Embed Size (px)
Citation preview

HMCL211
www.endeavour.edu.au
Session 11
Clinical Skills 1
Naturopathic/Nutritional Medicine
Departments

© Endeavour College of Natural Health www.endeavour.edu.au 2
Introduction
o Case-taking skills & SOAP algorithms
o Models for organising information and
making informed decisions
• Introduction to SOAP note documentation
• Subjective vs Objective information (S vs OAP,
symptoms versus signs), how to differentiate data
• Professional communication & interaction
• Building patient/practitioner rapport
• Asking the right questions (leading, open-ended)
• Prioritising information

© Endeavour College of Natural Health www.endeavour.edu.au 3
Client Care
o Client Care is essentially about TWO things:
Evaluation & Management
o Evaluation, like it sounds, is essentially
determining what we believe is going on;
o Management, of course, is what we intend to
do about it.
© Endeavour College of Natural Health www.endeavour.edu.au 4
Client Care
o On a clinical level:
o Evaluation is more specifically the history and
case-taking, the examinations and everything
that leads to our assessment.
o Management is therefore the therapeutic
strategy and treatment plan(s).
Image: Experienced strategic planner,
www.rtacpa.com, viewed 26th November 2014

© Endeavour College of Natural Health www.endeavour.edu.au 5
SOAP
o A common, globally used acronym that is
helpful in describing and organizing client care
is SOAP:
• S=Subjective
• O=Objective
• A=Assessment
• P=Plan

© Endeavour College of Natural Health www.endeavour.edu.au 6
SOAP
o SOAP serves as evaluation tool which helps
provide a rationale for plan(s)
o SOAP note documentation systems are used
by all types of providers (Acupuncturists,
Nutritionists, Naturopaths, Nurses, GP’s,
Surgeons) across the world. Once
understood, it is a simple and very helpful
system to implement.

© Endeavour College of Natural Health www.endeavour.edu.au 7
SOAP
o Effective SOAP documentation help you to:
• Organise the clinical data.
• Facilitate clinical reasoning.
• Effectively communicate essential
information to other health care
professionals involved in client care e.g. the
supervisor, student colleagues.

© Endeavour College of Natural Health www.endeavour.edu.au 8
Subjective Data
o S (Subjective) data is essentially the client's
experience. It includes:
• What they FEEL; their SYMPTOMS.
• It’s the client's description of their
presenting complaint and information given
by the client or caregiver.
• Things observed about the client
(Holle, 2014)

© Endeavour College of Natural Health www.endeavour.edu.au 9
Subjective Data
o S (Subjective) data may be gathered from:
• The presenting complaint (PC)
• The history of illness
• The past medical history
• Family history
• Social history
o What are some examples of subjective data?

© Endeavour College of Natural Health www.endeavour.edu.au 10
Objective Data
o O (Objective) data is what we (the clinician)
can appreciate including:
• What we can see or MEASURE.
• The client's SIGNS.
• Information gathered by verifiable means
• Only pertinent data included
o What are some examples of objective data?

© Endeavour College of Natural Health www.endeavour.edu.au 11
Objective Data
o O (Objective) data may be gathered from:
• The primary source is physical examination but O
also includes laboratory values and diagnostic
tests/procedures
• Vitale signs – temperature, pulse, RR and BP
• Weight, height and waist measurement
• Physical examination – CV, skin, Iris, tongue, etc
• Nutritional signs examination – deficiency signs
• Laboratory evaluations – lipids, iron studies, urine
• Diagnostic tests – X-ray, CT, MRI scans
(Holle, 2014)

© Endeavour College of Natural Health www.endeavour.edu.au 12
Assessment
o A (Assessment) is the evaluation of the
collected subjective and objective information.
o This stage involves critical thinking by the
practitioner.
o The assessment of what is happening for the
client serves as a rationale for the treatment
plan(s)
o The assessment stage is always client and
encounter specific (i.e. individual)
(Holle, 2014)

© Endeavour College of Natural Health www.endeavour.edu.au 13
Plan
• P (Plan) is perhaps the easiest to understand; it is
the action steps and treatment plan needed for
each identified and assessed problem.
• The plan consists of the therapeutic strategy, the
treatment aims (both short- and long-term),
prescription, expected outcomes and any
necessary follow-up.
• PLAN may very well include referrals, additional
investigations.

© Endeavour College of Natural Health www.endeavour.edu.au 14
SOAP
o A simple way of understanding the relevance
of SOAP algorithms and how to implement
them in client care is:
S + O = A P o The Subjective + Objective data combine to
lead us to the Assessment which ultimately
drives our Plan.

© Endeavour College of Natural Health www.endeavour.edu.au 15
SOAP
o Potential issues with SOAP:
• Speaking: Poor elocution skills.
• Acquisition of Knowledge: Topic specific knowledge
deficits (facts or experience).
• Facts: Reports incorrect facts or omits facts.
• Expectations: Unaware of needs of listener or
standards.
• Reasoning: Omits or incorrectly applies clinical
reasoning.

© Endeavour College of Natural Health www.endeavour.edu.au 16
SOAP
Group Discussion:
o How might SOAP fit into client encounters?
o How might SOAP effect data collection?
o How might SOAP determine chart notes?
o How might SOAP specifically incorporate the
principles of Natural Medicine:
• First do no harm
• Find the cause
• Treat the whole person

© Endeavour College of Natural Health www.endeavour.edu.au 17
Professional Communication &
Interaction
Practitioner - Practitioner
© Endeavour College of Natural Health www.endeavour.edu.au 18
Professional Communication
o As discussed in Session 6, the need for
effective inter-professional communication is
important for:
• Effective integrative health care for clients
• Risk minimisation with regard to conventional and
CAM interactions and client safety events
o To this end, standardised formats provide a
way of minimising barriers and improving
communication e.g. SBAR(Pierantozzi, 2013)

© Endeavour College of Natural Health www.endeavour.edu.au 19
Professional Communication
(Pierantozzi, 2013)

© Endeavour College of Natural Health www.endeavour.edu.au 20
Professional Communication
From Primum Non Nocere: “As one GP registrar
describes:
When a client presents with a list of tests
requested by the naturopath without any
explanation as to why they are even needed,
this just leaves a sour taste in my mouth. If I
have to converse with another treating physician
the least I do is write a letter of referral. It’s an
integral component in the continuity of the
client's care.”(Pierantozzi, 2013)

© Endeavour College of Natural Health www.endeavour.edu.au 21
Referral
o Referral should be made when client’s needs
cannot be met by practitioner
o Should be done in consultation with client
o Should not be done to avoid “difficult and
unenjoyable work”
o Useful in case of people with special needs,
e.g. cultural and language differences
(Geldard, 2009)

© Endeavour College of Natural Health www.endeavour.edu.au 22
Referral
Referral Letter
o Use SBAR or similar convention
o A summary of the key medical facts will save
time and assists the other practitioner in
clinical decision making.
o Outline important points of reference e.g.
• Jenny Smith (PCOS diagnosed 2011, Metformin
500mg TDS)
(Pierantozzi, 2013, Arthur, 2014)

© Endeavour College of Natural Health www.endeavour.edu.au 23
Referral
o Use medical language and conventions
• Avoid ‘naturopathic language’ e.g. adrenal
fatigue, leaky gut, immune modulating
• Include all units of measurement
• Use tables to summarise medical history if
extensive
o Report accurately
• e.g. client reports or suspects gluten intolerance
• Use quotation marks when reporting the client's own
words.
(Arthur, 2014)

© Endeavour College of Natural Health www.endeavour.edu.au 24
Referral
o Be reasonable with your requests
• Choose the tests that are indicated. A request for
tests is not a ‘wish list’.
• Know which tests you can request e.g. T3, T4 and
RT3 can’t be subsidised without a prior diagnosis
of thyroid disease or TSH outside of reference
range.
o Provide a rationale
• Present a clear justification for any requests
– e.g. Iron studies (vegetarian diet)
• Include references where appropriate
(Arthur, 2014)
© Endeavour College of Natural Health www.endeavour.edu.au 25
Best Practice
o If a client is referred to you by another
practitioner, medical or complementary it is
standard practice to follow up with the
referring practitioner.
• If the client isn’t going back to the referring
practitioner, you may just send an email to thank
them.
• If you will be working with the referring practitioner
you would send a more comprehensive report
back about the client you have in common.

© Endeavour College of Natural Health www.endeavour.edu.au 26
Best Practice
o If the client is part of an integrative team of
practitioners including the referring
practitioner e.g. acupuncture,
musculoskeletal therapist and naturopath
you may provide your client with a report to
share or communicate with all parties.
o While you may not receive the same
courtesy in return, best practice should be
adopted when working with both medical and
complementary practitioners.

© Endeavour College of Natural Health www.endeavour.edu.au 27
CommunicationActivity:
o Review the Template referral Letter. (Lecturers
are to access this via the Clinic Hub on the
LMS under the Nutrition or Naturopathy Green
Tab and project it on to the board for this
exercise).
o View and discuss Referral Letter Example 1
and 2 from your weekly readings.
o For more about interprofessional
communication read: Primum Non Nocere
from your weekly readings.

© Endeavour College of Natural Health www.endeavour.edu.au 28
Building patient/practitioner rapport

© Endeavour College of Natural Health www.endeavour.edu.au 29
Conflicting Views
o Responsibility for good interaction tends to be seen by
clients as the responsibility of the practitioner.
o Conventional medical contact can be seen as:
• Getting information out of clients
• Imparting information to clients
• <5% of doctor’s comments is friendly or sociable
• 25% of medical consultations, the chief concerns had
not been elicited. (Persaud, 2005)
o Take care that you don’t just see your client as a
source of information.

© Endeavour College of Natural Health www.endeavour.edu.au 30
Rapport Building and Relationship
Maintenanceo Rapport building is an integral part of
developing an ongoing practitioner/patient
relationship.
o A strong relationship is essential for effective
clinical encounters.
o A warm greeting, eye contact, a brief
personal/non-medical interaction, checking in
on family or an important life event can take
less than 5 minutes but builds client trust and
connection.(Mauksch, 2008)

© Endeavour College of Natural Health www.endeavour.edu.au 31
Rapport Building
o Caution, if you haven’t established
connection with your client, there may be
insufficient trust to engage in small talk.
o Don’t engage in too much small talk as it
may railroad the reason for the consultation.
o As the relationship develops, ‘check-in’ with
your clients to re-establish the relationship.
(Mauksch, 2008)

© Endeavour College of Natural Health www.endeavour.edu.au 32
Acknowledging
o Clients often give clues to indicate thoughts
or feelings relating to their illness or
behaviour.
o Acknowledge these in an empathic way – it
may allow the client to reveal beliefs about
illness, preferences about treatment/care or
underlying drivers of illness.
o Empathy (not sympathy) can help focus a
discussion and/or invite further exploration of
issues. (Mauksch, 2008)

© Endeavour College of Natural Health www.endeavour.edu.au 33
Non-verbal communication
o Pick up non-verbal cues from your clients.
• Are they distressed?
• What is their mood like and how do their demeanor
and body language change during the
consultation?
o This may give clues to difficulties they may have
that they cannot express verbally.
o If people become uncomfortable during a line of
questioning, their body language may become
“closed”; they may cross their arms and legs and
fail to keep eye contact.

© Endeavour College of Natural Health www.endeavour.edu.au 34
Habits to Avoid
1. Dismissing the subject matter as uninteresting
• it may vitally be interesting to the client
2. Feigning attention
• give your full attention. clients pick up when you are ‘faking it’
3. Avoiding difficult material
• this is often the heart of the matter for the client
4. Allowing distractions
• be present with the client. Phones, emails etc. can be addressed at a later date.

© Endeavour College of Natural Health www.endeavour.edu.au 35
Habits to Avoid
5. Finding fault with the speaker
• Be compassionate in your dealings with clients
6. Becoming overstimulated by something the speaker says
• Withhold evaluation until comprehension is complete - hear the speaker out
7. Wasting the advantage of thought-speech speed
• Speaking 100 words per min (WPM), thought 500 wpm. Don’t use the difference to float off on tangents or plan your meal for dinner. Use it to really listen to everything the client is saying and not saying, between the lines etc.

© Endeavour College of Natural Health www.endeavour.edu.au 36
Habits to Avoid
8. Allowing emotion-laden words to arouse personal antagonism
• Compassion and non-judgment are key to building therapeutic relationships.
9. Listening only for details or facts
• The story come from the whole person, not just the facts
10.Using medical jargon as this widens the gap for the clients understanding of illness

© Endeavour College of Natural Health www.endeavour.edu.au 37
Asking the right questions

© Endeavour College of Natural Health www.endeavour.edu.au 38
Professional Questioning Skills
o During the process of developing a trusting,
collaborative relationship with your client you
start to become more confident in the skilled
use of professional and sensitive questions.
o As with attending, following and reflecting,
good use of questioning can encourage
clients to communicate their needs better.

© Endeavour College of Natural Health www.endeavour.edu.au 39
Professional Questioning Skills
Skilled use of questions:
1. Provide a framework to guide/direct the session
2. Allow the session to flow well and move along to the
benefit of both the client and the practitioner – keep it
on track
3. Open up new areas for discussion
4. Assist in focussing and clarifying client concerns
5. Support client self-exploration, bringing out additional
specifics
6. Helps the practitioner more fully understand the
issues at hand
(Ivey & Ivey, 2007)

© Endeavour College of Natural Health www.endeavour.edu.au 40
Initial Question
o Initial Question(s):
• If possible you want the client to describe their
presenting problem(s) in their own words.
• Encourage them to be as descriptive as possible.
• Open ended questions are a good way to allow the
client the time and space to ‘present’ their
problems.
o Examples include:
• "What brings your here? How can I help you? What
seems to be the problem?“
(Goldberg, A Practical Guide to Clinical Medicine)

© Endeavour College of Natural Health www.endeavour.edu.au 41
Open & Closed Questions
o Closed questions – can be answered in a
single word or a short phrase e.g.
• Do you experience anxiety?
• Do you go to the toilet daily?
What are the advantages and disadvantages of
closed questions?
© Endeavour College of Natural Health www.endeavour.edu.au 42
Open & Closed Questions
o Open questions – are likely to receive
extended, more detailed answers.
o They start with what, why, how, describe.
• How have you been after your operation?
• What do you think is keeping you awake at night?
What are the advantages of open questions?

© Endeavour College of Natural Health www.endeavour.edu.au 43
Open & Closed Questions
o Open questions disadvantages:
• Individual clients give varying degrees of detail
• Responses may lack relevance or be buried in
useless detail
• Questions may be too general or allow clients to go
off track too easily
• Extended answers can take time.

© Endeavour College of Natural Health www.endeavour.edu.au 44
Follow up questions
o There is no ideal way to question clients
however there are ways of encouraging client
responses/openness.
Read page 32 Verbal Responses – Assisting the
Narrative, and page 33 Examiner’s Verbal
Responses of the Reading- Verbal Responses
from Physical Examination & Health
Assessment, 7th ed, Jarvis.

© Endeavour College of Natural Health www.endeavour.edu.au 45
Sensitive & Proactive Questioning
Skillso Questions have a down side as well and can
easily be abused in the interview process.
o Some issues include:
• Bombarding/ grilling/ interrogating the client – too
many questions at once
• Multiple questions – does not allow to fully express
themselves or finish each question appropriately
• Questions as statements e.g. ‘Don’t you think that
doing more exercise would be good for you?’

© Endeavour College of Natural Health www.endeavour.edu.au 46
Sensitive & Proactive Questioning
Skillso Why questions can be used inappropriately
e.g. ‘Why did you eat that if you knew it was
not good for you?’
o Using questions to overly control the session
and the content – can be used intrusively and
for the practitioner’s gain or curiosity rather
than furthering the interview.
(Ivey & Ivey, 2007)

© Endeavour College of Natural Health www.endeavour.edu.au 47
The Art of Questioning
Clarification:
• Check back with the client to ensure
understanding or to check a specific detail
• If client says something that was unfamiliar
to you – CLARIFY
• e.g. the client names a condition that you
are not familiar with

© Endeavour College of Natural Health www.endeavour.edu.au 48
The Art of Questioning
Encouragement for client to talk openly:
o You may have asked a personal question
which is of a sensitive nature to the client –
the client starts to answer, but stops talking:
o Encourage by letting them know they can
continue or asking about the specific issue
e.g. “You mentioned that the problem started
due to a ‘bad lifestyle” in your early 20’s, can
you tell me more about that”

© Endeavour College of Natural Health www.endeavour.edu.au 49
The Art of Questioning
Digressing/Avoiding Answer:
o The client does not seem to answer your question directly. May be a sign that they are concealing something or are embarrassed to answer.
• E.g. How many alcoholic drinks do you have on a weekly basis?
• Ans: Oh, I’m not quite sure – maybe 2 or 4
o Invite the client to answer in more detail if it is pertinent to the presenting complaint

© Endeavour College of Natural Health www.endeavour.edu.au 50
The Art of Questioning
o Going in circles:
o Client seems to being repeating the same
thing over and over.
o Summarise what the client has repeatedly
said and move on to the next question.

© Endeavour College of Natural Health www.endeavour.edu.au 51
The Art of Questioning
o Check your understanding:
• The client has mentioned something that their
doctor has told them about a side effect of their
medication. You did not quite understand:
• So, the medication you are taking at present may
be contributing to how you are feeling?
o Check Client understanding:
• Throughout the consultation, ask the client if there
is anything they wish to ask YOU!!

© Endeavour College of Natural Health www.endeavour.edu.au 52
Questioning and Diversity
o Western style questioning can be experienced
as intrusive or rude for people from other
cultures.
o For example, people from Aboriginal
communities and from other, usually
collective, communities can sometimes
experience a breach of trust by insensitively
and unskilled questioning.
(Ivey & Ivey, 2007)

© Endeavour College of Natural Health www.endeavour.edu.au 53
Questioning and Diversity
o Sometimes people from a range of diverse
backgrounds such as gay, lesbian or
transgender may already feel ‘under the
societal microscope’ and may experience
unskilled use of questions as invasive or more
about the practitioner than about them
(Ivey & Ivey, 2007)

© Endeavour College of Natural Health www.endeavour.edu.au 54
Questioning and Diversity
o In summary, be sensitive always to the
individual you have in front of you at any point
and be aware that each person will respond
differently to questioning.
(Ivey & Ivey, 2007)

© Endeavour College of Natural Health www.endeavour.edu.au 55
Asking the Right Questions
Unfamiliar phrases
The client has used an unfamiliar phase.
"Could you explain what you think the doctor
meant by saying 'there's been hiccup' with your
condition?"
Encourage without bias
The client is getting into sensitive areas and
has stopped talking. You want to encourage
without bias or prejudice
"You say things started to fall apart when you
started drinking heavily".
Digressing
The client is digressing and is not answering
your question directly.
"Perhaps I'm mistaken, but weren't you going to
tell me about what you did the last time you felt
this type of discomfort?”
Going in circles
The client has been going in circles, saying
the same things over and over. You want to
move on.
“Let me summarise what I understood you to say.
You said…Now was there anything else effecting
your problem”
Clarification
The client has just said something that does
not seem to agree with a statement made
earlier. You want to clarify
"I thought you said earlier that ... Now I hear you
saying …Would you mind going over that for me
please so that I get it right in my mind".
© Endeavour College of Natural Health www.endeavour.edu.au 56
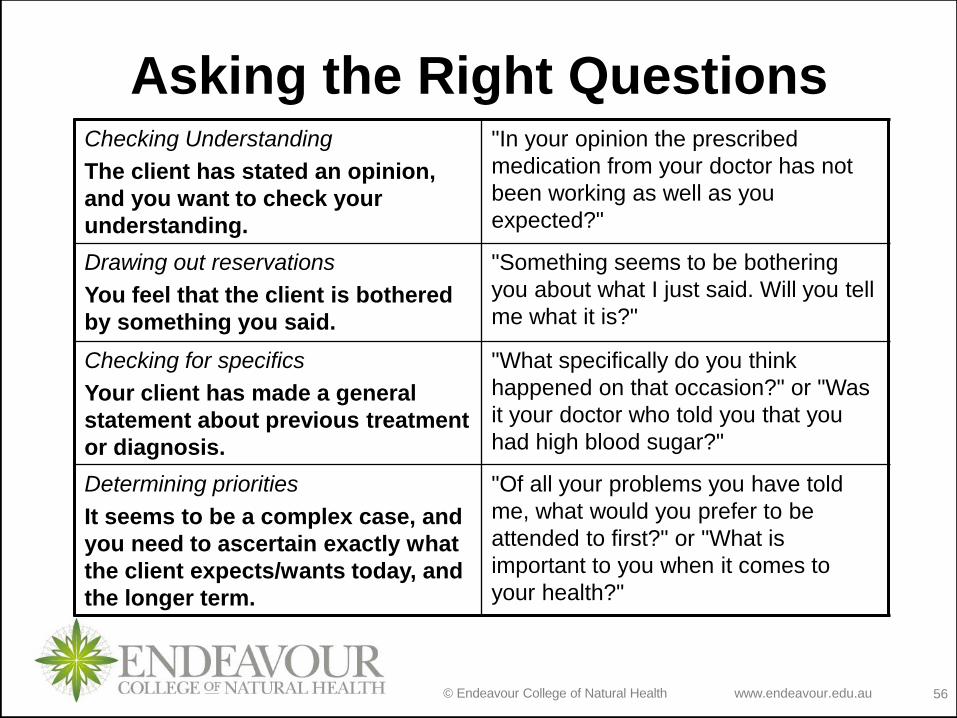
Asking the Right QuestionsChecking Understanding
The client has stated an opinion,
and you want to check your
understanding.
"In your opinion the prescribed
medication from your doctor has not
been working as well as you
expected?"
Drawing out reservations
You feel that the client is bothered
by something you said.
"Something seems to be bothering
you about what I just said. Will you tell
me what it is?"
Checking for specifics
Your client has made a general
statement about previous treatment
or diagnosis.
"What specifically do you think
happened on that occasion?" or "Was
it your doctor who told you that you
had high blood sugar?"
Determining priorities
It seems to be a complex case, and
you need to ascertain exactly what
the client expects/wants today, and
the longer term.
"Of all your problems you have told
me, what would you prefer to be
attended to first?" or "What is
important to you when it comes to
your health?"
© Endeavour College of Natural Health www.endeavour.edu.au 57
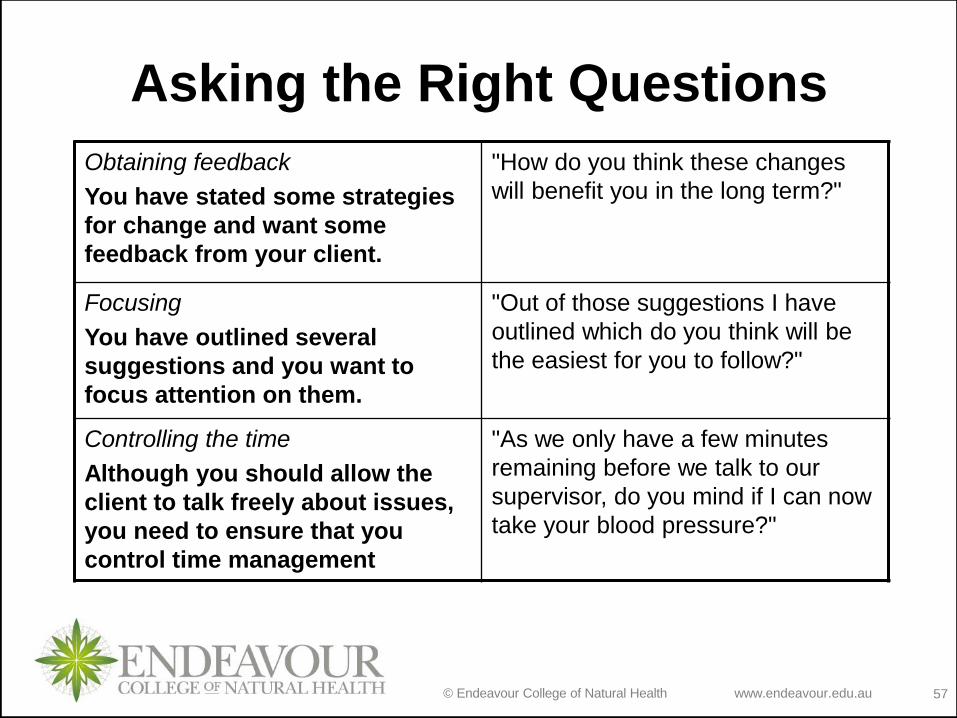
Asking the Right Questions
Obtaining feedback
You have stated some strategies
for change and want some
feedback from your client.
"How do you think these changes
will benefit you in the long term?"
Focusing
You have outlined several
suggestions and you want to
focus attention on them.
"Out of those suggestions I have
outlined which do you think will be
the easiest for you to follow?"
Controlling the time
Although you should allow the
client to talk freely about issues,
you need to ensure that you
control time management
"As we only have a few minutes
remaining before we talk to our
supervisor, do you mind if I can now
take your blood pressure?"

© Endeavour College of Natural Health www.endeavour.edu.au 58
Avoiding the Wrong QuestionsAvoid asking yes/no questions
Not "Is your arthritis very painful?"
But "Tell me about your arthritis …"
Avoid asking multiple choice questions
Not "Is the pain dull, throbbing, or …?"
But "Describe the pain."
Avoid putting your words into the client's
mouth
Not "Do you eat oily fish 2 or 3 times a
week?"
But "Tell me about your diet."… "Any
fish?" … "What type?" … "How often?"
Avoid making presumptions
Not "That must have been very distressing
for you."
But "How did your feel about that?"
Avoid being apologetic, but remain sensitive
Not "Would you mind terribly if I asked you
about your libido?"
But "Libido can be a good measure of
health. How has your libido been recently?"
Avoid being overly empathetic
Not "Oh, I had that! I know exactly what
you are going through"
But "I can only guess what you are going
through. Tell me all about it."

© Endeavour College of Natural Health www.endeavour.edu.au 59
Helpful TechniquesUse continuation phrases "And then …?" or "What happened next?"
or even just an empathetic murmur or an
encouraging nod of the head may be
enough for the client to continue.
Reflect what has just been said,
summarizing.
"So, after your daughter left home, and
you broke your hip, your husband starting
drinking heavily …"
Try to get the client's own idea of the cause
of the dis-ease
Why do you suppose you get so angry at
those times?"
or "Do have any idea why you have
psoriasis?"
Explore feelings (if appropriate - remember
you are not a trained counsellor)
"When you finally got the diagnosis, how
did you feel?"
Final check before moving on. "Is there anything more you can tell me
about your kidney condition?"
Move on, eliciting more symptoms or
concerns.
"Anything else?"
© Endeavour College of Natural Health www.endeavour.edu.au 60
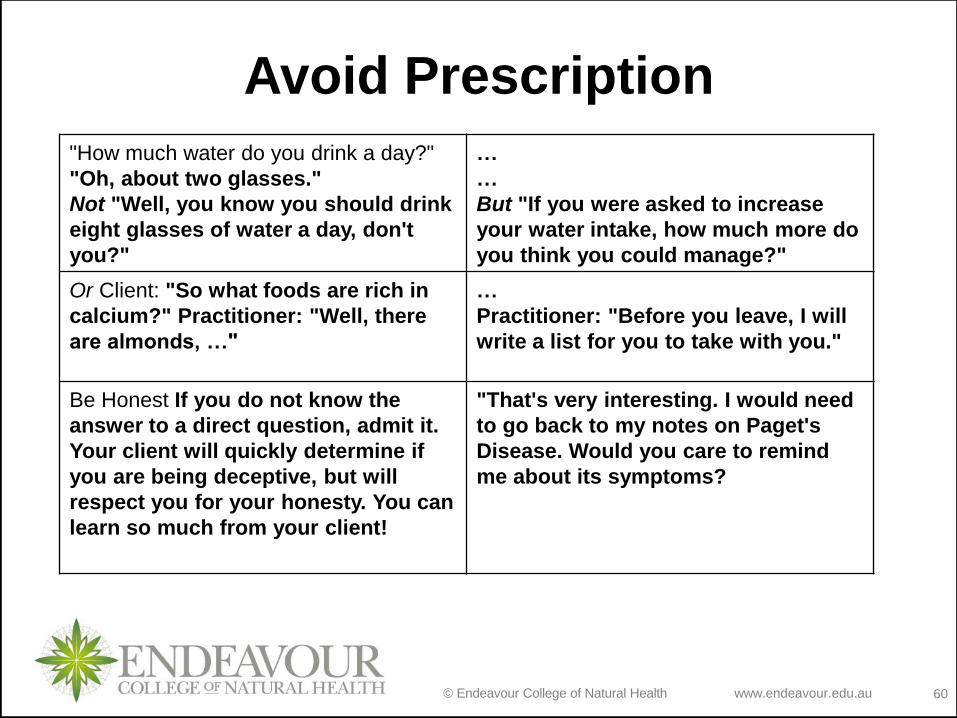
Avoid Prescription
"How much water do you drink a day?"
"Oh, about two glasses."
Not "Well, you know you should drink
eight glasses of water a day, don't
you?"
…
…
But "If you were asked to increase
your water intake, how much more do
you think you could manage?"
Or Client: "So what foods are rich in
calcium?" Practitioner: "Well, there
are almonds, …"
…
Practitioner: "Before you leave, I will
write a list for you to take with you."
Be Honest If you do not know the
answer to a direct question, admit it.
Your client will quickly determine if
you are being deceptive, but will
respect you for your honesty. You can
learn so much from your client!
"That's very interesting. I would need
to go back to my notes on Paget's
Disease. Would you care to remind
me about its symptoms?
© Endeavour College of Natural Health www.endeavour.edu.au 61
Traps of Interviewing
Read page 35 of Physical Examination & Health
Assessment, 6th ed:
Ten Traps of Interviewing
In pairs, discuss if there are any of the 10 ‘traps’
you identify with and ways you can overcome
these traps.

© Endeavour College of Natural Health www.endeavour.edu.au 62
Prioritising information
© Endeavour College of Natural Health www.endeavour.edu.au 63
o Document the most important presenting complaint or
acute problem first!
o Recognising symptoms/responses that demand an
urgent assessment as compared to those that are of
lower priority will come with time and experience.
o Give all client complaints careful consideration as they
may be markers of something more serious or
underlying.
o Some, however, will become "a something" (a
recognizable clinical entity) or "a nothing".
(Goldberg, A Practical Guide to Clinical Medicine)
Prioritising

© Endeavour College of Natural Health www.endeavour.edu.au 64
Prioritising
o When determining the first problem, consider:
• Acuity – is the condition short or long standing?
Does it need immediate consideration?
• Severity – does the condition have serious health
implications or is it life threatening?
• Reason for consult/referral – an assessment,
treatment plan, to talk over possible treatment
options, practitioner or ideas shopping
• Scope of practice – are you qualified or
experienced enough to treat the client's condition,
do you feel confident to do so?

© Endeavour College of Natural Health www.endeavour.edu.au 65
Prioritising
o When determining the first problem, consider:
• New/previously unidentified problems – has a
potentially serious problem emerged during
questioning or between consults?
• Worsening of previously identified problem
• Ability to resolve the problem (vitality) – is the client
vital enough to heal/recover from a problem, will a
problem need ongoing management, medical or
otherwise
• Remainder of problems addressed in descending
order

© Endeavour College of Natural Health www.endeavour.edu.au 66
Case Study
o Read HMCL211_SN11_Case Study and
answer the following questions:
o How would you prioritise John’s issues?
• Go through the priority considerations with each of
John’s presenting complaints and any elicited
complaints.
• Would you refer John for further assessment or
care? If so, in pairs write a letter of referral to the
practitioner of choice outlining why you have
referred him. Include all pertinent case details. Use
the Template Referral Letter from the Hub.

© Endeavour College of Natural Health www.endeavour.edu.au 67
References
o Goldberg C, A Practical Guide to Clinical Medicine,
<http://meded.ucsd.edu/clinicalmed/history.htm>, viewed 26th November
2014
o Holle, L, Salvo, M, 2014, SOAP Note Lecture, archive.saber.wijiti.net,
viewed 26th November 2014
o Ivey A.E & Ivey M.B, 2007, Intentional Interviewing and Counselling,
Thomson Brooks/ Cole: California
o Jarvis, C 2012, Physical examination & health assessment, 6th edn,
Elsevier Saunders, St Louis, MO.

© Endeavour College of Natural Health www.endeavour.edu.au 68
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and communicated to you by or on
behalf of the Australian College of Natural Medicine Pty Ltd (ACNM)
trading as Endeavour College of Natural Health, FIAFitnation, College
of Natural Beauty, Wellnation - Pursuant Part VB of the Copyright Act
1968 (the Act).
The material in this communication may be subject to copyright under
the Act. Any further reproduction or communication of this material by
you may be the subject of copyright protection under the Act.
Do not remove this notice.





























