Embed Size (px)
Citation preview

November 1993 Sankara Nethralaya Number 5
Serving India for 15 Years – 1978 – 1993 An Open House was held on Octorber 2 –3 at Sankara Nethralaya featuring talks by consultants on various eye problems and exhibits. One big difference from last year was that the exhibits were made more interative: -children could check their binocular vision themselves; -people understood the concept of a blind spot by a simple experiment;
-people could see an intraocular lens through a microscope; -many of them could for the first time see a human chromosome under the microscopes displayed by the genetics department of the Vision Research Foundation. The talks by consultants were well attended and the halls were packed, with people spilling on to the corridors. The talks were accompanied by slides, patient education
videos and animated discussion between the consultant and the audience. More than 1500 people visited the exhibition, and response was uniformaly good. One visitor when asked whether there was any poster he did not understand – said proudly “I understand everything!” A lot of people including medical students were seen noting down information from the displays. The response of the visitors could be gauged by their comments and suggestions. There was a unanimous request for another exhibition next year. Some even wanted it more frequently. There was also a request to have more posters in Tamil.

On October 3, 1993, the new block was dedicated to His Holiness Paramacharya Sri Chandrashekharendra Saraswati Swamy of Kanchi Kamakoti Peetam on the occasion of his 100th birthday. His Holiness Sri Jayendra Saraswati and His Holiness Sri Vijayendra Saraswati dedicated the building. The building will be called the Mahyco Block after Mr. B.R.Barwale of Mahyco (Maharastra Hybrid Seeds Company) who donated a large sum of money to the Foundation.
Nethralaya looks back on 15 years of service, treatment and giving – giving the gift of sight.

Nethralaya News In keeping with the aim to educate the public regarding health and eye care, Nethralaya is trying to spread the message regarding galactrosemia during pregency leading to congenital cataract in children. Pregnant women coming to Nethralaya are being warned about this possible complication, and prominent posters are being displayed. An attempt is being made to educate the public in Tamil and English on avoiding milk in galactosemia through social service organizations. The message about galactosemia is also being spread through the department of Obsterics and Gynecology in the medical colleges and the maternity hospitals. Exclusive camps for pregnant women will be conducted at Nethralaya where urine samples will be collected and tested.
* Tobacco plants imbibe concentrated cadmium salts from earth, Hence smoke from cigarettes and beedies contains significant amounts of cadmium which is unphysiological and a toxic element like mercury. It is reported that smokers have increased levels of cadmium in blood, milk and tissues. The cadmium binds with haemoglobin in the blood, kidneys and liver with a maximum in the lungs. West and other scientists from John Hopkins Medical School, USA reported that cataract developed in the nucleus(middle portion) of the lens on smoking. When smoking was stopped for a reasonable time, the cataract cleared. As the cataract was reversible, it was thought that it could not be cellular damage but just a chemical pathology. An accumulations of cadmium in the lens in smokers of relatively younger age could cause cataract by various mechanisms. The department of biochemistry at Nethralaya in collaboration with Stanley Medical College, Government Veterinary College and Indian Institute of Technology (I.I.T) analysed cadmium in the blood and lens of the smokers. Analysis of cadmium was done in the blood and lens of the smokers (average age57) who smoke not less than ten beedies a day continuously for many years and non-smokers of the same age group. It was found that there was a significant accumulation of cadmium in both the blood and the lens of the smokers. Such an accumulation of cadmium may have a role in cataractogenesis in chronic smokers. In a similar experiment with smokers and non-smokers of average age of 35 years, increased levels of cadmium was found in the blood of smokers though, the extent of accumulation was not as high as in chronic smokers of age group 57.
* Dr.S.S.badrinath and Dr.(Mrs) Vasanthi Badrinath attended the workshop held at Assam Nethralaya from September 24-28 on the basic steps of vitreo-retinal surgery and recent developments.
*

A workshop – “Update on corneal topography” tookl place at Nethralaya on October 7, 1993. Dr.Prema Padmanabhan was the organizing secretary. Dr.Charles Casebeer, a cornea specialist from U.S.A was the guest speaker.
* The Molecular Biology and Genetics laboratory was inaugurated on September 6, 1993. Dr.M.Dharmarajan former professor of Genetics, Madras Veterinary College presided over the function.
* A workshop on “Training of Trainers in ECCE & IOL surgery” organized by the Government of India, Ministry of Health was held at our hospital premises.
*
Looking Ahead December 2 – 3, 1993 The third annual meeting of the Glaucoma Society of India will be held at Sankara Nethralaya. It will consist of panel discussions and case presentations in addition to a medical and laser update. December 6, 1993 Shri Bhagawan Mahavir Vitreo Retinal Service and Nethralaya together are organizing an Advanced course on Diseases of the Vitreous and Retina.
This issue of EyeLights is sponsored by: Rampion Eyetech Pvt.Ltd. – Kailash, New Sharda Mandir Road, Paldi, Ahmedabad – 380 007 Apex Laboratories Pvt.Ltd. – 44, Gandhi Mandapam Road, Kotturpuram, Madras – 600 085 Khosla & Company - Sudesh Building, Kennedy Bridge, Nanachowk, Bomaby – 400 007

Refractive Errors of the Eye In a normal eye, the light rays from a distant object are focused on the retina, when the eye is at rest.
When a refractive error occurs, the light rays do not come to a focus on the reina. Refractive errors are the most common cause of poor vision. Lenses correct a refractive error by altering the paths of light rays to cancel out the misfousing introduced by defects in the eye’s own focusing system.
The eye does not focus the way a camera does. Most of the job is done by the cornea, which is not adjustable. The lens, behind the cornea, is adjustable to make the slight changes necessary to focus on the retina. Unlike a camera lens, the human lens does not move back and forth to make these adjustments, instead, it changes its shape. Variations in the shape may affect the ability to focus and may make glasses necessary. These variations introduce three common defects of vision – Hyperopia Myopia Astigmatism Hyperopia This is caused by -an eyeball that is slightly shorter front to back than a normal eye. -insufficient curvature of the cornea. As a result, the lightrays from an object come to a focus at a point behind the retina.
These conditions have little effect on the ability to see objects more than 20 feet away, because light rays from distant objects are essentially parallel are require little bending inward to make them converge at a point on the retina. However, near objects do appear blurred, because the rays of light are diverging when they reach the eye. The remedy is simple and effective; The addition of an external convex lens supplies the converging power essential to bring the light
rays to focus on the cornea.
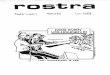
Myopia This condition is caused by an eye ball that is too long. As a result, the light rays from an object come to a focus in front of the retina. Due to this condition, near objects are seen more clearly than distant ones. Myopia usually develops in the school going age and ceases when full maturity is reached. The Progress of myopia cannot be halted or accelerated.
A concave lens provides the requisite correcting power to bring light rays to a focus on the retina. Astigmatism
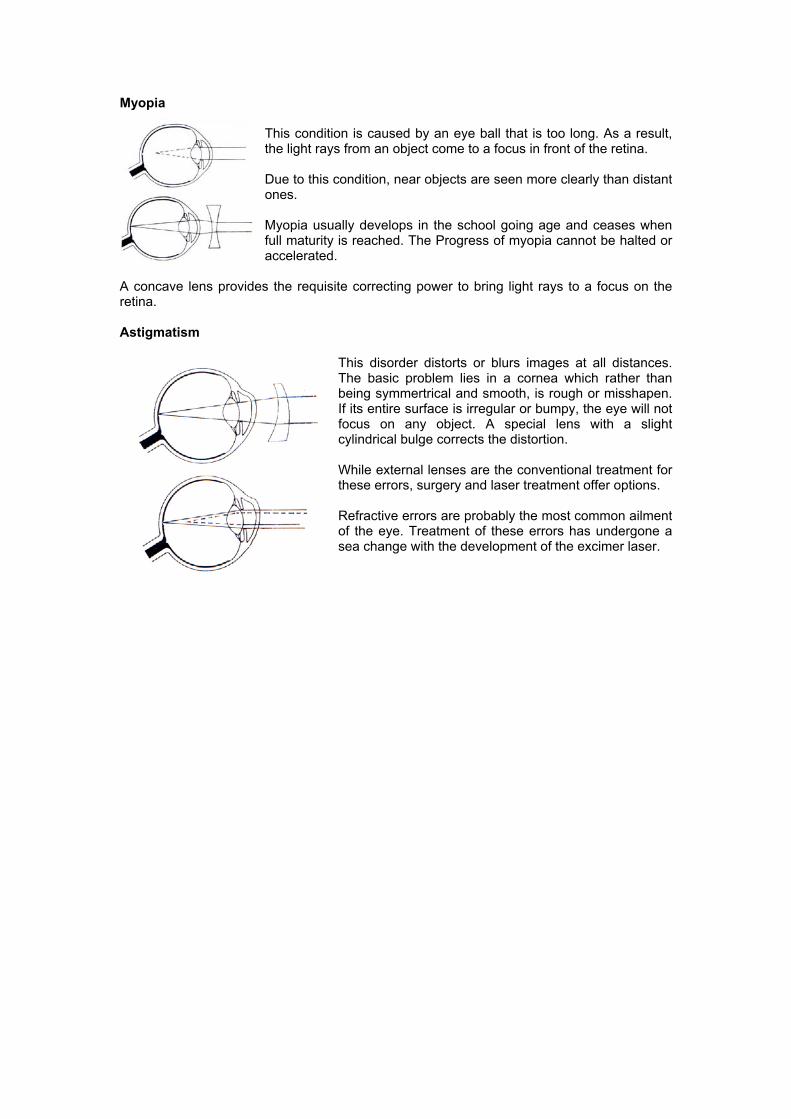
This disorder distorts or blurs images at all distances. The basic problem lies in a cornea which rather than being symmertrical and smooth, is rough or misshapen. If its entire surface is irregular or bumpy, the eye will not focus on any object. A special lens with a slight cylindrical bulge corrects the distortion. While external lenses are the conventional treatment for these errors, surgery and laser treatment offer options. Refractive errors are probably the most common ailment of the eye. Treatment of these errors has undergone a sea change with the development of the excimer laser.
Will Spectacles become Obsolete? The revolution that microsurgical tools have brought in the treatment of common eye ailments has been unparalleled. One new instrument, the laser, which generates an intense, sharply focused beam of light, can painlessly burn precise holes in tissue in a fraction of a second to remedy several eye disorders. The laser offers an alternative that requires no hospitalization and none of the emotional ordeal of operating room surgery. The patient, sitting up, places his chin on a special rest to keep his head steady. After using a drop or two of anesthetic to numb the cornea, the ophthalmologist taps a foot pedal four or five times. As early as 1949, ophthalmologists attempted to burn the tissues away with beams of sunlight focused through a complicated optical system. Later various other powerful light sources were used for this so-called photocoagulation, but no other instrument can match the laser for the intensity and precision of its beam. What is the Excimer Laser? The Excimer laser used to sculpt the cornea uses argon fluoride (ArF), which is an inert gas, to produce invisible ultraviolet energy. The word “excimer” is a contraction of “excited dimmer”. Dimer merely refers to a combination of two atoms. The laser energy generated is precisely focused by sophisticated optical delivery systems. Excimer laser have been used in industry for several years. After extensive testing in animals and then blind and partially sighted human eyes, they are now used in the treatment of myopia and other refractive disorders and also superficial opacities of the cornea. Excimer lasers have very short pulses, and hence their penetration into tissue is extremely small. How does the laser work? The laser works by a process called photoablative decomposition. The high energy photons of the laser beam destroy the intermolecular bonds in corneal tissue resulting in tissue removal. There is no appreciable damage to the surrounding tissues. What are the uses of the Excimer Laser? Photo-therapeutic keratectomy; Refers to the procedure whereby the laser is used to remove superficial opacities from the cornea. Photorefractive keratectomy refers to the procedure whereby the laser is used to correct refractive errors. The procedure is performed on an outpatient basis and no hospitalization is needed. The actual laser treatment takes about 20 seconds, while the entire procedure would take 20-30 minutes.

The procedure which is painless, is performed after instilling local anesthetic drops in the eye. Following the treatment, the eye is patched. The patch is discarded after about 48 hours after the procedure but this can be easily controlled by analgesics. Only one eye is treated at a time. Final stabilization of vision occurs at 3 to 6 months. The Summit excimer has been used to perform almost 30,000, procedures and the results have been encouraging. Some patients may need a second laser procedure either to remove residual myopia or to treat a trouble some corneal haze that has been seen to persist in a small percentage of patients after 6 months. Clinical trials have established the long term safety of this procedure. Minor complications encountered include under or over correction, some regression of effect, a mild anterior stromal haze that usually regresses by 1-6 months, and reactivation of Herpes simplex virus corneal involvement in some patients.
Thus, one of the major advantages of the excimer laser system is the precision with which it removes tissue. Also, the adjacent stromal tissue suffers neither distortion nor damage, Armed with the ability to create such precise alterations in the corneal curvature, the surgeon is able to tackle the problem of correcting myopia in a reliable and reproducible fashion. While most of the applications of the excimer laser today are in correcting myopia, rapid advances are also being made in the use of this later to treat astigmatism and heperopia.
Today one person in three is unlucky enough to suffer poor vision mostly refractive errors of the eye. As a result, glasses or contact lenses are the most common physical aid worn. In the 1970s, Russian surgeons began to repair the cornea by making cuts on the corneal surface with diamond tipped knives.
The eximer laser borrows the sam idea, but uss a fine knife – the laser beam. The excimer laser works in the ultra violet range, with pulses that are potent enough to wear away the cornea, but too brief to cause damage. Prior to the excimer laser, surgical correction of refractive errors was a tedious procedure involving hospitalization and the risks that go with it. Thus is was only greatest need that compelled an individual to undergo surgery. The excimer laser changes all that. It is now a 20 minute procedure with no hospital stay, and that makes it an appealing thought. Considering the problems associated with glasses that are noticeable and breakable, and contact lenses that slip, excimer treatment becomes a possible alternative.
However, spectacles cannot be avoided all together. Excimer treatment is possible only when the power in the eyes has stabilized. Since this normally happens at maturity, people under the age of 20 will have to continue wearing glasses. Reading glasses for the aged to compensate for the stiffening of the lens will also be required. It is a futuristic scenario akin to science fiction to think of the world without glasses. However with the strides made by science, one is justified in asking the question – will spectacles become obsolete?
Myopia Correction Profile Hyperopia Correction Profile

What is an Eye Examination In spite of all precaution, disease threatens or attacks the eye, with consequences that range from discomfort to blindness and it must be averted or cured. Sooner or later, most people need eyeglasses. The need generally begins during childhood or adolescence and chages throughout life so that the eyes require new lens prescriptions from time to time. Oddly enough, many people who should be using eye glasses are not aware of it, for the eye has amazing power to adapt to abnormalities. Dr.David Miller of Harward relates the case of a nurse who worked with him in surgery. While she was preparing the instruments table for an operation, one of the very fine sutures, with the needle attached, fell into the black-and-white checkered floor by accident. She was on her hands and knees looking for the suture and needle – a seemingly futile effort on such a confusing background. All at once she stopped, reached down, and came up grinning with the suture. Not long after this episode, she came into the eye clinic for a routine checkup, and proved to be extremely nearsighted. “Yet,” he noted, “under my very eyes, this nurse had performed a visual miracle.” The scheduling of eye checkups is important, Most doctors now recommend that the first complete examination take place when a child is about three years old. Vision is rapidly stabilizing at that stage, but it is still flexible enough to be corrected for problems of development. For children with healthy eyes, the second visit should be made at the age of five or six, just before they start elementary school. From then on, those youngsters who wear corrective lenses should be examined every 18 months or so; those who do not, at intervals of 2 or 3 years. There are three kinds of professionals specializing in eye care, and the differences among them confuse many people. An ophthalmologist is a medical doctor with advanced training in eye disorders – this specialist tests eyes for all kinds of diseases and defects, prescribes corrective lenses, administers eye medicines and performs eye operations. An optometrist is not a physican but rather an expert in testing eyes for focusing defects and in prescribing lenses to correct them. This practitioner does not treat other disorders, but may detect them in the course of an examination and will refer those cases to an ophthalmologist. The optician is a licensed technician comparable to a pharmacist. This specialist fills prescription lenses for the customer. He performs no examinations and prescribes no remedies. The obvious choice for all-round eye care and regular examinations is the most versatile of these professionals, the ophthalmologist physican. However, when corrective lenses are required, the optometrist is sometimes the most skilled as fitting lenses is his only work. Apart from knowing who to consult, one should also be aware of when to undergo an eye examination.

1.Ocular signs and symptoms a.Loss, distortion or dimness of vision. b.Pain in and around the eyes c.Excessive tears or discharge from the eyes d.Swelling of the eyelids or protrusion of the eye e.Double vision, floaters, flashes, etc. f.Sudden crossing or deviation of the eye 2.Risk factors for ocular disease a.Diabetes b.Hypertension c.Family history of glaucoma, cataract, squint d.Retinal detachment e.Over the age of 65 3.Other Factors a.Patients on long term medication such as steroid etc. b.Children with a family history of ocular disease c.Premature babies Even a routine eye examination requires an array of machines whose magnifying lenses, high intensity light beams and delicate probes allows a doctor to watch an eye in action, look for signs of disease or optical flaws and even measure pressure inside the eye ball. A thorough eye examination aims at the diagnosis, treatment, improvement and preservation of vision. 1.It begins with a detailed study of the ocular and relevant medical history. 2.Then the doctor examines the lids and the visible part of the eyeball for any signs of redness, inflammation or growths. 3.Then,preliminary tests for muscle balance, depth perception, peripheral vision,color blindness and faulty focus are conducted. These tests involve simple maneuvers as reading an eye chart with one eye covered, looking at pictures through 3-D glasses, and following a penlight or the doctor’s moving finger with the eyes. The standard test, which measures the ability to make out details of distant objects, is familiar enough. With one eye covered, the patient reads aloud the lines of letters or numbers on a chart or projection screen 6 meters away. Each line is set in a type size smaller than the one above, it; when the subject reaches a line whose individual characters are too small to be distinguished, the test for that eye is tested. The smallest type that the patient is able to read gives a numerical grade for vision—6\36, 6\12, or the 6\6 that is generally considered normal. Each eye receives its own rating – a person may have 6\6 vision in one eye and 6\12 in the other. The ratings compare a patient’s eyes with those of an anonymous young man who lived more than a century ago in the Netherlands. The eye charts is called the Snellen chart, after th Dutch ophthalmologist, Dr.Herman Snellen, who perfected it in 1864. Having worked out a system of printed lines graduated in size, Dr.Snellen sought for a standard or bench mark against which to measure the sight of his subjects. He found it in his own assistant, a man of acute and exceptionally adopted by Dr.Snellen as normal. The name of the assistant is lost to history, but people all over the world have been pitting their sight against his ever since.

The first number in a Snellen rating is the distance of the subject from the chart – always 6 metres. The second number, which is different for each line on the chart, is the distance at which Dr.Snellen’s assistant was able to read that line. 4.Then the doctor may check reflexes for blinking and producing tears. 5.The ophthalmologist then goes on to study the interior of the eye aided by the unique anatomy of the organ. The eye is the only structure in the body made up of transparent components – the cornea, the open pupil, the lens and the fluids that fill the eyeball. The doctor studies the interior of the eye, taking advantage of the fact that when the pupil is enlarged and kept open with dilating drops, it becomes a two-way window. A slit lamp focuses a narrow beam of light at a sharp angle into a patient’s eye while the doctor inspects inner and outer sections of her eye through a microscope. The light reaching the eye at an angle reveals defects not visible under head-on illumination – just as an apparently clear watch crystal shows scratches at angles across it. 6.On an eye anesthetized and stained with dye that glows phosphorescent blue, the doctor tests for glaucoma with an applanation tonometer. 7.After the patient’s pupils have been dilated and his near focusing muscles temporarily paralyzed with eye drops, the doctor asks him to look across the darkened room while he surveys the rear wall of his inner eye through an ophthalmoscope. A light in the instrument’s shaft bounces off an angled mirror just above it into the eye and the retina;from a series of lenses on a rotating wheel under his finger, the doctor selects one that gives him a clear view. Because the retina is the only part of the body where nerves and blood vessels are visible, the doctor making an ophthalmoscope examination can detect signs of disorders such as high blood pressure and diabetes as well damage to the retina and optic nerve. Based on his examination, the doctor will prescribe the treatment -spectacles or contact lenes -vision therapy -low vision aids -referral to physicians for general health problems -medication -surgery

AN APPEAL AN APPEAL
Eye care is not merely the need of the blind or those approaching blindness. There are millions of perfectly healthy people in the world who have refractive errors of the eye and require glasses.
Eye care is not merely the need of the blind or those approaching blindness. There are millions of perfectly healthy people in the world who have refractive errors of the eye and require glasses. The yardstick for a good medical institution is not merely one that can provide quality care in specialized cases, but one that can provide it in all cases however minor the problem might be.
The yardstick for a good medical institution is not merely one that can provide quality care in specialized cases, but one that can provide it in all cases however minor the problem might be. That is the aim of Sankara Nethralaya – to give the best care to your eyes, and the eyes of those around you. That is the aim of Sankara Nethralaya – to give the best care to your eyes, and the eyes of those around you. So come and join the Ophthalmic Mission Trust. So come and join the Ophthalmic Mission Trust. For questions about tax except status and contributions, please contact. For questions about tax except status and contributions, please contact. Mr. S.V.Acharya, Secretary and Treasurer, Mr. S.V.Acharya, Secretary and Treasurer, Ophthalmic Mission Trust Inc., Ophthalmic Mission Trust Inc., 14613, Pomml Drive, 14613, Pomml Drive, Rockville, Rockville, Maryland 20850 Maryland 20850 USA USA Phone : (301) 251 0378 Phone : (301) 251 0378 Fax : (202) 293 0448 Fax : (202) 293 0448 For those of you in India and elsewhere, please contact: For those of you in India and elsewhere, please contact: Dr.S.S.Badrinath Dr.S.S.Badrinath Medical Director Medical Director Medical Research Foundation Medical Research Foundation 18, College Road, 18, College Road, Madras 600 006 Madras 600 006 Tamil Nadu Tamil Nadu India India Phone : (044) 827 1616 Phone : (044) 827 1616 Fax : (044) 825 4180 Fax : (044) 825 4180 Come, give the gift of sight Come, give the gift of sight

Talking to R.K.Narayanan “When I as about 7 or 8 years old, I kept praying that the doctor would prescribe glasses for me. I thought it a very smart thing to have.” It is with this sort of wry humour that R.K.Narayanan talks about most things in life. It is the flavour that characterizes his writing, and colours his outlook on the world. A patient of Nethralaya, he goes on to talk about eye treatment in the early days.” It was torture, “ he says. However he applauds the sentiments of the doctors back then who seldom told their patients the details of what was wrong. “The more you learn about physical health, the less peaceful you are. “Back in the 1920s, the concept of blood pressure was unknown. There was drawing room talk about a new notion called blood pressure – people would laugh and joke about it. “It’s not just the fact that a little knowledge is a dangerous thing. It’s unwanted knowledge that is dangerous thing.
“One cannot deny the value of information, but it creates complexes. I never question the doctor, I just implicitly follow his advice. “Nowadays there is too must information, too much media pressure, and a lot of talk about things that are of no concern to us. “At any rate, at my age, you want to be aloof from everything. I don’t watch anything, and it’s not worth watching either.” It was propably this view of life that allowed him to enjoy the isolation imposed on him during his cataract surgery.
“It was great fun having cataract. You see much less – why should you see so much?
They ( Nethralaya) pampered me. While recuperating with his eyes bandaged, he wrote the story called “Breath of Lucifer” It is a story about the experience of a person undergoin the surgery, who is dragged out of isolation, by a drunken nurse who believes that the building is on fire. “Nature has so designed us, “he says in the story, “that we are compelled to spend at least eight hours out of twenty four with eyes shut in sleep or in an attempt to sleep. It is a compensatory arrangement, perhaps, for the strain the visual faculty undergoes during our waking hours, owing to the glut of image impinging on it.” He dictated the story while his eyes were bandaged, and the prologue to the story is characterized by his insight in his descriptions of the surgery and the discomfort preceding it. “Unnoticed, little by little my right eye had been growing dimmer in the course of a year or two. I felt annoyed by the presence of a smudge of oil on the lens of my spectacles which I pulled out and wiped with a handkerchief every other minute. When I tried to read, the smudge appeared on the first line and traveled down, line by line, and also touched up the faces and friends and foes alike whenever I happened to examine a photograph. As I raised

my eyes the blot also lifted itself upward. I couldn’t watch a movie without noticing an unseemly mole on the star’s much prized face. No amount of cleaning my spectacles was any us.” “Everyone speaks of the simplicity of the operation, “ he goes on to say. “It’s simple in the sense that it is painless, accomplished without bloodshed. But it is a delicate and responsible task demanding the utmost concentration of his (the surgeon’s) power at his finger tips, which will have to be hover with the lightness of the butterfly over the patient’s eye….” R.K.Narayanan is a weaver of words – words that say and do just what he wants. His is the power is expression and three
simple words express all he has to say about Nethralaya – “They pampered me.”
Edited, designed and produced by Masterpage For Private Circulation Only Printed at Gnanodays Press













![SEĆANJE SVILE....QMLJH SRH]LMH 7DQMH .UDJXMHYLü 9UDWLR VH 9RORÿD, 1966. Nesan,1973. Stud, 1978. Samica, 1986. 2VPHMDN RPþLFH, 1993. Divlji bulevar, 1993. Muška srma, l993. Duša](https://img.pdfslide.net/doc/110x75/60c35ab691e3002a7428b440/seanje-qmljh-srhlmh-7dqmh-udjxmhyl-9udwlr-vh-9rord-1966-nesan1973.jpg)