Embed Size (px)
Citation preview
Severe Proliferative Vitreoretinopathy and Retinal Detachment
II. Surgical Results with Scleral Buckling
AKITOSHI YOSHIDA, MD, PATRICK C. HO, MD,* CHARLES L. SCHEPENS, MD,* J. WALLACE McMEEL, MD, * JOSEPH E. DUNCAN, MD
Abstract: Prior to the era of vitrectomy, scleral buckling was used to treat 521 eyes with total retinal detachment and proliferative vitreoretinopathy (PVR) of various degrees of severity. The retina was reattached for at least six months in 46.9% of eyes; the anatomic success rate decreased with increasing severity of PVR. Within each grade of PVR, the reattachment rate was higher for eyes with smaller breaks than for eyes with larger breaks, and the prognosis was not worse when smaller breaks were found than when no breaks were found. The cumulative success rate rose with increasing number of reoperations. None of the anatomically successful cases had a final visual acuity of no light perception; 82.9% of them achieved a visual acuity of counting fingers or better. The prognosis for visual improvement after successful scleral buckling was unrelated to the preoperative severity of PVR. Severe intraoperative complications occurred in 5.0% of the eyes, all of which resulted in failure. [Key words: proliferative vitreoretinopathy, retinal detachment, scleral buckling.] Ophthalmology 91 : 1538-1543, 1984
Severe proliferative vitreoretinopathy (PVR) is a common cause of failure of retinal detachment surgery. Although closed vitrectomy is now frequently used to treat cases of severe PVR, they can often be managed successfully by scleral buckling techniques alone. This study evaluates the efficacy of scleral buckling in advanced cases of PVR and establishes a basis for comparison with other treatment methods.
MATERIALS AND METHODS
This series comprises 521 eyes in 504 patients with total retinal detachment and PVR of various degrees of
From the Eye Research Institute of Retina Foundation, and Retina Associates,* Boston.
Supported in part by the Massachusetts Lions Eye Research Fund, Inc.
Reprint requests to Library, Eye Research Institute, 20 Staniford St. , Boston, MA 02114.
1538
severity. All eyes were treated with scleral buckling between 1956 and 1966, thus prior to the era of vitrectomy. Eyes with penetrating ocular trauma or diabetic retinopathy were excluded.
Visual acuity testing, measurement of intraocular pressure, slit-lamp examination, and detailed fundus drawing were performed in all cases preoperatively and during the postoperative period. The initial clinical findings have been reported previously. I The operation was considered anatomically successful if the retina was reattached, either throughout the fundus or with narrow, dry retinal folds not extending to the retinal breaks and limited to less than one quadrant, for at least six months after operation. Any retinal redetachment during the follow-up period was considered an anatomic failure. Excluded from the data for anatomic success are some eyes that achieved retinal reattachment but were observed for less than six months postoperatively.
We used the PVR classification proposed by the Retina Society Terminology Committee.2 The grade of PVR was determined retrospectively from the detailed
YOSHIDA. et aI • PVR II
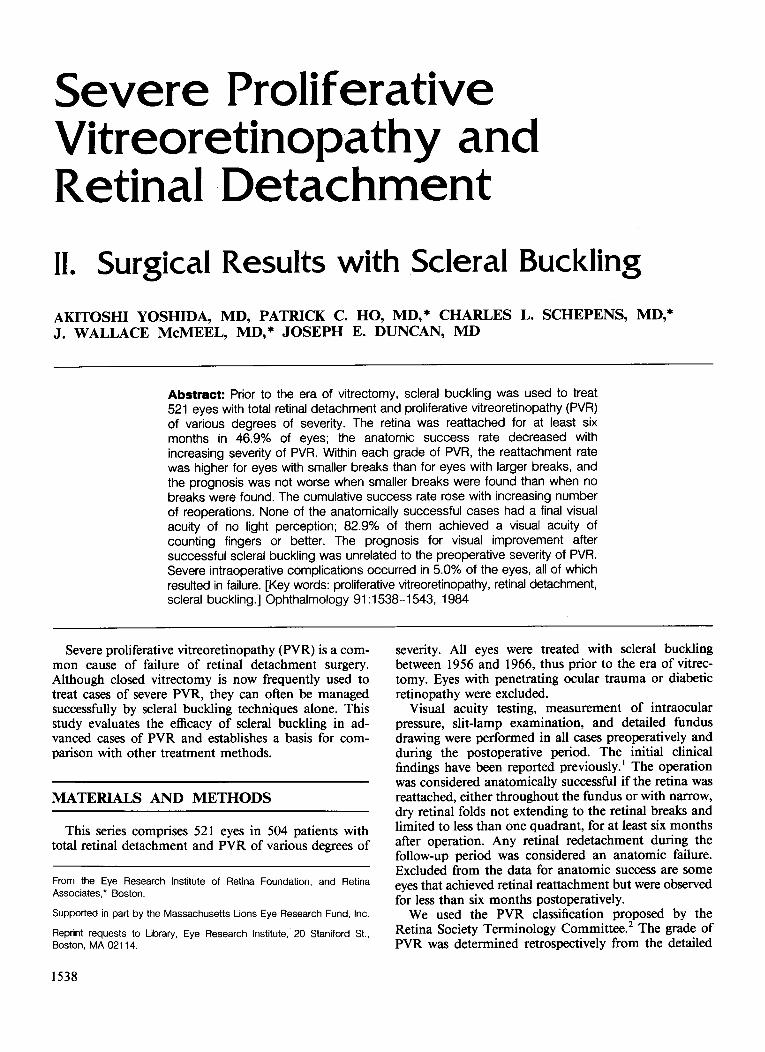
Table 1. Anatomic Success by Grade of Proliferative Vitreoretinopathy (PVR) in Patients Seen Prior to the Era of Vitrectomy
Reattachment with Less Than 6
Months' No. of Eyes Anatomic Successes' Follow-up
Grade Undergoing No. of Anatomic of PVR Scleral Buckling Successes' + Failures No. (%)t No. (%):j:
C-1 3 1 1 (100.0) 2 (66.7) C-2 27 24 21 (87.5) 3 (11.1) C-3 47 36 26 (72.2) 11 (23.4) 0-1 211 166 85 (51.2) 45 (21.3) 0-2 130 108 45 (41.7) 22 (16.9) 0-3 103 89 21 (23.6) 14 (13.6)
Total 521 424 199 (46.9) 97 (18.6)
• With at least 6 months' follow-up. t % equals the no. of anatomic successes divided by the no. of anatomic successes + failures, expressed as a percentage. :j: % equals the no. of reattachments with less than six months' follow-up divided by the no. of eyes undergoing scleral buckling, expressed as a
percentage.
preoperative fundus drawings, but without knowledge of the surgical result. The preoperative fundus drawings were also used to assess the size of the retinal breaks, which was noted in terms of "clock hours" on the retinal circumference. Smaller breaks were defined as smaller than one clock hour; larger breaks, as equal to or larger than one clock hour.
SURGICAL PROCEDURES
The scleral buckling procedure performed at that time has been described previously.3.4 Briefly, a lamellar scleral undermining was created around the localization marks. Diathermy was applied to the thinned scleral bed in a grid pattern. The appropriate implant was placed under the mattress sutures on the scleral flaps. The size of the scleral bed and the choice of implant depended on the width and height of the buckling effect desired. A circling element was placed around the globe. Subretinal fluid was released.
Segmental buckles were used, with a circling element, in 468 eyes (89.8%), and 3600 buckling procedures in 53 eyes (10.2%). Polyethylene was the buckling material in 180 eyes (34.5%), a silicone rubber implant plus circling polyethylene tube in 128 eyes (24.6%), and a circling silicone band over a grooved silicone rubber implant in 213 eyes (40.9%). Intraocular injections were performed in 137 eyes (26.3%): saline in 122 eyes (23.4%), air in 3 eyes (0.6%), silicone oil in 8 eyes (1.5%), and hyaluronic acid in 4 eyes (0.8%).
STATISTICAL METHODS
In analyzing these data, we used the two statistical methods previously described: I (1) x/, Pearson's chisquare test, and (2) z, the normal deviate test for a linear trend in proportions related to the severity ofPVR.
RESULTS
Of 521 eyes, 338 (64.9%) had one scleral buckling operation, 130 (25.0%) had two operations, and 53 (10.2%) had three or more operations.
Table 1 shows the anatomic results for each grade of PVR. The overall anatomic success rate after at least 6 months was 46.9%. This figure does not include the 97 cases in which the retina was reattached but the followup was less than 6 months. The anatomic success rate decreased with increasing severity of PVR (P < 0.0001).
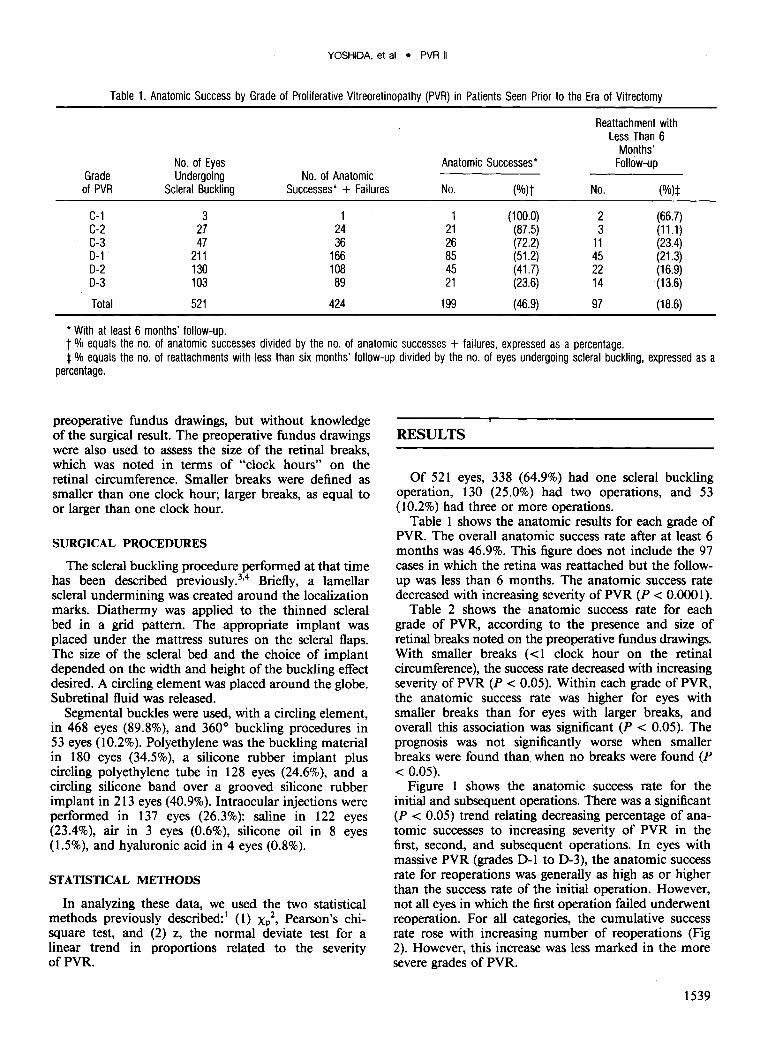
Table 2 shows the anatomic success rate for each grade of PVR, according to the presence and size of retinal breaks noted on the preoperative fundus drawings. With smaller breaks « 1 clock hour on the retinal circumference), the success rate decreased with increasing severity of PVR (P < 0.05). Within each grade of PVR, the anatomic success rate was higher for eyes with smaller breaks than for eyes with larger breaks, and overall this association was significant (P < 0.05). The prognosis was not significantly worse when smaller breaks were found than. when no breaks were found (P < 0.05).
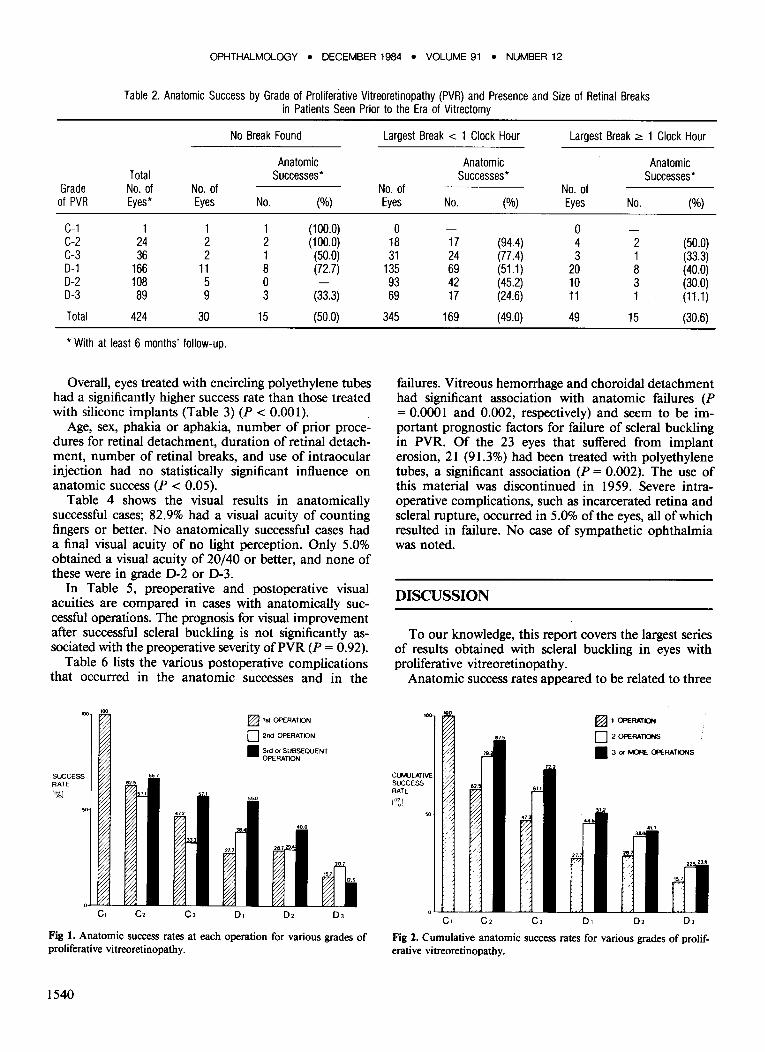
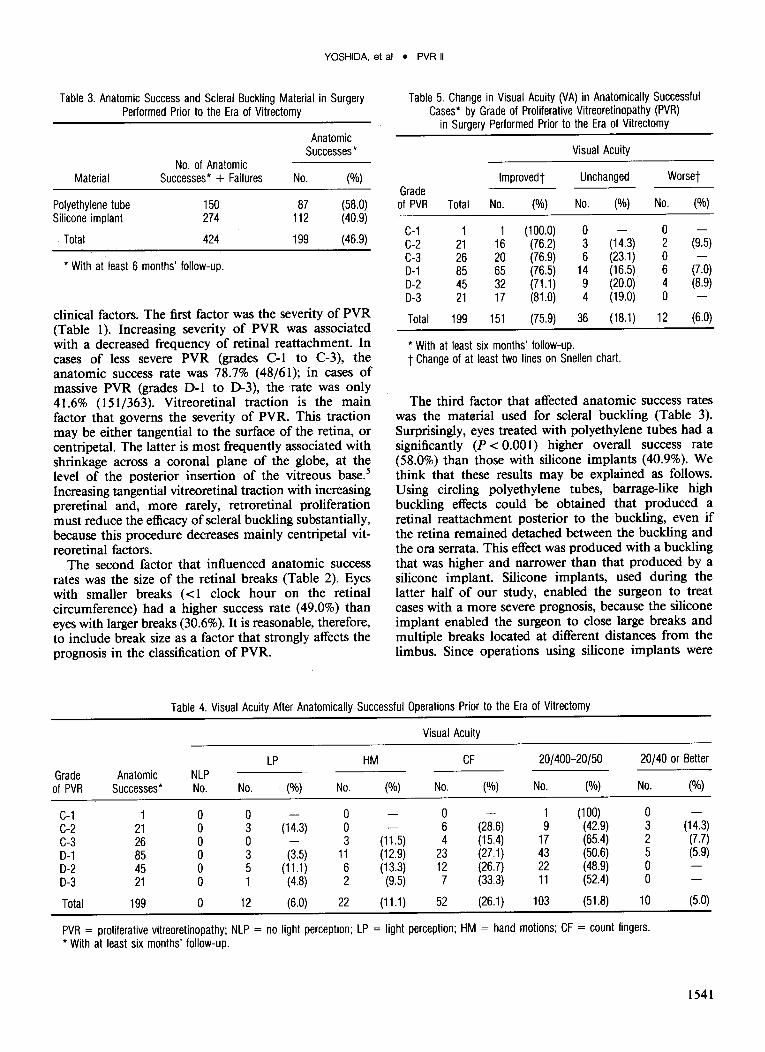
Figure 1 shows the anatomic success rate for the initial and subsequent operations. There was a significant (P < 0.05) trend relating decreasing percentage of anatomic successes to increasing severity of PVR in the first, second, and subsequent operations. In eyes with massive PVR (grades D-l to D-3), the anatomic success rate for reoperations was generally as high as or higher than the success rate of the initial operation. However, not all eyes in which the first operation failed underwent reoperation. For all categories, the cumulative success rate rose with increasing number of reoperations (Fig 2). However, this increase was less marked in the more severe grades of PVR.
1539
OPHTHALMOLOGY • DECEMBER 1984 • VOLUME 91 • NUMBER 12
Table 2. Anatomic Success by Grade of Proliferative Vitreoretinopathy (PVR) and Presence and Size of Retinal Breaks in Patients Seen Prior to the Era of Vitrectomy
No Break Found
Anatomic Total Successes*
Grade No. of No. of of PVR Eyes* Eyes No. (%)
C-1 1 1 1 (100.0) C-2 24 2 2 (100.0) C-3 36 2 1 (50.0) 0-1 166 11 8 (72.7) 0-2 108 5 0 0-3 89 9 3 (33.3)
Total 424 30 15 (50.0)
* With at least 6 months' follow-up.
Overall, eyes treated with encircling polyethylene tubes had a significantly higher success rate than those treated with silicone implants (Table 3) (P < 0.00 I).
Age, sex, phakia or aphakia, number of prior procedures for retinal detachment, duration of retinal detachment, number of retinal breaks, and use of intraocular injection had no statistically significant influence on anatomic success (P < 0.05).
Table 4 shows the visual results in anatomically successful cases; 82.9% had a visual acuity of counting fingers or better. No anatomically successful cases had a final visual acuity of no light perception. Only 5.0% obtained a visual acuity of 20/40 or better, and none of these were in grade D-2 or 0-3.
In Table 5, preoperative and postoperative visual acuities are compared in cases with anatomically successful operations. The prognosis for visual improvement after successful scleral buckling is not significantly associated with the preoperative severity ofPVR (P = 0.92).
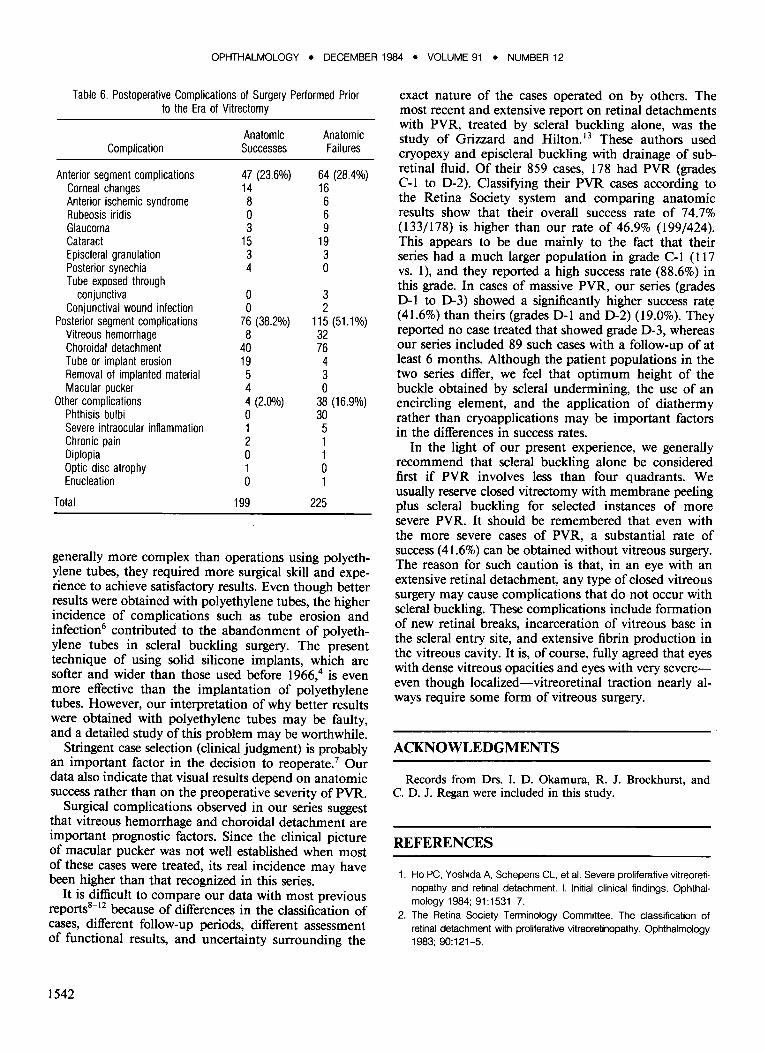
Table 6 lists the various postoperative complications that occurred in the anatomic successes and in the
SUCCESS RATE
1%1
c.
66 .7
7.'
3 .3
C2 D.
~ l SI OPERATION
o 2nd OPERATION
• 3rd (J( SUBSEQUENT OPERATION
'.0
",,0.0
28 .1 29."
0 2
Fig 1. Anatomic success rates at each operation for various grades of proliferative vitreoretinopathy.
1540
Largest Break < 1 Clock Hour Largest Break ~ 1 Clock Hour
Anatomic Anatomic Successes* Successes*
No. of No. of Eyes No. (%) Eyes No. (%)
0 0 18 17 (94.4) 4 2 (50.0) 31 24 (77.4) 3 1 (33.3)
135 69 (51.1) 20 8 (40.0) 93 42 (45.2) 10 3 (30.0) 69 17 (24.6) 11 1 (11.1)
345 169 (49.0) 49 15 (30.6)
failures. Vitreous hemorrhage and choroidal detachment had significant association with anatomic failures (P = 0.0001 and 0.002, respectively) and seem to be important prognostic factors for failure of scleral buckling in PVR. Of the 23 eyes that suffered from implant erosion, 21 (91.3%) had been treated with polyethylene tubes, a significant association (P = 0.002). The use of this material was discontinued in 1959. Severe intraoperative complications, such as incarcerated retina and scleral rupture, occurred in 5.0% ofthe eyes, all of which resulted in failure. No case of sympathetic ophthalmia was noted.
DISCUSSION
To our knowledge, this report covers the largest series of results obtained with scleral buckling in eyes with proliferative vitreoretinopathy.
Anatomic success rates appeared to be related to three
-CLM.JLATlIIE SUCCESS RATE
1%1
I [,:;;
~ f?:
~ f1
~ V ~/
C.
" .5
,J!l
ill
~
r~ ;/
~
'---~-
C2 CJ
~ I OPERATION
o 2 OPERATlONS
• 3 (J( MORE OPERATIONS
51.2
~ ~41.7
r ~ ~21.6
'-t....:.;~ '-'--'~ ~~ D. D2 OJ
Fig 2. Cumulative anatomic success rates for various grades of proliferative vitreoretinopathy.
YOSHIDA. et al • PVR II
Table 3. Anatomic Success and Scleral Buckling Material in Surgery Performed Prior to the Era of Vitrectomy
No. of Anatomic Material Successes· + Failures
Polyethylene tube 150 Silicone implant 274
Total 424
• With at least 6 months' follow-up.
Anatomic Successes·
No. (%)
87 (58.0) 112 (40.9)
199 (46.9)
clinical factors. The first factor was the severity of PVR (Table 1). Increasing severity of PVR was associated with a decreased frequency of retinal reattachment. In cases of less severe PVR (grades C-l to C-3), the anatomic success rate was 78.7% (48/61); in cases of massive PVR (grades D-l to D-3), the rate was only 41.6% (151/363). Vitreoretinal traction is the main factor that governs the severity of PVR. This traction may be either tangential to the surface of the retina, or centripetal. The latter is most frequently associated with shrinkage across a coronal plane of the globe, at the level of the posterior insertion of the vitreous base. 5
Increasing tangential vitreoretinal traction with increasing preretinal and, more rarely, retroretinal proliferation must reduce the efficacy of scleral buckling substantially, because this procedure decreases mainly centripetal vitreoretinal factors.
The second factor that influenced anatomic success rates was the size of the retinal breaks (Table 2). Eyes with smaller breaks « 1 clock hour on the retinal circumference) had a higher success rate (49.0%) than eyes with larger breaks (30.6%). It is reasonable, therefore, to include break size as a factor that strongly affects the prognosis in the classification of PVR.
Table 5. Change in Visual Acuity (VA) in Anatomically Successful Cases· by Grade of Proliferative Vitreoretinopathy (PVR)
in Surgery Performed Prior to the Era of Vitrectomy
Visual Acuity
Improvedt Unchanged Worset Grade of PVR Total No. (%) No. (%) No. (%)
C-1 1 1 (100.0) 0 0 C-2 21 16 (76.2) 3 (14.3) 2 (9.5) C-3 26 20 (76.9) 6 (23.1) 0 0-1 85 65 (76.5) 14 (16.5) 6 (7.0) 0-2 45 32 (71.1) 9 (20.0) 4 (8.9) 0-3 21 17 (81 .0) 4 (19.0) 0
Total 199 151 (75.9) 36 (18.1) 12 (6.0)
• With at least six months' follow-up. t Change of at least two lines on Snellen chart.
The third factor that affected anatomic success rates was the matorial used for scleral buckling (Table 3). Surprisingly, eyes treated with polyethylene tubes had a significantly (P < 0.00 I) higher overall success rate (58.0%) than those with silicone implants (40.9%). We think that these results may be explained as follows. Using circling polyethylene tubes, barrage-like high buckling effects could be obtained that produced a retinal reattachment posterior to the buckling, even if the retina remained detached between the buckling and the ora serrata. This effect was produced with a buckling that was higher and narrower than that produced by a silicone implant. Silicone implants, used during the latter half of our study, enabled the surgeon to treat cases with a more severe prognosis, because the silicone implant enabled the surgeon to close large breaks and multiple breaks located at different distances from the limbus. Since operations using silicone implants were
Table 4. Visual Acuity After Anatomically Successful Operations Prior to the Era of Vitrectomy
Visual Acuity
LP HM CF 20/400-20/50 20/40 or Better Grade Anatomic NLP
of PVR Successes· No. No. . (%) No. (%) No. (%) No. (%) No. (%)
C-1 1 0 0 0 0 1 (100) 0 C-2 21 0 3 (14.3) 0 6 (28.6) 9 (42.9) 3 (14.3) C-3 26 0 0 3 (11.5) 4 (15.4) 17 (65.4) 2 (7.7) 0-1 85 0 3 (3.5) 11 (12.9) 23 (27.1) 43 (50.6) 5 (5.9) 0-2 45 0 5 (11.1) 6 (13.3) 12 (26.7) 22 (48.9) 0 0-3 21 0 1 (4.8) 2 (9.5) 7 (33.3) 11 (52.4) 0
Total 199 0 12 (6.0) 22 (11.1) 52 (26.1) 103 (51.8) 10 (5.0)
PVR = proliferative vitreoretinopathy; NLP = no light perception; LP = light perception; HM = hand motions; CF = count fingers . • With at least six months' follow-up.
1541
OPHTHALMOLOGY • DECEMBER 1984 • VOLUME 91 • NUMBER 12
Table 6. Postoperative Complications of Surgery Performed Prior to the Era of Vitrectomy
Anatomic Anatomic Complication Successes Failures
Anterior segment complications 47 (23.6%) 64 (28.4%) Corneal changes 14 16 Anterior ischemic syndrome 8 6 Rubeosis iridis 0 6 Glaucoma 3 9 Cataract 15 19 Episcleral granulation 3 3 Posterior synechia 4 0 Tube exposed through
conjunctiva 0 3 Conjunctival wound infection 0 2
Posterior segment complications 76 (38.2%) 115 (51.1%) Vitreous hemorrhage 8 32 Choroidal detachment 40 76 Tube or implant erosion 19 4 Removal of implanted material 5 3 Macular pucker 4 0
Other complications 4 (2.0%) 38 (16.9%) Phthisis bulbi 0 30 Severe intraocular inftammation 1 5 Chronic pain 2 1 Diplopia 0 1 OptiC disc atrophy 1 0 Enucleation 0 1
Total 199 225
generally more complex than operations using polyethylene tubes, they required more surgical skill and experience to achieve satisfactory results. Even though better results were obtained with polyethylene tubes, the higher incidence of complications such as tube erosion and infection6 contributed to the abandonment of polyethylene tubes in scleral buckling surgery. The present technique of using solid silicone implants, which are softer and wider than those used before 1966,4 is even more effective than the implantation of polyethylene tubes. However, our interpretation of why better results were obtained with polyethylene tubes may be faulty, and a detailed study of this problem may be worthwhile.
Stringent case selection (clinical judgment) is probably an important factor in the decision to reoperate.7 Our data also indicate that visual results depend on anatomic success rather than on the preoperative severity of PVR.
Surgical complications observed in our series suggest that vitreous hemorrhage and choroidal detachment are important prognostic factors. Since the clinical picture of macular pucker was not well established when most of these cases were treated, its real incidence may have been higher than that recognized in this series.
It is difficult to compare our data with most previous reports8
-12 because of differences in the classification of
cases, different follow-up periods, different assessment of functional results, and uncertainty surrounding the
1542
exact nature of the cases operated on by others. The most recent and extensive report on retinal detachments with PVR, treated by scleral buckling alone, was the study of Grizzard and Hilton. 13 These authors used cryopexy and episcleral buckling with drainage of subretinal fluid. Of their 859 cases, 178 had PVR (grades C-I to 0-2). Classifying their PVR cases according to the Retina Society system and comparing anatomic results show that their overall success rate of 74.7% (133/178) is higher than our rate of 46.9% (199/424). This appears to be due mainly to the fact that their series had a much larger population in grade C-I (I17 vs. I), and they reported a high success rate (88.6%) in this grade. In cases of massive PVR, our series (grades 0-1 to 0-3) showed a significantly higher success rate (41.6%) than theirs (grades 0-1 and 0-2) (19.0%). They reported no case treated that showed grade 0-3, whereas our series included 89 such cases with a follow-up of at least 6 months. Although the patient populations in the two series differ, we feel that optimum height of the buckle obtained by scleral undermining, the use of an encircling element, and the application of diathermy rather than cryoapplications may be important factors in the differences in success rates.
In the light of our present experience, we generally recommend that scleral buckling alone be considered first if PVR involves less than four quadrants. We usually reserve closed vitrectomy with membrane peeling plus scleral buckling for selected instances of more severe PVR. It should be remembered that even with the more severe cases of PVR, a substantial rate of success (41.6%) can be obtained without vitreous surgery. The reason for such caution is that, in an eye with an extensive retinal detachment, any type of closed vitreous surgery may cause complications that do not occur with scleral buckling. These complications include formation of new retinal breaks, incarceration of vitreous base in the scleral entry site, and extensive fibrin production in the vitreous cavity. It is, of course, fully agreed that eyes with dense vitreous opacities and eyes with very severeeven though localized-vitreoretinal traction nearly always require some form of vitreous surgery.
ACKNOWLEDGMENTS
Records from Drs. I. D. Okamura, R. J. Brockhurst, and C. D. J. Regan were included in this study.
REFERENCES
1. Ho PC, Yoshida A, Schepens CL, et al. Severe proliferative vitreoretinopathy and retinal detachment. I. Initial clinical findings. Ophthalmology 1984; 91 :1531-7.
2. The Retina SOCiety Terminology Committee. The classification of retinal detachment with proliferative vitreoretinopathy. Ophthalmology 1983; 90:121-5.
YOSHIDA, et al • PVR II
3. Schepens CL. Scleral buckling procedures. Trans Am Acad Ophthalmol Otolaryngol 1958; 62:206-18.
4. Schepens Cl. Scleral buckling with circling element. Trans Am Acad Ophthalmol OtolaryngoI1964; 68:959-79.
5. McMeel JW, Buzney SM. Treatment of rhegmatogenous detachment in massive preretinal retraction. In: Symposium on Medical and Surgical Diseases of the Retina and Vitreous; Transactions of the New Orleans Academy of Ophthalmology. St Louis: CV Mosby, 1983; 137-43.
6. Regan CDJ, Schepens CL. Erosion of the ocular wall by circling polyethylene tubing; a late complication of scleral buckling. Am J Ophthalmol 1964; 57:79-83.
7. Schepens CL: Retinal Detachment and Allied Diseases. Philadelphia: WB Saunders, 1983; 493.
8. Havener WHo Massive vitreous retraction. Ophthalmic Surg 1973; 4(2):22-67.
9. Havener WHo Massive vitreous retraction. Int Ophthalmol Clin 1976; 16(1):135-55.
10. Scott JD. The treatment of massive vitreous retraction by the separation of pre-retinal membranes using liquid silicone. Mod Probl Ophthalmol 1975; 15:285-90.
11. Grey RHB, Leaver PK. Silicone oil in the treatment of massive preretinal retraction. I. Results in 105 eyes. Br J Ophthalmol 1979; 63:355-60.
12. Machemer R, Laqua H. A logical approach to the treatment of massive periretinal proliferation. Ophthalmology 1978; 85:584-93.
13. Grizzard WS, Hilton GF. Scleral buckling for retinal detachments complicated by periretinal proliferation. Arch Ophthalmol 1982; 100:419-22.
1543








![l O Journal of Clinical & Experimental C …...developing rhegmatogenous retinal detachment [1-3]. Left untreated, a chronic retinal detachment can lead to complications such as proliferative](https://img.pdfslide.net/doc/110x75/5e6881d4802d47373f0932ef/l-o-journal-of-clinical-experimental-c-developing-rhegmatogenous-retinal.jpg)







![An epidemiological model for proliferative kidney disease ... · An epidemiological model for proliferative ... [18, 35]. Overt infec-tion ... An epidemiological model for proliferative](https://img.pdfslide.net/doc/110x75/5c00b25409d3f225538b84ad/an-epidemiological-model-for-proliferative-kidney-disease-an-epidemiological.jpg)












