Embed Size (px)
Citation preview

http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information: Published online http://www.cconline.org© 2008 American Association of Critical-Care Nurses
2008;28:98-123Crit Care Nurse ArbourCarol A. Rauen, Marianne Chulay, Elizabeth Bridges, Kathleen M. Vollman and RichardPastureSeven Evidence-Based Practice Habits: Putting Some Sacred Cows Out to
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.shtmlInformation for authors
http://www.editorialmanager.com/ccnSubmit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.shtmlEmail alerts
by AACN. All rights reserved. © 2008 ext. 532. Fax: (949) 362-2049. Copyright101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050,Association of Critical-Care Nurses, published bi-monthly by The InnoVision Group Critical Care Nurse is the official peer-reviewed clinical journal of the American
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

98 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
if validated, reliable, and usefulevidence leads to such change. Nursesare at the forefront of evidence-basedapproaches.2
The Institute of Medicine definesevidence-based practice (EBP) as“the integration of best research,clinical expertise, and patient val-ues in making decisions about thecare of individualized patients.”3
Research findings are a collection offacts. They become evidence whenthe findings are relevant and usefulin particular clinical circumstances.4
Using research to guide clinicaldecision making is a shift in culturefrom basing decisions on opinion,past experiences, and precedents tobasing decisions on science, research,and evidence.5 The Agency for Health-care Research and Quality publishedMaking Health Care Safer: A CriticalAnalysis of Patient Safety Practices.6
This document outlines 79 evidence-based practices and targets relatedto patient safety. The 11 recommen-dations with the strongest researchsupport have a direct connection tocritical care practice (Table 1).
Carol A. Rauen, RN, MS, CCNS, CCRN, PCCNMarianne Chulay, RN, PhDElizabeth Bridges, RN, PhD, CCNSKathleen M. Vollman, RN, MSN, CCNSRichard Arbour, RN, MSN, CCRN, CNRN
Seven Evidence-Based Practice Habits: Putting SomeSacred Cows Out to Pasture
Evidence-Based Practice
Nursing has deeplyrooted traditions.As far back as Flo-rence Nightingale inthe 19th century,
nurses prided themselves on patientadvocacy, infection control (beforegerm theory), and physical care ofthe entire body, not limiting thefocus to management of disease orsigns and symptoms.1 These earlyroots established the philosophy ofnursing. Nurses labeled what theydo as caring or the art of nursing.
Critical care nurses find them-selves in a unique situation. We haveour feet deeply rooted in the art ofnursing. Yet our hands and mindsreach for the scientific basis that ourhighly technical, physiological, andpharmacological specialty requires.To base our practice on science, wemust use research to answer ques-tions, establish protocols, and pro-mote critical thinking and decisionmaking at the bedside. Doing sorequires us to be willing and able tochange practices, regardless of thetradition and commonly held beliefs,
PRIME POINTS
• About 30% to 40% ofpatients do not receivecare consistent with cur-rent scientific evidence.
• Are we doing what isbest for our patientswith the current evi-dence available to us?
• Do not instill normalsaline (physiologicalsalt solution) beforeendotracheal suctioning.
• Use chest radiogra-phy to confirm correctplacement of nasogas-tric tubes.
• Attention to correctplacement of electrocar-diography leads isimperative.
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

In this article, we cover 7 evidence-based practice (EBP) recommenda-tions that clinicians should considerimplementing into their practice.Much of this research is not newand has met with resistance at thebedside despite clear evidence that itrepresents best practice. We alsoaddress the traditional approach
and offer recommendations forimplementing the changes. MarianneChulay addresses instillation of nor-mal saline (physiological salt solu-tion) with endotracheal suctioningand verification of nasogastric tubeplacement. Elizabeth Bridges reviewsthe current evidence and recom-mendations for accurate measure-
ment of blood pressure and selec-tion of electrocardiography leads.Kathleen Vollman delineates theresearch and recommendations forpatients’ positioning and mobility.Richard Arbour discusses use of theGlasgow Coma Scale in neurologi-cal assessment and management ofintracranial hypertension.
Instillation of Normal SalineBefore Endotracheal Suction-ing: Helpful or Harmful?
Most hospital policies and pro-cedures for management of artificialairways include instilling 5 to 10 mLof normal saline before endotrachealsuctioning is done.7 This nursingand respiratory therapy routine wasadvocated as a way to improve oxy-genation and removal of secretionsby thinning thick secretions andstimulating coughing to assist withmobilization of secretions. Althoughinstillation of normal saline is along-practiced suctioning interven-tion, no research has ever docu-mented the benefit of this practice,and some researchers have foundthe practice potentially harmful.
Effect on OxygenationIn most experimental studies8-13
on the effect of instillation of normalsaline before endotracheal suction-ing, oxygen saturation or PaO2 wasevaluated as the primary end point;in only a single study14 was mixedvenous oxygenation evaluated. Inthese studies, oxygen saturationwas significantly lower with instilla-tion of saline than with no instilla-tion of saline,8-10 or the results of the2 methods (saline vs no saline) didnot differ.11,12 In no studies to datedid instillation of normal salinebefore suctioning improve oxygen
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 99
Carol A. Rauen is an independent critical care clinical nurse specialist in Silver Spring,Maryland.
Marianne Chulay is a consultant in clinical research and critical care nursing in Gaines -ville, Florida.
Elizabeth Bridges is an assistant professor at the University of Washington School of Nurs-ing in Seattle and a clinical nurse researcher at the University of Washington MedicalCenter in Seattle.
Kathleen M. Vollman is a clinical nurse specialist, educator, and consultant at AdvancingNursing LLC in Northville, Michigan.
Richard Arbour is a critical care clinical nurse specialist at Albert Einstein Medical Centerin Philadelphia, Pennsylvania.
Corresponding author: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, 14800 Fireside Dr., Silver Spring, MD 20905(e-mail: [email protected]).
To purchase reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
Authors
Table 1 Practices related to patients’ safety strongly supported by evidencea
Appropriate use of prophylaxis to prevent venous thromboembolism in patients at risk
Use of perioperative β-blockers in appropriate patients to prevent perioperative morbidity and mortality
Use of maximum sterile barriers while placing central intravenous catheters to preventinfections
Appropriate use of antibiotic prophylaxis in surgical patients to prevent postoperativeinfections
Asking that patients recall and restate what they have been told during the informedconsent process
Continuous aspiration of subglottic secretions to prevent ventilator-associated pneumonia
Use of pressure-relieving bedding materials to prevent pressure ulcers
Use of real-time ultrasound guidance during insertion of central catheters to prevent complications
Patient self-management of warfarin to achieve appropriate outpatient anticoagulationand prevent complications
Appropriate provision of nutrition, with a particular emphasis on early enteral nutritionin critically ill and surgical patients
Use of antibiotic-impregnated central venous catheters to prevent catheter-related infections
a Based on information from Shojania et al.6
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

the results. In the one, small study16
(N = 12) in which the weight of thesaline was taken into account, seri-ous flaws in the study design (lackof randomization of the interven-tions) make the results invalid.
Although an alleged benefit ofinstillation of saline is improvementin removal of secretions, to date noadequately reported scientific stud-ies support that contention. Thislack of research is no doubt partlydue to the methodological issuesassociated with the measurementof secretion volumes in clinical stud-ies, meriting further research todetermine the best way to quantifyremoval of pulmonary secretions.17
Effect on Thinning SecretionsAlthough clinicians often believe
that instillation of normal saline“thins” thick pulmonary secretions,
no research has ever shown that thisbelief is correct. In fact, experts inairway humidification long agopointed out the fallacy of this notion,because small-particle humidifica-tion, not administration of a fluidbolus, is required to achieve anysemblance of incorporation of fluid
saturation compared with suction-ing without instillation of saline.
An interesting finding in studies8-13
that showed decreases in oxygena-tion after instillation of saline beforesuctioning was that return to base-line oxygenation levels did not occuruntil at least 3 to 5 minutes after thesuctioning procedure was finished.Although the decrease in oxygena-tion with instillation of normalsaline may not be dramatic, it is farfrom a transient derangement.
Effect on Removal of SecretionsSeveral researchers9,12,15,16 have
attempted to determine if moresecretions are removed with suction-ing when normal saline is instilledthan when suctioning is done with-out instillation of saline. By weigh-ing the volume of secretions removedduring suctioning, the researchers
hoped to quantify differencesbetween the 2 methods of suction-ing. However, in all but a singlestudy, researchers did not take intoaccount the weight of the salineinstilled in their calculations, creat-ing a serious flaw in the experimen-tal design of the study and negating
100 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
into thick secretions.18(p504) And evensmall-particle humidification fallsshort of actually “thinning” secre-tions noticeably. Experts18-20 recom-mend systemic hydration to decreasethe viscosity of pulmonary secre-tions, because thick secretions reflectdehydration of mucous glands. Thetopical application of a 5- or 10-mLbolus of normal saline to thick mucuswill not lead to incorporation of thesaline into the mucus.21
For clinicians who believe thatnormal saline thins secretions, trythe following experiment to see foryourself what impact administrationof a bolus of normal saline has onthick secretions.22 The next time youuse suctioning, use a mucus trap tocollect some of the thick secretions.Then, insert 5 to 10 mL of normalsaline into the trap and observe howthe saline remains separate from the
mucus, even after vigorous shaking.Let the mixture sit a while to validatethat even with exposure over time, themucus and fluid remain separate fromeach other. If normal saline cannotthin thick secretions in a mucus trapwith really vigorous shaking, it cer-tainly cannot do it in a patient’s lungs.
In a laboratory study of endotracheal tubes that hadrecently been removed from patients in the intensivecare unit, the amount of bacteria evacuated from the endof endotracheal tubes was 5 times greater when a bolusof normal saline was administered through the endotra-cheal tube before the suction catheter was introducedthan when a suction catheter alone was passed throughthe endotracheal tube.
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

Risks of Bacterial ContaminationIn 2 studies,23,24 researchers
reported that instillation of normalsaline may place the patient at riskfor hospital-acquired pneumonia.Rutula et al23 found that the rims ofthe individual-dose vials of normalsaline were often contaminated withbacterial organisms just beforeinsertion of the fluid into the endo-tracheal tube. On the basis of thetype of bacterial organisms foundon the rim, they hypothesized thatthe contamination of the vial hadoccurred when clinicians had“popped” the top off the vial with athumb. Although the researchers23
did not evaluate infection of patients,introduction of bacterial organismsbecause of contamination duringadministration of the fluid is cer-tainly theoretically possible.
In a laboratory study24 of endo-tracheal tubes that had recentlybeen removed from patients in theintensive care unit (ICU), the amountof bacteria evacuated from the endof endotracheal tubes was 5 timesgreater when a bolus of normalsaline was administered through theendotracheal tube before the suctioncatheter was introduced than whena suction catheter alone was passedthrough the endotracheal tube. Theinvestigators24 hypothesized that asimilar high load of bacterial con-tamination of the pulmonary systemmight occur when normal saline isinstilled into the endotracheal tubeduring suctioning. The instillationof normal saline may act as a vehicleto “wash” the bacteria that normallycling to the inner aspects of the arti-ficial airway into the lung, poten-tially leading to infection. Haglerand Traver24 did not evaluate clinicalinfection; however, they pointed out
that instillation of saline beforeendotracheal suctioning may havesome unintended outcomes.
Although the normal saline thatis instilled should be sterile and with-out preservatives, isolated cases ofoutbreaks of bacterial pneumoniadue to vials of normal saline con-taminated during the manufactur-ing process have been reported.25,26
Surveys of Nursing PracticeIn several reports7,27-29 since 1996,
researchers have described how oftennurses and respiratory therapistsinstill normal saline before endotra-cheal suctioning. In most of thestudies,7,27,29 25% to 33% of nursesroutinely or frequently instillednormal saline before suctioning.Twice as many respiratory thera-pists as nurses instilled normalsaline.7,29 In a 1996 survey,28 pedi-atric critical care nurses almost uni-versally instilled normal salinebefore doing suctioning. Most ofthe hospitals surveyed indicatedthat instillation of normal salinebefore endotracheal suctioning wasincluded in the hospital’s policy/procedure for suctioning.7
EBP RecommendationsResources for EBP recommenda-
tions are unanimous in their recom-mendation that instillation ofnormal saline should not be per-formed as a routine step with endo-tracheal suctioning. Fromreviews19,20,30,31 of the literature on thetopic to national guidelines32-34 forEBP procedures, experts in airwaymanagement practices reiterate thatdespite some practitioners beliefs,no credible, scientific informationsupports the routine use of instilla-tion of normal saline with endotra-
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 101
cheal suctioning. In addition to thelack of any theoretical benefit, nostudies have shown that instillationof normal saline is beneficial topatients, and some researchers havefound it detrimental.
Verification of ProperPlacement of Gastric andPostpyloric Tubes: What Isthe Best Way?Incidence of Inadvertent Pulmonary Placement
The incidence of inadvertentplacement of gastric or postpylorictubes into the lungs, instead of thegastrointestinal system, with blindinsertion at the bedside is notclearly known. Most of the informa-tion about inadvertent placementhas come from case reports.35,36
According to 2 research studiesdone to determine the sensitivityand specificity of capnography fordetecting inadvertent pulmonaryplacement of gastric and postpy-loric tubes, the incidence of pul-monary placement was 11% (11 of100 attempts) when verified bychest radiography37 and 20% (4 of20 attempts) when verified by car-bon dioxide waveforms.38 Even ifthe actual clinical incidence is lowerthan observed in these limited stud-ies, the complications associatedwith a feeding tube placed in thelung can be lethal; thus, a 100%effective method for verifyingproper location of such tubes isneeded.
Methods of Detecting InadvertentPulmonary Placement
A variety of methods have beenadvocated to detect when a gastricor postpyloric tube has been intro-duced into the pulmonary system:
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

auscultation during air insufflationthrough the tube, pH testing of aspi-rated fluid, visual inspection of aspi-rated fluid, detection of carbondioxide in the tube, and radio -graphic tube verification.
Auscultation During Air Insuffla-tion Through the Tube. Auscultationover the gastric abdominal area dur-ing rapid insufflation of air into thedistal end of a gastrointestinal tubeis commonly performed after atube is inserted. Research on airinsufflation has never documentedthat this technique is accurate foridentifying inadvertent intubationof the lungs. Numerous case reportsof documented inadvertent pul-monary intubation despite ausculta-tion over the gastric area of airduring insufflation, though, havebeen published.36,39,40 In the early1990s, researchers found that airinsufflation with auscultation overthe gastric area could not be used topredict the inadvertent placementof a gastric tube into the lungs.39
Because of the proximity of the lungsand stomach, it is not surprisingthat the sounds created by air insuf-flation through the tube could easilybe transmitted to adjacent areas,causing clinicians to err in deter-mining proper tube placement.
Testing the pH of Aspirated Fluid.Another technique that has beenadvocated over the years to identifyinadvertent pulmonary intubationwith gastric tubes is measuring thepH of fluids aspirated immediatelyafter tube placement.41,42 It washypothesized that because pul-monary secretions have an alkalinepH and gastric contents have anacidic pH, this simple bedside pro-cedure could allow quick identifica-tion of tube location. Because a
variety of situations can alter the pHof the gastric contents from acid toalkaline (drugs that change gastricpH, enteral feeding) and such situa-tions are common in critically illpatients, the usefulness of this tech-nique is limited. The outcome of pHtesting is helpful only if the fluidtested is acidic, thus verifying gastricplacement. If the fluid is alkaline, thegastric contents may be alkaline orthe tube may be in the lung. Becauseof the lack of specificity of the pHtechnique and the numerous situa-tions and conditions that lead toalkaline gastric contents, experts36,43-45
no longer advocate the use of pHtesting to verify tube location.
Visual Inspection of Aspirated Fluid.Visual inspection of the color of fluidaspirated from the tube has beenadvocated as a method to differenti-ate gastric fluid (green, dark yellow)from pulmonary fluid (white, lightyellow). In the only study46 in whichvisual inspection of fluid was evalu-ated as a way of determining gastricor pulmonary location of the tube,visual inspection was a poor predic-tor of tube location. Similar to gas-tric pH, the colors of gastric andpulmonary secretions are altered bya variety of conditions, making devel-opment of a standard difficult.
Presence of Carbon Dioxide in theTube. Most recently, in several smallstudies,37,38,47-51
investigatorsevaluated theuse of devices tomeasure thepresence of car-bon dioxide inthe tube as away to deter-mine if thelungs have been
inadvertently entered. Because car-bon dioxide is present only inexhaled pulmonary gases and not inthe gastric contents, this techniquemay be helpful in differentiatingbetween the 2 locations. In stud-ies37,38,47-50 in which end-tidal carbondioxide monitors or disposable,color-indicator carbon dioxidedevices were connected to the gas-trointestinal tube during insertion,detection of carbon dioxide with thedevices allowed successful detectionof gastric tubes that had beenplaced in the lungs. In all but a sin-gle study,51 no instances of falseidentification of pulmonary place-ment were noted.37,38,47-50 The resultsof these studies show promise forfinding a bedside technique thatallows accurately detection of inap-propriate pulmonary intubation.Because of the consequences ofmissing an incorrect placement of agastric tube, additional studies areneed to validate carbon dioxidedetection techniques in larger andmore diverse populations of patientsand in a variety of clinical situations.Of particular interest is the abilityof multiple caregivers to correctlyinterpret the color indications dis-played by the disposable carbondioxide device and to determine iffluid obstruction in the gastroin-testinal tube and/or contamination
102 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Table 2 Correct size of blood pressure cuff according tocircumference of patient’s arma
Arm circumference,b cm
22-26
27-34
35-44
45-52
Cuff size, cm
Small adult, 12 x 22
Adult, 16 x 30
Large adult, 16 x 36
Adult–thigh, 16 x 42
a Based on data from Pickering et al.54
b Arm circumference is measured midway between acromion and olecranon.
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

of the carbon dioxide indicatoraffects the accuracy of the device.
EBP RecommendationsAt this time, national guidelines
and expert opinion indicate that thebest method for confirming the loca-tion of blindly inserted gastrointesti-nal tubes is chest radiography.36,43-45,52,53
The radiopaque marker on each tubemakes radio graphic detection of inad-vertent pulmonary placement clear,because the tube marker is easilyseen by a radiologist in the right orleft main bronchus, structures easilydiscerned on a chest radiograph.
Use of radiography to validateplacement of small-bore gastroin-testinal tubes is a clinically commonpolicy in many facilities becauseinadvertent pulmonary intubationsare thought to be more commonwith this type of tube. However, in astudy by Burns et al,50 the incidenceof pulmonary intubations did notdiffer between large- and small-boregastric tubes. At this time, nationalguidelines recommend that properplacement of gastric tubes should beconfirmed by radiographic means.
Accurate Measurements ofBlood Pressure
In addition to the nationalguidelines54 for blood pressure meas-
urement, a growing body of evi-dence supports specific proceduraltechniques that will improve theaccuracy and reliability of noninva-sive and invasive measurement ofarterial blood pressure.55
How Do You Pick the CorrectCuff Size?
The American Heart Associationrecommendations for correct sizesof blood pressure cuffs are summa-rized in Table 2. Selection of theappropriate cuff size is importantbecause a cuff that is too smallyields an overestimation of bloodpressure and a cuff that is too largeyields an underestimation of bloodpressure.56
Does Arm Position Make a Difference for Noninvasive Measurement of Blood Pressure?
As with intra-arterial blood pres-sure monitoring,57-59 the appropriatereference level for noninvasivemeasurement of blood pressure isthe heart54 (Figure 1). Blood pres-sure will be overestimated if the armis below the heart and underesti-mated if the arm is positionedabove the heart. Correct positioningof the arm is particularly importantif the patient is sitting up or stand-ing. If the arm is parallel to the
patient or supported on the arm-rest, the systolic and diastolic bloodpressures may be 10 mm Hg higherthan if the arm is supported hori-zontally at heart level (level of themidsternum),60-65 and in patientswith hypertension, the difference inarm position can cause an overesti-mation of systolic blood pressure20 mm Hg.64 With the patientsupine, the arm should be sup-ported at the level of the phlebosta-tic axis (one-half the distance fromthe sternum to the back) ratherthan placed on the bed, a situationthat causes an overestimation ofsystolic and diastolic blood pres-sures of 3 to 5 mm Hg.61,62,66 If apatient is in a lateral recumbentposition, the noninvasive measure-ments of blood pressure takenfrom the “up arm” may be 13 to 17mm Hg lower than measurementsin supine patients, and blood pres-sure measurements from the “downarm” are either inconsistent or sim-ilar to measurements obtained withthe patient supine.67-69
How Should Blood Pressure BeMeasured in Obese Patients?
Obesity alone does not affectthe accuracy of blood pressuremeasurements.70 Blood pressuremeasured in the forearm can be
104 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Figure 1 Correct positioning of the arm for blood pressure measurements in the sitting, supine (0º backrest elevation), and supinewith backrest positions. The arm should be supported and at the level of the heart (midsternum).Reprinted from AACN Practice Alert,55 with permission.
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

measure the blood pressure 3 timesand use the mean value, and (2) inpatients with severe bradycardia,slow deflation of the cuff (target inbradycardia, 2 to 3 mm Hg per pulse)to prevent underestimation of sys-tolic blood pressure and overesti-mation of diastolic blood pressure.A potential limitation of the use ofoscillometric measurement ofblood pressure in patients withmarked arrhythmias is that withthis method the maximal oscilla-tion (mean arterial pressure) isdetected and the systolic and dias-tolic blood pressures are estimated.In patients with atrial fibrillation orfrequent ectopy, the beat-to-beatvariability of stroke volume and theheight of the oscillation may pre-clude the accurate measurement ofthe mean arterial pressure and thusthe systolic and diastolic bloodpressures. Conversely, auscultatedsystolic blood pressure may beoverestimated or underestimatedon the basis of selection of the firstKorotkoff sound. In a comparison75
of 3 sets of auscultated and oscillo-metric measurements of bloodpressure in patients with rate-con-trolled atrial fibrillation, the mean(standard deviation) measurementsof blood pressure for each methodwere as follows: systolic, manual:126 (18) mm Hg, oscillometric: 131(12) mm Hg; diastolic, manual: 72(15) mm Hg, oscillometric: 73 (15)mm Hg. These findings suggest thatthe methods are interchangeable.Because the algorithms for differentoscillometric blood pressuremachines vary, the results of a sin-gle study cannot be generalized toother monitors.76 If a patient isusing an oscillometric cuff at home,the results should be validated by
using auscultation. The accuracy ofoscillometric measurements ofblood pressure in patients withunstable atrial fibrillation has notbeen evaluated.
Should We Compare the ArterialBlood Pressure With the CuffPressure to Ensure That the Arterial Pressure Is Accurate?
The practice of using oscillomet-ric brachial pressure to determineif an arterial pressure monitoringsystem is accurate and to decidewhether to monitor the arterialpressure or the cuff pressure is notevidence based. The following fac-tors should be considered whenevaluating this practice. First, theaortic, brachial, and radial measure-ments of blood pressure are not thesame. As a blood pressure wavemoves into the peripheral vascula-ture, it is modified with an increasein systolic blood pressure and adecrease in diastolic blood pressure,whereas the mean arterial pressureis relatively unchanged. Generally,more central (aortic, femoral,brachial) measurements of systolicblood pressure are lower than radialmeasurements of systolic bloodpressure by 7 to 14 mm Hg and aresimilar to or higher than diastolicblood pressure by 1 to 9 mm Hg,whereas the mean arterial pressureis unchanged.70,77 Second, the differ-ences in systolic blood pressurechange with aging (radial approxi-mately the same as aortic systolicblood pressure),78,79 vasoconstriction(radial < brachial and femoral),80-83
and vasodilatation (femoral approx-imately the same as radial; aortic ≤radial).84,85 In addition to evaluatingan absolute pressure, monitoring fortrends or changes in blood pressure
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 105
used if a correct cuff cannot befound54,71,72; however, blood pressurein the forearm may be higher thanblood pressure in the upper arm.For example, in a study73 of patientswho were morbidly obese, only 19%had systolic and 28% had diastolicblood pressure measurements inthe forearm within 10 mm Hg ofthe measurements in the upperarm.
The challenge with measuringblood pressure in patients who aremorbidly obese is finding an appro-priately sized cuff, although new cuffsare being developed that have longlength but normal width. For every5-cm increase in arm circumference(starting at 35 cm), use of a standardcuff leads to an overestimation ofsystolic blood pressure by 3 to 5 mmHg and diastolic blood pressure by1 to 3 mm Hg compared with anappropriately sized large cuff.74 Tosize the cuff correctly, measure thecircumference of the patient’s armmidway between the elbow and thewrist. Cuff size should be similar tothat specified in the guidelines forupper arm circumference (Table 2).The cuff should be centered betweenthe elbow and wrist, and the armshould be supported at the level ofthe heart.60-64
Can You Use an Automatic(Oscillometric) Cuff to MeasureBlood Pressure in Patients WithAtrial Fibrillation?
No evidence-based guidelines areavailable for noninvasive measure-ment of blood pressure in patientswith arrhythmias. Current recom-mendations based on the AmericanHeart Association consensus54 forauscultated blood pressure inpatients with arrhythmias are (1)
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

are (1) an increased emphasis onavoiding formation of microbubbles,including completely filling the dripchamber and using minimal pres-sure during initial flushing of thecatheter, and (2) the use of the rocketflush89 (ie, vigorously flushing thesystem with 10 mL of flush solutionthrough the proximal port to removeany hidden microbubbles). Therocket flush should never be per-formed when the catheter is in placein a patient because of the risk ofretrograde air embolization. Whenthis protocol (minus the fast flush)was used, 59% of pressure systemswith a blood reservoir had adequatedynamic response characteristics and41% were underdamped. The additionof the fast flush markedly improvedthe systems (92% adequate/ optimaland 8% underdamped).88 Validated,evidence-based algorithms87,90 are
over time to guide clinical decisionsis equally important. Finally, themore important clinical questions arewhether the blood pressure is ade-quate, if a given method accuratelyreflects central blood pressure, andwhether the technical aspects of themethod have been optimized.
What Steps Will Improve theDynamic Response Characteristicsof the Invasive Arterial PressureMonitoring System?
Arterial pressure monitoring sys-tems, particularly those with bloodreservoirs, tend to be underdamped,which may lead to an overestimationof systolic pressure and an underes-timation of diastolic pressure.86,87 Avalidated evidence-based protocolfor preparation for an invasivecatheter is presented in Table 3.88
Two points to note in this protocol
also available to optimize a systemonce it is in use in a patient.
Selection of Electrocardiographic Leads
Electrocardiographic (ECG) mon-itoring is performed for 3 primaryreasons: detection of arrhythmiaand conduction disturbance, moni-toring of the ST segment, and moni-toring of the QT interval.
TelemetryAre 3-Lead Systems Equivalent to
5-Lead Systems for Monitoring Wide-Complex Tachycardia? For a 3-leadsystem, a modified chest lead (MCL-1 or MCL-6) should be used insteadof lead II for the differential diagno-sis of wide-complex tachycardia.91,92
Use of an MCL requires the follow-ing modifications in lead placement:right arm electrode on left shoulder,
106 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Table 3 Evidence-based protocol for preparation of an invasive pressure cathetera
1. Cleanse hands
2. Gather supplies (intravenous fluid, pressure monitoring kit, 10-mL syringe, and pressure bag)
3. Prime pressure monitoring system to remove all air a. Remove pressure monitoring kit from package, open blood salvage reservoir, tighten connections, close roller clamp, turn stop-
cock OFF to patient (off toward distal end), and remove vented stopcock cap b. Invert bag of intravenous fluid and, using sterile technique, insert spike into itc. Leave the spiked bag upside down, open roller clamp, and simultaneously activate fast-flush device continuously while gently squeezing
to apply pressure to bag of intravenous fluids to slowly clear air from bag and drip chamber; completely fill the drip chamber with intravenous fluid
d. Turn bag upright once fluid is advanced sufficiently past the drip chambere. Apply gentle pressure (50 mm Hg) to the bag (or hang the bag about 30 inches above distal end of tubing) and activate fast-flush
device, advance fluid, priming the stopcockf. Orient the blood reservoir so that air will be completely removed by the advancing fluid (tilt distal end upright at 45º), and continue
flushing to prime the entire catheter g. Close reservoir and flush catheter to move any residual air bubbles from the reservoirh. Perform rocket flush (NEVER PERFORM WHEN CATHETER IS IN PATIENT)
(1) Turn stopcock off to distal end of catheter (“off to patient”)(2) Attach 10-mL syringe to stopcock near the transducer by using sterile technique and slowly withdraw intravenous fluid to fill
syringe(3) Turn stopcock off to transducer(4) Flush line quickly with 10 mL of normal saline from syringe to remove any remaining air bubbles(5) Turn stopcock off(6) Inspect catheter, remove any remaining air by fast flushing and rocket flush as needed(7) Remove syringe and cap stopcock with closed cap by using sterile technique
5. Place bag of fluid into a pressure bag and inflate bag to 250-300 mm Hg and check for air in catheter
6. Evaluate dynamic response characteristics; goal: adequate or optimal
a Based on data from Bridges et al.88
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from
segment monitoring in 250patients, 55 (22%) had transientmyocardial ischemia and of these55, 41 (75%) had silent ischemia.Similarly, in another study100 of18 394 hours of 12-lead ST-segmentmonitoring in patients after anacute myocardial infarction or PCI,463 ischemic events were detectedand of these, 80% were silent. Silentischemic episodes might be missedif ECG monitoring is intermittent.
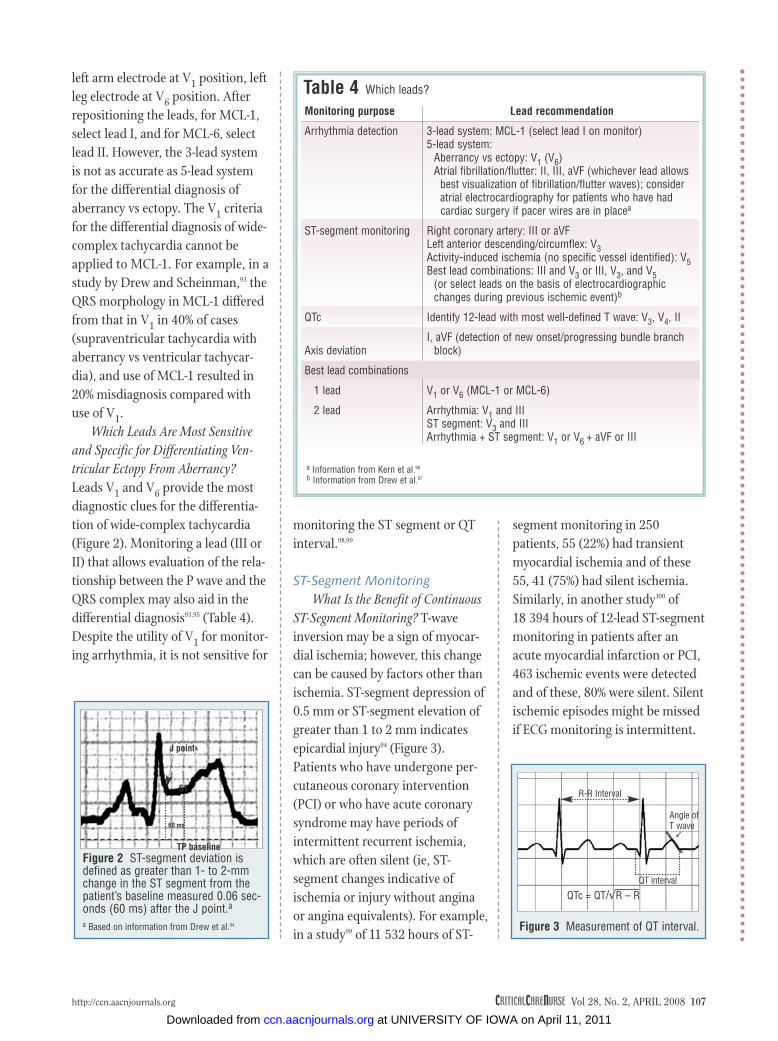
Figure 2 ST-segment deviation isdefined as greater than 1- to 2-mmchange in the ST segment from thepatient’s baseline measured 0.06 sec-onds (60 ms) after the J point.aa Based on information from Drew et al.94
TP baseline
ST
60 ms
J point
monitoring the ST segment or QTinterval.98,99
ST-Segment MonitoringWhat Is the Benefit of Continuous
ST-Segment Monitoring? T-waveinversion may be a sign of myocar-dial ischemia; however, this changecan be caused by factors other thanischemia. ST-segment depression of0.5 mm or ST-segment elevation ofgreater than 1 to 2 mm indicatesepicardial injury94 (Figure 3).Patients who have undergone per-cutaneous coronary intervention(PCI) or who have acute coronarysyndrome may have periods ofintermittent recurrent ischemia,which are often silent (ie, ST-segment changes indicative ofischemia or injury without anginaor angina equivalents). For example,in a study99 of 11 532 hours of ST-
left arm electrode at V1 position, leftleg electrode at V6 position. Afterrepositioning the leads, for MCL-1,select lead I, and for MCL-6, selectlead II. However, the 3-lead systemis not as accurate as 5-lead systemfor the differential diagnosis ofaberrancy vs ectopy. The V1 criteriafor the differential diagnosis of wide-complex tachycardia cannot beapplied to MCL-1. For example, in astudy by Drew and Scheinman,93 theQRS morphology in MCL-1 differedfrom that in V1 in 40% of cases(supraventricular tachycardia withaberrancy vs ventricular tachycar-dia), and use of MCL-1 resulted in20% misdiagnosis compared withuse of V1.
Which Leads Are Most Sensitiveand Specific for Differentiating Ven-tricular Ectopy From Aberrancy?Leads V1 and V6 provide the mostdiagnostic clues for the differentia-tion of wide-complex tachycardia(Figure 2). Monitoring a lead (III orII) that allows evaluation of the rela-tionship between the P wave and theQRS complex may also aid in thedifferential diagnosis93,95 (Table 4).Despite the utility of V1 for monitor-ing arrhythmia, it is not sensitive for
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 107
Table 4 Which leads?
Lead recommendation
3-lead system: MCL-1 (select lead I on monitor)5-lead system:
Aberrancy vs ectopy: V1 (V6)Atrial fibrillation/flutter: II, III, aVF (whichever lead allows
best visualization of fibrillation/flutter waves); consider atrial electrocardiography for patients who have had cardiac surgery if pacer wires are in placea
Right coronary artery: III or aVFLeft anterior descending/circumflex: V3Activity-induced ischemia (no specific vessel identified): V5Best lead combinations: III and V3 or III, V3, and V5
(or select leads on the basis of electrocardiographicchanges during previous ischemic event)b
Identify 12-lead with most well-defined T wave: V3, V4, II
I, aVF (detection of new onset/progressing bundle branchblock)
V1 or V6 (MCL-1 or MCL-6)
Arrhythmia: V1 and III ST segment: V3 and IIIArrhythmia + ST segment: V1 or V6 + aVF or III
Monitoring purpose
Arrhythmia detection
ST-segment monitoring
QTc
Axis deviation
Best lead combinations
1 lead
2 lead
a Information from Kern et al.96
b Information from Drew et al.97
Figure 3 Measurement of QT interval.
R-R Interval
Angle ofT wave
QT interval
QTc = QT/√R – R
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

Should You Select the Bedside Leadon the Basis of the Patient’s ST-SegmentElevation “Fingerprint” During PCI?The ST-segment “fingerprint” is thelead with the maximal ST-segmentdeviation (Figure 2) during an acutemyocardial infarction or a PCI.101
The usefulness of the ST-segmentfingerprint varies depending on theintent of the monitoring. The fin-gerprint is useful in detecting acutereocclusion after a PCI.100,101 However,Drew et al100 found that when thefingerprint was used, 53% of recur-rent ischemic events were notdetected. Of note, leads V1 and IIdid not show ST-segment deviationin 42% of cases. Additionally,ischemia may be detected in multi-ple leads for a given patient.102 Ifcontinuous multilead ST-segmentmonitoring is not available, the ECGleads that are most sensitive andspecific for detecting ischemiashould be used98,99 (Table 4).
QT-Interval MonitoringHow Should the QT Interval Be
Measured? Most of the recommen-dations for QT-interval monitoringare based on expert opinion.95,103 TheQT interval, which represents theduration of electrical activation(depolarization) and recovery (repo-larization), is measured from thestart of the QRS complex to the pointwhere the T wave returns to the TPbaseline (Figure 3). One suggestion toaid in identifying this point is to drawa tangent along the steepest part ofthe downslope of the T wave; the endof the QT interval is where this lineintersects the TP baseline. If a U waveis present, the QT interval is meas-ured from the onset of the QRS com-plex to the lowest point between theT and the U wave (Figure 4); how-
ever, if the U wave is large andmerges with the T wave, it shouldbe included in the measurement.103
Lead II may provide the best separa-tion between the T and the U waves.If a biphasic T wave is present, thepoint of the final return of the T waveto baseline should be used. No con-sensus has been reached on how tomeasure the QT interval during atrialfibrillation. One suggestion is to takethe QTc from the shortest and longestR-R intervals and average the 2 val-ues.104 The same lead should be usedfor serial measurements.
Because the QT interval isinversely related to heart rate, itmust be corrected or normalized toa heart rate of 60/min. The mostcommonly used formula to normal-ize the QT interval (QTc) is theBazett formula,105 which is the QTdivided by the square root of thepreceding R-R interval in seconds:
QTc = QT/√R-R Debate is increasing about the
use of the Bazett formula, because itresults in an underestimation of theQTc at low heart rates and overesti-mations of it at high heart rates.106,107
A normal QTc is less than 0.46seconds in women and less than 0.45seconds in men. An abnormal QTcfor women is greater than 0.48 sec-onds and for men is greater than0.47 seconds. A QTc greater than0.5 seconds is considered an increasedrisk for torsades de pointes, although
torsades de pointes may also developin patients with a QTc less than 0.5seconds.103 There is no QTc belowwhich a patient is considered free ofrisk for arrhythmias.104
Can Bedside Monitoring Replace the12-Lead ECG for the Diagnosis of Pro-longed QTc? 12-Lead ECG is the stan-dard for the diagnosis of prolongedQT interval, and it cannot be replacedby bedside monitoring. The QTinterval should be measured manu-ally from the same lead, and the cor-rected value should be averaged over3 to 5 beats.103 The QTc should bemeasured before the start of proar-rhythmic therapy, at the time of theanticipated peak plasma level of thedrug, after a change in drug dosage,and every 8 to 12 hours or moreoften if the QTc is prolonged.98,108
Bedside monitoring may beuseful in detecting changes in theQTc and determining if an additional12-lead ECG should be obtained. Ina study109 in which QTc measure-ments from a 12-lead ECG werecompared with those from a bed-side monitor (leads I/II), with a cut-off of 0.46 seconds, the monitor QTcagreed with the 12-lead ECG in 72%.However, in 26%, the QTc from thebedside monitor was greater than0.46 seconds, whereas the 12-leadQTc was within normal limits; andin 2%, the 12-lead QTc was longerthan 0.46 seconds, whereas thebedside monitor was within normallimits (bedside QTc sensitivity 50%,specificity 92%). This high speci-ficity and low sensitivity means thatepisodes of prolonged QTc will notgenerally be missed when a bedsideECG is used; however, prolongedQTc may be overdiagnosed. Thediagnosis of prolonged QTc madeon the basis of values on the bedside
108 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Figure 4 Measurement of QT intervalwhen a U wave is present.
T wave U wave
QT interval
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from
monitor should be confirmed with a12-lead ECG.
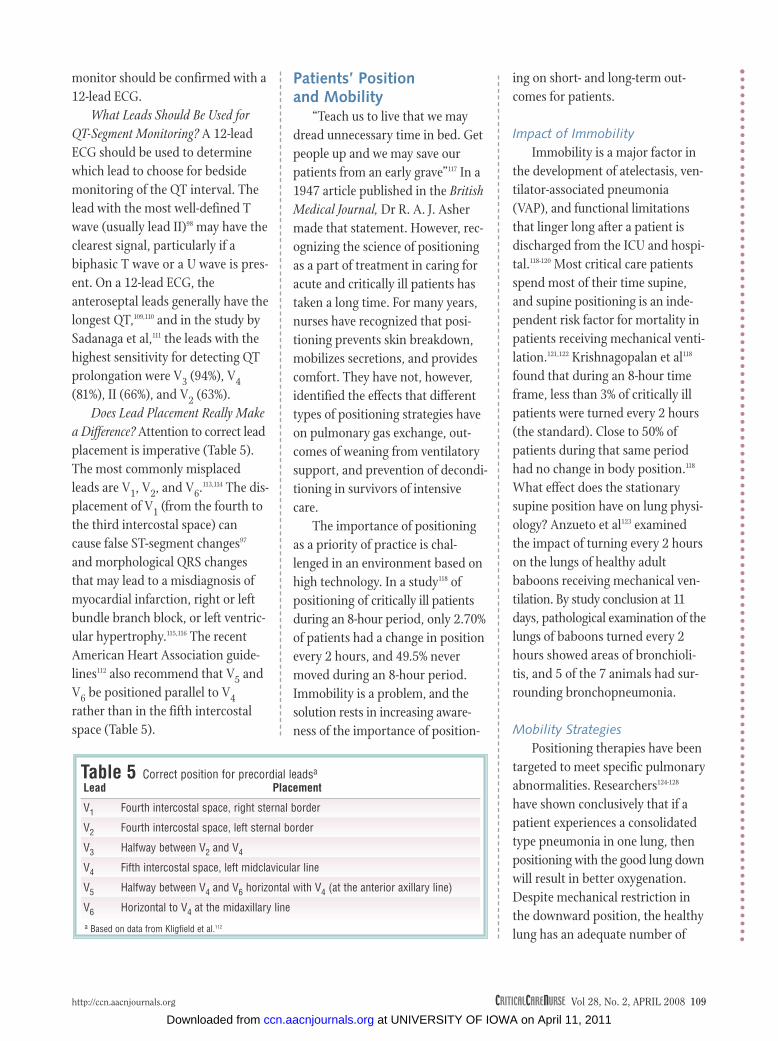
What Leads Should Be Used forQT-Segment Monitoring? A 12-leadECG should be used to determinewhich lead to choose for bedsidemonitoring of the QT interval. Thelead with the most well-defined Twave (usually lead II)98 may have theclearest signal, particularly if abiphasic T wave or a U wave is pres-ent. On a 12-lead ECG, theanteroseptal leads generally have thelongest QT,109,110 and in the study bySadanaga et al,111 the leads with thehighest sensitivity for detecting QTprolongation were V3 (94%), V4(81%), II (66%), and V2 (63%).
Does Lead Placement Really Makea Difference? Attention to correct leadplacement is imperative (Table 5).The most commonly misplacedleads are V1, V2, and V6.113,114 The dis-placement of V1 (from the fourth tothe third intercostal space) cancause false ST-segment changes97
and morphological QRS changesthat may lead to a misdiagnosis ofmyocardial infarction, right or leftbundle branch block, or left ventric-ular hypertrophy.115,116 The recentAmerican Heart Association guide-lines112 also recommend that V5 andV6 be positioned parallel to V4rather than in the fifth intercostalspace (Table 5).
Patients’ Position and Mobility
“Teach us to live that we maydread unnecessary time in bed. Getpeople up and we may save ourpatients from an early grave”117 In a1947 article published in the BritishMedical Journal, Dr R. A. J. Ashermade that statement. However, rec-ognizing the science of positioningas a part of treatment in caring foracute and critically ill patients hastaken a long time. For many years,nurses have recognized that posi-tioning prevents skin breakdown,mobilizes secretions, and providescomfort. They have not, however,identified the effects that differenttypes of positioning strategies haveon pulmonary gas exchange, out-comes of weaning from ventilatorysupport, and prevention of decondi-tioning in survivors of intensivecare.
The importance of positioningas a priority of practice is chal-lenged in an environment based onhigh technology. In a study118 ofpositioning of critically ill patientsduring an 8-hour period, only 2.70%of patients had a change in positionevery 2 hours, and 49.5% nevermoved during an 8-hour period.Immobility is a problem, and thesolution rests in increasing aware-ness of the importance of position-
ing on short- and long-term out-comes for patients.
Impact of ImmobilityImmobility is a major factor in
the development of atelectasis, ven-tilator-associated pneumonia(VAP), and functional limitationsthat linger long after a patient isdischarged from the ICU and hospi-tal.118-120 Most critical care patientsspend most of their time supine,and supine positioning is an inde-pendent risk factor for mortality inpatients receiving mechanical venti-lation.121,122 Krishnagopalan et al118
found that during an 8-hour timeframe, less than 3% of critically illpatients were turned every 2 hours(the standard). Close to 50% ofpatients during that same periodhad no change in body position.118
What effect does the stationarysupine position have on lung physi-ology? Anzueto et al123 examinedthe impact of turning every 2 hourson the lungs of healthy adultbaboons receiving mechanical ven-tilation. By study conclusion at 11days, pathological examination of thelungs of baboons turned every 2hours showed areas of bronchioli-tis, and 5 of the 7 animals had sur-rounding bronchopneumonia.
Mobility StrategiesPositioning therapies have been
targeted to meet specific pulmonaryabnormalities. Researchers124-128
have shown conclusively that if apatient experiences a consolidatedtype pneumonia in one lung, thenpositioning with the good lung downwill result in better oxygenation.Despite mechanical restriction inthe downward position, the healthylung has an adequate number of
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 109
Table 5 Correct position for precordial leadsa
Lead
V1
V2
V3
V4
V5
V6
a Based on data from Kligfield et al.112
Placement
Fourth intercostal space, right sternal border
Fourth intercostal space, left sternal border
Halfway between V2 and V4
Fifth intercostal space, left midclavicular line
Halfway between V4 and V6 horizontal with V4 (at the anterior axillary line)
Horizontal to V4 at the midaxillary line
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

functioning alveoli to match gravity-dependent perfusion and thus pro-mote effective gas exchange. Forpatients with bilateral lung disease,the best position is selected on thebasis of the severity of the patient’slung disease and critical illness. Formany patients, turning every 2 hoursis not enough to preserve the oxy-genating ability of the lungs or toprevent pneumonia.128,129 When therisk for complications of immobilityare high, the use of rotational ther-apy is often considered.
Kinetic therapy/table-based rota-tion and continuous lateral rotationtherapy reduce the incidence of VAPand atelectasis.129-135 The results ofstudies134,135 on the contribution of
rotational therapy to reducing dura-tion of ventilatory support and lengthof stay in the ICU are conflicting. Inmost studies, patients were rotatedmore than 18 hours a day to achievemaximum benefit and the therapywas started as early as possible.Researchers have not yet determinedwhether the degree or the fre-quency of rotation is the crucial fac-tor. Ahrens et al134 randomized 234medical-surgical trauma patients toreceive rotation therapy or standardcare and measured the impact onVAP, lobar atelectasis, and length ofstay. Rotational therapy resulted ina significant reduction in the occur-rence of VAP and lobar atelectasisbut had no effect on length of stay.134
Four systematic reviews129,136-138 of theliterature on rotational therapy haveindicated similar results. In the mostrecent review,138 regardless of therotational degree achieved, the pro-portion of patients with VAP wassignificantly lower for the rotationgroups than for the control groups(P<.001; Figure 5).
For patients with severe acuterespiratory distress syndrome(ARDS), rotational therapy may notbe sufficient to prevent complica-tions and improve gas exchange.One strategy examined as a mecha-nism for recruiting alveoli andimproving gas exchange in patientswith ARDS is use of the prone posi-tion. In recent systematic reviews143-145
110 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Figure 5 Meta-analysis of pneumonia (with subgroups of prophylaxis and treatment for respiratory dysfunction): rotation versuscontrol.
Study or subcategory Rotation
Proportion of patients with pneumonia
ControlOdds ratio (fixed)
95% CI
Odds ratio (fixed)95% CI
Demarest et al139
Fink et al131
Gentilello et al132
Kelley et al133
Kirschenbaum et al140
Summer et al135
Traver et al141
Whiteman et al142
deBoisblanc et al130
Subtotal (95% CI)
4/14
19/48
13/38
13/25
10/20
7/42
17/59
14/36
11/51
108/333
45/137
45/137
3.45
14.55
7.58
6.77
6.52
5.38
10.24
8.04
9.95
72.49
27.51
27.51
100.00
0.17 (0.02, 1.72)
0.24 (0.09, 0.65)
0.44 (0.13, 1.42)
0.36 (0.10, 1.30)
0.21 (0.05, 0.98)
0.54 (0.15, 2.01)
0.55 (0.21, 1.42)
0.68 (0.25, 1.86)
0.35 (0.12, 1.01)
0.40 (0.27, 0.58)
0.34 (0.18, 0.67)
0.34 (0.18, 0.67)
0.38 (0.27, 0.53)
Weight,%
Favors treatment
Favors control
1 520.2 0.50.1 10Test for heterogeneity: χ2 = 4.16, df = 9 (P = .90), I2 = 0%Test for overall effect: Z = 5.63 (P < .001)
Pneumonia and prophylaxis
Pneumonia treatment
Ahrens et al134
Subtotal (95% CI)
Total (95% CI)
1/16
7/51
5/27
5/18
3/17
4/41
8/44
10/33
6/69
49/316
14/97
14/97
Test for heterogeneity: χ2 = 4.03, df = 8 (P = .85), I2 = 0%Test for overall effect: Z = 4.68 (P < .001)
Test for heterogeneity: not applicableTest for overall effect: Z = 3.12 (P = .002)
63/413 153/470
Abbreviation: CI, confidence interval.Reprinted from Goldhill et al,138 with permission.
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

of the literature on prone positioning,more than 70% of all ARDS patientsstudied responded to prone posi-
tioning with a 20% increase in PaO2or an increase greater than 20 in theratio of PaO2 to fraction of inspired
oxygen within 2 hours of the turn.Gattinoni et al146 and Guerin et al147
published the anticipated definitive
112 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Figure 6 Suggested algorithm for positioning critically ill patients.Reprinted from Ahrens et al,150 with permission from ADVANCING NURSING LLC.
Progressive Mobility Algorithm for Critically Ill Patients
Mobility Recommendation: Turn Patient Every Two Hours, Assess Every Twelve Hours for Risk for Pulmonary Complications and Deconditioning and Follow Appropriate Process
Is patient immobile plus one or more...• Lobar collapse / atelectasis,
excessive secretions, and/or•P/F ratio <200 and/or FiO2
>40% with a PaO2 of 80 mmHg• Hemodynamic instability with
manual turning (�SaO2,�BP and �HR)2, or
• Decreased mental status
Initiate / continuecontinuous lateral rotation
therapy (CLRT)1
(18hrs/day)2
Has situation resolved?(assess every 24 hours)
Does patient have...• Severe ARDS (FiO2 of
40% and 10 PEEP and/or a P/F ratio of <100, and/or
• Have other lungrecruitment strategies (i.e.,PEEP) been maximized orfailed and the FiO2 remains>60%, or
• Pulmonary statuscontinuing to deteriorate?
Initiate / continue prone positioning2
Maintain rotational therapywhen the patient is supine
Has situation resolved?(assess every24 hours)
Continue CLRT and progressiveupright mobility process2
Is patient...• Deconditioned by >3
days of immobility, or• Ready to begin ventilator
weaning, or• Does patient require
orthostatic training toupright positioning?
Initiate / continueprogressive uprightmobility process2,3
Is patient successfullyambulating?
Discontinue progressive uprightmobility process
Y Y
Y Y
Y
N
When indications for CLRT are resolved and patient can besafely mobilized in other ways
(HOB >30°, manually turn withoutinstability, tolerate up in chair), go to
progressive upright mobility2
• Assess adherence to adequacy of turn and hrs/day CLRT guideline
• Adjust therapy and continue• Does patient meet criteria
for prone positioning?
Have therapy goalschanged to
palliative care?
YDiscontinue therapy
NNot a candidate
N
N
• Assess adherence to prone position guidelines
• Assess need for CLRT
Have therapy goalschanged to
palliative care?
YDiscontinue prone position
Not a candidate
N
N
N
N
N
N
Y
A.
B.
C.
AuthorsTom Ahrens, DSN, RN, CCRN, CS, FAAN
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

outcomes research for the use ofprone positioning in patients withARDS/acute lung injury. The resultswere less than promising, indicatingno improvement in mortality in adiverse critically ill population. Thesenegative outcomes may have beeninfluenced by a number of method-ological challenges.148 In both stud-ies,146,147 the average range of tidalvolume was greater than 9 mL/kgin both groups, and as indicated inthe landmark ARDS Network venti-lator study,149 tidal volumes greaterthan 6 mL/kg may contribute toventilator-induced lung injury. Aphase 3 trial of prone positioningwith patients receiving 6 mL/kg tidalvolume and positioned prone morethan 18 hours a day is under way.
Progressive Mobility: Combating Deconditioning
Once a patient’s hemodynamicstatus allows forms of mobilization,every attempt should be made toprogressively mobilize the patient todangle the legs, sit in a chair, bearweight, and walk to decrease thesevere muscle wasting that occurs incritically ill patients.121 Hemodynamicinstability is due to spending pro-longed periods in a stationary posi-tion or the establishment of a“gravitational equilibrium.”145 Thephysical deconditioning and chal-lenges with hemodynamic instabilitythat occur with bed rest can be dealtwith by using a stepwise mobilityprogression program (Figure 6). Oncea patient’s cardiovascular system isstable when the head of bed is higherthan 30º, a progressive mobilityprogram can be started. The goal isto progress in a stepwise fashion byincreasing the height of the head ofthe bed, followed by placing the legs
in a dependent position. If this changeis tolerated, dangling of the legs andthen weight bearing should begin assoon as possible. The next step issupported ambulation. The mobilityprogram can be performed safelywhile the patient is intubated andreceiving mechanical ventilation.151
One group152 who used the bed-chairposition 3 times a day for patientswho met the criteria for mobiliza-tion reported a decrease in ICUlength of stay and occurrence ofVAP.
Methods and equipment thatsupport stepwise mobility progres-sion are essential to meet the physi-ological demands of the healingprocess. Having the methods andequipment will allow nurses to dowhat the evidence indicates is theright thing with minimal use ofmanpower. Mobility is a fundamen-tal nursing activity that requiresin-depth knowledge and skill foreffective use in critically ill patients.As a core component of care, mobil-ity helps in managing secretions,reducing feelings of powerlessness,preventing muscle wasting, improv-ing gas exchange, and decreasingthe incidence of atelectasis and VAP.Matching the right time of the ill-ness to the right positioning strategywill help achieve good outcomes forpatients. Nurses have a uniqueopportunity to affect patients out-comes noninvasively through theindependent activity of mobility.
EBP RecommendationsEBP practice recommendations
for positioning are as follows:• If a patient experiences consol-
idated pneumonia in one lung, posi-tioning with the good lung downwill result in better oxygenation.
• Progressive mobilization todangling legs, standing, and walkingare safe for intubated patients.
• Patients breathe better andexperience improved oxygenationwith higher elevations of the head ofthe bed if their hemodynamic statusis such that they can tolerate the ele-vation.
• For many critically ill patients,turning every 2 hours is not enoughto preserve the oxygenating abilityof the lungs or to prevent healthcare–acquired pneumonia.
• Kinetic and continuous lateralrotation therapy reduces the risk ofVAP in patients receiving mechanicalventilation. Optimal benefit dependson early placement and more than18 hours of rotation per day. Researchhas not yet determined whether thedegree or the frequency of rotationis the crucial factor.
• Prone positioning improvesoxygenation but has not yet beenshown to affect mortality.
• Use of the prone position shouldbe considered after conventionalstrategies for lung recruitment havebeen tried unsuccessfully.
The Glasgow Coma Scalein Neurological Assessment
For decades, the level of con-sciousness has been deservedlydescribed as the most sensitive andthe earliest indicator of progres-sion in intracranial abnormalitiessuch as intracranial hyperten-sion.153,154 Since its introduction in1974, the Glasgow Coma Scale(GCS)155 has been used in manyclinical areas to assess and docu-ment consciousness and respon-siveness. The GCS is used to assigna numerical value to a set ofresponses in 3 spheres: eye opening,
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 113
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

widely used but does have someimportant drawbacks and limita-tions (Table 7). Patients with spe-cific clinical states such as locked-insyndrome, catatonia, and psycho -genic coma may have a GCS scoreindicating depression of conscious-ness and responsiveness.157 Thesepatients may actually have a higher
motor responses, and verbalresponses (Table 6).
Limitations of the GCS in Neurological Evaluation
The GCS was initially intendedto standardize patients’ assessmentand improve communication aboutneurological status.156 The GCS is
degree of brain responsivenessthan initially estimated solely onthe basis of GCS assessment.
In locked-in syndrome, patientsare awake and can follow commandssuch as select eye movements. Addi-tional skeletal muscle movement isnot possible because of paralysisbelow the third cranial nerve.157 Incatatonic states, patients mayappear unresponsive, but electroen-cephalographic evaluation indicateslow-amplitude, high-frequencyactivity rather than slow-wave,high-amplitude activity associatedwith unresponsive states due tostructural or metabolic braininjury.157 In psychogenic coma,electroencephalographic evaluationindicates an awake rhythm.157
Even with these limitations, theGCS is used extensively, and theGCS score is incorporated into manycritical care documentation records,trauma and emergency medicine doc-umentation systems, and other clini-cal scoring systems. Additionallimitations exist in each of the 3
114 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
Table 7 Limitations of the Glasgow Coma Scale in clinical neurological evaluationa
Global limitations
No direct incorporation of assessment of brain stem functionEquivocal findings when verbal response is assessed in patients with an artificial airwayIncreased focus on verbal rather than motor responsesLack of sensitivity to clinical states mimicking depressed consciousness such as locked-in syndrome, catatonic states, and psychogenic
comaCultural differences between clinician and patientLanguage differences preventing understanding of questions or verbal commandsHearing deficit preventing understanding of questions or verbal commands
Domain-specific limitations
Eye openingDamage of the oculomotor nerve (eyelid/eye opening) from trauma or surgery may prevent an awake patient from opening the
affected eye
Verbal responseDamage of speech centers, artificial airway, hearing deficit, or not understanding the question may yield an inappropriate low score
Motor responseHearing deficit or inconsistency in noxious stimulation by clinician may yield inappropriately low score
a Based on data from Sternbach,156 Cartlidge,157 and Edwards.158
Table 6 Scoring on the Glasgow Coma Scalea
Response
Eye openingOpens eyes spontaneouslyOpens eyes in response to speechOpens eyes in response to painful stimulation (eg, airway suctioning)Does not open eyes in response to stimulation
Motor responseFollows commandsMakes localized movement in response to painful stimulationMakes nonpurposeful movement in response to painful stimulationUpper extremity flexion/lower extremity extension to painExtends all extremities to painNo response to pain
Verbal responseOriented to person, place, and timeConfused conversationInappropriate wordsIncomprehensible soundsNo response
Score
4321
654321
54321
a Based on data from Arbour153 and Teasdale and Jennett.155
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

appropriate to preserve the optionof organ donation for family mem-bers.153 GCS scores determined inthe prehospital setting and afterarrival in the acute care setting cor-relate closely and are predictive ofoutcome as well as potential needfor neurosurgical intervention.161 AGCS score of 3 in a patient with reac-tive pupils is predictive of potentiallybetter outcomes and suggests thatthe patient might benefit fromaggressive resuscitation.162
Research and Alternatives to the GCS
Because of the limitations of theGCS, research into alternative neu-rological assessment tools is ongoing.One tool, the Full Outline of UnRe-sponsiveness (Table 9), has beenstudied in multiple clinical settingsby members of several disciplines,including critical care/neurosciencenurses, neurology residents, andneurointensivists.163 The tool is easyto use and has good interrater
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 115
Table 8 Clinical uses of the Glasgow Coma Scalea
Rapid assessment, documentation and communication of neurological status
Guidance for therapeutic decisions and timing of invasive procedures such as monitor-ing of intracranial pressure and ventricular drainage
Assessing progression of brain injury or neurological improvement over time
Determining baseline neurological status as a starting point for therapeutic interventions
Assessment of neurological status after ingestion of a toxin
Predictive value regarding clinical and neurological outcome after brain injury a Based on data from Edwards,158 Heard and Bebarta,159 Tien et al,160 and Davis et al.161
spheres assessed by the GCS (Table7). In patients with these limitations,the GCS score may provide inaccuratedata on consciousness, motor func-tion, and arousal.
The effectiveness of the GCSdepends on the ability of a patientto respond and interact with a clini-cian. Optimal neurological assess-ment will indicate clinical statesthat interfere with and limit the effi-cacy of the GCS. Deep sedation/analgesia produces a drug-induceddepression of consciousness, arousal,and cognitive ability, making theGCS ineffective. In this setting, asedation assessment tool may behighly appropriate. Neuromuscularblockade, in a dose-related manner,produces skeletal muscle relaxationin which a patient may potentiallybe awake but appears to be poorlyresponsive solely because of drugeffects on neuromuscular transmis-sion, not brain function. In eachinstance, optimal evaluation of thecentral nervous system is facilitatedby using electrophysiological moni-toring.
Predictive Value of GCS ScoresIn clinical practice, the GCS score
is used for multiple purposes, includ-ing guiding therapeutic decisions,predicting outcomes, and evaluatingpatients after they have ingested atoxin159 (Table 8).
Available research supports thepredictive value of GCS scores forclinical outcomes, particularly whenthe scores are used in context withother neurological data. Patientswith a GCS score of 3 and fixed,dilated pupils after brain traumahave no reasonable chance for sur-vival.160 Aggressive resuscitationand physiological support may be
Table 9 Criteria used to determine scores on the Full Outline of UnResponsivenessa
Eye response4 = Eyelids open or opened, tracking, or blinking on command3 = Eyelids open but not tracking2 = Eyelids closed but open to loud voice1 = Eyelids closed but open to pain0 = Eyelids remain closed with pain
Motor response4 = Thumbs-up, fist, or peace sign3 = Localizing to pain2 = Flexion response to pain1 = Extension response to pain0 = No response to pain or generalized myoclonus status
Brain stem reflexes4 = Pupil and corneal reflexes present3 = One pupil wide and fixed2 = Pupil or corneal reflexes absent1 = Pupil and corneal reflexes absent0 = Absent pupil, corneal, and cough reflexes
Respirations4 = Not intubated, regular breathing pattern3 = Not intubated, Cheyne-Stokes breathing pattern2 = Not intubated, irregular breathing1 = Respirations greater than ventilator rate0 = Respirations at ventilator rate or apnea
a Based on data from Lieberman et al,162 and Wijdicks et al.163
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

agreement between experiencedand novice nurses from the neuro-science ICU and other nurses.164
Moreover, it adds brain stem andrespiratory assessment and providesadditional information beyond thatprovided by the GCS.163,164 It canassist in detecting disorders suchas uncal herniation and locked-insyndrome164 and in predicting in-hospital mortality.163,164
EBP RecommendationsBest clinical practice for neuro-
logical assessment includes optimaland consistent use of the GCS plusinclusion of other neurological datasuch as assessment of brain stemreflexes; eye examination, includingpupil reactivity and extraocularmovement; vital signs; and respira-tory rate, depth, and pattern. Bestpractice also demands that the neu-rological evaluation include consid-eration of clinical state, concurrentinjury, and drug therapy. A neuro-logical evaluation compromised bydepression of consciousness or con-current drug therapy should be sup-plemented by neuroimaging165 orneurophysiological (electroenceph -alographic)166,167 evaluation.
Management of IntracranialHypertension
Intracranial pressure is the totalpressure produced within the skullby cerebrospinal fluid, blood, andbrain.153,168-170 In order to maintain sta-ble intracranial pressure, an increasein volume of one component must bebalanced by a decrease in volume ofone or both of the other compo-nents.153,168,169 Selective manipulationof these components is a mainstay oftherapy for intracranial hypertension,and in attempts to improve patients’
outcomes, each component is thesubject of ongoing research.
Modulation of Volume of Cerebrospinal Fluid: Intraventricular Drain
Drainage of cerebrospinal fluidis a hallmark of aggressive manage-ment of intracranial hypertensionand is indicated for sustained eleva-tions of intracranial pressure greaterthan 20 mm Hg.171 Further indica-tions include depressed level of con-sciousness such as a GCS score of 8 orlower.170,172 Drainage of cerebrospinalfluid improves management ofintracranial pressure and cerebralperfusion pressure (CPP) as well asclinical and neurological outcomes,particularly for younger patients inwhom coordinated, mechanism-based management is used, withinterventions tailored more specifi-cally to the underlying pathophysio-logical changes.173 An example isdrainage of cerebrospinal fluid inthe management of hydrocephalusdue to subarachnoid hemorrhage.Drainage of cerebrospinal fluid willremain a mainstay of therapy aftertraumatic brain injury173 and afterother clinical states such as hydro-cephalus after subarachnoid hemor-rhage. Such drainage may havepredictable effects in decreasingintracranial pressure and increasingCPP when done in a controlled,protocol-directed manner.174 Inpatients with intracranial hyperten-sion, initially refractory elevationsof intracranial pressure, drainage ofcerebrospinal fluid was effective andwas associated with improved func-tional outcome and lower mortality6 months after injury.175 Drainage ofcerebrospinal fluid also is not associ-ated with marked risks to other body
systems as is drug-induced coma orhypothermia.176 Available evidencestrongly supports drainage of cere-brospinal fluid as an effective moni-toring and therapeutic technique.
Modulation of Brain Volume:Mannitol and Hypertonic Saline
Modulating brain volume (80%of intracranial volume) is a focusfor aggressive intervention.Osmotherapy with an agent such asmannitol to reduce brain volumeworks by 2 mechanisms. First,agents such as mannitol produce anosmotic gradient that draws waterout from otherwise swollen braintissue. Second, agents such as man-nitol reduce blood viscosity andhematocrit and augment cerebralblood flow.168,170,176-178
Mannitol has been used exten-sively as an osmotic diuretic formany years.168 It can be administeredas a bolus or as an infusion.168,170
Recent studies170,175 suggest earlier useof high-dose mannitol (eg, 1.4 g/kg)may be more effective than standard-dose therapy in improving intracra-nial pressure and outcomes. Bolusdosing of mannitol is generally moreeffective than continuous infusion.168
Limitations of mannitol includehyperosmolality and volume lossfrom osmotic diuresis. Also, withlonger duration such as several daysof therapy, rebound elevation ofintracranial pressure may occur.178
Hypertonic saline, an osmoticagent with a concentration of sodiumchloride that exceeds that of physio-logical saline (0.9%),178,179 has morerecently been studied and used tomanage intracranial hypertension.Concentrations of hypertonic salineused to manage intracranial hyper-tension include 2%, 3%, 5%, 7%,
116 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

7.5%, and 23%.178,179 In addition toreducing intracranial pressure,hypertonic saline augments hemo-dynamic stability179 and intravascu-lar volume.168,170,177 In some studiesand some patients, hypertonicsaline has been more effective thanmannitol for treatment of elevatedintracranial pressure. When manni-tol and hypertonic saline were com-pared in patients who had brainswelling and intracranial hyperten-sion after ischemic stroke, hyper-tonic saline was more effective inreducing intracranial pressure andsupporting CPP.177 Hypertonic salineis also effective in managingintracranial pressure in patientsrefractory to mannitol, includingpatients who have had brain traumaand ischemic stroke.177,178 Optimalconcentration, volume, bolus vsinfusion dosing, and tim-ing/duration of therapy with hyper-tonic saline and targeted clinicalstate have not yet been determined.Hypertonic saline may be mosteffective with patient-specific titration of therapy, includ-ing volume, dosing interval, andconcentration targeted to specificclinical goals, including CPP,intracranial pressure, and othermonitored parameters.
Metabolic Suppression: Therapeutic Hypothermia
Therapeutic hypothermia is thecontrolled depression of body tem-perature to 36ºC or lower.169 Goalsof therapeutic hypothermia includecontrolling refractory elevations ofintracranial pressure and modulat-ing effects of secondary braininjury.169 Multiple factors are associ-ated with secondary brain injury,including release of excitatory neu-
rotransmitters, calcium release,hyperemia, inflammatory response,brain edema, and intracranialhypertension.169,180 Many of theseconsequences are temperaturedependent and potential targets fortherapeutic hypothermia.169,180 Ther-apeutic hypothermia improvesneurological outcomes after cardiacarrest.181,182 Therapeutic hypothermiais also effective in controlling dan-gerous refractory elevations ofintracranial pressure.
In patients with hepatic failure,neurophysiological changes such asbrain edema, cerebral hyperemia,loss of autoregulation, and intracra-nial hypertension are, among others,risk factors for poor clinical and neu-rological outcomes.183 Of particularconcern are elevations in intracranialpressure exceeding 30 to 50 mm Hg,which are associated with severehepatic failure.183,184 Mortality due tointracranial hypertension in patientswith acute liver failure is approxi-mately 20%.184 Mild to moderatetherapeutic hypothermia with coretemperature approximately 32ºC to34ºC is safe and effective for con-trolling elevations in intracranialpressure refractory to other therapiesin the ICU immediately before andduring liver transplantation.183-185
One review186 of multiple stud-ies concluded that therapeutichypothermia after traumatic braininjury was effective in reducingintracranial pressure and may reducerisks of mortality and poor neuro-logical outcome. Multiple aspectsof therapeutic hypothermia havebeen researched, such as durationof therapy. Long-term therapy (5days vs 2 days) was associated withimproved outcomes such as controlof intracranial pressure.187 In chil-
dren, preliminary data from a study188
of 48 patients suggested that thera-peutic hypothermia is most likelysafe, effective for control of intracra-nial pressure, and associated with apotential trend toward improvedfunctional outcomes 3 to 6 monthsafter injury. In a study189 of patientswith severe head injury, patientstreated with hypothermia had signifi-cant higher CPP than did patients inthe normothermic and hyperthermicsubgroups. In another investigation,190
optimal body temperature for reduc-ing intracranial hypertension inpatients with severe brain injury wasbetween 35.0ºC and 35.5ºC.
Therapeutic hypothermia poten-tially can have marked effects onmultiple body systems. Risks includecoagulopathy, cardiovascular insta-bility, and increased risk ofinfection.183,191,192 Optimal use of thera-peutic hypothermia may ultimatelybe best when titrated as a patient-specific and mechanism-based ther-apy to desired core and braintemperature. Best practices for dura-tion of therapy, rate of temperaturedecrease and rewarming, and targettemperature as well as optimal selec-tion of patients are not yet deter-mined. Therapeutic hypothermiamay be used as an option on an indi-vidual basis for refractory intracra-nial hypertension. The currentlyavailable evidence does not supportroutine use of therapeutic hypother-mia after traumatic brain injury.
Modulating Cerebral Blood Volume:Controlled Hyperventilation
Decreasing arterial carbon diox-ide levels via controlled hyperventi-lation has long been used to controlintracranial pressure by reducingcerebral blood flow. Hyperventilation
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 117
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

reduces elevated intracranial pressurebut risks ischemic injury.193 Reductionin intracranial pressure is also tran-sient for a given degree of hypocap-nia.193,194 Because of the risks of brainischemia, particularly during the first24 hours after brain trauma, whencerebral blood flow is already com-promised, prolonged hyperventila-tion (PaCO2 25-30 mm Hg) for morethan a few hours pending optimaluse of definitive therapy for controlof intracranial pressure may causeglobal or localized cerebralischemia.194 Reductions in cerebralblood flow may last longer thanreductions in intracranial pressureduring controlled hyperventila-tion.193 Effects of controlled hypocap-nia in reducing intracranial pressureare well established,194,195 but therisks associated with this treatmentinclude brain ischemia and pooroutcomes. Because of its effects oncerebral hemodynamics, blood flow,and ischemic risk, long-term use ofhyperventilation is not supported bythe available evidence.193-195 The useof hyperventilation in patients withtraumatic brain injury best sup-ported by the evidence is in manage-ment of acute elevations inintracranial pressure pendingaggressive use of definitive thera-pies specific to the cause of the ele-vation,193,194 such as optimal use ofosmotic or metabolic suppressiontherapies. Longer term applicationof hyperventilation may have a role
when cerebral metabolic parameterssuch as brain tissue oxygenation aremonitored, permitting real-timetitration of therapy to a patient-specific metabolic state.194,196
SummaryMany of the studies used to
develop the EBP recommendationsdescribed here were nursing research.Nurses asked questions about prac-tice and, using the scientific process,undertook the challenge to find theanswers. Once evidence is discovered,it is left to nurses at the bedside toimplement the appropriate change.Sometimes the change actuallymakes practice easier. For example,not icing cardiac output solutionwas easy to implement and savednursing time but it took almost adecade before it became commonpractice. It is estimated that 30% to40% of patients do not receive careconsistent with the current scientificevidence.5 In a self-review of use ofEBP in their unit during a 1-yearperiod, IIan et al197 found that theyimplemented their own approvedprotocols only 50% of the time.Ironically, they discovered that itwas the “sickest patients” who wereleast likely to receive commonlyrecommended best practices.Pravikoff et al198 examined nurses’perceptions about readiness forEBP implementation and foundthat, after lack of time, the secondhighest barrier was a “lack of valuefor research in practice.” Larrabee etal199 found that a nurse’s “attitude”about research was a key factor asto whether the nurse was likely tobe supportive of EBP changes. Plostand Nelson200 implemented 9 EBPprotocols in their 35-bed ICU, andafter 3 years, they found that the use
of protocols simplified processes,standardized care, facilitatedpatients’ safety, and reduced costs.
Two major challenges are beforeus. We must continue to answerclinical questions with research,and we must implement the EBPrecommendations that will assist usin providing best practice. As notedby Titler et al,201 “Although educa-tion is necessary to change practice,alone it is not sufficient.” If it tookonly posting an article in the bath-room or a poster in the back roomto change practice, this article wouldnot have been necessary. It will takethe dedication of advanced practiceand bedside nurses to evaluate theirown practice and the needs of theirpatients and a continued vigilanceto ask, Are we doing what is bestfor our patients with the currentevidence available to us?
“The most cost-effective oppor-tunity to improve the quality of carewill not come from discovering newtherapies, but from discoveringhow to deliver therapies that areknown to be effective.”5 CCN
AcknowledgmentsWe thank the American Association of Critical-Care Nurses, Linda Bell, Nancy Munro, and theentire Advance Practice Work Group for theirinsight to pull the group together to present thisinformation at the 2007 National Teaching Insti-tute as an Expert Panel on Evidence-Based Practice.
Financial DisclosuresNone reported.
References1. Nightingale F. Notes on Nursing. Philadel-
phia, PA: JB Lippincott; 1859 (reprint 1992).2. Porter-O’Grady T. Push parameters for-
ward using evidence-based approaches.Nurs Manage. 2007;38(6):58-61.
118 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
eLettersNow that you’ve read the article, create or con-tribute to an online discussion about this topicusing eLetters. Just visit http://ccn.aacnjournals.org and click “Respond to This Article” in eitherthe full-text or PDF view of the article.
To learn more about evidence-based therapy,read “Using Evidence and Process Improve-ment Strategies to Enhance Healthcare Out-comes for the Critically Ill: A Pilot Project,”by Carol W. Hatler et al in the AmericanJournal of Critical Care, 2006;15(5):549-555.Available online at www.ajcconline.org.
d•t
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

3. Committee on Health Professions Educa-tion Summit. Greiner AC, Knebel E, eds.Health Professions Education: A Bridge toQuality. Washington, DC: National Acade-mies Press; 2003. Quality Chasm Series.
4. Bucknall T. A gaze through the lens of deci-sion theory toward knowledge translationscience. Nurs Res. 2007;56(4 suppl):560-566.
5. Spies CD, Bosse G, Breuer JP, Schröder T,Kersten R. Overcoming barriers to guide-line implementation. Crit Connections. April2007. http://www.sccm.org/Publications/Critical_Connections/Archives/April_2007/Pages/Overcoming_Barriers.aspx. AccessedJanuary 30, 2008.
6. Shojania KG, Duncan BW, McDonald KM,et al, eds. Making Health Care Safer: A Criti-cal Analysis of Patient Safety Practices. Evi-dence Report/Technology Assessment No.43. (Prepared by the University of Califor-nia at San Francisco–Stanford Evidence-based Practice Center under Contract No.290-97-0013), Rockville, MD: Agency forHealthcare Research and Quality; July 2001.AHRQ publication 01-E058.
7. Sole ML, Byers JF, Ludy J, Zhang Y, BantaCM, Brummel K. A multisite survey of suc-tioning techniques and airway managementpractices. Am J Crit Care. 2003;12:220-232.
8. Ackerman MH, Mick DJ. Instillation of nor-mal saline before suctioning in patientswith pulmonary infections: a prospectiverandomized controlled trial. Am J Crit Care.1998;7:261-266.
9. Ackerman MH, Gugerty B. The effect ofnormal saline bolus instillation in artificialairways. J Soc Otorhinolaryngol Head NeckNurs. Spring 1990:14-17.
10. Ackerman M. The effect of saline lavageprior to suctioning. Am J Crit Care. 1993;2:326-330.
11. Akgul S, Akyolcu N. Effects of normalsaline on endotracheal suctioning. J ClinNurs. 2002;11(6):826-830.
12. Bostick J, Wendelgass S. Normal salineinstillation as part of the suctioning proce-dure: effects on PaO2 and amount of secre-tions. Heart Lung. 1986;16:532-537.
13. Ridling D, Martin L, Bratton S. Endotrachealsuctioning with or without instillation ofisotonic sodium chloride solution in criti-cally ill children. Am J Crit Care. 2003:12:212-219.
14. Kinloch D. Instillation of normal saline dur-ing endotracheal suctioning: effects onmixed venous oxygen saturation. Am J CritCare. 1999;8:231-240.
15. Gray J, MacIntyre N, Kronenberger W. Theeffects of bolus normal-saline instillation inconjunction with endotracheal suctioning.Respir Care. 1990;35:785-790.
16. Reynolds P, Hoffman L, Schlichtig R,Davies P, Zullo T. Effects of normal salineinstillation on secretion volume, dynamiccompliance and oxygen saturation[abstract]. Am Rev Respir Dis. 1990;141:42(suppl):A574.
17. Steuer JD, Stone KS, Nickel J, Steinfeld Y.Methodologic issues associated with secre-tion weight as a dependent variable inresearch using closed-system suctioncatheters. Nurs Res. 2000;49:295-299.
18. Burton G, Hodgkin J, Wark J. RespiratoryCare: A Guide to Clinical Practice. 4th ed.Philadelphia, PA: JB Lippincott; 1997.
19. Blackwell B. Normal saline instillation withendotracheal suctioning: primum non
nocere (first do no harm). J Adv Nurs. 1999;29:928-934.
20. Ackerman MH, Ecklund MM, Abu-JumahM. A review of normal saline instillation:implications for practice. Dimens Crit CareNurs. 1996;15(1):31-38.
21. Demlers R, Saklad M. Mimimizing theharmful effects of mechanical aspiration.Heart Lung. 1975;2:542-545.
22. Chulay M. Why do we keep putting salinedown endotracheal tubes? It’s time for achange in the way we suction! CapsulesComments. 1994;2(4):7-11.
23. Rutula W, Stiegel M, Sarubbi F. A potentialinfection hazard associated with the of dis-posable saline vials. Infect Control. 1984;5:170-172.
24. Hagler D, Traver G. Dislodgement of bacteriafrom endotracheal tubes by saline and suc-tion catheter. Am J Crit Care. 1993;2(3):261
25. Labarca J, Trick W, Peterson C, et al. A mul-tistate nosocomial outbreak of Ralstoniapickettii colonization associated with anintrinsically contaminated respiratory caresolution. Clin Infect Dis. 1999;29:1281-1286.
26. McNeil MM, Solomon SL, Anderson RL, etal. Nosocomial Pseudomonas pickettii colo-nization associated with a contaminatedrespiratory therapy solution in a specialcare nursery. J Clin Microbiol. 1985;22(6):903-907.
27. Schwenker D, Ferrin M, Gift A. A survey ofendotracheal suctioning with instillation ofnormal saline. Am J Crit Care. 1998;7:255-260.
28. Swartz K, Noonan D, Edwards-Beckett J. Anational survey of endotracheal suctioningtechniques in the pediatric population.Heart Lung. 1996;25:52-60.
29. Sole ML, Byers JF, Ludy J, Zhang Y, OsttrowCL. Suctioning techniques and airway man-agement practices: pilot study and instru-ment evaluation. Am J Crit Care. 2002;11:363-368.
30. Raymond S. Normal saline instillationbefore suctioning: helpful or harmful? Areview of the literature. Am J Crit Care.1995;2(6):467-473.
31. Celik SA, Kanan N. A current conflict: use ofisotonic sodium chloride solution on endo-tracheal suctioning in critically ill patients.Dimens Crit Care Nurs. 2006;25(1): 11-14.
32. St John R, Seckel M. Airway management.In: Burns S, ed. Care of Mechanically Venti-lated Patients. 2nd ed. Sudbury, MA: Jones& Bartlett; 2007:3-40.
33. St John R. Airway and ventilatory manage-ment. In: Chulay M, Burns S, eds. AACNEssentials of Critical Care Nursing. New York,NY: McGraw-Hill Inc; 2006:111-144.
34. Chulay M. Suctioning: endotracheal or tra-cheostomy tube. In: Carlson K, Wiegand D,eds. AACN Procedure Manual for CriticalCare. 5th ed. Philadelphia, PA: Elsevier;2005:62-70.
35. Lipman T, Kessler T, Arabian A. Nasopul-monary intubation with feeding tubes: casereports and review of the literature. J Par-enter Enteral Nutr. 1985;9:618-620.
36. Metheny NA, Meert KL, Clouse RE. Com-plications related to feeding tube placement.Curr Opin Gastroenterol. 2007;23(2):178-182.
37. Kindropp AS, Drover JW, Heyland DK.Capnography confirms correct feeding tubeplacement in intensive care unit patients.Can J Anaesth. 2001;48(7):705-710.
38. Burns SM, Carpenter R, Truitt JD. Reporton the development of a procedure to pre-
vent placement of feeding tubes into thelungs using end-tidal CO2 measurements.Crit Care Med. 2001;29:936-939.
39. Metheny N, McSweeney M, Wehrle MA,Wiersema L. Effectiveness of the ausculta-tory method in predicting feeding tubelocation. Nurs Res. 1990;39:262-267.
40. Metheny N. Titler, M. Assessing placement offeeding tubes. Am J Nurs. 2001;101(5):36-45.
41. Metheny N, Reed L, Wiersema L, et al.Effectiveness of pH measurements in pre-dicting feeding tube placement: an update.Nurs Res. 1993;42:324-331.
42. Metheny N, Stewart B, Smith L, et al. pHand concentration of bilirubin in feedingtube aspirates as predictors of tube place-ment. Nurs Res. 1999;25:318-323.
43. Metheny N. Preventing respiratory compli-cations of tube feedings: evidence-basedpractice. Am J Crit Care. 2006;15:360-369.
44. McClave SA, DeMeo MT, DeLegge MH, etal. North American Summit on Aspirationin the Critically Ill Patient: consensus state-ment. J Parenter Enteral Nutr. 2002;26(suppl):S80-S85.
45. Practice alert: verification of feeding tubeplacement. American Association of Critical-Care Nurses Web site. http://www.aacn.org/AACN/practiceAlert.nsf/Files/DEF/$file/Dye%20in%20Enteral%20Feeding%204-2005.pdf. Accessed January 20, 2008.
46. Metheny N, Reed L, Berglund B, Wehrle M.Visual characteristics of aspirates fromfeeding tubes as a method of predictingtube location. Nurs Res. 1994;43:282-287.
47. D’Souza C, Kilam S, D’Souza U, et al. Pul-monary complications of feeding tubes: anew technique of insertion and monitoringmalposition. Can J Surg. 1994;37:404-408.
48. Thomas B, Falcone R. Confirmation ofnasogastric tube placement by colorimetricdetection of carbon dioxide: a preliminaryreport. J Am Coll Nutr. 2001;17:195-197.
49. Araujo-Preza C, Melhado M, Gutierrez F,Maniatis T, Casellano M. Use of capnome-try to verify feeding tube placement. Crit CareMed. 2002;30:2255-2259
50. Burns SM, Carpenter R, Blevins C, et al.Detection of inadvertent airway intubationduring gastric tube insertion: capnographyversus a colorimetric carbon dioxide detec-tor. Am J Crit Care. 2006;15:188-195.
51. Elpern E, Killeen K, Talla E, Perez G, GurkaD. Capnometry and air insufflation forassessing initial placement of gastric tubes.Am J Crit Care. 2007;16:544-549.
52. Marderstein EL, Simmons RL, Ochoa JB.Patient safety: effect of institutional proto-cols on adverse events related to feedingtube placement in the critically ill. J Am CollSurg. 2004;199(1):39-47.
53. Bourgault AM, Ipe L, Weaver J, Swartz S,O’Dea P. Development of evidence-basedguidelines and critical care nurses’ knowl-edge of enteral feedings. Crit Care Nurse.2007;27(4):17-29.
54. Pickering TG, Hall JE, Appel LJ, et al. Rec-ommendations for blood pressure measure-ment in humans and experimental animals,I: blood pressure measurement in humans.A statement for professionals from the Sub-committee of Professional and Public Edu-cation of the American Heart AssociationCouncil on High Blood Pressure Research.Circulation. 2005;111(5):697-716.
55. Practice alert: noninvasive blood pressuremonitoring. American Association of Criti-
120 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

cal-Care Nurses Web site. http://www.aacn.org/AACN/practiceAlert.nsf/vwdoc/pa2. Issued May 11, 2006. Revised June2006. Accessed January 30, 2008.
56. Bur A, Herkner H, Vlcek M, et al. Factorsinfluencing the accuracy of oscillometricblood pressure measurement in critically illpatients. Crit Care Med. 2003;31:793-799.
57. Kirchoff K, Rebenson-Piano M, Patel M.Mean arterial pressure readings: variationswith positions and transducer level. NursRes. 1984;33:343-345.
58. McCann U, Schiller H, Carney D, et al.Proper transducer level for arterial bloodpressure measurement [abstract]. Chest.1999;116(suppl):281S.
59. Netea RT, Bijlstra PJ, Lenders JW, et al.Influence of the arm position on intra-arte-rial blood pressure measurement. J HumHypertens. 1998;12:157-160.
60. Pickering TG. Blood pressure variability andambulatory monitoring. Curr Opin NephrolHypertens. 1993;2:380-385.
61. Netea RT, Lenders JW, Smits P, et al. Armposition is important for blood pressuremeasurement. J Hum Hypertens. 1999;13:105-109.
62. Netea RT, Elving LD, Lutterman JA, et al.Body position and blood pressure measure-ment in patients with diabetes mellitus. J Intern Med. 2002;251:393-399.
63. Adiyaman A, Verhoeff R, Lenders JW, et al.The position of the arm during blood pres-sure measurement in sitting position. BloodPress Monit. 2006;11:309-313.
64. Mourad A, Carney S, Gillies A, et al. Armposition and blood pressure: a risk factorfor hypertension? J Hum Hypertens. 2003;17:389-395.
65. Familoni OB, Olunuga TO. Comparison ofthe effects of arm position and support onblood pressure in hypertensive and nor-motensive subjects. Cardiovasc J S Afr. 2005;16(2):85-8.
66. Netea RT, Lenders JW, Smits P, et al. Bothbody and arm position significantly influ-ence blood pressure measurement. J HumHypertens. 2003;17:459-462.
67. Newton KM. Comparison of aortic andbrachial cuff pressures in flat supine and lat-eral recumbent positions. Heart Lung. 1981;10:821-826.
68. van der Steen MS, Pleijers AM, Lenders JW,Thien T. Influence of different supine bodypositions on blood pressure: consequencesfor night blood pressure/dipper-status. J Hypertens. 2000;18(12):1731-1736.
69. Cavelaars M, Tulen JH, Man ‘t Veld AJ,Gelsema ES, van den Meiracker AH. Assess-ment of body position to quantify its effecton nocturnal blood pressure under ambula-tory conditions. J Hypertens. 2000;18(12):1737-1743.
70. Schell K, Bradley E, Bucher L, et al. Clinicalcomparison of automatic, noninvasivemeasurements of blood pressure in the fore-arm and upper arm. Am J Crit Care. 2005;14(5):232-241.
71. Singer AJ, Kahn SR, Thode HC Jr, et al.Comparison of forearm and upper armblood pressures. Prehosp Emerg Care. 1999;3:123-126.
72. Schell K, Lyons D, Bradley E, et al. Clinicalcomparison of automatic, noninvasivemeasurements of blood pressure in the fore-arm and upper arm with the patient supineor with the head of the bed raised 45
degrees: a follow-up study. Am J Crit Care.2006;15:196-205.
73. Umana E, Ahmed W, Fraley MA, AlpertMA. Comparison of oscillometric andintraarterial systolic and diastolic bloodpressures in lean, overweight, and obesepatients. Angiology. 2006;57(1):41-45.
74. Pierin AM, Alavarce DC, Gusmao JL, et al.Blood pressure measurement in obesepatients: comparison between upper armand forearm measurements. Blood PressMonit. 2004;9:101-105.
75. Fonseca-Reyes S, De Alba-Garcia JG, Parra-Carrillo JZ, et al. Effect of standard cuff onblood pressure readings in patients withobese arms: how frequent are arms of a“large circumference”? Blood Press Monit.2003;8(3):101-106.
76. Jani B, Bulpitt CJ, Rajkumar C. Blood pres-sure measurement in patients with ratecontrolled atrial fibrillation using mercurysphygmomanometer and Omron HEM-750CP device in the clinic setting. J HumHypertens. 2006;20:543-545.
77. Stewart MJ, Gough K, Padfield PL. Theaccuracy of automated blood pressure meas-uring devices in patients with controlledatrial fibrillation. J Hypertens. 1995;13(3):297-300.
78. Pauca AL, Wallenhaupt SL, Kon ND,Tucker WY. Does radial artery pressureaccurately reflect aortic pressure? Chest.1992;102(4): 1193-1198.
79. Fournier A, Safar M. Accurate measure-ment of blood pressure [letter]. JAMA.2003; 289(21):2793-2794.
80. Pauca AL, Kon ND, O’Rourke MF. The sec-ond peak of the radial artery pressure waverepresents aortic systolic pressure in hyper-tensive and elderly patients. Br J Anaesth.2004;92:651-657.
81. Dorman T, Breslow MJ, Lipsett PA, et al.Radial artery pressure monitoring underes-timates central arterial pressure duringvasopressor therapy in critically ill surgicalpatients. Crit Care Med. 1998;26:1646-1649.
82. Mignini MA, Piacentini E, Dubin A. Periph-eral arterial blood pressure monitoring ade-quately tracks central arterial bloodpressure in critically ill patients: an obser-vational study. Crit Care. 2006;10:R43.
83. Pytte M, Dybwik K, Sexton J, et al. Oscillo-metric brachial mean artery pressures arehigher than intra-radial mean artery pres-sures in intensive care unit patients receiv-ing norepinephrine. Acta AnaesthesiolScand. 2006;50:718-721.
84. Urzua J, Sessler DI, Meneses G, et al. Ther-moregulatory vasoconstriction increasesthe difference between femoral and radialarterial pressures. J Clin Monit. 1994;10:229-236.
85. Yazigi A. Blood pressure measurements inthe radial and femoral artery [letter]. ActaAnaesth Scand. 2002;46:1176-1178.
86. Soderstrom S, Sellgren J, Ponten J. Aorticand radial pulse contour: different effects ofnitroglycerin and prostacyclin. AnesthAnalg. 1999;89:566-572.
87. Gore S, Middleton R, Bridges E. Analysis ofan algorithm to guide decision makingregarding direct and oscillometric bloodpressure measurement [abstract]. Am JRespir Crit Care Med. 1995;151:A331.
88. Bridges E, Evers KG, Schmelz J, et al. Inva-sive pressure monitoring at altitude[abstract]. Crit Care Med. 2005;33:A13.
89. Promonet C, Anglade D, Menaouar A, etal. Time-dependent pressure distortion ina catheter-transducer system: correctionby fast flush. Anesthesiology. 2000;92:208-218.
90. Bridges ME, Middleton R. Direct arterial vsoscillometric monitoring of blood pres-sure: stop comparing and pick one (a deci-sion-making algorithm). Crit Care Nurse.1997; 17(3):58-66, 68-72.
91. Drew BJ, Scheinman MM. Value of electro-cardiographic leads MCL1, MCL6 andother selected leads in the diagnosis ofwide QRS complex tachycardia. J Am CollCardiol. 1991;18(4):1025-1033.
92. Drew BJ, Scheinman MM, Dracup K.MCL1 and MCL6 compared to V1 and V6in distinguishing aberrant supraventricularfrom ventricular ectopic beats. Pacing ClinElectrophysiol. 1991;14:1375-1383.
93. Drew BJ, Scheinman MM. ECG criteria todistinguish between aberrantly conductedsupraventricular tachycardia and ventricu-lar tachycardia: practical aspects for theimmediate care setting. Pacing Clin Electro-physiol. 1995;18:2194-2208.
94. Drew BJ, Wung SF, Adams MG, et al. Bed-side diagnosis of myocardial ischemia withST-segment monitoring technology: meas-urement issues for real-time clinical deci-sion making and trial designs. J Electro - cardiol. 1997;30(suppl):157-165.
95. Drew BJ, Califf RM, Funk M, et al. AHAscientific statement: practice standards forelectrocardiographic monitoring in hospi-tal settings. An American Heart Associa-tion Scientific Statement from the Councilson Cardiovascular Nursing, Clinical Cardi-ology, and Cardiovascular Disease in theYoung: endorsed by the International Soci-ety of Computerized Electrocardiology andthe American Association of Critical-CareNurses. J Cardiovasc Nurs. 2005;20:76-106.
96. Kern L, McRae M, Funk M. ECG monitor-ing after cardiac surgery. AACN Adv CritCare. 2007;18:294-304.
97. Drew BJ, Krucoff MW. Multilead ST-seg-ment monitoring in patients with acutecoronary syndromes: a consensus state-ment for healthcare professionals. ST-Seg-ment Monitoring Practice GuidelineInternational Working Group. Am J CritCare. 1999;8:372-388.
98. Drew BJ, Tisdale LA. ST-segment monitor-ing for coronary artery reocclusion follow-ing thrombolytic therapy and coronaryangioplasty: identification of optimal bed-side monitoring leads. Am J Crit Care. 1993;2:280-292.
99. Drew BJ, Adams MG, Pelter MM, et al. ST-segment monitoring with a derived 12-leadelectrocardiogram is superior to routinecardiac care unit monitoring. Am J CritCare. 1996;5:198-206.
100. Drew BJ, Pelter MM, Adams MG, WungSF, Chou TM, Wolfe CL. 12-Lead ST-seg-ment monitoring vs single-lead maximumST-segment monitoring for detectingongoing ischemia in patients with unsta-ble coronary syndromes. Am J Crit Care.1998; 7(5):355-363.
101. Krucoff MW, Parente AR, Bottner RK, etal. Stability of multilead ST-segment “fin-gerprints” over time after percutaneoustransluminal coronary angioplasty and itsusefulness in detecting reocclusion. Am JCardiol. 1988;61:1232-1237.
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 121
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

102. Klootwijk P, Meij S, von Es GA, et al. Com-parison of usefulness of computer assistedcontinuous 48-h 3-lead with 12-lead ECGischaemia monitoring for detection and quan-titation of ischaemia in patients with unstableangina. Eur Heart J. 1997;18:931-940.
103. Anderson ME, Al-Khatib SM, Roden DM,et al. Cardiac repolarization: current knowl-edge, critical gaps, and new approaches todrug development and patient manage-ment. Am Heart J. 2002;144:769-781.
104. Al-Khatib SM, LaPointe NM, Kramer JM, etal. What clinicians should know about theQT interval. JAMA. 2003;289:2120-2127.
105. Bazett H. An analysis of time-relation ofelectrocardiogram. Heart. 1920;7:353-357.
106. Malik M. Errors and misconceptions inECG measurement used for the detection ofdrug induced QT interval prolongation. JElectrocardiol. 2004;37(suppl):25-33.
107. Sadanaga T, Sadanaga F, Yao H, et al. Heartrate dependent modification of the QTccut-off values can improve accurate evalua-tion of QT prolongation. Am J Cardiol.2004;93:772-775.
108. Drew BJ, Funk M. Practice standards forECG monitoring in hospital settings: execu-tive summary and guide for implementa-tion. Crit Care Nurs Clin North Am. 2006;18:157-168, ix.
109. Rimmer LK, Rimmer JD. Comparison of 2methods of measuring the QT interval. AmJ Crit Care. 1998;7:346-354.
110. Cowan JC, Yusoff K, Moore M, et al. Impor-tance of lead selection in QT interval meas-urement. Am J Cardiol. 1988;61:83-87.
111. Sadanaga T, Sadanaga F, Yao H, FujishimaM. An evaluation of ECG leads used toassess QT prolongation. Cardiology.2006;105(3):149-154.
112. Kligfield P, Gettes LS, Bailey JJ, et al. Rec-ommendations for the standardization andinterpretation of the electrocardiogram, I:the electrocardiogram and its technology—a scientific statement from the AmericanHeart Association Electrocardiography andArrhythmias Committee, Council on Clini-cal Cardiology; the American College ofCardiology Foundation; and the HeartRhythm Society: endorsed by the Interna-tional Society for Computerized Electrocar-diology. Circulation. 2007;115:1306-1324.
113. Wenger W, Kligfield P. Variability of precor-dial electrode placement during routineelectrocardiography. J Electrocardiol. 1996;29:179-184.
114. Bupp JE, Dinger M, Lawrence C, et al.Placement of cardiac electrodes: written,simulated, and actual accuracy. Am J CritCare. 1997;6:457-462.
115. Rudiger A, Schob L, Follath F. Influence ofelectrode misplacement on the electrocar-diographic signs of inferior myocardialischemia. Am J Emerg Med. 2003;21:574-577.
116. MacAlpin RN. Clinical significance of QScomplexes in V1 and V2 without other elec-trocardiographic abnormality. Ann Nonin-vasive Electrocardiol. 2004;9:39-47.
117. Asher RAJ. The dangers of going to bed. BrMed J. 1947;4:967.
118. Krishnagopalan S, Johnson W, Low LL,Kaufman LJ. Body position of intensive carepatients: clinical practice versus standards.Crit Care Med. 2002;30:2588-2592.
119. Guideline for the Prevention of HealthcareAssociated Pneumonia, 2004. Centers forDisease Control and Prevention, Healthcare
Infection Control Practices Advisory Com-mittee. Atlanta, GA: Centers for DiseaseControl and Prevention; 2004
120. Rubin M. The physiology of bedrest. Am JNurs. 1988;88(1):50-58.
121. Herridge MS, Cheung AM, Tansey CM.One-year outcomes in survivors of the acuterespiratory distress syndrome. N Engl JMed. 2003;348(8):683-693.
122. Kollef MH. Ventilator-associated pneumo-nia: a multivariate analysis. JAMA. 1993;270(16):1965-1970.
123. Anzueto A, Peter JI, Seidner SR. Effects ofcontinuous bed rotation and prolongedmechanical ventilation on healthy, adultbaboons. Crit Care Med. 1997;25(9):1560-1564.
124. Zack MB, Pontoppidan H, Kazemi H. Theeffects of lateral positions on gas exchangein pulmonary disease. Am Rev Respir Dis.1974;110(1):49-55.
125. Ibanez J, Raurich JM, Abizanda R, Clara-monte R, Ibanez P, Bergada J. The effect oflateral positions on gas exchange in patientswith unilateral lung disease during mechani-cal ventilation. Intensive Care Med. 1981;7:231-234.
126. Remolina C, Khan AU, Santiago TV, EdelmanNH. Positional hypozemia in unilateral lungdisease. N Engl J Med. 1981;304(9): 523-525.
127. Kaneko K, Milic-Emili J, Dolovich MB, Daw-son A, Bates DV. Regional distribution of ven-tilation and perfusion as a function of bodyposition. J Appl Physiol. 1966;21:767-777.
128. Ray JF, Ost L, Moallem S, Sanoudos GM, etal. Immobility, hypoxemia and pulmonaryarteriovenous shunting. Arch Surg. 1974;109:537-541.
129. Choi SC, Nelson LD. Kinetic therapy in crit-ically ill patients: combined results basedon meta-analysis. J Crit Care. 1992;7:57-62.
130. deBoisblanc BP, Castro M, Everret B, et al.Effect of air-supported, continuous, pos-tural oscillation on the risk of early ICUpneumonia in nontraumatic critical illness.Chest. 1993;103:1543-1547.
131. Fink MP, Helsmoortel CM, Stein KL, LeePC, Cohn SM. The efficacy of an oscillatingbed in the prevention of lower respiratorytract infection in critically ill victims ofblunt trauma: a prospective study. Chest.1990;97:132-137.
132. Gentilello L, Thompson DA, Tonnesen AS,et al. Effect of a rotating bed on the incidenceof pulmonary complications in critically illpatients. Crit Care Med. 1988;16:783-786.
133. Kelley RE, Vibulsresth S, Bell L, Duncan RC.Evaluation of kinetic therapy in the preven-tion of complications of prolonged bed restsecondary to stroke. Stroke. 1987;18:638-642.
134. Ahrens T, Kollef M, Stewart J, Shannon W.Effect of kinetic therapy on pulmonary com-plications. Am J Crit Care. 2004;13:376-383.
135. Summer WR, Curry P, Haponik EF, NelsonS, Elston R. Continuous mechanical turningof intensive care unit patients shortenslength of stay in some diagnostic-relatedgroups. J Crit Care. 1989;4:45-53.
136. Marik PE, Fink MP. One good turn deservesanother [editorial]! Crit Care Med. 2002;30(9):2146-2148.
137. Hess DR. Patient positioning and ventila-tor-associated pneumonia. Respir Care.2005;50(7):892-898.
138. Goldhill DR, Imhoff M, McLean B, Wald-mann C. Rotational bed therapy to preventand treat respiratory complications: a review
and meta-analysis. Am J Crit Care. 2007;16(1):50-62.
139. Demarest GB, Schmidt-Nowara W, Vance LW,Altman AR. Use of the kinetic treatment tableto prevent the pulmonary complications ofmultiple trauma. West J Med. 1989;150:35-38.
140. Kirschenbaum L, Azzi E, Sfeir T, Tietjen P,Astiz M. Effect of continuous lateral rota-tional therapy on the prevalence of ventila-tor-associated pneumonia in patientsrequiring long-term ventilatory care. CritCare Med. 2002;30:1983-1986.
141. Traver GA, Tyler ML, Hudson LD, SherrillDL, Quan SF. Continuous oscillation: out-come in critically ill patients. J Crit Care.1995;10:97-103.
142. Whiteman K, Nachtmann L, Kramer D,Sereika S, Bierman M. Effects of continuouslateral rotation therapy on pulmonary com-plications in liver transplant patients. Am JCrit Care. 1995;4:133-139.
143. Curley MAQ. Prone positioning of patientswith acute respiratory distress syndrome: asystematic review. Am J Crit Care. 1999;8(6):397-405.
144. Pelosi P, Brazzi L, Gattinoni L. Prone positionin ARDS. Eur Respir J. 2002;20:1017-1028.
145. Vollman KM. Prone positioning in thepatient with acute respiratory distress syn-drome: the art and science. Crit Care NursClin North Am. 2004;16:319-336.
146. Gattinoni L, Tognoni G, Pesenti A, TacconeP, Mascheroni D, Labarta V. Effect of pronepositioning on the survival of patients withacute respiratory failure. N Engl J Med.2001;345:568-573.
147. Guerin C, Gaillard S, Lemasson S, et al.Effects of systemic prone positioning inhypoxic acute respiratory failure: a random-ized controlled trial. JAMA. 2004;292(19):2379-2387.
148. Marini JJ, Rubenfeld G. Pro/con clinicaldebate: the use of prone positioning in themanagement of patients with acute respira-tory distress syndrome. Crit Care Forum.2002;6:15-17.
149. The Acute Respiratory Distress SyndromeNetwork. Ventilation with lower tidal vol-umes as compared with traditional tidalvolumes for acute lung injury and the acuterespiratory distress syndrome. N Engl JMed. 2000;342(181):1301-1308.
150. Ahrens T, Burns S, Phillips J, Vollman K,Whitman J. Progressive mobility guidelinesfor critically ill patients. Advancing NursingLLC; 2005. http://www.vollman.com/pdf/SugGdlns.pdf. Accessed January 30, 2008.
151. Bailey P, Thomsen GE, Spuhler VJ, et al.Early activity is feasible and safe in respira-tory failure patients. Crit Care Med. 2007;35:139-145.
152. Tracey M. Mobility protocol: nursing standardof care. Crit Care Nurse. 2004;24(4):87-88.
153. Arbour R. Intracranial hypertension: moni-toring and nursing assessment. Crit CareNurse. 2004;24(5):19-20, 22-26, 28-32.
154. Hickey JV. The Clinical Practice of Neurologi-cal and Neurosurgical Nursing. 4th ed.Philadelphia, PA: Lippincott Williams &Wilkins; 2002.
155. Teasdale G, Jennett B. Assessment of comaand consciousness. Lancet. 1974;2:81-84.
156. Sternback GL. The Glasgow Coma Scale. J Emerg Med. 2000;19(1):67-71.
157. Cartlidge N. States related to or confusedwith coma. J Neurol Neurosurg Psychiatry.2001;71(suppl 1):i18-i19.
122 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

158. Edwards SL. Using the Glasgow Coma Scale:analysis and limitations. Br J Nurs. 2001;10:92-101.
159. Heard K, Bebarta VS. Reliability of the Glas-gow Coma Scale for the emergency depart-ment evaluation of poisoned patients. HumExp Toxicol. 2004;23(4):197-200.
160. Tien HC, Cunha JRF, Wu SN, et al. Dotrauma patients with a Glasgow Coma Scalescore of 3 and bilateral fixed and dilatedpupils have any chance of survival? JTrauma. 2006;60(2):274-278.
161. Davis DP, Serrano JA, Vilke GM, et al. Thepredictive value of field versus arrival Glas-gow Coma Scale score and TRISS calcula-tions in moderate-to-severe traumatic braininjury. J Trauma. 2006;60(5):985-990.
162. Lieberman JD, Pasquale MD, Garcia R,Cipolle MD, Mark Li P, Wasser TE. Use ofadmission Glasgow Coma Score, pupil sizeand pupil reactivity to determine outcomefor trauma patients. J Trauma. 2003;55(3):437-443.
163. Wijdicks EFM, Bamlet WR, MaramattomBV, Manno EM, McClelland RL. Validationof a new coma scale: the FOUR score. AnnNeurol. 2005;58:585-593.
164. Wolf CA, Wijdicks EFM, Bamlet WR,McClelland RL. Further validation of theFOUR Score coma scale by intensive carenurses. Mayo Clin Proc. 2007;82:435-438.
165. Stevens RD, Bhardwaj A. Approach to thecomatose patient. Crit Care Med. 2005;34(1):31-41.
166. Young GB. The EEG in coma. J Clin Neuro-physiol. 2000;17(5):473-485.
167. Arbour R. Continuous nervous system mon-itoring: EEG, the bispectral index and neu-romuscular transmission. AACN Adv CritCare. 2003;14(2):185-207.
168. Marcous KK. Management of increasedintracranial pressure in the critically ill childwith an acute neurological injury. AACNClin Issues. 2005;16:212-231.
169. Wright JE. Therapeutic hypothermia intraumatic brain injury. Crit Care Nurs Q.2005;28:150-161.
170. Vincent JL, Berré J. Primer on medical man-agement of severe brain injury [publishedcorrection appears in Crit Care Med.2005;33(9):2157]. Crit Care Med. 2005;33(6):1392-1399.
171. Albano C, Comadante L, Nolan S. Innova-tions in the management of cerebral injury.Crit Care Nurs Q. 2005;28:135-149.
172. The Brain Trauma Foundation. The Ameri-can Association of Neurological Surgeons.The Joint Section on Neurotrauma and Crit-ical Care. Recommendations for intracranialpressure monitoring technology. J Neuro-trauma. 2000;17:497-506.
173. Shore PM, Thomas NJ, Clark RS. Continu-ous versus intermittent cerebrospinal fluiddrainage after severe traumatic brain injuryin children: effect on biochemical markers. JNeurotrauma. 2004;21:1113-1122.
174. Kerr ME, Weber BE, Sereika SM, WilbergerJ, Marion DW. Dose response to cere-brospinal fluid drainage on cerebral perfu-sion in traumatic brain-injured adults.Neurosurg Focus. 2001;11:1-7.
175. Abadal-Centellas JM, Liompart-Pou JA,Homar-Ramirez J, et al. Neurologic outcomeof posttraumatic refractory intracranialhypertension treated with external lumbardrainage. J Trauma. 2007;62:282-286.
176. Helmy A, Vizcaychipi M, Gupta AK. Trau-
matic brain injury: intensive care manage-ment. Br J Anaesth. 2007;99(1):32-42.
177. Rasian A, Bhardwag A. Medical manage-ment of cerebral edema. Neurosurg Focus.2007;22(5):E12.
178. White H, Cook D, Venkatesh B. The use ofhypertonic saline for treating intracranialhypertension after traumatic brain injury.Anesth Analg. 2006;102:1836-1846.
179. Mortimer DS, Jancik J. Administering hyper-tonic saline to patients with severe traumaticbrain injury. J Neurosci Nurs. 2006;38:142-146.
180. Sahuquillo J, Vilalta A. Cooling the injuredbrain: how does moderate hypothermia influ-ence the pathophysiology of traumatic braininjury. Curr Pharm Des. 2007;13:2310-2322.
181. Ong MEH, Peberdy MA, Sampson R, OrnatoJP. Controlled therapeutic hypothermia post-cardiac arrest compared with standardintensive care unit therapy [abstract]. AcadEmerg Med. 2006;13(suppl 1):S176.
182. The Hypothermia After Cardiac Arrest StudyGroup. Mild therapeutic hypothermia toimprove the neurologic outcome after car-diac arrest. N Engl J Med. 2002;346:549-556.
183. Vaquero J, Rose C, Butterworth RF. Keepingcool in acute liver failure: rationale for useof mild hypothermia. J Hepatol. 2005;43:1067-1077.
184. Jalan R, Damink SW, Deutz NE, Hayes PC,Lee A. Moderate hypothermia in patientswith acute liver failure and uncontrolledintracranial hypertension. Gastroenterology.2004;127:1338-1346.
185. Jalan R, Olde Damink SW, Deutz NE, et al.Moderate hypothermia prevents cerebralhyperemia and increase in intracranialpressure in patients undergoing liver trans-plantation for acute liver failure. Transplan-tation. 2003;75:2034-2039.
186. McIntyre LA, Fergusson DA, Hebert PC,Moher D, Hutchinson JS. Prolonged thera-peutic hypothermia after traumatic braininjury in adults: a systematic review. JAMA.2003;289:2992-2999.
187. Jiang JY, Xu W, Ga GY, et al. Effect of long-term mild hypothermia or short-term mildhypothermia on outcome of patients withsevere traumatic brain injury. J Cereb BloodFlow Metab. 2006;26:771-776.
188. Adelson PD, Ragheb J, Kanev P, et al. PhaseII clinical trial of moderate hypothermiaafter severe traumatic brain injury in chil-dren. Neurosurgery. 2005;56(4):740-754.
189. Soukup J, Zauner A, Doppenberg EM, et al.The importance of brain temperature inpatients after severe head injury: relation-ship to intracranial pressure, cerebral per-fusion pressure, cerebral blood flow andoutcome. J Neurotrauma. 2002;19:559-571.
190. Tokutomi T, Morimoto K, Miyagi T, Yam-aguchi S, Ishikawa K, Shigemori M. Opti-mal temperature for the management ofsevere traumatic brain injury: effect ofhypothermia on intracranial pressure, sys-temic and intracranial hemodynamics, andmetabolism. Neurosurgery. 2003;52(1):102-111.
191. Vaquero J, Blei AT. Mild hypothermia forcute liver failure: a review of mechanisms ofaction. Clin Gastroenterol. 2005;39(suppl2):s147-s157.
192. Manzarbeitia C. Liver transplantation. http://www.emedicine.com/MED/topic3510.htm.Updated November 1, 2007. Accessed Jan-
uary 30, 2008.193. Robertson C. Every breath you take: hyper-
ventilation and intracranial pressure. CleveClin J Med. 2004;71(suppl 1):S14-S15.
194. Stocchetti N, Maas AIR, Chieregato A, vander Plas AA. Hyperventilation in headinjury: a review. Chest. 2005;127:1812-1827.
195. Steiner LA, Balestreri M, Johnston AJ, et al.Hyperventilation-induced reductions incerebral blood flow velocity outlive thereduction in intracranial pressure in head-injured patients [abstract]. Crit Care. 2003;7(suppl 2):P074.
196. Oertel M, Kelly DF, Lee JH, et al. Efficacy ofhyperventilation, blood pressure elevation,and metabolic suppression therapy in con-trolling intracranial pressure after headinjury. J Neurosurg. 2002;97:1045-1053.
197. IIan R, Fowler R, Geerts R, et al. Knowl-edge translation in critical care: factorsassociated with prescription of commonlyrecommended best practices for critically illpatients. Crit Care Med. 2007;35(7):1696-1702.
198. Pravikoff D, Tanner A, Pierce S. Readinessof US nurses for evidence-based practice:many don’t understand of value researchand have had little or no training to helpthem find evidence on which to base prac-tice. Am J Nurs. 2005;105(9):40-51.
199. Larrabee J, Sions J, Fanning M, WithrowML, Ferretti A. Evaluation of a program toincrease evidence-based practice change. JNurs Adm. 2007;37(6):302-310.
200. Plost G, Nelson DP. Empowering criticalcare nurses to improve compliance withprotocols in the intensive care unit. Am JCrit Care. 2007;16(2):153-156.
201. Titler M, Everett L, Adams S. Implicationsfor implementation science. Nurs Res.2007;56(4):S53-S59.
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 123
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from

124 CRITICALCARENURSE Vol 28, No. 2, APRIL 2008 http://ccn.aacnjournals.org
• Turning critically ill patients every 2 hours may not beenough to preserve the oxygenating ability of the lungsor to prevent healthcare-acquired pneumonia.
• Kinetic and continuous lateral rotation therapy reducesthe risk of ventilator-associated pneumonia in patientsreceiving mechanical ventilation. Optimal benefitdepends on early placement and more than 18 hours of rotation per day.
The Glasgow Coma Scale in Neurological Assessment• For neurological assessment, use the Glasgow Coma Scale in
combination with other evaluation of brain stem reflexes;eye examination, including pupil reactivity and extraocularmovement; vital signs; and evaluation of respiratory rate,depth, and pattern. Neurological evaluation compro-mised by depression of consciousness or concurrent drugtherapy should be supplemented by neuroimaging orneurophysiological (electroencephalographic) evaluation.
Management of Intracranial Hypertension• To manage intracranial hypertension, balance an increase
in the volume of any 1 of the 3 components of totalintracranial pressure (cerebrospinal fluid, blood, brain)by a decrease in the volume of the other 2 components.
• Drainage of cerebrospinal fluid is indicated for sus-tained elevations of intracranial pressure greater than20 mm Hg and in patients with a score of 8 or lower onthe Glasgow Coma Scale.
• In some patients, hypertonic saline is more effectivethan mannitol in treating intracranial hypertension.
• Currently available evidence does not support routine useof therapeutic hypothermia after traumatic brain injury.
• Long-term use of controlled hyperventilation to modulatecerebral blood volume is not supported by the availableevidence.
CCN Fast Facts CRITICALCARENURSEThe journal for high acuity, progressive, and critical care
Rauen CA, Chulay M, Bridges E, Vollman KM, Arbour R. Seven evidence-based practice habits: putting some sacred cows out topasture. Crit Care Nurse. 2008;28(2):98-124.
This article and an online version of the CE test may be found online athttp://ccn.aacnjournals.org.
FactsAccording to estimates, 30% to 40% of patients do
not receive care consistent with current scientific evi-dence. Advanced practice and bedside nurses must eval-uate their own practice and the needs of their patientsand ask, Are we doing what is best for our patients withthe current evidence available to us?
Instillation of Normal Saline Before Endo-tracheal Suctioning: Helpful or Harmful?• Do not instill normal saline (physiological salt solution)
before endotracheal suctioning.
Best Way to Verify Proper Placement ofNasogastric and Pyloric Tubes• Use chest radiography to confirm correct placement ofnasogastric tubes.
Accurate Measurements of Blood Pressure• For accurate noninvasive measurement of blood pressure,
choose the correct size cuff and position the patient’sarm at the level of the heart. Validated evidence-basedalgorithms are available to optimize use of invasive arte-rial pressure monitoring systems.
Selection of Electrocardiographic Leads• Attention to correct placement of electrocardiography
leads is imperative. Wide-complex tachycardia is bestassessed with leads V1 and V6.
Mobility• Match the right time of illness to the right positioning
and mobility strategy.• If a patient experiences consolidated pneumonia in one
lung, positioning with the good lung down will result inbetter oxygenation.
• Progressive mobilization to dangling legs, standing, andwalking is safe for intubated patients.
• Patients breathe better and experience improved oxygena-tion with higher elevations of the head of the bed if theirhemodynamic status is such that they can tolerate theelevation.
Seven Evidence-Based Practice Habits: Putting Some Sacred Cows Out to Pasture
at UNIVERSITY OF IOWA on April 11, 2011ccn.aacnjournals.orgDownloaded from