in a strictly user-independent manner (Svarer et al. 2005). This approachallowed automatic co-registration of a template set of tenMRIs to a new subject’s MRI. The identified transformationparameters were used to define VOIs in the new subject
Baseline Drop-out Follow-up
Age, years 26.9 (5.5) 25.4 (5.6) 27.6 (5.4)
Gender, m/f 10/5 13/2 10/5
PANSS
Positive 19.5 (5.4) 19.4 (5.0) 15.7 (6.6)*
Negative 20.3 (6.1) 23.5 (6.6) 18.4 (6.5)
General 38.0 (8.7) 40.2 (4.8) 33.0 (11.1)
Total 77.8 (17.1) 83.0 (11.0) 67.0 (22.8)
Quetiapine dose (mg) – – 383.0 (144.7)
Plasma quetiapine (ng/ml) – – 352.0 (201.6)
Plasma nor-quetiapine (ng/ml) – – 173.0 (77.4)
Serotonin2A blockade – – 64%
Serotonin2A global binding potential 2.30 (0.43) 2.20 (0.30) –
Table 1 Demographics andclinical data for baseline, drop-outs and follow-up patients (SDin parentheses)
* p<0.01
Fig. 1 Cortical serotonin2A re-ceptor displacement of [18F]altanserin by quetiapine in onehealthy control subject
586 Psychopharmacology (2011) 213:583–592
MRI space, and through the co-registration these VOIswere transferred onto the PET images.
Quantification of serotonin2A receptor blockade
The distribution volume (VT) of a radioligand is defined asthe ratio of the radioligand concentration in tissue targetregion (CT, kBq·cm
−3) to that in plasma (CP, kBq·mL−1) atequilibrium (Innis et al. 2007). CP represents the concen-tration of parent radioligand in plasma.
VT ¼ CT=CP ð1ÞA global measure of serotonin2A receptor blockade (O)
was calculated from the distribution volumes in theunblocked (VT) condition and in the partially blockedcondition (VT,b).
O ¼ 1� VT;b � VND
VT � VNDð2Þ
where VND is the distribution volume of the nondisplace-able tracer, i.e., the free and non-specifically bound tracer.Rearrangement of equation 2 leads to:
VT;b ¼ 1� Oð ÞVT þ OVND ð3ÞBy inserting corresponding values for each measured
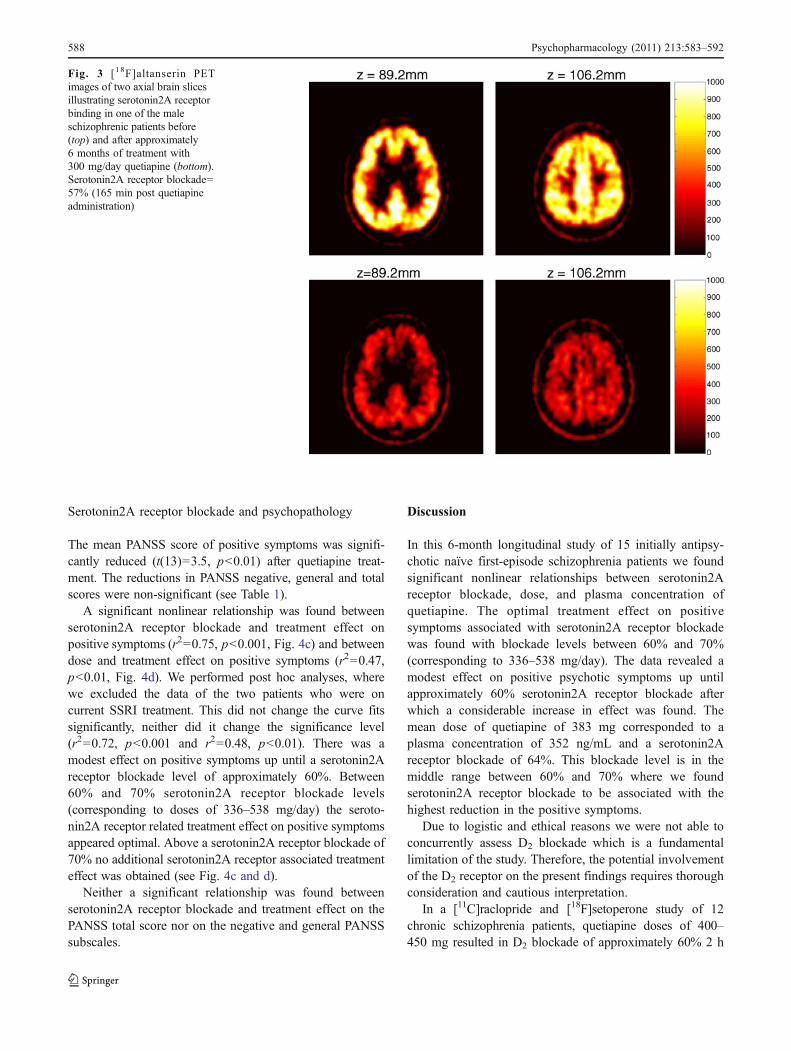
brain region in the unblocked and partially blockedcondition, a blockade plot (Fig. 2) can be made for eachindividual, and hence, an estimate of the global blockadecan be determined in each individual using linear regressionanalysis (Pinborg et al. 2007).
A one-site binding hyperbola model (Kapur et al. 2000)was used to evaluate the relationship between serotonin2Areceptor blockade and the corresponding plasma quetiapineconcentration and dose using the following equation:
O ¼ Emax � XEC50 þ X
ð4Þ
where Emax is the maximum receptor blockade (100%), X=quetiapine plasma concentration (ng/mL) or dose (mg) andEC50 is the estimated quetiapine plasma concentration (ng/mL) or dose (mg) associated with 50% maximal receptorblockade.
Statistics
All statistical analyses were performed with SPSS®. Alldata was normally distributed according to the Kolmo-gorov–Smirnov test, therefore only parametric statisticswere performed. Potential outliers were tested with theGrubbs’ test (Grubb 1969). Differences in PANSS scoresbetween baseline and follow-up were examined with pairedsamples Student’s t tests. Linear regression analysis wasused to calculate global serotonin2A receptor blockadebased on regional values. Similarly, regression analysis wasused to examine the extent to which global serotonin2Areceptor blockade was associated with treatment effects.The latter were calculated as the difference in PANSSscores between baseline and follow-up. Curvefitting wasperformed using GraphPad Prism®. P=0.05 (two-sided)was employed as the level of significance for all tests.
Results
Attrition
The patients who dropped out (n=15) during the 6 monthstreatment period were not significantly different from thosewho completed the study with regards to age, gender,PANSS scores or global baseline serotonin2A receptorbinding potential (see Table 1).
Serotonin2A receptor blockade
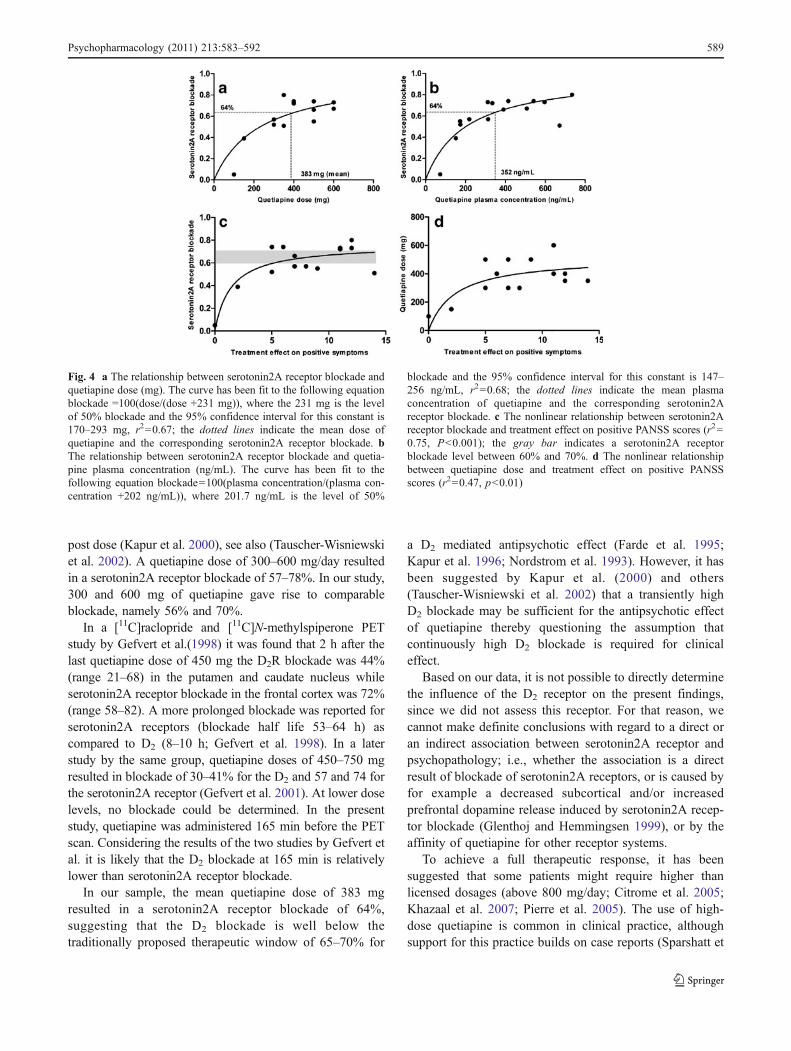
The equation of the one-site binding hyperbola that was usedto fit serotonin2A receptor blockade and quetiapine plasmaconcentration revealed an EC50 value of 201.7 ng/mL, with a95% confidence interval of 147.2–256.3 ng/mL, r2=0.68(see Fig. 4b).
The mean dose of quetiapine was 383 mg (range 100–600 mg) corresponding to a serotonin2A receptor blockadeof 64% and a plasma concentration of 352 ng/mL (range74–735 ng/mL; see also Fig. 3). Similarly, the equation thatwas used to fit serotonin2A receptor blockade andquetiapine dose resulted in a EC50 value of 231 mg witha 95% confidence interval of 170–293 mg, r2=0.67 (seeFig. 4a).
There was no statistically significant difference in thecerebellar distribution volume with and without quetiapinetreatment.
Fig. 2 Blockade plot in one of the patients showing paired (left andright) distribution volumes of the VOIs in the unblocked (VT) andpartially blocked situation (VT,b). Regression line: Y=0.6034x+0.7499, r2=0.9677, serotonin2A receptor blockade=40%
Psychopharmacology (2011) 213:583–592 587
Serotonin2A receptor blockade and psychopathology
The mean PANSS score of positive symptoms was signifi-cantly reduced (t(13)=3.5, p<0.01) after quetiapine treat-ment. The reductions in PANSS negative, general and totalscores were non-significant (see Table 1).
A significant nonlinear relationship was found betweenserotonin2A receptor blockade and treatment effect onpositive symptoms (r2=0.75, p<0.001, Fig. 4c) and betweendose and treatment effect on positive symptoms (r2=0.47,p<0.01, Fig. 4d). We performed post hoc analyses, wherewe excluded the data of the two patients who were oncurrent SSRI treatment. This did not change the curve fitssignificantly, neither did it change the significance level(r2=0.72, p<0.001 and r2=0.48, p<0.01). There was amodest effect on positive symptoms up until a serotonin2Areceptor blockade level of approximately 60%. Between60% and 70% serotonin2A receptor blockade levels(corresponding to doses of 336–538 mg/day) the seroto-nin2A receptor related treatment effect on positive symptomsappeared optimal. Above a serotonin2A receptor blockade of70% no additional serotonin2A receptor associated treatmenteffect was obtained (see Fig. 4c and d).
Neither a significant relationship was found betweenserotonin2A receptor blockade and treatment effect on thePANSS total score nor on the negative and general PANSSsubscales.
Discussion
In this 6-month longitudinal study of 15 initially antipsy-chotic naïve first-episode schizophrenia patients we foundsignificant nonlinear relationships between serotonin2Areceptor blockade, dose, and plasma concentration ofquetiapine. The optimal treatment effect on positivesymptoms associated with serotonin2A receptor blockadewas found with blockade levels between 60% and 70%(corresponding to 336–538 mg/day). The data revealed amodest effect on positive psychotic symptoms up untilapproximately 60% serotonin2A receptor blockade afterwhich a considerable increase in effect was found. Themean dose of quetiapine of 383 mg corresponded to aplasma concentration of 352 ng/mL and a serotonin2Areceptor blockade of 64%. This blockade level is in themiddle range between 60% and 70% where we foundserotonin2A receptor blockade to be associated with thehighest reduction in the positive symptoms.
Due to logistic and ethical reasons we were not able toconcurrently assess D2 blockade which is a fundamentallimitation of the study. Therefore, the potential involvementof the D2 receptor on the present findings requires thoroughconsideration and cautious interpretation.
In a [11C]raclopride and [18F]setoperone study of 12chronic schizophrenia patients, quetiapine doses of 400–450 mg resulted in D2 blockade of approximately 60% 2 h
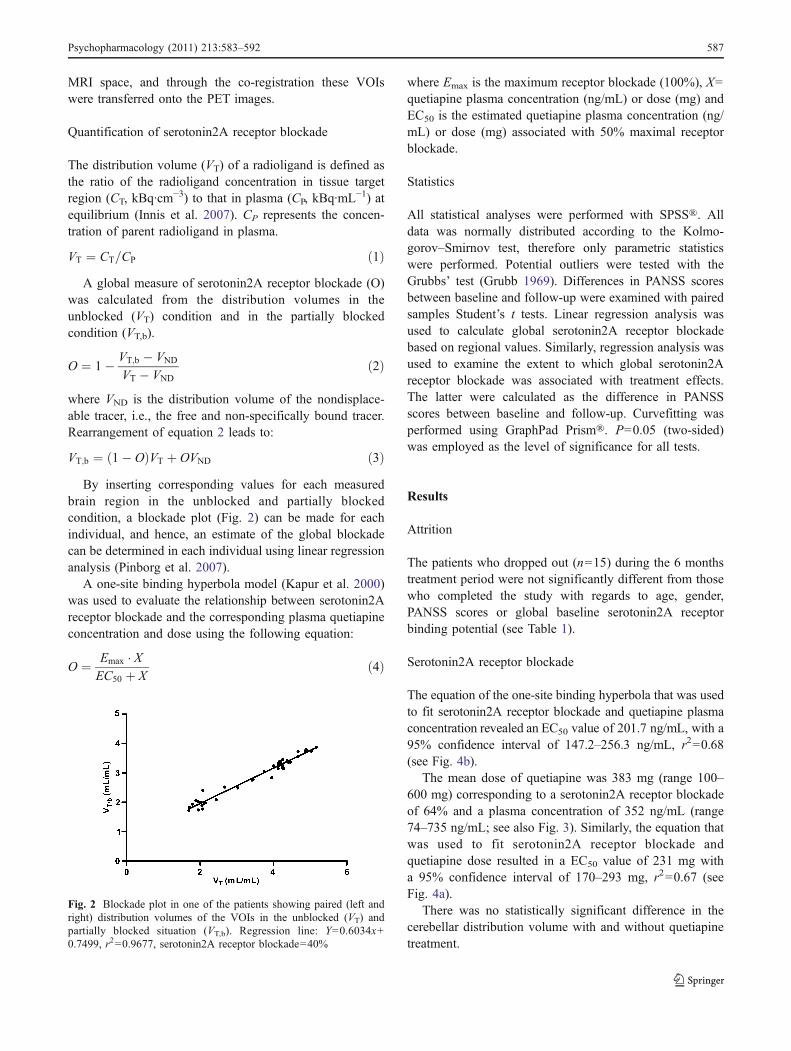
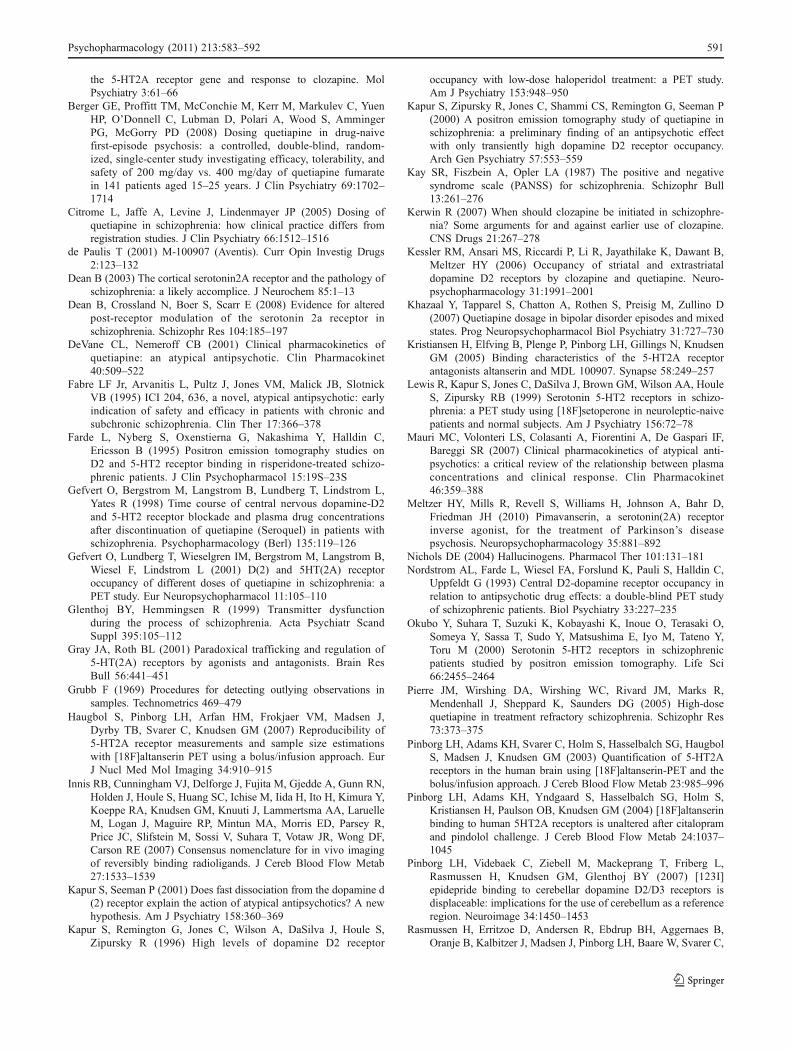
Fig. 3 [18F]altanserin PETimages of two axial brain slicesillustrating serotonin2A receptorbinding in one of the maleschizophrenic patients before(top) and after approximately6 months of treatment with300 mg/day quetiapine (bottom).Serotonin2A receptor blockade=57% (165 min post quetiapineadministration)
588 Psychopharmacology (2011) 213:583–592
post dose (Kapur et al. 2000), see also (Tauscher-Wisniewskiet al. 2002). A quetiapine dose of 300–600 mg/day resultedin a serotonin2A receptor blockade of 57–78%. In our study,300 and 600 mg of quetiapine gave rise to comparableblockade, namely 56% and 70%.
In a [11C]raclopride and [11C]N-methylspiperone PETstudy by Gefvert et al.(1998) it was found that 2 h after thelast quetiapine dose of 450 mg the D2R blockade was 44%(range 21–68) in the putamen and caudate nucleus whileserotonin2A receptor blockade in the frontal cortex was 72%(range 58–82). A more prolonged blockade was reported forserotonin2A receptors (blockade half life 53–64 h) ascompared to D2 (8–10 h; Gefvert et al. 1998). In a laterstudy by the same group, quetiapine doses of 450–750 mgresulted in blockade of 30–41% for the D2 and 57 and 74 forthe serotonin2A receptor (Gefvert et al. 2001). At lower doselevels, no blockade could be determined. In the presentstudy, quetiapine was administered 165 min before the PETscan. Considering the results of the two studies by Gefvert etal. it is likely that the D2 blockade at 165 min is relativelylower than serotonin2A receptor blockade.
In our sample, the mean quetiapine dose of 383 mgresulted in a serotonin2A receptor blockade of 64%,suggesting that the D2 blockade is well below thetraditionally proposed therapeutic window of 65–70% for
a D2 mediated antipsychotic effect (Farde et al. 1995;Kapur et al. 1996; Nordstrom et al. 1993). However, it hasbeen suggested by Kapur et al. (2000) and others(Tauscher-Wisniewski et al. 2002) that a transiently highD2 blockade may be sufficient for the antipsychotic effectof quetiapine thereby questioning the assumption thatcontinuously high D2 blockade is required for clinicaleffect.
Based on our data, it is not possible to directly determinethe influence of the D2 receptor on the present findings,since we did not assess this receptor. For that reason, wecannot make definite conclusions with regard to a direct oran indirect association between serotonin2A receptor andpsychopathology; i.e., whether the association is a directresult of blockade of serotonin2A receptors, or is caused byfor example a decreased subcortical and/or increasedprefrontal dopamine release induced by serotonin2A recep-tor blockade (Glenthoj and Hemmingsen 1999), or by theaffinity of quetiapine for other receptor systems.
To achieve a full therapeutic response, it has beensuggested that some patients might require higher thanlicensed dosages (above 800 mg/day; Citrome et al. 2005;Khazaal et al. 2007; Pierre et al. 2005). The use of high-dose quetiapine is common in clinical practice, althoughsupport for this practice builds on case reports (Sparshatt et
Fig. 4 a The relationship between serotonin2A receptor blockade andquetiapine dose (mg). The curve has been fit to the following equationblockade =100(dose/(dose +231 mg)), where the 231 mg is the levelof 50% blockade and the 95% confidence interval for this constant is170–293 mg, r2=0.67; the dotted lines indicate the mean dose ofquetiapine and the corresponding serotonin2A receptor blockade. bThe relationship between serotonin2A receptor blockade and quetia-pine plasma concentration (ng/mL). The curve has been fit to thefollowing equation blockade=100(plasma concentration/(plasma con-centration +202 ng/mL)), where 201.7 ng/mL is the level of 50%
blockade and the 95% confidence interval for this constant is 147–256 ng/mL, r2=0.68; the dotted lines indicate the mean plasmaconcentration of quetiapine and the corresponding serotonin2Areceptor blockade. c The nonlinear relationship between serotonin2Areceptor blockade and treatment effect on positive PANSS scores (r2=0.75, P<0.001); the gray bar indicates a serotonin2A receptorblockade level between 60% and 70%. d The nonlinear relationshipbetween quetiapine dose and treatment effect on positive PANSSscores (r2=0.47, p<0.01)
Psychopharmacology (2011) 213:583–592 589

al. 2008). For example, seven patients refractory totreatment with quetiapine in doses up to 800 mg/day, whowere subsequently treated with doses of 1,200–2,400 mg/day, showed modest to moderate clinical improvements interms of positive psychotic symptoms, behavioral distur-bances, violent behavior, and sociability. Currently, itcannot be ruled out that some patients have an additionaltherapeutic effect by very high doses of quetiapine, but thisneeds to be confirmed in controlled trials.
The present study indicates a serotonin2A receptorassociated therapeutic window on positive symptoms inresponding patients in the range between 60% and 70%blockade (336 and 538 mg quetiapine) in antipsychotic-naïvefirst-episode schizophrenia. Our observations may suggestthat in doses higher than approximately 538 mg/day (70%blockade) the antipsychotic effect of quetiapine may predom-inately be mediated through dopaminergic blockade. Thissuggests that patients who require high quetiapine dosesrequire a higher D2 blockade than can be obtained with lowquetiapine doses. Consequently, this could suggest thatpatients who respond to low doses of quetiapine (below538 mg) are those patients who rather require serotonin2Areceptor than D2 blockade. Interestingly, a recent meta-analysis (Sparshatt et al. 2008) on dose and clinical responseof quetiapine suggested that a low dose of 300–400 mg/dayis the optimal dose in first-episode patients (see also Bergeret al. 2008).
One of the strengths of the current study is theinclusion of only drug-naïve first-episode schizophreniapatients. In this sense, the patient group was homoge-nous, and avoided several possible confounding factorsassociated with illness, chronicity, age, and prior expo-sure to antipsychotic medication. Furthermore, due to thelongitudinal design obvious noise in the data as related toin between subject comparisons were avoided. Apartfrom the above-mentioned complexity regarding theinterpretation of the data resulting from the absence ofsimultaneous D2 and serotonin2A receptor assessments,there are additional limitations in the present study thatneed to be addressed.
At follow-up, we only obtained a binding measure in themedicated state. Therefore, we cannot make direct infer-ences regarding a potential paradoxical down-regulation ofserotonin2A receptors caused by the quetiapine treatment assuggested in (Dean 2003; Gray and Roth 2001).Hence, itcannot be excluded that the volume of distribution in theblocked state (VT,b) at follow-up might have been reducedby the 6 months quetiapine treatment. If indeed true, thenthis would have resulted in an overestimation of ourserotonin2A receptor occupancy data according to formula 2in the “Methods and materials” section.
Ideally, two scans should have been performed at follow-up, one in the medicated state and one at a quetiapine
plasma level of zero after discontinuation. However, forethical and logistical reasons this was not done.
Two out of the 15 patients were co-treated with SSRIsduring the treatment period, one with fluoxetine, the otherwith citalopram. Since these two compounds affect theserotonergic neurotransmitter system, they could haveinfluenced our results. The effect of chronic SSRI treatmenton serotonin2A receptor density is unclear, since differentSSRIs show different effects on serotonin2A receptors.Fluoxetine has been reported to have either no effect or toincrease serotonin2A receptor density or to increasereceptor number (Gray and Roth 2001). In contrast, chroniccitalopram treatment down-regulates serotonin2A receptors(Gray and Roth 2001). However, we have previously foundthat [18F]altanserin binding to serotonin2A receptors isinsensitive to an acute citalopram (SSRI) challenge(Pinborg et al. 2004). For these reasons, we performedpost hoc analyses, where we excluded the data of the twopatients who were on current SSRI treatment. This did notchange the curve fits significantly.
In conclusion, the present study suggests a therapeuticrole of the serotonin2A receptor for treatment of positivesymptoms in schizophrenia either directly or indirectly viainteractions with the dopaminergic system or other receptorsystems. The data point to a serotonin2A receptor associ-ated therapeutic window on positive symptoms in the rangebetween 60% and 70% blockade (336–538 mg/day ofquetiapine) in antipsychotic-naïve first-episode schizophre-nia. Future studies with concurrent measurement of otherreceptor systems are warranted.
Acknowledgments The study was sponsored by Danish MedicalResearch Council, Copenhagen Hospital Cooperation ResearchCouncil, Copenhagen University Hospital, Bispebjerg, The Universityof Copenhagen, Faculty of Health Sciences, The Copenhagen CounselResearch Foundation, The Gangsted Foundation, The LundbeckFoundation and a nonrestricted grant from AstraZeneca. We wouldlike to thank Dr Jacob Madsen and the PET & Cyclotron Unit,Copenhagen University Hospital Rigshospitalet, Denmark for techni-cal support.
Disclosure/conflicts of interest The authors have nothing todisclose and report no conflicts of interest.
References
Adams KH, Pinborg LH, Svarer C, Hasselbalch SG, Holm S, HaugbolS, Madsen K, Frokjaer V, Martiny L, Paulson OB, Knudsen GM(2004) A database of [(18)F]-altanserin binding to 5-HT(2A)receptors in normal volunteers: normative data and relationshipto physiological and demographic variables. Neuroimage21:1105–1113
Arranz MJ, Munro J, Owen MJ, Spurlock G, Sham PC, Zhao J, KirovG, Collier DA, Kerwin RW (1998) Evidence for associationbetween polymorphisms in the promoter and coding regions of
590 Psychopharmacology (2011) 213:583–592
the 5-HT2A receptor gene and response to clozapine. MolPsychiatry 3:61–66
Berger GE, Proffitt TM, McConchie M, Kerr M, Markulev C, YuenHP, O’Donnell C, Lubman D, Polari A, Wood S, AmmingerPG, McGorry PD (2008) Dosing quetiapine in drug-naivefirst-episode psychosis: a controlled, double-blind, random-ized, single-center study investigating efficacy, tolerability, andsafety of 200 mg/day vs. 400 mg/day of quetiapine fumaratein 141 patients aged 15–25 years. J Clin Psychiatry 69:1702–1714
Citrome L, Jaffe A, Levine J, Lindenmayer JP (2005) Dosing ofquetiapine in schizophrenia: how clinical practice differs fromregistration studies. J Clin Psychiatry 66:1512–1516
de Paulis T (2001) M-100907 (Aventis). Curr Opin Investig Drugs2:123–132
Dean B (2003) The cortical serotonin2A receptor and the pathology ofschizophrenia: a likely accomplice. J Neurochem 85:1–13
Dean B, Crossland N, Boer S, Scarr E (2008) Evidence for alteredpost-receptor modulation of the serotonin 2a receptor inschizophrenia. Schizophr Res 104:185–197
DeVane CL, Nemeroff CB (2001) Clinical pharmacokinetics ofquetiapine: an atypical antipsychotic. Clin Pharmacokinet40:509–522
Fabre LF Jr, Arvanitis L, Pultz J, Jones VM, Malick JB, SlotnickVB (1995) ICI 204, 636, a novel, atypical antipsychotic: earlyindication of safety and efficacy in patients with chronic andsubchronic schizophrenia. Clin Ther 17:366–378
Farde L, Nyberg S, Oxenstierna G, Nakashima Y, Halldin C,Ericsson B (1995) Positron emission tomography studies onD2 and 5-HT2 receptor binding in risperidone-treated schizo-phrenic patients. J Clin Psychopharmacol 15:19S–23S
Gefvert O, Bergstrom M, Langstrom B, Lundberg T, Lindstrom L,Yates R (1998) Time course of central nervous dopamine-D2and 5-HT2 receptor blockade and plasma drug concentrationsafter discontinuation of quetiapine (Seroquel) in patients withschizophrenia. Psychopharmacology (Berl) 135:119–126
Gefvert O, Lundberg T, Wieselgren IM, Bergstrom M, Langstrom B,Wiesel F, Lindstrom L (2001) D(2) and 5HT(2A) receptoroccupancy of different doses of quetiapine in schizophrenia: aPET study. Eur Neuropsychopharmacol 11:105–110
Glenthoj BY, Hemmingsen R (1999) Transmitter dysfunctionduring the process of schizophrenia. Acta Psychiatr ScandSuppl 395:105–112
Gray JA, Roth BL (2001) Paradoxical trafficking and regulation of5-HT(2A) receptors by agonists and antagonists. Brain ResBull 56:441–451
Grubb F (1969) Procedures for detecting outlying observations insamples. Technometrics 469–479
Haugbol S, Pinborg LH, Arfan HM, Frokjaer VM, Madsen J,Dyrby TB, Svarer C, Knudsen GM (2007) Reproducibility of5-HT2A receptor measurements and sample size estimationswith [18F]altanserin PET using a bolus/infusion approach. EurJ Nucl Med Mol Imaging 34:910–915
Innis RB, Cunningham VJ, Delforge J, Fujita M, Gjedde A, Gunn RN,Holden J, Houle S, Huang SC, Ichise M, Iida H, Ito H, Kimura Y,Koeppe RA, Knudsen GM, Knuuti J, Lammertsma AA, LaruelleM, Logan J, Maguire RP, Mintun MA, Morris ED, Parsey R,Price JC, Slifstein M, Sossi V, Suhara T, Votaw JR, Wong DF,Carson RE (2007) Consensus nomenclature for in vivo imagingof reversibly binding radioligands. J Cereb Blood Flow Metab27:1533–1539
Kapur S, Seeman P (2001) Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics? A newhypothesis. Am J Psychiatry 158:360–369
Kapur S, Remington G, Jones C, Wilson A, DaSilva J, Houle S,Zipursky R (1996) High levels of dopamine D2 receptor
occupancy with low-dose haloperidol treatment: a PET study.Am J Psychiatry 153:948–950
Kapur S, Zipursky R, Jones C, Shammi CS, Remington G, Seeman P(2000) A positron emission tomography study of quetiapine inschizophrenia: a preliminary finding of an antipsychotic effectwith only transiently high dopamine D2 receptor occupancy.Arch Gen Psychiatry 57:553–559
Kay SR, Fiszbein A, Opler LA (1987) The positive and negativesyndrome scale (PANSS) for schizophrenia. Schizophr Bull13:261–276
Kerwin R (2007) When should clozapine be initiated in schizophre-nia? Some arguments for and against earlier use of clozapine.CNS Drugs 21:267–278
Kessler RM, Ansari MS, Riccardi P, Li R, Jayathilake K, Dawant B,Meltzer HY (2006) Occupancy of striatal and extrastriataldopamine D2 receptors by clozapine and quetiapine. Neuro-psychopharmacology 31:1991–2001
Khazaal Y, Tapparel S, Chatton A, Rothen S, Preisig M, Zullino D(2007) Quetiapine dosage in bipolar disorder episodes and mixedstates. Prog Neuropsychopharmacol Biol Psychiatry 31:727–730
Kristiansen H, Elfving B, Plenge P, Pinborg LH, Gillings N, KnudsenGM (2005) Binding characteristics of the 5-HT2A receptorantagonists altanserin and MDL 100907. Synapse 58:249–257
Lewis R, Kapur S, Jones C, DaSilva J, Brown GM, Wilson AA, HouleS, Zipursky RB (1999) Serotonin 5-HT2 receptors in schizo-phrenia: a PET study using [18F]setoperone in neuroleptic-naivepatients and normal subjects. Am J Psychiatry 156:72–78
Mauri MC, Volonteri LS, Colasanti A, Fiorentini A, De Gaspari IF,Bareggi SR (2007) Clinical pharmacokinetics of atypical anti-psychotics: a critical review of the relationship between plasmaconcentrations and clinical response. Clin Pharmacokinet46:359–388
Meltzer HY, Mills R, Revell S, Williams H, Johnson A, Bahr D,Friedman JH (2010) Pimavanserin, a serotonin(2A) receptorinverse agonist, for the treatment of Parkinson’s diseasepsychosis. Neuropsychopharmacology 35:881–892
Nichols DE (2004) Hallucinogens. Pharmacol Ther 101:131–181Nordstrom AL, Farde L, Wiesel FA, Forslund K, Pauli S, Halldin C,
Uppfeldt G (1993) Central D2-dopamine receptor occupancy inrelation to antipsychotic drug effects: a double-blind PET studyof schizophrenic patients. Biol Psychiatry 33:227–235
Okubo Y, Suhara T, Suzuki K, Kobayashi K, Inoue O, Terasaki O,Someya Y, Sassa T, Sudo Y, Matsushima E, Iyo M, Tateno Y,Toru M (2000) Serotonin 5-HT2 receptors in schizophrenicpatients studied by positron emission tomography. Life Sci66:2455–2464
Pierre JM, Wirshing DA, Wirshing WC, Rivard JM, Marks R,Mendenhall J, Sheppard K, Saunders DG (2005) High-dosequetiapine in treatment refractory schizophrenia. Schizophr Res73:373–375
Pinborg LH, Adams KH, Svarer C, Holm S, Hasselbalch SG, HaugbolS, Madsen J, Knudsen GM (2003) Quantification of 5-HT2Areceptors in the human brain using [18F]altanserin-PET and thebolus/infusion approach. J Cereb Blood Flow Metab 23:985–996
Pinborg LH, Adams KH, Yndgaard S, Hasselbalch SG, Holm S,Kristiansen H, Paulson OB, Knudsen GM (2004) [18F]altanserinbinding to human 5HT2A receptors is unaltered after citalopramand pindolol challenge. J Cereb Blood Flow Metab 24:1037–1045
Pinborg LH, Videbaek C, Ziebell M, Mackeprang T, Friberg L,Rasmussen H, Knudsen GM, Glenthoj BY (2007) [123I]epidepride binding to cerebellar dopamine D2/D3 receptors isdisplaceable: implications for the use of cerebellum as a referenceregion. Neuroimage 34:1450–1453
Rasmussen H, Erritzoe D, Andersen R, Ebdrup BH, Aggernaes B,Oranje B, Kalbitzer J, Madsen J, Pinborg LH, Baare W, Svarer C,
Psychopharmacology (2011) 213:583–592 591

Lublin H, Knudsen GM, Glenthoj B (2010) Decreased frontalserotonin2A receptor binding in antipsychotic-naive patients withfirst-episode schizophrenia. Arch Gen Psychiatry 67:9–16
Small JG, Hirsch SR, Arvanitis LA, Miller BG, Link CG (1997)Quetiapine in patients with schizophrenia. A high- and low-dosedouble-blind comparison with placebo. Seroquel study group.Arch Gen Psychiatry 54:549–557
Snigdha S, Horiguchi M, Huang M, Li Z, Shahid M, Neill JC, MeltzerHY (2010) Attenuation of phencyclidine-induced object recog-nition deficits by the combination of atypical antipsychotic drugsand pimavanserin (ACP 103), a 5-hydroxytryptamine(2A) recep-tor inverse agonist. J Pharmacol Exp Ther 332:622–631
Sparshatt A, Jones S, Taylor D (2008) Quetiapine: dose–responserelationship in schizophrenia. CNS Drugs 22:49–68
Svarer C, Madsen K, Hasselbalch SG, Pinborg LH, Haugbol S,Frokjaer VG, Holm S, Paulson OB, Knudsen GM (2005) MR-based automatic delineation of volumes of interest in humanbrain PET images using probability maps. Neuroimage 24:969–979
Tan PZ, Baldwin RM, Van Dyck CH, Al-Tikriti M, Roth B, Khan N,Charney DS, Innis RB (1999) Characterization of radioactivemetabolites of 5-HT2A receptor PET ligand [18F]altanserin inhuman and rodent. Nucl Med Biol 26:601–608
Tauscher-Wisniewski S, Kapur S, Tauscher J, Jones C, Daskalakis ZJ,Papatheodorou G, Epstein I, Christensen BK, Zipursky RB(2002) Quetiapine: an effective antipsychotic in first-episodeschizophrenia despite only transiently high dopamine-2 receptorblockade. J Clin Psychiatry 63:992–997
Trichard C, Paillere-Martinot ML, Attar-Levy D, Blin J, Feline A,Martinot JL (1998) No serotonin 5-HT2A receptor densityabnormality in the cortex of schizophrenic patients studied withPET. Schizophr Res 31:13–17
Verhoeff NP, Meyer JH, Kecojevic A, Hussey D, Lewis R, Tauscher J,Zipursky RB, Kapur S (2000) A voxel-by-voxel analysis of [18F]setoperone PET data shows no substantial serotonin 5-HT(2A)receptor changes in schizophrenia. Psychiatry Res 99:123–135
Willendrup P, Pinborg LH, Hasselbalch SG, Adams KH, Stahr K,Knudsen GM, Svarer C (2008) Assessment of the precision in co-registration of structural MR-images and PET-images with localizedbinding. Int Congress Series, ISBN: 0444515674, 275–280
Wing JK, Babor T, Brugha T, Burke J, Cooper JE, Giel R, JablenskiA, Regier D, Sartorius N (1990) SCAN. Schedules for clinicalassessment in neuropsychiatry. Arch Gen Psychiatry 47:589–593
Woods RP, Cherry SR, Mazziotta JC (1992) Rapid automatedalgorithm for aligning and reslicing PET images. J ComputAssist Tomogr 16:620–633
592 Psychopharmacology (2011) 213:583–592





























