Embed Size (px)
Citation preview

Setting up the NOAC Service & Taking it to Primary Care
Satinder Bhandal
Consultant Anticoagulation Pharmacist
November 2015
Buckinghamshire Health Care NHS Trust

Quiz 1. What is the most serious side effect of NOACs?
a) GI b) rashes c)bleeding d) renal failure
2. What is the half life of the NOACs in normal renal function?
a) 12h b) 24h c) 36h d) 48h
3. What percentage of patients stop NOACs at 2years due to side effects?
a) 5% b) 10% c) 20% d) 50%
4. The dose of rivaroxaban must be appropriate for which of the following:
a) RF b) Weight c) Gender d) Age

The Statistics Annual data
• Estimate 16,100 strokes are averted including 4,400 fatal strokes by current warfarin treatment
• 54% of people requiring anticoagulation receive it
• 8.74% of people requiring anticoagulation have declined it or it is recorded it is contra-indicated
• Another 46% need anticoagulation
Cost & Benefits of Antithrombotic Therapy in England: An Economic Analysis based on GRASF-AF (NHS Improving Quality Report – November 2014)

AF and NICE
• Dabigatran and rivaroxaban approved 2012
• Apixaban approved 2013
• Need to implement NICE guidance
• Need to ensure patients benefit from these new drugs
• Ensure safe prescribing
• Need to reduce avoidable strokes
• Manage the entry of these new drugs

Challenges
• Politics
• Lack of experience with NOACs
– On job learning
• Lack of clarity on place of NOACs
• Demanding / mis-informed patients
• Securing funding


Commissioning a Specialist Anticoagulant Decision Unit
• Convened a meeting of all the key stakeholders
• Agreed criteria for NOAC use
• Agreed who could initiate NOACs
• Agreed to commission a specialist NOAC service
• Agreed referral pathways
• Agreed responsibilities of GPs and specialist clinic

GP diagnoses patient
with AF and refers to
NOAC service
NOAC clinic decides on anticoagulation option with
patient in line with Bucks criteria
•Start warfarin
•Prescribe
•Counsel patient
•Alert Card
•Information Pack
•Start NOAC,
•Prescribe
•Counsel patient,
•Anticoagulant Alert Card
•Information pack
If warfarin and NOAC
unsuitable, consider referral to
cardiologist
Refer into usual A/C clinic •Second contact by phone at 2 weeks: Address issues/concerns/compliance Discharge to GP for continuation
•If switching NOAC, repeat above stages •If switched to warfarin, refer to A/C clinic
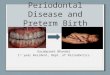
New AF patient from primary care

Patient with AF identified requiring A/C
Non- urgent -
refer to NOAC clinic CHA2DS2VASC>/= 6 but no TIA or
stroke: refer to NOAC clinic for urgent
initiation 72hours
NOAC clinic agrees anticoagulation with patient in line with Bucks criteria
•Start warfarin
•Prescribe
•Counsel patient
•Anticoagulation Alert Card
•Information pack
•Start/continue NOAC
•Prescribe
•Counsel patient
•Anticoagulant Alert Card
•Information Pack
If warfarin and NOAC
unsuitable, consider
referral to Cardiologist
Recent TIA or stroke
• Stroke Team starts A/C
•Refers to NOAC Clinic clinic
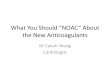
Hospital Referral Pathway

Patient on Warfarin but needs review
as may require NOAC
Stops warfarin & considers referral to
cardiologist
•Start NOAC,
•Prescribe
•Counsel patient,
•Anticoagulant Alert Card •Information pack
Continues warfarin with further
counselling and discharges to
usual warfarin monitoring clinic
NOAC Clinic reviews
patient
•Second contact by phone at 2
weeks:
Address
issues/concerns/complian
ce
Discharge to GP for
continuation
•If switching NOAC, repeat
above stages
•If switched to warfarin, refer to
A/C clinic
Patient referred by GP or BHT clinicians as
poor control on warfarin

The Consultation • 30 minute structured consultation
• Involve patient / relative / carer
• Carry out risk/benefit assessment
• Educate on stroke risks & need for anticoag
• Shared decision making
a)Start anticoag b) Choice of anticoagulant
• Prescribe and counsel
• Follow up arrangements
• Helpline

Agree the right drug for the patient
• Stroke risk
• Bleeding risk
• Extreme age
• Extreme weight
• Co-morbidities
• Renal function
• Liver function
• Risk of ICH
• TTR
• Risk of side effects
• Need for MDS
• Lack of licensed antidotes for NOACs
• Mitral stenosis or mechanical heart valve
• Adherence with complex regimens
• Compliance issues

Locally Agreed Criteria for NOAC Use
NEW PATIENTS
• High risk of interactions with warfarin leading to unacceptable INR fluctuations which cannot be addressed.
• Co-morbidities which make INR control challenging e.g. unstable severe COPD or recurrent cellulitis
• Regular INR monitoring is difficult or impractical after exploring all possible alternatives eg. immobile patients requiring home visits from phlebotomy
• Adherence to variable and complex warfarin dosage regimens is likely to be poor
• Secondary prevention of Af patients with recent stroke or TIA. To be referred by secondary care stroke service

Locally Agreed Criteria for NOAC Use (2)
EXISTING WARFARIN PATIENTS
• Poor INR control (TTR < 65%) despite evidence of compliance
• Allergy to or intolerable side effects from warfarin which would require warfarin withdrawal

Counselling
Patient explanation Condition / Purpose of medicine /Duration
If NOAC, lack of antidote
How to take in relation to food & regimen
Monitored dosage aids – warfarin and dabigatran not in dosette
Compliance
Action if missed dose
Alert Card
Informing healthcare professionals (surgery /dental/injections/pregnancy/meds)
Interactions – pain relief /OTC medicines
Side-effects/ Warning signs/ Emergency
Alcohol /Diet
Follow up arrangements


Telephone Follow up
Questions for Patient or Carer
Have you had a chance to start taking your medicine yet?
How are you getting on with it?
Are you having any problems with you new medicine or concerns?
Do you understand why you need anticoagulation?
Do you think you are getting any side-effects or unexpected effects?
Have you missed any doses or changed when you take it?
Do you have anything else you would like to know or
anything you would like me to go over again?

Identifying the Opportunities
• High cost medicines
• Medicines with complex prescribing regimens
• Narrow therapeutic medicines
• Medicines requiring shared decision making and intensive adherence support
• Combination prescribing for new patients, naïve to medicines

Develop new skills
• Independent prescribing
• Have expertise in area in which you wish to set up new service
• Network with local leaders in the specialism

Find a Champion
• Engage Chief Pharmacist and CCGs Pharmacists
• Meet informally with key stakeholders
• Get buy in from them
• Get them to advocate for you
• You should have agreement with them for what you want to achieve before the formal decision making meeting

Business Case
• Find out locally accepted format
• Use the same headings
• Account for administration time
• Ask finance to help
• Be realistic about timescales for implementation including writing and approval of shared care guidelines, care pathways, referral forms, service specification

Audit
• Agree what data your commissioners will require
• Agree timing and frequency
• Decide other audits you need to conduct for the development of your service
• Research?

Celebrate Your Success
• Talk about your work
• Write up audit results
• Publish
• Acknowledge others input
• Maintain relationships with stakeholders
• Continue to deliver a good service

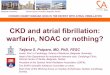
NOAC Service Audit
If a friend or relative needed similar treatment, would you be happy to recommend the standard of care in the clinic?
0
10
20
30
40
50
60
70
Extremely likely Likely Neither likely orunlikely
Unlikely Extremely unlikely Don't know
If a friend or relative needed similar treatment, would you be happy to recommend the standard of care in the clinic?

Did you have confidence and trust in the pharmacist?
0
10
20
30
40
50
60
70
80
90
Yes definitely Yes, to some extent No, not really
Did you have confidence and trust in the pharmacist?

Were you involved as much as you wanted to be in decisions about your treatment?
0
10
20
30
40
50
60
70
80
90
Yes definitely Yes, to some extent No, not really
Were you involved as much as you wanted to be in decisions about your treatment?

Did a member of staff explain the purpose of the medicines you were to take at home in a way you could
understand?
0
10
20
30
40
50
60
70
80
90
Yes , completely Yes to some extent No I did not need anexplanation
I had no medicines
Did a member of staff explain the purpose of the medicines you were to take at home in a way you couldunderstand?

Did a member of staff tell you about medication side effects to watch for when you went home?
0
10
20
30
40
50
60
70
80
Yes , completely Yes to some extent No I did not need anexplanation
Did a member of staff tell you about medication side effects to watch for when you went home?

Moving the Services to Primary Care
Making the most opportunities
• Having the right skills, knowledge and expertise
• Having capacity to expand
• Act quickly
• Make full use of your team, stakeholders & Chief Pharmacist
•

Moving the NOAC Service into GP Practices (1)
• HCA practice based anticoag clinic pulled
• Very elderly patients anticoagulated at the practice
• Difficult for them to access acute provider clinics
• Urgent replacement service required and CCG approached NOAC service
• NOAC service stepped in with a GP practice based weekly clinic

Moving the NOAC Service to GP Practices (2)
• Any Qualified Provider for anticoagulation clinics
• Competition from other providers – Boots, GP practices, other acute trusts
• BHT has taken on some GP practices
• Out reach clinics set up in GP practices for warfarin dosing and local NOAC service for patients

Moving the NOAC Service to GP Practices (3)
• Poorly controlled patients on warfarin
• GPs auditing there own anticoagulant clinic patients to ensure they are well controlled and referring patients to be considered for a NOAC are an opportunity
• Large batch of referrals from a practice presents an opportunity
• Running a clinic in first such practice to review patients for a NOAC within the practice

Summary
• How the NOAC service was established
• Care pathways in Bucks
• Consultation
• Identifying & being ready to benefit from opportunities
• Business Cases
• Developing your service into primary care