Embed Size (px)
Citation preview

Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1108
_____________________________ _____________________________
Severe Sleep Problemsamong Infants
A Five-Year Prospective Study
BY
MALENA THUNSTRÖM
ACTA UNIVERSITATIS UPSALIENSISUPPSALA 2002

Dissertation for the Degree of Doctor of Philosophy (Faculty of Medicine) in Paediatricspresented at Uppsala University in 2002
ABSTRACT
Thunström, M. 2002. Severe Sleep Problems among Infants. A Five-Year ProspectiveStudy. Acta Universitatis Upsaliensis. Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1108. 77 pp. Uppsala. ISBN 91-554-5201-9.
The aim of this thesis was to explore the prevalence of parentally experienced infant sleepproblems, with special interest in severe problems, in a total community sample of 2 518infants aged between 6 and 18 months. Factors associated with severe sleep problems weresought. Parents reported 16 % of the infants to have difficulties in falling asleep at night,and 30 % to have frequent night waking. Severe sleep problems were associated withfrequent night meals, psychosocial problems in the family, exhaustion and depression inthe mother, and parental stress. An association with infant difficultness, high activity andproblematic behaviour was also found.
In a five-year prospective study a group of children fulfilling specific criteria for severesleep problems in infancy (N=27) was followed after an interventional sleep programmeand compared with a control group regarding sleep characteristics, behaviour anddevelopment. One month after an interdisciplinary treatment programme, combiningbehavioural technique with family work, the average number of times the case babies wokeup had diminished from 6.0 to 1.8 times per night. A 92 % rate of improvement wasreported.
The changes were stable over time. Comparisons with the controls during five yearsrevealed no significant group difference in sleep characteristics. Concerning behaviour anddevelopment, however, there were significant differences. At the age of 5.5 years, seven ofthe children in the former sleep problem group met the criteria for the diagnosis ofattention-deficit/hyperactivity disorder. No control child qualified for the diagnosis.
Close follow-ups of infants with combined severe sleep and behavioural problems are recommended.
Key words: Sleep disorders, infant, behavioural therapy, psychosocial problems, attention-deficit/hyperactivity disorder.
Malena Thunström, Department of Women´s and Children´s Health, Uppsala UniversityChildren´s Hospital, SE-751 85 Uppsala, Sweden
© Malena Thunström 2002
ISSN 0282-7476ISBN 91-554-5201-9
Printed in Sweden by Uppsala University, Tryck & Medier, Uppsala 2002
To all sleepy children

LIST OF PAPERSThis thesis is based on the following papers, which will be referred to in thetext by their Roman numerals:
I Thunström M.Severe sleep problems among infants in a normal population in Sweden:prevalence, severity and correlates. Acta Paediatrica 1999; 88: 1356-1363.
II Thunström M.Severe sleep problems among infants: family and infant characteristics.Ambulatory Child Health 1999; 5: 27-41.
III Thunström M.A 2.5-year follow-up of infants treated for severe sleep problems.Ambulatory Child Health 2000; 6: 225-235.
IV Thunström M.Severe sleep problems in infancy associated with subsequentdevelopment of attention–deficit/hyperactivity disorder at 5.5 years ofage. Acta Paediatrica. Accepted for publication.
V Thunström M.A 5-year follow-up of infants with severe sleep problems. Manuscript.
Reprints were made with the permission of the publishers.

CONTENTS
INTRODUCTIONGeneral background 7Maturation of sleep pattern in childhood 7Definition and classification of sleep disorders 9Assessment of sleep 11Epidemiology of sleep problems:prevalence, severity and persistence 12Correlates to disturbed sleep 14Treatment of sleep problems in childhood 15Attention-deficit/hyperactivity disorder (ADHD) and sleep 16Aims of the studies 21
METHODSDesign and subject selection 22 Study I 22 Study II-IV 22 Study V 24Procedures and measures 24
Study I 24Questionnaire on sleep and background factors 24Study II, III, V 25Questionnaires on sleep, family and infant characteristics and sleep diaries. 26Treatment programme 28Study IV 30Screening instrument for ADHD 30Assessment methods 31
Statistics 33
RESULTSPrevalence and classification of sleep problems 33Family and infant characteristics associated with severe infant sleep problems 36Short-term and long-term outcome of an interdisciplinary sleep treatment programme 44Factors associated with subsequent development of attention-deficit/hyperactivity disorder 48
DISCUSSIONGeneral discussion 52Validity of the results 58Conclusions and clinical implications 61ACKNOWLEDGEMENTS 63REFERENCES 65

7
INTRODUCTION
General background
Sleep plays a major role in children´s well-being and is strongly influenced by
the child´s health status, psychological stress and family issues as well as by
multiple aspects of his or her culture and environment. Also, children´s sleep
patterns affect their well-being within the same wide range of health and
psychosocial phenomena.
Research has shown that sleep problems in infants and young children are
prevalent. Cross-sectional studies show that between 15 % and 35 % of all
children aged between 6 months and 5 years are reported by their parents to
show some type of sleep disturbance (22,69,76,98,100,102).
Before six months of age it is doubtful whether the label "sleep disturbance"
should be used, since during this period night waking is necessary in order to
fulfil the needs of frequent nutrition of the child. This is also the period
needed to reorganize the sleep pattern of the newborn to a more mature
pattern (85).
Maturation of normal sleep pattern in childhood
Sleep and sleep stages are defined by specific patterns of electro-
physiologically recorded brain activity, muscle tone and eye movements.
These polysomnographic measures divide sleep into two principal states:
sleep associated with rapid eye movements, "REM sleep", and sleep without
rapid eye movements, "non–REM sleep" (28). The REM component of sleep,
which dominates during the foetal period and the early months of life (50 %
of the sleep time), is thought to play a crucial role with regard to brain

8
development (105). The amount of REM sleep decreases to 30 % during the
first year of life and the REM–non REM state cycle also undergoes
maturational changes. In newborns and very young infants the cycle lasts
approximately 40 to 60 minutes. At two years of age the cycle has increased
to 75 minutes and continues to increase to an average of 84 minutes in 5-year-
olds (65).
A newborn baby does not distinguish day from night. Both sleeping and
eating take place around the clock, equally distributed over a 24-hour-period,
and the two processes are linked in time to each other. The baby wakes up to
eat and most often goes back to sleep while suckling and being fed at the
breast.
Gradually, in the course of the baby´s first year, a transition to a more regular
pattern of eating and sleeping takes place (10). The child acquires a pattern of
regular meals during daytime, a period of prolonged sleep during the night
and one, or most often two, short naps during daytime. Eating and sleeping
are increasingly separated, and, normally, the one-year-old child has grown
out of the habit of going to sleep while eating.
Temporary nightwaking in occasional periods of short duration is very
common among infants (42), but in the absence of any current physical
disease, a normal development and maturing of the central nervous system
(10) and normal parental handling (10,125), 90 % of one-year-olds sleep all
night (85). Prolonged and complicated sleep problems, however, have a
tendency to remain, especially from the first year of life to later childhood
(1,21,67,92). Moreover longitudinal studies (20,41,60,115) have indicated
that the attitudes and (over-) responsiveness of the parents to the signals of the
child in the parent–infant interaction could play a role in the maintenance of
the sleep problems of the child.

9
Other possible causative and maintaining mechanisms that have been studied
include factors in the genetic, somatic, psychological and psychosocial areas
(19-20,32,61,81,89). Prolonged, complicated sleep problems show a picture
of multiproblem, where the separate factors seem to amplify each other in
vicious circles. Factors affecting the child, the stressed and exhausted parents
and the social situation probably influence each other reciprocally and
interfere with the normal maturation of the sleep pattern.
Definition and classification of sleep disorders
Sleep problems in childhood are classified according to the International
Classification of Sleep Disorders: Diagnostic and Coding Manual (ICSD,
1990, American Sleep Disorder Association) into the following categories:
1. Dyssomnia
Dyssomnia comprises disorders that cause either insomnia (most common) or
excessive sleepiness (rare). Childhood insomnia is most often seen in limit-
setting sleep disorder (in which inadequate enforcement of bedtimes by the
parent results in the child stalling or refusing to go to bed at an appropriate
time) and in sleep-onset association disorder (in which the onset of sleep in
the child is impaired by the absence of a certain object or set of
circumstances). The first conditions is often called "sleep refusal" or "bedtime
struggles" ( a vivid expression) and has been reported in 5-10 % of a normal
population of preschool children (44). The second condition is often called
"frequent night-waking", when the child needs parental intervention of some
form several times every night to go back to sleep, and is seen in 15-20 % of
all children between 6 months and 3 years of age (44,98). Severity is
systematically classified along an axis in the ICSD, 1990, but this
classification and coding system has not been widely used in studies.

10
The ICSD criteria of severe sleep refusal (limit-setting sleep disorder) require
five or more episodes per night of stalling, calling out or leaving the bedroom.
The ICSD criteria of severe night waking problems (sleep-onset association
disorder) require a prolonged sleep latency and over three nightly wakings, or
two or three wakings, each lasting over 10 minutes or one lasting over 15
minutes. The awakenings occur at least five nights per week. Corresponding
detailed definitions for mild and moderate forms of the different sleep
disturbances are also found in the ICSD.
Nocturnal eating syndrome and schedule disorders are other types of
insomnia. Nocturnal eating (drinking) syndrome is characterized by recurrent
awakenings, with the inability to return to sleep without eating or drinking,
preferably breastmilk or formula. In schedule disorder the distribution of
sleep in terms of nap frequency and length across a 24-hour period, the sleep-
wake cycle, is altered in a way that comes into conflict with social
expectations and habits. The child´s sleep occurs at an inappropriate time.
Of course these definitions are cultural, as are the expectations of what is
"normal" infant sleep. Breast-fed babies throughout the world wake at night
and fall asleep at the breast, and in industrialized societies, in which the ICSD
1990 was written, we may have established inappropriate expectations from
experience with bottle-fed infants.
Nevertheless, parents of children with the above-mentioned sleep patterns
report themselves to be exhausted and in need of paediatric help.
Paediatricians, therefore, must have a good knowledge of infant sleep and
factors related to severe problems.
Excessive sleepiness is seen in the rare disorder, narcolepsy, and more often
in the obstructive sleep apnea syndrome.
11
2. Parasomnia
Parasomnia comprises disorders that intrude into or occur during sleep that
are not, primarily disorders of the states of sleep and wakefulness per se.
Included here are confusional arousals, sleepwalking, sleep terrors, sleep
talking and sleep bruxism. Parasomnia is seen predominantly in children aged
3-12 years, where it encompasses 1-6 % of the population (7).
3. Medical/Psychiatric Sleep Disorders
Medical/Psychiatric Sleep Disorders comprise the medical and psychiatric
disorders commonly associated with sleep disturbance. In acute and chronic
illness (123), above all in diseases with pains or itching sensations, (38) sleep
problems are common, but the most difficult and prolonged sleep problems
are seen in mentally retarded children and children with autism, indicating a
common factor of dysfunction of the central nervous system (16).
Assessment of sleep
Clinical assessment of sleep disorders in children includes developmentally
appropriate history-taking of sleep-wake behaviour, including medical,
psychiatric as well as family and psychosocial issues (8,42,84). Physical
examination should be performed, with special attentiveness to signs of
diseases accompanied by pains, breathing difficulties or itching sensations.
Questionnaires and sleep logs or sleep diaries are valuable tools in the process
of detailed history-taking concerning sleep-wake complaints (8,121).
Actigraphy was developed as a practical measure for long-term quantification
of sleep/wake periodicity of movement, since both infants and children have a
lower activity level in sleep than in wakefulness. A small motion sensor and
12
digital recorder is worn on a wrist and later downloaded into a computerized
analysis system. Advantages include noninvasiveness, ease of use and
automated scoring. Accuracy for sleep-wake discrimination has been reported
to be 85-93 % (111-112).
Audio and video recordings as well as polysomnography or other specialized
laboratory test are seldom used in infant studies. In clinical practice, selected
complicated cases are referred to sleep clinics with extended laboratory
devices (multichannel recordings, cardiorespiratory video systems, pulse
oximetry) (24,58).
Results from studies comparing parental reports with objective sleep
measures (109) show that parents are accurate reporters of sleep schedule
measures such as sleep onset and sleep duration. They overestimate, however,
the time that their infants spend in actual sleep and underestimate the number
of their night wakings. According to that result, short sleep duration and many
night wakings reported by parents of small infants should be regarded as a
minimum rather than be suspected of being an exaggeration by exhausted
care-takers.
Epidemiology of sleep problems: prevalence, severity
and persistence
Sleep disturbances in infants and young children, such as night waking and
bedtime struggles, are among the most common behaviour problems
encountered in paediatric practice. Night waking occurs in 15 % to 35 % of
children aged between 6 months and 5 years (17-18,21,59,69,76,94,98,102)
and the prevalence of bedtime struggles varies from 6 % to 16 % in the first 2
years (18,76,94) according to previous studies.
13
These earlier studies show that approximately one preschool child out of four
shows some kind of sleep problem, most often of short duration. A small
group of children, however, approximately 5 %, have more longlasting and
complicated sleep disturbances that can have an influence both on the health
of the child and on the function of the whole family.
Information on the long-term course of sleep problems in children (33,70-71),
and particularly in preschool children, is sparse. Richman, in her survey of
cross-sectional and longitudinal studies of disorders of initiating and
maintaining sleep (100), concludes that although correlations for waking
problems at different ages are reported low in schoolchildren (70), a
considerable number of preschool children have persistent sleep problems.
Especially during the first 2 to 3 years, the probability of continued waking is
high.
Infants who are irritable, sleep little and cry frequently during the early weeks
of life are more likely to be poor sleepers during the second year of life
(20,23). One survey (60) found that just under half (44 %) of those children
waking regularly at 6 months were still waking at 1 year. Furthermore almost
the same proportion (41 %) of the night wakers at 1 year were still waking at
18 months, and from 18 months to 2 years just over half of the children (54
%) continued waking. Conversely, 80 % to 90 % of nonwakers at these ages
continued to sleep well. Continuity after 2 years was less marked: 71 % of
night wakers at 2 years of age slept well at 3 years of age, and 86 % of wakers
at 3 slept well at 4.5 years of age.
Another community survey (103) found more problems. Of those with
bedtime problems at 3 years of age, 25 % still had problems at 4 years of age.
For night waking problems the figure was 36 %. Persistence of the same
problems in children 4 to 8 years of age was 40 % and 17 %, respectively.
14
There was a small core of persistent wakers, who Richman (100) speculates
could be particularly susceptible to irregular sleep patterns because of
neurophysiological or temperamental factors.
In another study (129) children with persistent sleep problems from 8 months
to 3 years of age (41 %), were found to be more likely to have behaviour
problems, especially temper tantrums and behaviour management problems,
than were children without persistent sleep problems. Finally, 84 % of sleep-
disturbed two-year-olds still had persistent sleep disturbances 3 years later in
a study (67) that found that persistent sleep disturbances had a significant
relationship with increased frequency of stress factors in the environment.
Different definitions of night waking and bedtime problems in different
studies contribute to generating different prevalence, severity and persistency
figures, but in summary, longlasting and complicated sleep problems seem to
have a tendency to remain, especially from the first year of life to later
childhood (1,21,67,92) and to be associated with behavioural problems
(119,129) as well as extreme tiredness and stress in the family (1,13,51,53).
Correlates to disturbed sleep
Factors in the genetic, somatic, psychological and psychosocial areas
correlate to disturbed sleep, as possible causative or maintaining mechanisms.
Genetic vulnerability, perinatal and medical disorders, temperamental
difficultness in the child, psychological (over-) responsiveness of the parents,
parental insecurity and stress, psychosocial problems, and development of
vicious circles (19-20,32,61,82,89) have been documented.
The effects of insufficient and disturbed sleep in children include daytime
behavioural problems. The children do not necessarily indicate their sleep loss
by obvious daytime somnolence (119). On the contrary, a hyperactive

15
behaviour might be the only indicator of sleep deprivation in a child, with
resolution of the behaviour problem following successful treatment of the
sleep disturbance (46). The effect of chronically disturbed sleep on the parents
is extreme tiredness (30,47,98,125,129), and several studies have shown that
severe sleep problems in infants and toddlers (pre-school children) are
associated not only with extreme tiredness and but also with psychiatric (73)
and physical illness in the family, especially depression in the mother. The
parents of children with severe sleep problems often seek help, and
associations with marital problems (19-20,82,89) and even child abuse have
been described (30,61,67). A heightened risk of later development of
behavioural problems and school difficulties also exists for children with
severe sleep problems (31-32,67,83).
Treatment of sleep problems in childhood
The methods suggested in the management of sleep difficulties range from
total acceptance (117) (usually meaning taking the child to the parents´ bed)
to ignoring all crying, with many variations in between. A number of
treatment programs, based on behavioural techniques, have been described in
the literature (73). These include establishing night-time routines and rituals,
reorganizing settling and waking times, minimizing night-time attention by
gradually withdrawing reinforcers, controlled crying by graduated extinction
(progressive delay responding) or straight extinction ("crying it out"), and
scheduled anticipatory waking where parents arouse and then resettle their
child 15-60 minutes before expected spontaneous awakings.
Studies of these techniques show high rates of improvement (80-90 %) when
used with support from a therapist (5,63,97,101,118). Sedatives are
commonly used and may be helpful in the short-term, but have been shown to
have long-term benefits only when used in combination with a behavioural
16
programme (51). The studies carried out to investigate the success of
behavioural programmes rarely have follow-up periods longer than three
months (47,56,73,79,81,126,128).
Attention-deficit/hyperactivity disorder (ADHD) and
sleep
Sleep problems are frequently reported in children and adolescents with
attention-deficit/hyperactivity disorder (ADHD) (14,25,66,88,104,124).
Parents perceive children with ADHD to have greater sleep difficulty than
normally developing children, and anecdotal reports of practising clinicians
suggest that the sleep of children with ADHD is often reported by parents to
have been disturbed from the very beginning of the child´s life, ever since
infancy: "He has never slept through a whole night in his entire life."
Previously, based on clinical experience, sleep disturbance among children
with ADHD was so widely presumed that it was included as one of the
diagnostic criteria for the disorder (DSM-III; American Psychiatric
Association, 1980). However, further research and re-examinations (14) led to
the exclusion of the sleep disturbance criterion in the 1987 version of the
DSM-III-manual. The present diagnostic criteria for ADHD (DSM-IV, 1994)
are presented in Box 1.

17
Box 1. Diagnostic criteria for attention-deficit/hyperactivity disorder (DSM-IV, 1994)*
A. Either (1) or (2):
(1) six (or more) of the following symptoms of inattention have persisted for at least6 months to a degree that is maladaptive and inconsistent with developmentallevel:
Inattention(a) often fails to give close attention to details or makes careless mistakes in
schoolwork, work, or other activities(b) often has difficulty sustaining attention in tasks or play activities(c) often does not seem to listen when spoken to directly(d) often does not follow through on instructions and fails to finish schoolwork,
chores, or duties in the workplace (not due to oppositional behaviour orfailure to understand instructions)
(e) often has difficulty organizing tasks and activities(f) often avoids, dislikes, or is reluctant to engage in tasks that require sustained
mental effort (such as schoolwork or homework)(g) often loses things necessary for tasks or activities (e.g., toys, school
assignments, pencils, books, or tools)(h) is often easily distracted by extraneous stimuli(i) is often forgetful in daily activities
(2) six (or more) of the following symptoms of hyperactivity-impulsivity havepersisted for at least 6 months to a degree that is maladaptive and inconsistentwith developmental level:
Hyperactivity(a) often fidgets with hands or feet or squirms in seat(b) often leaves seat in classroom or in other situations in which remaining
seated is expected(c) often runs about or climbs excessively in situations in which it is
inappropriate (in adolescents or adults, may be limited to subjective feelingsof restlessness)
(d) often has difficulty playing or engaging in leisure activities quietly(e) is often "on the go" or often acts as if "driven by a motor"(f) often talks excessively
Impulsivity(g) often blurts out answers before questions have been completed(h) often has difficulty awaiting turn(i) often interrupts or intrudes on others (e.g., butts into conversations or games)
A. Some hyperactive-impulsive or inattentive symptoms that caused impairment werepresent before age 7 years.
B. Some impairment from the symptoms is present in two or more settings (e.g., at school[or work] and at home).

18
C. There must be clear evidence of clinically significant impairment in social, academic,or occupational functioning.
D. The symptoms do not occur exclusively during the course of a PervasiveDevelopmental Disorder, Schizophrenia, or other Psychotic Disorder and are not betteraccounted for by another mental disorder (e.g., Mood Disorder, Anxiety Disorder,Dissociative Disorder, or a Personality Disorder).
* American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed (DSM-IV). Washington, DC: American Psychiatric Press, 1994.
A detailed and systematic review of empirical research published since 1970
on sleep disturbances in children with ADHD, encompassing sixteen relevant
studies, was published in 1998 by Corkum, Tannock and Moldofsky (35).
They found that although subjective accounts of sleep disturbances in ADHD
were prevalent (based on sleep diaries, questionnaires and interviews),
objective verification of these disturbances (by polysomnographs, actigraphy
or video) was less robust (13). In fact, the only consistent objective findings
were that children with ADHD displayed more movements during sleep but
did not differ from normal controls in total sleep time (39,78,121). Further
studies by the same authors have confirmed this picture (34) and pointed to a
complex relationship between sleep problems and ADHD. In a recent study
(80) the conclusion was drawn that although subjective sleep difficulties are
common in ADHD youths, they are frequently accounted for by comorbidity
and pharmacotherapy.
However, when convincing evidence exists of sleeplessness in an overactive
child, attempts should be made to increase or improve the sleep because, in
some cases, the ADHD features may be the result of poor sleep (37,121). The
effects of sleep loss in children include tiredness, difficulties with focused
attention, low threshold to express negative affect (irritability and easy
frustration), and difficulty modulating impulses and emotions (37). In some
cases these symptoms may resemble ADHD. This has been reported in
children with obstructive sleep apnoea, with improvement of behaviour
following treatment (53).
19
ADHD-associated sleep disturbances may be improved by medication with
clonidine
(93,127). Improvements can also be achieved by administration of stimulant
drugs late in the day (29,93,121,127) even if insomnia secondary to stimulant
medication is a well-known adverse effect in some children (15,35,120).
Prospective, randomized, double-blind, placebo-controlled, long-term studies
of stimulant treatment for childhood attention-deficit problems have,
however, showed that for this patient group in general, early awakenings and
disturbed sleep tend to occur less frequently with stimulant treatment than at
baseline, i.e. without treatment (49).
In their review of the literature (35), Corkum, Tannock and Moldofsky
conclude that the exact nature of the sleep problems in children with ADHD
remains to be determined. Many relevant issues need new and better
methodological approaches. One interesting field is Periodic Limb
Movements in Sleep (PLMS) in children with ADHD, which has been
recently studied by Picchietti et al (90-91). PLMS are repetitive flexions of
the toes, feet, legs, thighs and/or the arms which recur periodically during
sleep. Sleep disruptions often accompany these movements, which in studies
using polysomnography and electromyography have been shown to be more
prevalent in children with ADHD than in control children.
Studies using retrospective data on sleep patterns in infancy among children
with ADHD are scarce. Trommer et al (124) compared 48 schoolchildren with
ADD (with and without hyperactivity) with 30 controls using retrospective
parental questionnaires which covered the ages 0 to 12 months and 1 to 4
years. The ADD children were reported to have had more frequent arousals
than the controls had both in the first year and from 1 to 4 years. However,
there is an obvious risk of selective memory bias in such studies.
20
Other prospective studies than the one included in this thesis on children with
severe sleep problems in infancy, concerning the risk of later development of
inattention and hyperactivity-impulsivity, have to our knowledge not yet been
performed.

21
Aims of the studies
The aims of this 5-year prospective study were:
1. to provide epidemiological data on infant sleep-wake characteristics and
the prevalence and severity of sleep problems in a general population, as
perceived by parents
(Study I),
2. to explore medical, psychological and psychosocial child and family
characteristics associated with severe infant sleep problems (Studies I och
II),
3. to investigate the changes in sleep in a group of severely sleep-disturbed
infants after a specific treatment programme combining behavioural
technique and interdisciplinary family work (Study III),
4. to prospectively follow and compare a group of children identified with
severe sleep problems in infancy with a control group regarding the
development of symptoms of attention-deficit/hyperactivity disorder
(ADHD) (Study IV) and regarding further sleep pattern (Studies III and
V),
5. to explore factors in infancy which are associated with subsequent
development of ADHD in later childhood (Study IV).

22
METHODS
Design and subject selection
Study I
A total community sample of 2 518 infants aged between 6 and 18 months
were approached using a parental questionnaire. The response rate was 83 %.
Data from the collection procedure point to a non-selective drop-out, not
reflecting presence or absence of sleep problems. Severe sleep problems as
defined by the ICSD were found in 129 of the children (6.2 %) who were
studied in detail, with the rest of the population as controls.
Studies II-IV
Those 6 to 12 month-old children in the community sample who fulfilled
specific inclusion criteria for severe and chronic sleep problems (N = 27)
created the case group.
Inclusion criteria were:
- the child should be reported by parents to have a prolonged sleep latency
and over three nightly wakings occurring at least five nights per week. This
pattern of disrupted sleep should have prevailed for a period of at least
6 months.
- infant age between 6 and 12 months at inclusion in the study. (The reason
for restriction of the study to this age group was limited resources and the
ambition to investigate all children with severe sleep problems in a specific
population with home visits by the same paediatrician).

23
- full-term pregnancy with a birth weight of greater than 2 500 grams and
gestational age of at least 37 weeks.
- the parents should report the need of help. (This criteria turned out to be
unnecessary. All parents of children with the above-mentioned sleep
problems reported themselves to be in need of help. This was true even for
the non-European parents in this group, who co-slept with their breastfed
child according to their cultural norms. They all reported much need for
help with their child´s sleep within the context of the Swedish
industrialized society).
- the parents should be able to communicate in Swedish or English.
The exclusion criterion was:
- signs of significant organic causes of the sleep problem identified by
hospital examinations and laboratory tests.
Among the 28 families with infants fulfilling the set inclusion criteria,
(i.e. 2 % of the sample of 1 259 children aged between 6 and 12 months), one
family was not able to participate because they moved to another part of the
country. The other 27 families agreed to participate in the study. Sixteen of
the children were boys, eleven girls. None of them fulfilled the exclusion
criteria. All were basically healthy and went further in the study.
A control group was matched with regard to age and sex. The infant of a
particular sex who fell next in age sequence to the case infant in the Child
Health Center (CHC) register was chosen as a control. A further criterion was
that no sleep problems were reported on the questionnaire. Of 33 families
contacted, 27 agreed to participate.
24
Study V
In addition to the original control group, an extended control group was
created from the questionnaire – study I, consisting of four control children
for each case child. The controls were matched for age and sex, had no
reported sleep problems in the questionnaire at 6 to 12 months and were still
living in Sweden five years later.
Procedure and measures
Study 1
In January 1996 data were collected in a parent population study in the urban
district of Uppsala (the fourth largest municipality in Sweden). A
questionnaire, constructed especially for this study, was sent to all parents
with an infant born during the period from July 1994 to July 1995.
Questionnaire on sleep and background factors
The instrument covered the following areas: social and demographic
background, pregnancy and birth, sleep-wake characteristics, parental
behaviour, and feeding problems.
Most items in the questionnaire had a 5-step response scale with verbal
definitions of each scale step. A few items had response categories with
yes/no answers. The items were constructed in close accordance with the
ICSD classification in addition to subjective parental rating scales of the
severity of the problem. No validation process was possible for these scales,
since the explicit aim of the questions was to measure early sleep problems as
perceived by parents.
25
Study II, III, V
A home visit was scheduled when parents had received information about the
study and agreed to participate in the research project.
The author, who is a clinically active a paediatrician, interviewed the parents
about the infant’s sleep characteristics and family members’ previous and
present state of health. The infant’s interaction with the parents and normal
activity were observed, and the development of the child was assessed. A
thorough somatic examination of the child was also performed. Information
about demographic variables, perceptions of parenting and infant
temperament, life events and social support was collected in a questionnaire
that the mothers filled in after the home visit. The following week the parents
kept a special Sleep Diary of the sleep of their child. This diary was brought
to the special CHC center where the parents of the children in the case group
received advice, counselling and support in the form of a behavioural training
programme, in order to overcome the sleep problems of their child. The sleep
programme was carried out as detailed later. The paediatrician was of course
aware of the group status of the families visited. In order to reduce the
possible influence of this, the assessments of the psychosocial problems were
compared with data from the CHC and the medical records of all the children.
This was done by two independent assistants who were blind to infant group
status.
One month after inclusion in the study the parents in the problem group were
sent another 7-day sleep diary and a general questionnaire about their opinion
of the help received. At one year, two and a half years and five years,
respectively, from inclusion, contact was made by mail, and a questionnaire
and sleep diary were filled in by the parents of both the problem group and
the control group. For ethical reasons the study design did not include any
placebo intervention group (i.e. untreated children in the problem group), as
26
studies of behavioural programmes have shown high rates of improvement
(80-90 %) (5,63,97,101,118).
Questionnaires on sleep, family and infant characteristics, and
sleep diaries
The home visit covered questions about sleeping characteristics and the state
of health of the family and comprised open-ended questions, scored on
yes/no, 3-step or 5-step response scales. Sleep characteristics were covered in
five questions that allowed a classification of the child’s sleep
pattern/problem according to the definitions of ICSD, 1990, in a 24-hour
recall of the infant’s sleep, and questions about the circumstances surrounding
getting the child to sleep. The following week the parents filled in a special
Sleep Diary of the sleep of their child in which the amount of night and
daytime sleep was recorded. In addition information was recorded about clock
time into bed, sleep latency, settling time, arousals (time and length), morning
wake time, in bed awake – and out of bed time, and day time naps (time and
length). All data were measured in minutes. Parental and sibling sleep
problems during infancy were also probed. In order to assess the infant’s
general development, the procedure used at the CHC was employed (National
Board of Health and Welfare, 1991), including an assessment of gross and
fine motor skills, as well as language, social, cognitive, and neurological
development. Development was rated on 5-step scales ranging from very late
for age to well above chronological age level.
The health status of the family was addressed by two questions about medical
pregnancy and delivery complications, and by four concerning the family’s
contact with medical care and health status during the infant’s lifetime.
Answers to questions about health were supplemented with information from
medical records.

27
Assessment of the psychosocial situation of the family was based on self-
disclosure during the medical interview (e.g. reports of unemployment,
financial restraints, conflicts between the infant’s parents, conflicts with the
infant’s grandparents, family health problems, substance abuse). Psychosocial
problems were rated by the author as none, minor or major. In order to reduce
the possible influence of the authors´ knowledge of the group status of the
child, the assessments of psychosocial problems were compared with data
from the CHC and medical records. This was done by two independent
assistants who were blind to infant group status. The findings showed an
interrater correlation of r = 0.95 when one assistant’s ratings of the listed
observations of the paediatrician (author) was compared with the other
assistant’s ratings of data from the CHC and medical records. The interrater
correlation between the author’s ratings and the assistant’s ratings was
r = 0.98.
Information about family demographic variables (ethnicity, age and
education, employment, housing and financial situation, and number of
children) was gathered by a questionnaire mothers completed after the home
visit. Maternal perceptions of parenting were obtained through semi-
structured questions scored by mothers on 5-step response scales. The
inventory, a revised Swedish version of R. Abidin´s Parenting Stress Index
(PSI; Abidin, 1990) (2,74,130), contained 34 items in 5 subscales that focused
on parental feelings of competence/incompetence, restriction by parental role,
social isolation, spouse relationship problems, and health problems.
To measure infant temperament, the Baby Behaviour Questionnaire (BBQ)
and the Toddler Behaviour Questionnaire (TBQ) (54-55) were used. In the
methodological work with the TBQ, a construct corresponding to difficultness
has been developed, consisting of low manageability as the most important

28
characteristic. This construct, based on 5-step response scales, was used in the
present study.
The occurrence of infants’ problematic behaviour during the previous month
was reported by mothers in the home interview. Questions in the interview
were related to sleeping habits, thumb or dummy sucking, screaming and
whining, shyness, activity, restlessness and lack of concentration, temper
tantrums and the mothers’ perception of the child as troublesome, difficult to
handle. Maternal ratings on 2-point response scales (yes, no) were used.
Treatment programme
The methods used were based on the following premise which was explained
to parents: "During the night all children have some spells of light sleep
during which they easily wake. The problem is not that the child wakes up but
that it cannot slip back to sleep without the help of a parent rocking or feeding
it. The way the baby is settled to sleep in the evening will be its preferred way
of returning to sleep after natural wakings. In order to have a child that returns
to sleep by itself, you have to accustom it to settle on its own".
The programme included:
Controlled crying
Controlled crying, or more positively called controlled comforting, implies
that the parent spends a few minutes settling the child, then leaves it for
gradually increasing lengths of time with brief and warm, but firm,
reassurance and resettling in between, yet avoiding taking the child out of its
cot. No feeding is given, and the child should be drowsy but still awake when
put into bed. The intervals between reassurance increase from initially one
minute up to five minutes at most. This procedure was used (if needed) every
29
time the baby was settled by day or night, and whenever it woke and cried at
night. Consistency was emphasized. A nurse and a child psychologist
supported the parents by daily telephone calls for 1-2 weeks and then tried to
help them to develop confidence in the programme and to manage on their
own.
Day and night routines
Overtired babies do not sleep well at night. Two daytime sleeps of about 1-1½
hours were encouraged, together with a regular pattern of feeds, play times
(with plenty of parental involvement) and sleep. The precise times could be
varied somewhat to fit in with each family situation, but it was important to
ensure that feeds and sleep were separated.
General help and information were given as appropriate, e.g. about nutrition,
feeding practices and play techniques. The great range of normal behaviour
and development was discussed with the parents.
Parents were encouraged to be agreed about the programme management and
to find ways to get support and time out for themselves in order to maintain
the energy needed to care for a baby or toddler. Problems such as relationship
stresses, social problems, depressive moods and parental health problems
were addressed if appropriate.
Medication
Five children with deeply depressed and exhausted parents were given
sedatives (alimemazine) for two weeks at the beginning of the programme, in
combination with the behavioural programme, in order for the parents to be
able to sleep directly and thereby regain some mental strength.

30
Study IV
A screening procedure for ADHD was carried out 4.5 to 5 years after
inclusion in the study, when the children had reached the age of 5.5 years. In
case of screen posivity, further assessment methods were used to diagnose
ADHD.
Screening instrument for ADHD
The screening procedures were identical for all children in the study and
comprised the following:
(i) a Parent Psychomotor Questionnaire (PPQ) containing four questions
pertaining to the child’s psychomotor development for completion by parents
and rated on a scale of normal/abnormal (95).
(ii) a previously validated Preschool Questionnaire (PSQ) comprising six
items pertaining to the child’s attentional, motor, language and perceptual-
conceptual capacity for completion by the preschool teacher and rated on a
scale of normal/abnormal (96).
(iii) a motor examination, performed by a nurse who had received special
training. The examination was carried out at the CHC, according to a
standardized screening of motor abilities that comprised six items rated on a
scale of normal/abnormal (48).
The screening procedures were in accordance with the battery recommended
by the Swedish National Board of Health and Welfare for screening for minor
neurodevelopmental/psychiatric disorders in preschool children at the CHCs
(72,96).
31
The criteria for screen positivity were: (a) one or more abnormal scores on
either the PPQ or the PSQ in combination with one or two abnormalities on
the motor examination or (b) three abnormalities on the motor examination.
Children not fulfilling these criteria in the screening procedure were
considered screen-negative. The criteria for screen-positivity were chosen so
as to identify children with ADHD as well as those with other
neurodevelopmental and neuropsychiatric problems (72).
The screening methods used in this study have been psychometrically
examined in previous Swedish studies (45,48,50,96) and have been found to
have good inter-rater and test-retest reliability.
Assessment methods
The assessment methods used for diagnosis comprised a detailed history,
psychiatric and neurodevelopmental examination, neuropsychological
assessment and speech/language evaluation.
The first assessment was performed by the local multidisciplinary district
CHC teams including the local psychologists, speech therapists,
physiotherapists and paediatricians outside the original sleep study
organization. Those teams were thus unaware of the group status of the
children examined. The psychological examination included an assessment of
development with Griffiths´ Developmental Scale II (52) in addition to a
detailed history and a clinical neuropsychological assessment of symptoms of
inattention, hyperactivity, impulsivity and behavioural problems. The speech
therapists used clinically accepted assessment methods of language
comprehension, phonological and grammatical problems, and the
physiotherapists administered the Scandinavian motor-perceptual scale MPU
32
(57). The local paediatrician performed a paediatric physical examination of
the child with the focus on neurological functioning.
The second examining paediatrician with special training in child
neuropsychiatry (author M.T.) was unaware of the results of the previous
assessment performed by the local team members while performing the
second step in the assessment procedure, a home visit.
A medical, developmental and behavioural history was taken at a home
interview with the parents, using a standardized interview schedule. The
criteria for ADHD according to the DSM-IV were checked during this
interview, and each criterion was rated as 'definitively met', 'possibly met' or
'not met'. Inter-rater reliability of results obtained at this type of ADHD
interview is excellent (72).
Routine paediatric psychical examination and a brief neurodevelopmental
examination in accordance with the method outlined by Gillberg et al. (48)
were also performed at the home visit. Inter-rater reliability for this
standardised assessment is good to excellent with values of Pearson r ranging
from 0.68 to 1.00 for individual items (50).
Diagnosis
A comprehensive diagnosis was made in each case after all neuropsychiatric
assessments had been completed on the basis of the available information.
The diagnosis ADHD was set in children meeting the criteria for this
diagnosis of the DSM-IV (Box 1).

33
Statistics
For analysis of the data, the statistical program SAS (113) was used in all
studies. Group comparisons for dichotomous variables were executed with
Chi-square analyses or Fisher’s exact test (two-tailed) when an expected cell
value was less than 5. For variables with 3-,5- or 7-step response scales,
comparisons were made with t-tests. In group comparisons, the more
conservative alpha level of 0.01 was used because of the large number of
tests.
RESULTS
Prevalence and classification of sleep problems (Study I)Sleep problems: Descriptive dataPrevious sleep problems, irrespective of duration or type, were reported for
48.3 % of the total child population. At the time of inquiry, 40.8 % of the
children were reported to have episodes of evening sleep refusal, including
minor and transient problems. The sleep refusal was considered a severe or
very severe problem by 3.8 % of the parents.
With respect to night-waking, 62.3 % of the children had current problems,
irrespective of severity and duration. The night-wakings were considered a
severe or very severe problem by 5.6 % of the families.
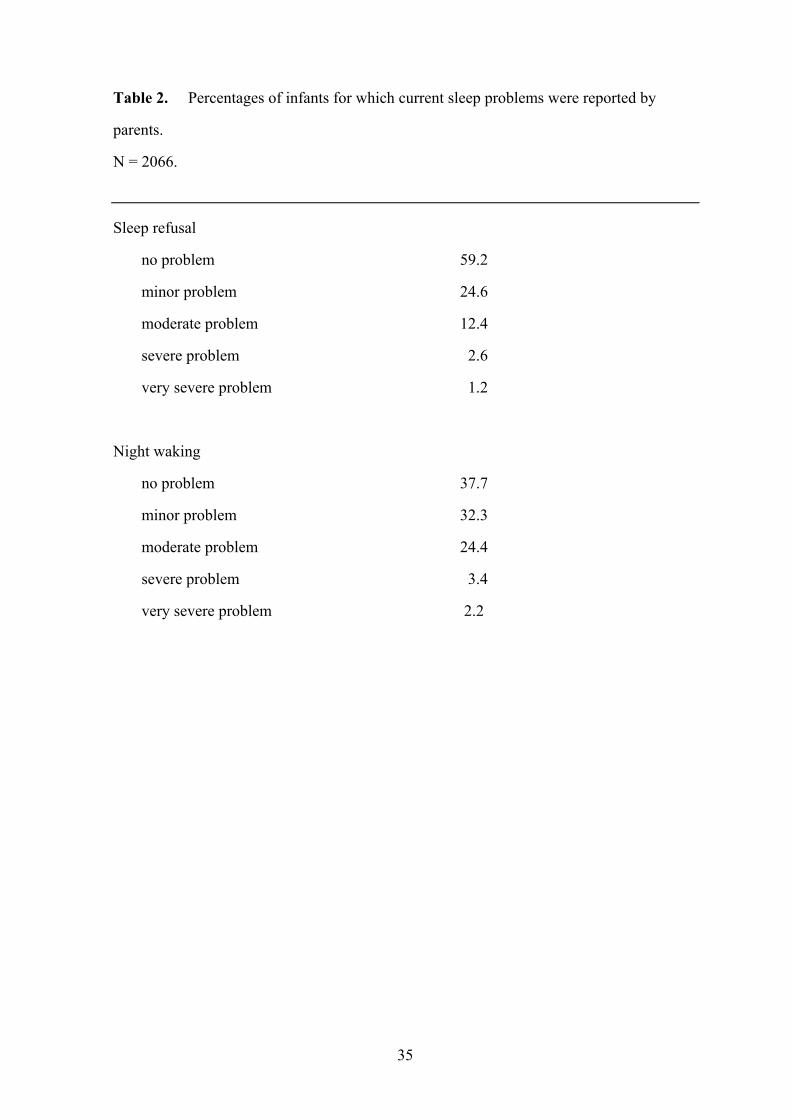
Table 2 gives descriptive data for sleep refusal and night-waking problems
measured with parental rating scales. Table 1 gives descriptive data classified
according to the operational definitions of ICSD. The frequency of severe
sleep refusal and severe night-waking problems in the total child population
varied between 3.8 % and 6.2 % in these measurements, with the parents

34
being slightly more tolerant in their judgement and opinions than the ICSD
scales.
Table 1. Percentages of infants that fulfilled the ICSD criteria of severe sleep refusal
(limit-setting sleep disordera) and severe nightwaking problems (sleep-onset association
disorderb).
_________________________________________________________________________
Ages 6-12 months, N = 1048 Ages 13-20 months, N = 1018
Totc Chronicd Totc Chronicd
_________________________________________________________________________
Severe sleep refusal 4.9 3.2 3.1 2.2
Severe night waking
problems 8.6 2.7 3.8 2.6
_________________________________________________________________________
Note: More than one problem can be reported for a child.
a) The ICSD criteria of severe limit-setting sleep disorder require five or more episodes per night of
stalling, calling out or leaving the bedroom.
b) The ICSD criteria of severe sleep-onset association disorder require a prolonged sleep latency and over
three nightly wakings, or two or three wakings each lasting over 10 minutes or one lasting over 15
minutes. The awakenings occur at least five nights per week.
c) Percentages of children for which problems were reported.
d) Proportion of children with chronic problems.
Chronic sleep refusal (limit-setting sleep disorder) requires a duration of 3 months or longer. Chronic
night-waking problems (sleep-onset association disorder) require a duration of 6 months or longer.
35
Table 2. Percentages of infants for which current sleep problems were reported by
parents.
N = 2066.
Sleep refusal
no problem 59.2
minor problem 24.6
moderate problem 12.4
severe problem 2.6
very severe problem 1.2
Night waking
no problem 37.7
minor problem 32.3
moderate problem 24.4
severe problem 3.4
very severe problem 2.2

36
Family and infant characteristics associated with severeinfant sleep problems (studies I and II)
Comparison of severe sleep problem group (N = 129) with a
control group (N = 1937) (Study I).
Sex, siblings, age distribution, pregnancy and delivery
There were more boys in the problem group (60 %) compared with controls
(51 %)
(X2 (1, N=2066) = 4.01, p < 0.05). No significant difference was found for the
presence of siblings. The age distribution of children in the problem group
was uneven, with an overrepresentation of children aged 8, 9 and 10 months
(42%) compared with controls (26%)(X2 (1, N=2066) =15.09, p <0.001).
There were no significant group differences in prematurity or birthweight.
Family sleep problems
No significant group differences were found concerning previous childhood
sleep problems within the family (mother, father and siblings analyzed
separately). In the problem group 12 % of the mothers, 10 % of the fathers
and 27 % of the siblings were reported to have had sleep problems in the first
years of life. Corresponding figures among controls were 10.8 and 23 %,
respectively.
Parental behaviour
Significant group differences were found concerning kinds of parental
intervention when the child refused to go to bed in the evening and when the
child needed to go back to sleep after waking up in the night. In the problem
37
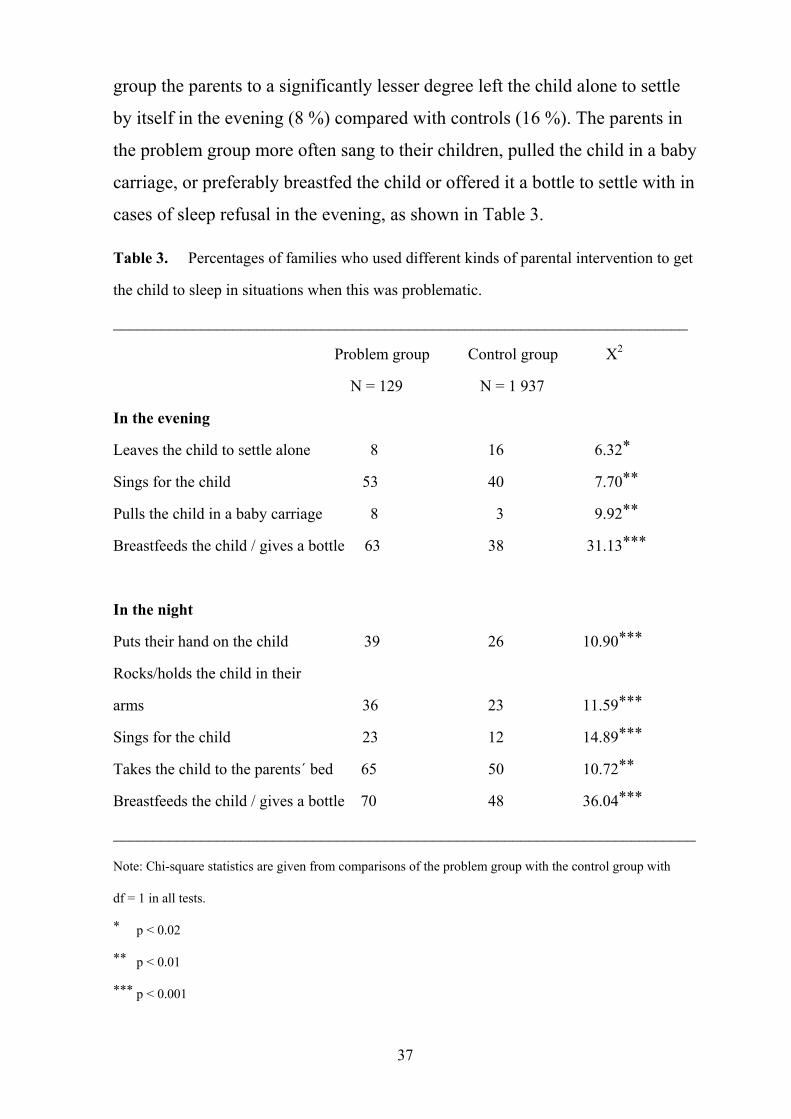
group the parents to a significantly lesser degree left the child alone to settle
by itself in the evening (8 %) compared with controls (16 %). The parents in
the problem group more often sang to their children, pulled the child in a baby
carriage, or preferably breastfed the child or offered it a bottle to settle with in
cases of sleep refusal in the evening, as shown in Table 3.
Table 3. Percentages of families who used different kinds of parental intervention to get
the child to sleep in situations when this was problematic.
________________________________________________________________________
Problem group Control group X2
N = 129 N = 1 937
In the evening
Leaves the child to settle alone 8 16 6.32*
Sings for the child 53 40 7.70**
Pulls the child in a baby carriage 8 3 9.92**
Breastfeeds the child / gives a bottle 63 38 31.13***
In the night
Puts their hand on the child 39 26 10.90***
Rocks/holds the child in their
arms 36 23 11.59***
Sings for the child 23 12 14.89***
Takes the child to the parents´ bed 65 50 10.72**
Breastfeeds the child / gives a bottle 70 48 36.04***
_________________________________________________________________________
Note: Chi-square statistics are given from comparisons of the problem group with the control group with
df = 1 in all tests.
* p < 0.02
** p < 0.01
*** p < 0.001

38
During the night the parents in the problem group also intervened more than
the control group parents in situations when the child woke up and needed to
go back to sleep. Table 3 shows significant group differences in the following
interventions: putting parents’ hand on the child, rocking/holding the child in
parents’ arms, singing for the child, taking the child to the parents’ bed and,
above all, breastfeeding the child or giving the child a bottle.
Feeding problems
Feeding problems were defined here as difficulties in eating solids, with
refusal and preference for breast-milk or formula. Comparisons of the group
with severe sleep problems and the control group revealed significant
differences. Feeding problems were reported for 33 % of the problem group
compared with 15 % of the controls
(X2 (1, N = 2 066) = 29.33, p < 0.001), and 18 % of the problem group
parents reported themselves as being in current need of help with the feeding
problem of their child, compared with 6 % of the control parents (X2 (1, N =
2 066) = 25.03, p < 0.001).
Health
Comparisons of the presence of eczema, allergy and nutritional intolerance
between the problem group and the control group showed no significant
differences. Neither could any differences be found concerning frequency of
occurrence of diarrhoea, constipation, colds, otitis or fever. However, more
worries and anxiety concerning infant health were reported in the problem
group than in the control group. Although there was no difference in the
frequency of colds or ear infections between the groups, the parents of the
affected children in the problem group were significantly more worried over
the diseases than were corresponding control parents: colds t (df=125) = 3.37,
p < 0.001; otitis t (df = 551) = 3.69, p < 0.001.

39
In this study severe sleep problems were found to be correlated with parental
worries and anxiety concerning infant health (although the children were
reported as being as healthy as the controls), infant feeding problems and
intensive parental interventional behaviour (especially feeding) during the
evening and night. A common factor of insecurity in the parental role is
suggested.
Comparison of severe and chronic infant sleep problem group (N
= 27) with a control group (N = 27) (Study II)
Sleeping characteristics
More case infants were breastfed (59 %) than were controls (15 %) (X2 (1, N
= 54) = 11.44, p < 0.001). Most case infants (78 %) were fed immediately
before going to sleep, whereas this was true for only 37 % of the controls (X2
(1, N = 54) = 9.16, p < 0.01).
Feeding was used by the parents of case children as a method of getting the
child to sleep. Consequently most case infants (18 out of 27,67 %) fell asleep
in the arms of their mother, whereas most of the control children fell asleep
alone in their own beds (16 out of 27,59 %). These differences, however,
were not significant.
During the night most of the case infants (56 %) slept in their parents’ bed
(co-sleeping), whereas this was very uncommon among controls. Only one of
the control children slept in the parents’ bed; the remaining control children,
26 out of 27 (96 %), slept in their own bed (X2, (1, N = 54) = 17.41, p <
0.001). Frequent night meals (5 meals or more) were given to 44 % of the
case infants. This pattern was not seen in any of the control children. The
majority of the controls (63 %) was not fed at all during the night.

40
Evaluation of sleep data (except that polysomnographic monitoring was not
used in this study) showed that 22 of 27 children in the problem group had a
sleep pattern consistent with the diagnosis, nocturnal eating (drinking)
syndrome. Four children in the problem group fulfilled criteria of sleep-onset
association disorder, and one child exhibited a sleep pattern characteristic of
schedule disorder.
Significant group differences were found concerning the childrens’ sleeping
time during the night based on a 7-day parental report in the form of a
detailed Sleep Diary (Table 4).
The case children’s mean sleeping time during the night was one and a half
hours less than that of the controls, and the case infant group woke up
significantly more often. A tendency towards group difference was also seen
concerning the children’s sleeping time during the day, with the case children
taking shorter day time naps. Over a 24-hour period the mean sleeping time
for the case children group was two hours less than that of the control group.
Table 4. Results from analyses of variance with means and standard deviations for
sleeping characteristics.
Cases (N = 27) Controls (N = 27)
M Sd M Sd p value*
Night-time sleep (in minutes) 557.7 78.78 647.6 45.36 0.0001
Number of night wakings 6.0 3.01 0.7 0.78 0.0001
Night time awake(length of arousal time atnight in minutes) 71.8 37.39 8.5 9.73 0.0001
Daytime sleep (in minutes) 107.6 61.11 138.1 43.60 0.0400
Sleep latency at bedtime 30.0 32.67 10.6 6.85 0.0053
Total sleep during a 24-hourperiod 665.3 91.54 785.7 47.42 0.0001
* p value from t-tests
41
The clock time into bed did not differ between the case and the control group,
but the sleep latency period was longer and, consequently, the settling time
later in the case group compared with the controls. No significant group
difference was found concerning morning wake time.
Previous sleeping problems in the family were more common among case
families (67 %) than among controls (7%) (X2 (1, N = 54) = 20.33,
p < 0.001).
Demographic characteristics
All mothers, except three in the case group and one in the control group, lived
with the
infant’s father. A significant difference was found with respect to parents’
ethnic origin
(X2 (1, N = 54) = 7.48, p <0.01); a higher proportion of case infants had a
non-Swedish parent. Even more uneven was the proportion of non-European
parents in the groups; 37 %
of the case children had one (7 %) or both (30 %) parents who originated
from a non-European country (Africa, South-America, Asia), whereas this
was true for only 4 % of the controls (X2 (1, N = 54) = 9.24, p < 0.01).
During the same time as this study was made, data were presented from the
Swedish Central Bureau of Statistics (SCB), in which Uppsala, where our
study was performed, was divided into areas of high, medium, and low-
income structure, based on family income. The majority of the case children
lived in low income areas, and a significant group difference was found
concerning family income, with financial problems reported in 48 % of the
case families compared to 11 % of the controls (X2 (1, N = 54) = 8.88,
42
p <0.01). Regarding housing conditions, the majority, 81 %, of the children
with sleep problems lived in blocks of flats as did the majority of the controls,
59 %. However, 37 % of the control children lived in a detached house in
residential districts compared with 11 % of the cases. This difference in
housing conditions was, however, not significant.
No significant differences between cases and controls were obtained for the
other demographic characteristics.
Health characteristics
A significant group difference was found concerning the psychosocial
situation in the family; case families had more psychosocial problems than the
control group. Comparisons of other variables related to somatic health in the
family and of infant development revealed no significant findings. Chi-square
analyses showed no significant differences in pregnancy and delivery
complications.
The parents of the case children reported symptoms related to chronic loss of
sleep with extreme tiredness and lack of energy (81 %). Feelings of
hopelessness, restlessness, inability to relax and irritation were common.
Many parents also reported sadness and crying and a sense of being close to
mental breakdown. Somatic and psychosomatic complaints were very
frequent (59 %) among parents of case children, such as headaches, pains in
shoulders and back or "the whole body", vertigo and dizziness, heart-
palpitation, fainting fits and loss of weight. Sexual problems were common
(33 %).
The parents of case children suffered from exhaustion, both physically and
mentally, and 11 case mothers (41 %) fulfilled the ICD-10-criteria for a
severe depressive episode. None of them had sought psychiatric help. Fifty-

43
two per cent of the case mothers reported feelings of guilt in relation to their
child, compared with 11 % of the controls
(X2 (1, N = 54) = 10.39, p <0.01). The pattern of interaction with the child
was affected, and 78 % of the case mothers reported feeling that the locus of
control of the situation and interaction was in their child. This feeling of being
controlled by the child was very uncommon in the control group, 11 % (X2 (1,
N = 54) = 24.30, p <0.001).
Although depressed and in expressed need of help, only 20 of the 27 case
parents (74 %) had asked for help at the Child Health Center. In the parent
questionnaire population study, the corresponding figure was 93 % among
parents who had experienced any sleep problem, including minor and
transient in their children. The reasons why the parents of the children with
the most serious sleep problems did not seek help were reported by them to be
difficulties with language, lack of energy and a sense of guilt that the sleep
problem of their child was their own fault.
Perceptions of parenting
Maternal perceptions of parenting differed significantly between groups.
Mothers of case infants had less positive perceptions of parenting and
experienced more parental stress, in particular feelings of incompetence and
restriction by the parental role, as well as perceived health problems.
Infant difficultness and problematic behaviours
Comparisons between case and control infants regarding difficultness and
problematic behaviours showed a significant group difference for
temperamental difficultness. Regarding problematic behaviours, a significant
group effect was found; cases had more problems than the control group. In

44
the assessment of the development of the children the paediatrician also rated
their activity level. More case infants were rated as very active (30 %)
compared with controls (0 %) (X2 (1, N = 54) = 9.39, p <0.01).
Independent ratings by the mothers revealed the same group difference; more
case infants were rated as very active (52 %) than were controls (0 %) (X2 (1,
N = 54) = 18.90, p <0.001.
Infants with severe and chronic sleep problems thus showed normal health
and general development, and had a normal growth pattern. Early severe sleep
problems were, however, found to be associated with a higher incidence of
breast-feeding, frequent
night meals as a method of putting the infant back to sleep, co-sleeping, and
previous sleeping problems in the family. They were also associated with
non-European origin, living in a low income area and with psychosocial
problems in the family, including financial problems, exhaustion and
depression in the mother, less positive perceptions of parenting and more
parental stress. There were also feelings of incompetence and restriction by
the parental role, as well as perceived health problems. An association with
infant difficultness, high activity and problematic behaviours was found.
Short-term and long-term outcome of an
interdisciplinary sleep treatment programme (Study III
and V)
Three sets of parents found that they could not agree with the premise on
which the programme was based, and therefore chose to leave the programme
without even trying it. Their children were reported to have unchanged severe
sleep problems one month later.

45
At the evaluation one month after the treatment programme had been initiated
in the 24 motivated families, significant changes had taken place. The average
number of times the babies woke up had decreased from 6.0 to 1.8 times per
night and night-time sleep had increased by an average of 67 minutes
(Table 5). The difference in total sleep during a 24-hour period between the
problem group and the control group had been reduced by 55 %, and the
difference in night-time sleep between the two groups had been reduced by
75 %. Ninety-two percent of the parents reported their children to have a good
sleep after treatment and were satisfied with advice and support. The sleep
pattern remained unchanged for two of the 24 problem children treated, and
no child had exaggerated sleep problems after treatment.
Table 5. Results from analyses of variance with means and standard deviations for
sleeping characteristics in the problem group, before and after treatment. N = 24.
Before treatment After treatment
M Sd M Sd p-value*
Night-time sleep (in minutes) 557.6 82.39 625.5 80.31 0.0059
Number of night wakings 6.0 3.17 1.8 1.48 0.0001
Night time awake (lengthof arousal time at night in minutes) 76.2 37.13 22.6 25.75 0.0001
Daytime sleep (in minutes) 102.5 60.66 106.1 39.44 NS
Total sleep during a 24-hourperiod 660.1 95.92 731.5 79.58 0.0074
*p value from t-tests

46
One year after the accomplishment of the sleep programme, the previous
problem group still had a good sleep. No significant differences were found
between the sleep duration of the formerly sleep-disturbed children and their
controls.
The follow-up after two and a half years showed no significant group
differences. The former problem group still slept as well as the controls.
Thus the changes were stable over time. The families in the case group also
managed to maintain the achieved changes in infant sleep behaviour on their
own; continuous therapist support was not necessary. This was true even for
formerly depressed and psychosocially burdened parents.
Five years after the initial contact the former problem group still slept as well
as the controls according to the parental ratings of sleeping characteristics
(Table 6). Concerning sleeping behaviour there was a tendency for the case
group to be judged by their parents to move more and be more restless during
sleep than were the controls. For the children in the problem group that at the
age of 5.5 years fulfilled the criteria for the diagnosis of attention-
deficit/hyperactivity disorder, this group difference in nocturnal restlessness
and movements reached significance (p < 0.0001). With respect to the
remaining sleeping behaviours as well as sleeping characteristics, the children
with ADHD as a group did not differ from the controls.

47
Table 6. Results from analyses of variance with means and standard deviations for
sleeping characteristics and behaviour during sleep, five years after initial contact
Cases (N = 24) Controls (N = 26)
M Sd M Sd p value*
Night-time sleep (in minutes) 628.8 56.08 639.5 43.79 NS
Number of night wakings 0.5 0.67 0.3 0.46 NS
Night time awake (length ofarousal time at night in minutes) 4.7 8.10 1.2 2.10 NS
Daytime sleep (in minutes) 0.0 0.00 0.0 0.00 NS**
Total sleep during a 24-hourperiod 628.8 56.08 639.5 43.79 NS
Behaviour (5-step scales): Cases (N = 24) Controls (N = 107)
Snoring or breathing
difficulties during sleep 0.3 0.45 0.5 0.92 NS
Head banging 0.2 0.65 0.0 0.23 NS
Restless movements 1.2 1.34 0.4 0.63 0.0123
Nightmares 0.7 0.65 0.5 0.50 NS
Sleep terrors (Pavor Nocturnus) 0.3 0.54 0.1 0.36 NS
Sleep walking (Somnambulism) 0.2 0.67 0.1 0.36 NS
Sleep talking (Somniloquy) 0.8 0.83 0.5 0.54 NS
Tooth grinding (Sleep Bruxism) 0.3 0.78 0.5 0.94 NS
Bedwetting 0.8 1.39 0.3 0.77 NS
Anxiety in the settling situation 0.1 0.29 0.1 0.41 NS
Protests against going to bed 1.0 1.41 0.5 0.71 NS
* p value from t-tests
** All values are the same for one class level

48
Factors associated with subsequent development of
attention-deficit/hyperactivity disorder (Study IV)
Of the 27 children with previously severe sleep problems in infancy (cases),
25 participated in the screening procedure for ADHD. Two families had
moved (returned to their home countries). Eight children in this group were
screen-positive and went further to assessment. Of those, one child did not
qualify for any diagnosis of neurodevelop-mental/neuropsychiatric disorder.
The rest, seven children in the former sleep problem group, met the criteria
for ADHD. Five of those children also had additional motor-perceptual
problems including gross motor, fine motor, perceptual and speech/language
dysfunction. Severe behavioural problems, dominated by conduct problems,
were seen in three of the children. One of the children was diagnosed by the
district paediatrician and the local CHC team before the screening study (at
4.5 years of age).
In the group of 27 control children, 25 agreed to participate in the general
screening. One family had moved and one refused to participate, referring to
lack of time.
One child among the controls was screen-positive but in the following
assessment procedure did not qualify for any diagnosis. To summarize, seven
of the former sleep problem children met the criteria for the diagnosis of
ADHD, compared with no child in the control group.
The diagnosis ADHD was thus significantly more prevalent in children who
previously had severe infant sleep problems than among the controls, 7/25
versus 0/25 (p < 0.01).
Factors associated with later development of ADHD in children with severe
infant sleep problems were sought by comparing infant data of those children
in the sleep problem group that later developed ADHD (N = 7) with infant
49
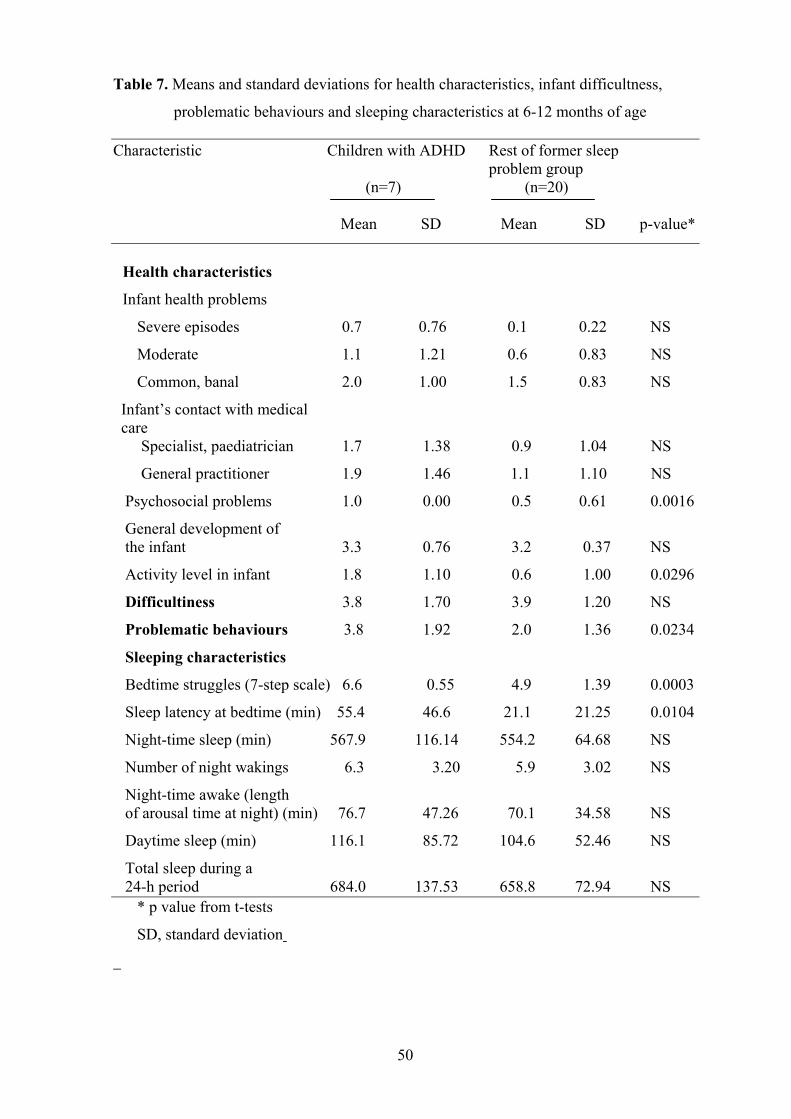
data from the rest of the problem group (N=20). Given severe sleep problems
in infancy, the following characteristics were associated with later diagnosis
of ADHD; psychosocial problems in the family, behavioural problems at
settling time (bedtime struggles) and a long sleep latency at bedtime (Table 7
and 8). There was also a tendency towards more behavioural problems during
daytime (problematic behaviours) in infancy, according to parental ratings
four and a half to five years earlier, in the children that later met the criteria
for ADHD. These children also tended to have been rated by the paediatrician
as very active as infants (Table 7).
50
Table 7. Means and standard deviations for health characteristics, infant difficultness,
problematic behaviours and sleeping characteristics at 6-12 months of age
Characteristic Children with ADHD Rest of former sleep problem group
(n=7) (n=20)
Mean SD Mean SD p-value*
Health characteristics
Infant health problems
Severe episodes 0.7 0.76 0.1 0.22 NS
Moderate 1.1 1.21 0.6 0.83 NS
Common, banal 2.0 1.00 1.5 0.83 NS
Infant’s contact with medical care Specialist, paediatrician 1.7 1.38 0.9 1.04 NS
General practitioner 1.9 1.46 1.1 1.10 NS
Psychosocial problems 1.0 0.00 0.5 0.61 0.0016
General development of the infant 3.3 0.76 3.2 0.37 NS
Activity level in infant 1.8 1.10 0.6 1.00 0.0296
Difficultiness 3.8 1.70 3.9 1.20 NS
Problematic behaviours 3.8 1.92 2.0 1.36 0.0234
Sleeping characteristics
Bedtime struggles (7-step scale) 6.6 0.55 4.9 1.39 0.0003
Sleep latency at bedtime (min) 55.4 46.6 21.1 21.25 0.0104
Night-time sleep (min) 567.9 116.14 554.2 64.68 NS
Number of night wakings 6.3 3.20 5.9 3.02 NS
Night-time awake (length of arousal time at night) (min) 76.7 47.26 70.1 34.58 NS
Daytime sleep (min) 116.1 85.72 104.6 52.46 NS
Total sleep during a 24-h period 684.0 137.53 658.8 72.94 NS * p value from t-tests
SD, standard deviation

51
Table 8. Number of families with different kinds of psychosocial problems when the child was 6-12 months old
Characteristic Children with ADHD Rest of former sleepproblem group
(n = 7) (n = 20)
Unemployment 2 0
Insecure employment 2 2
Single mother 2 1
Chronic disease/disablementin parent 2 2
Maternal depression 2 9
Serious family conflicts 2 4
Refugee status 3 2
Substance abuse 1 1
Previous assault andbattery against motherin the family 1 0
Father previously inprison 1 0 No psychosocial problem 0 11
Note: More than one problem can be reported per family
52
DISCUSSION
General discussion
Study I, performed on a large total community sample, confirms results from
other populations concerning the proportion of sleep problems as perceived
by parents
(20-22,67,69,92). The designation of infant sleep problems as an area of
major parental concern is obvious as parental reports showed that 16 % of the
infants aged between 6 and 18 months were judged to have moderate to
severe difficulties in falling asleep at night, and 30 % were reported to have
frequent night waking.
A core group of children with severe or even very severe sleep problems,
encompassing around 5 % of the population, could be identified in different
ways. About 4 % of the infants had sleep refusal problems that were
considered severe or very severe by parental rankings and by the more
operational definitions of ICSD. The corresponding figure for night-waking
problems was 6 %. Five per cent of the parents reported themselves as being
in current need of help.
Almost all parents had sought help at a CHC or more seldom at a paediatric
clinic. Only approximately half of the parents were satisfied with the help
obtained. Obviously something is lacking. Further studies of the interaction
between parents and professionals regarding sleep problems are needed in
order to determine the nature of the problem. Is there a problem in the
information provided, in the way it is provided, or are the parents’
expectations not in concordance with those of the profession? Further
research is urgent.

53
The delineation of factors associated with severe sleep problems was one of
the major aims of the study. Results both from study I and from study II
indicate that severe sleep problems are related to a number of factors. The
most striking factors associated with severe sleep problems in the parent
population study I were intensive parental interventional behaviour
(especially feeding) during the evening and night, parental worries and
anxiety concerning infant health (although their children were reported as
being as healthy as others) and infant feeding problems. The parents of the
children in the problem group seemed to be more insecure in their parental
role, a finding that was confirmed in study II. It is of course always difficult
to ascertain whether the behaviour of parents actually contributes to the
development of the sleep problem of the child or whether, because the child
acts in a particular way (will not settle or wakes and cries), the parents adopt
certain behaviours (eg rocking, feeding) to get the child to sleep. Works
undertaken by Kerr et al (68) in the area of prevention, however, support the
first view. Altering the parent’s behaviour in the early months of the child’s
life in a preventive study produced a statistically significant reduction in the
incidence of sleep problems in the intervention group when compared to a
control group at 9 months of age.
In study II, the closer study with in-depth interviews and examinations of the
sleep-disturbed infants, a number of factors associated with severe sleep
problems were found; characteristics of the child, of the parents and of their
psychological and social situation.
Infants with severe and chronic sleep problems showed normal health and
general development and had a normal growth pattern. Early severe sleep
problems were, however, found to be associated with a higher incidence of
breast-feeding, frequent night meals as a method of putting the infant back to
sleep, co-sleeping and previous sleeping problems in the family. They were
54
also associated with non-European origin, living in a low income area and
with psychosocial problems in the family, including financial problems,
exhaustion and depression in the mother, less positive perceptions of
parenting and more parental stress. There were also feelings of incompetence
and restriction by the parental role, and perceived health problems. An
association with infant difficultness, high activity and problematic behaviours
were found.
There are potential dependencies of certain of the demographic variables
(socio-economic status, ethnicity) and other variables (such as the rate of co-
sleeping, breastfeeding and nap frequency) which make it more difficult to
evaluate the contribution of each factor. However, we do not make any causal
conclusions but believe that it is of clinical importance for prevention and
early identification in child health care and clinical paediatric settings to be
able to point to and identify common patterns and risk conditions associated
with severe sleep problems.
Earlier findings were replicated in study II. More frequent night-waking has
been reported in breastfed infants, (3,9,26,40,71,89) and in children, most
often breastfed, who are given frequent nightmeals (3,89). An association
between co-sleeping all night and problems with bedtime struggles and night-
waking has also been reported by several studies (3,62,67,75-
77,86,98,114,125,129). Previous sleeping problems in the family have been
less investigated, and as an experienced researcher concluded: "little is known
about how variations in social expectations and norms are related to sleep
patterns or sleep problems" (100). A clear hereditary component is only
known in parasomniacs (64).
The association of sleep problems with psychosocial problems in the family,
including financial problems and overcrowding, is well known. (3)
Exhaustion (30) and depressive state, especially in the mother, have
previously been widely documented (73,76,98,129) as have less positive

55
perceptions of parenting (3,19,76). The parent-child interaction has been
studied, and oversensitivity to the signals of the child (20,89) as well as
insecurity in the parents have previously been found. Other contributors
include inadequate stimulation of the child, overanxiety, rigidity or
inconsistent handling from the parents (85) and health problems in the family
(76).
In recent years the temperament of the child has come into focus, and infant
temperamental difficultness in sleep problems has been documented,
(3,9,12,27,82,98-99) as well as problematic behaviour, (6,82,98,129). The
question of hyperactivity in the sleepless child is still controversial. It has
been stated that there is no convincing evidence that sleepless children in
general are hyperactive per se, and many of them "calm down" when their
parents change their attitudes and establish consistent routines (100). A core
group of true hyperactive children with sleep problems most certainly exists,
but in the majority of very active children, this activity level has been seen as
a consequence rather than a cause of their sleeplessness.
In study II we did not measure infant temperament before the sleep problem
started. This means that we cannot rule out the contribution of infants’
temperamental characteristics, and in study IV we later found that
approximately one in four children with severe sleep problems in infancy will
later qualify for the diagnosis of ADHD.
The results of study II are thus in line with earlier findings. What may be new
is the massive impact. Together, our results give a very complex, large-scale
picture of how the infant and family situation develops in cases of very severe
infant sleep problems. This is a picture in which multiple factors may amplify
each other in vicious circles. Characteristics of the child, of the parents and of
the situation may influence each other reciprocally. Of course there are
methodological limitations here. Interpretation of a multifactorial genesis of

56
the problem could not strictly be assigned from univariate analyses but a not
too improbable speculation is that when a vulnerable child with a
temperament characterized by difficultness, high activity, liveliness, a strong
will and stubbornness, and with heredity for difficulties in the regulation of
sleep and wakefulness, is born into a family with great psychosocial
problems, health difficulties or a tendency to depression in the parent(s), there
emerges a situation of excessive parental stress. Living in a foreign country,
with other child-rearing traditions and far away from relatives, as for the non-
European families (half of them refugees), adds even more stress to the
situation. The higher risk of sleep disturbances in children of first generation
immigrants, possibly due to a periodic effect of the stress of cultural change,
has recently been discussed by Rona et al (106). In such cases, the child’s
needs may exceed the parents’ capacity to meet them.
A feeling of insufficiency and insecurity in the parental role, desperation, and
finally depression, in the parent can be the result. The child, who probably
more than other children needs regularity and routines, is met instead by
resignation and easy solutions, such as pacifiers, on-demand breast-feeding
and co-sleeping. A chronic lack of sleep may be the result for the parents with
such consequences as extreme tiredness, physical and mental exhaustion,
irritability and relationship problems. For the child, there may be exaggerated
difficulties and behavioural problems that maintain the vicious circle.
Sleepless and depressed parents may have neither the energy to solve the
situation themselves nor an ability to grasp the situation and seek help.
Our study, with its very small drop-out rate, has identified an unselected
population of very difficult cases. Out of these, three quarters had
spontaneously sought help. The remaining quarter of the families had all
regularly visited their CHC for weight and length controls, and vaccinations,
but they had not mentioned the severe sleep problems of their child.

57
Thus, in order to discover the severe cases of sleep problems among infants
and young children, paediatricians and CHC need to actively ask parents
about the sleep of their children. Severe problems are otherwise
underreported.
In study III, infants with severe and chronic sleep problems showed
significant improvements in all night-time sleep characteristics after a
relatively short, but intensive and multi-disciplinary, intervention sleep
programme. The improvements proved to be stable over time, lasting the
whole follow-up period of five years. Continuous therapist support was not
necessary to maintain the changes in sleep behaviour. In fact no contact
between the special CHC team and the case families took place during the
follow-up period, besides the follow-up questionnaires and a few telephone
calls from three of the families.
Furthermore, earlier findings were replicated in this study. The benefits of a
brief behavioural intervention programme for improving sleep in infants and
young children have previously been documented (4,36,43,79,116,128). Of
course it cannot be ruled out that a gradual achievement of a normal sleep
pattern would have been the natural history for some of the children in the
problem group, even without treatment.
Controlled crying was only one part of the programme, but is perhaps the
most controversial one. It has been argued that leaving a child of this age to
cry for even short periods may affect its long-term feeling of security (117).
There is no support for this belief in our results. On the contrary, no case child
showed any signs of anxiety in the
settling situation one year after treatment, and the control children were more
prone to protest against going to bed than were the cases at the two-and-a-

58
half-year follow-up. However, further research on follow-ups of behavioural
sleep disturbances is needed.
Tendencies towards parasomnia (restless movements during sleep, head
banging, sleep walking) were seen in the case group at the follow-up at one
year but not at the two-and-a-half-year follow-up. After five years there was
only a slight tendency for the problem group to move more during sleep than
the controls. Further research will be necessary in order to determine whether
the infants with early sleep problems are more prone to develop true
parasomnia as they grow older than are the controls.
We believe the interdisciplinary approach in the clinical interventions to be
crucial (87,107). The whole family situation must be taken into consideration
(11) in order to overcome vicious circles of insecurity in the parental role,
feelings of insufficiency, desperation and, finally, depression. Given
understanding and the tools of a more secure way of parenting a child, the
majority of even heavily psychosocially burdened parents were able to
manage to help their child sleep well.
Validity of the results
The source of information is a crucial issue in the evaluation of sleep
disturbances in early childhood. The reliability and validity of parental reports
in the form of Sleep Diaries, the most common assessment instrument in
clinical practice, have been questioned in the literature. It has been stated that
parents might be unaware of many aspects of the sleep behaviour of their
infants during the night (6,108,111).
Consequently, a number of objective sleep measures have been employed,
including polysomnographic studies, pressure-sensitive mattresses, timelapse
video recordings and actigraphy (activity-based monitoring).
59
Results from studies comparing parental reports with objective sleep
measures (109) show that parents are acccurate reporters of sleep-schedule
measures such as sleep onset and sleep duration. They overestimate, however,
the time that their infants spend in actual sleep and underestimate the number
of their night wakings. According to that result, the short sleep duration and
many night wakings initially in our problem group should be regarded as a
minimum rather than be suspected of being an exaggeration by exhausted
parents. It could of course be argued that parents who co-sleep with their
children are likely to be aware of more night-time wakings than would parents
who sleep in different rooms. And since the parents in the problem group co-
slept with their children much more frequently than did parents in the control
group, one might suspect an artefact in reporting. However, the difference in
number of night wakings between the groups is very large, as is the difference
in length of reported time spent awake in the night. Even if an artefact cannot
be ruled out, it is not reasonable to believe it to have had a major impact on
the results.
The total community sample of 2 518 children, with a response rate of 83 %,
does not exhibit any known bias. Hence, results based on data from this
sample are assumed to be generalisable in children from similar
sociodemographic backgrounds, i.e. Scandinavian and probably North-
European larger cities.
Concerning reliability it has to be noted that strict alternative answers give
increased reliability but could be a threat to the validity by loss of
information. We tried to solve this dilemma by combining survey data with
interviews with both strict alternatives and open-ended questions.

60
The most controversial results in this thesis emerge in study IV, in which a
discussion of methodological issues is urgent. According to our results,
approximately one in four children with severe sleep problems in infancy will
later qualify for the diagnosis of ADHD. This is a figure which clearly
exceeds the estimated prevalence rate in this age group in a normal Swedish
population, 2.4-4 % (72). However, the small numbers of children involved in
the study, both at the screening and diagnostic stages, constitute an obvious
drawback. The small sample size limits the extent to which conclusions can
be drawn. We therefore regard our findings as preliminary and suggestive of a
need for larger-scale corroborative studies.
Nevertheless, even though numbers were small, the sample examined was
population-based and thus more likely to be representative of children with
severe infant sleep problems than most studies reporting on clinical case
series. Moreover, the drop-out rate at various stages of the study was very
small. The longitudinal prospective nature of the study is also an advantage.
Individual, family and social factors were associated with later development
of ADHD. Most striking were the associations with bedtime struggles and
psychosocial problems in the family. ADHD has been described as a
"biopsychosocial disorder", raising critical questions concerning the relations
between genetic, biological and environmental factors (122).
The findings that there were a number of family psychosocial problems
associated with the development of ADHD in infants with severe sleep
problems need a comment. It has been stated that parents of children with
ADHD have a high likelihood of ADHD themselves, and thus the family
dysfunction may be a by-product of the parents’ own adult type of ADHD-
related psychosocial difficulties.
61
What is then measured with the criteria of ADHD? Behaviour reflecting
genetic predisposition to a deviant functioning of the synapse–transmittor
system with difficulties in the regulation of sleep and wakefulness? Behaviour
reflecting psychosocial stress? Behaviour reflecting vulnerability and
difficultness in temperament? Potentially neuropathogenic events during the
pregnancy, perinatal and postnatal periods, which are known to be associated
with a heightened risk of development of ADHD (96), had been excluded
through the inclusion criteria. Again we return to the speculations in page 56.
And why do we see a positive development in sleep characteristics but not the
same concerning behaviour and development? This is an urgent task for
future research.
Conclusions and clinical implications
Sleep problems are a common parental concern during infancy, and many
parents seek advice and help from a CHC or paediatrician. Severe sleep
problems in infants and young children are complex problems with both
psychological and social factors involved, besides the strictly paediatric
issues. In addition, many families are not satisfied with the help they obtain
today. Even more serious, the severe cases are underreported by parents.
These findings have implications for the consultations at CHCs and for the
paediatric consultation in cases of severe sleep problems in infants and young
children. In order to discover the severe cases, health care personnel have to
actively ask parents about sleep problems. In addition to obtaining a thorough
history and making a complete medical examination of the child, physicians
also need to pay great attention to the situation of the parents, their worries,
and psychological and social conditions.

62
The possibility of a vicious circle developing deserves attention in clinical
interventions, which need to be interdisciplinary, taking the whole family
situation into consideration.
With a relatively short but intense treatment programme, combining
behavioural technique with family work, even severely sleep disturbed infants
and children, coming from families with depression and psychosocial
problems, can be helped to sleep well. Long-term improvements in sleep
pattern after the programme, extending over years, have been documented.
The results concerning the development of attention-deficit/hyperactivity
disorder call for heightened attentiveness and awareness among nurses and
doctors working with infants with sleep problems at CHCs and paediatric
clinics. Infant activity level, problematic behaviours and parent-infant
interaction have to be considered seriously, and both psychosocial,
behavioural and sleeping characteristics have to be taken into consideration.
Close follow-ups of children with combined severe and prolonged sleep,
activity and behavioural problems are recommended as neurodevelopmental
problems seem to be prevalent in this category of children.
63
ACKNOWLEDGEMENTS
The work reported in this thesis has been completed with the contribution of a
lot of individuals.
I wish to express my sincere gratitude to:
The parents and children who participated in the studies, for sharing their
experiences of life during the day and at night, and thus making this thesis
possible.
Professor Claes Sundelin, my supervisor, for excellent guidance in scientific
thinking, for generously sharing his knowledge and creating an ideal working
situation for me adapted to my needs, inspiring me and offering support and
advice from beginning to end in uncountable discussions.
Professor Jerker Hetta, my other supervisor, for expertise and advice in the
field of sleep research.
Colleages and friends at the Child Health Unit, Department of Women´s and
Children´s Health, Section for Pediatrics in Uppsala for comradeship and
generosity over the years.
Rut Magnusson for excellent secretarial assistance and personal support.
Monica Östberg, Margareta Dannaeus and Elisabet Hagelin, collegues at the
Special Child Health Center, for professional help in the sleep treatment
programme and Monica also in the work with Parental Stress Index, where
she generously shared her methods and data files with me.

64
Carina Lundin for patient and effective computer assistance.
Maurice Devenney for excellent English language service.
All nurses at the Child Health Centers (CHC) in Uppsala for their efforts and
important contributions to the work.
All paediatricians, psychologists, speech therapists and physiotherapists in the
local CHC teams for stimulating collaboration over the years.
My big family for loving care and support.
Financial support for this research was provided by grants from the Swedish
1st May Foundation and the Gillberg Foundation.

65
REFERENCES
1. Abe K, Ohta M, Amatomi M, Oda N. Persistance and predictive value of
behaviours of 3-year-olds: A follow-up study at 8 years. Acta Paedopsychiatrica
1982; 48:185-191.
2. Abidin RR. Parenting Stress Index (PSI)-Manual. Odessa FL: Psychological
Assessment Resources, Inc. 1990.
3. Adair R, Bauchner H. Sleep problems in childhood. Current Problems in Pediatrics
1993; 23(4):147-170.
4. Adair R, Zuckerman B, Bauchner H, Philipp B, Levenson S. Reducing night
waking in infancy: a primary care intervention. Pediatrics 1992; 89:585-588.
5. Adams L, Richert V. Reducing bedtime tantrums: Comparison between positive
routines and graduated extinction. Pediatrics 1989; 84:756-760.
6. Anders TF. Home recorded sleep in two and nine-month-old infants. Journal of the
Academy of Child Psychiatry 1978; 17:421-432.
7. Anders TF. Neurophysiological studies of sleep in infants and children. Journal of
Child Psychology and Psychiatry and Allied Disciplines 1982;23:75-83.
8. Anders TF, Eiben MS. Pediatric sleep disorder: a review of the past 10 years. J Am
Acad Child Adolesc Psychiatry 1997;36:9-20.
9. Anders TF, Keener MA. Sleepwake state development and disorders of sleep in
infants, children and adolescents. In Levine M, Carey W, Crocker A, Gross R.
Developmental – Behavioural Pediatrics. WB Saunders Company, Philadelphia,
USA.
10. Anders TF, Weinstein P. Sleep and its disorders in infants and children: A review.
Pediatrics 1972;50:312-324.

66
11. Armstrong KL, O´Danell H, McCallum R, Dadds M. Childhood sleep problems:
Association with prenatal factors and maternal distress/depression. J Paediatr-
Child-Health 1998; 34(3)263-266.
12. Atkinson E, Vetere A, Grayson K. Sleep disruption in young children. The
influence of temperament on the sleep patterns of pre-school children. Children
Care Health Dev 1995; 21(4):233-246.
13. Ball JD, Koloian B. Sleep patterns among ADHD children. Clinical Psychology
Review 1995; 15:681-691.
14. Ball JD, Tiernan M, Janusz J, Furr A. Sleep patterns among children with attention-
deficit/hyperactivity disorder: A reexamination of parent perceptions. Journal of
Pediatric Psychology 1997; 22(3):389-398.
15. Barkley RA, Mc Murrey MB, Edelbrock CS, Robbin K. Side effects of
methylphenidate in children with attention deficit hyperactivity disorder: a
systematic, placebo-controlled evaluation. Pediatrics 1990; 86:184-192.
16. Bartlett LB, Rooney V, Spedding S. Nocturnal difficulties in a population of
mentally handicapped children. British Journal of Medicine 1985;31:54-59.
17. Bax M. Sleep disurbance in the young child. British Medical Journal
1980;280:1177-1179.
18. Beltramini AV, Hertzig ME. Sleep and bedtime behaviour in preschool-aged
children. Pediatrics 1983;71:153-158.
19. Benoit D, Zeanah CH, Boucher C, Minde KK. Sleep disorders in early childhood:
association with insecure maternal attachment. Journal of Am Acad Child Adolesc
Psychiatry 1992;31:86-93.
20. Bernal JF. Night waking in infants during the first 14 months. Dev Med Child
Neurol 1973;15:760-769.

67
21. Bixler EO, Kales JD, Scharf MB, Kales A, Leo LA. Incidence of sleep disorders in
medical practice: A physician survey. Sleep Research 1976;6:62.
22. Blum NJ, Carey WB. Sleep problems among infants and young children. Pediatrics
in Review 1996;17(3):87-92.
23. Blurton-Jones N, Rosetti Ferreira MC, Farquar-Brown M, et al. The association
between perinatal factors and later night-waking. Developmental Medicine and
Child Neurology 1978;20:427-434.
24. Brouillette RT, Morielli A, Waters K. Establishing and running a pediatric sleep
laboratory. In: Loughlin G, Carroll J, Marcus C, ed. Sleep and Breathing in
Children. New York: Marcel Dekker, Inc, 2000;767-781.
25. Busby K, Firestone P, Pivik RT. Sleep patterns in hyperkinetic and normal
children. Sleep 1981; 4:366-383.
26. Carey W. Breastfeeding and night waking. Journal of Pediatrics 1975; 87:327-329.
27. Carey W. Night waking and temperament in infancy. J Pediatr 1974; 84:756-758.
28. Carskadon MA, Dement WC. Normal human sleep: an overview. In: Kryger M,
Roth T, Dement W, ed. Principles and practice of sleep medicine. Philadelphia:
W.B. Sounders Company, 1994:16-25.
29. Chatour I, Wells KC, Connors CK, Seidel WT, Shaw D. The effects of nocturnally
administered stimulant medication on EEG sleep and behaviour in hyperactive
childrens. Journal of the American Academy of Child Psychiatry 1984; 22:337-342.
30. Chavin W, Tinson S. Children with sleep difficulties. Health Visitor 1980;53:477-
480.
31. Choquet M, Facy F, Laurent F, et al. Les enfants à risque en âge préscolaire. Mise
en évidence par analyse topologique. Arch Fr Pediatr 1982;39:185-192.

68
32. Choquet M, Ledoux S. La valeur prognostique des indicateurs de risque précoces.
Etude longitudinale des enfants à risque à 3 ans. Arch fr pediatr 1985;42:541-546.
33. Clarkson S, Williams S, Silva PA. Sleep in middle childhood: a longitudinal study
of sleep problems in a large sample of Dunedin children aged 5-9 years. Aust
Paediatr J 1986;22:31-35.
34. Corkum P, Moldofsky H, Hogg-Johnson S, Humphries T, Tannock R. Sleep
problems in children with attention-deficit/hyperactivity disorder: Impact of
subtype, comorbidity and stimulant medication. J Am Acad Child Adolesc
Psychiatry 1999; 38(10):1285-1293.
35. Corkum P, Tannock R. Moldofsky H. Sleep disturbances in children with attention-
deficit/hyperactivity disorder. J Am Acad Child Adolesc. Psychiatry 1998;
37(6):637-646.
36. Cuthbertson J, Sackville S. Helping your child sleep through the night. Doubleday,
New York 1985.
37. Dahl R. The impact of inadequate sleep on children´s daytime cognitive function.
Seminars in Pediatric Neurology; 3(1):44-50.
38. Dahl R, Bernhisel-Broadbent J, Scanlon-Holdford S, Sampson H, Lugo M. Sleep
disturbances in children with atopic dermatitis. Arch Pediatr Adolesc Med
1995;149(8):856-860.
39. Dahl R, Puig-Antich J. Sleep disturbances in child and adolescent psychiatric
disorders. Pediatrician 1990; 17:32-37.
40. Daws D. Family relationships and infant feeling problems. Health Visit 1994; 67
(5):161-164.
41. Emde R, Walker S. Longitudinal study of infant sleep: Results of 14 subjects
studied at monthly intervals. Psychophysiology 1976;13:456-461.
69
42. Ferber R. Childhood Sleep Disorders. Neurologic Clinics 1996:14(3):493-511.
43. Ferber R. Sleep disorders in infants and children. In: Riley TL ed. Clinical Aspects
of Sleep and Sleep Disturbance. Butterworth Publications, Bostan 1985; 113-157.
44. Ferber R. The sleepless child. In Guilleminault C (eds) Sleep and its disorders in
children, 141-163. New York: Raven Press 1987.
45. Fernell E, Gillberg C, von Wendt L. Self-esteem in children with infantile
hydrocephalus and their siblings. Use of the Piers-Harris self-concept scale.
European Child and Adolescent Psychiatry 1992; 1:227-232.
46. France KG. Behaviour characteristics and security in sleep-disturbed infants treated
with extinction. J Ped Psychol 1992;17:467-475.
47. France KG, Hudson SM. Management of infant sleep disturbance: A review.
Clinical Psychology Review 1993;13(7):635-647.
48. Gillberg C, Carlström G, Rasmussen P, Waldenström E. Perceptual, motor and
attentional deficits in seven-year-old children. Neurological screening aspects. Acta
Paediatrica Scandinavica 1983; 72:119-124.
49. Gillberg C. Melander H, von Knorring A-L, Janols L-O, Thernlund G, Hägglöf B,
Eidevall-Wallin L, Gustafsson P, Kopp S. Long-term stimulant treatment of
children with attention-deficit hyperactivity disorder symptoms. A randomized,
double-blind, placebo-controlled trial. Arch Gen Psychiatry 1997; 54(9):857-864.
50. Gillberg IC, Winnergård I, Gillberg C. Screening methods, epidemiology and
evaluation of intervention in DAMP in preschool children. European Child and
Adolescent Psychiatry 1993; 2:121-135.
51. Green C. Toddler Taming. Doubleday, Sydney, Australia 1987.
52. Griffiths R. The abilities of babies. London: University of London Press. 1976.
70
53. Guilleminault C, Winkle R, Korobkin R, Simmons B. Children and nocturnal
snoring: evaluation of the effects of sleep related resistive load and daytime
functioning. European Journal of Pediatric, 1982; 139:165-171.
54. Hagekull B. The Baby and Toddler Questionnaires: empirical studies and
conceptual considerations. Scandinavian Journal of Psychology 1985; 26:110-122.
55. Hagekull B, Bohlin G. Individual stability in dimensions of infant behaviour. Infant
Behaviour and Development 1981; 4:97-108.
56. Haslam D. My child won´t sleep. Practitioner 1995; 239:730-732.
57. Holle B, Bönnelycke K, Kemp E, Thrane Mortensen L. Motorisk Perceptuell
Utveckling 0-7 år. Motor-Perceptual Development 0-7 years. Stockholm:
Psykologiförlaget. 1991 (in Swedish).
58. Jacob SV, Brouillette RT. Home monitoring of sleep and breathing in children. In:
Loughlin G, Carroll J, Marcus C, ed. Sleep and Breathing in Children. New York:
Marcel Dekker, Inc, 2000:783-795.
59. Jenkins S, Bax M, Hart H. Behaviour problems in preschool children. Journal of
Child Psychology and Psychiatry 1980;21:5-17.
60. Jenkins S, Owen C, Bax M, Hart H. Continuities of common behaviour problems in
preschool children. J Child Psychol Psychiatry 1984;25:75-89.
61. Jimmerson KR. Maternal, environmental and temperamental characteristics of
toddlers with and toddlers without sleep problems. Journal of Pediatric Health care
1991;5(2):71-77.
62. Johnson CM. Infant and toddler sleep: A telephone survey of parents in one
community. J Dev Pediatr 1991; 12:108-114.

71
63. Jones D, Verduyn C. Behavioural management of sleep problems. Archives of
Disease in Childhood 1983; 58:442-444.
64. Kales A et al. Hereditary factors in sleep walking and night terrors. Br J Psychiatry
1980; 137:111-118.
65. Kalm E, Fisher C, Edwards A. Twenty-four hour sleep patterns: comparison
between 2- to 3-year old and 4-to 6-year-old children. Arch Gen Psychiatry
1973;29:380.
66. Kaplan BJ, Mc Nicol J, Conte RA, Moghanclam HK. Sleep disturbance in
preschool-aged hyperactive and nonhyperactive children. Pediatrics 1987; 80:839-
844.
67. Kataria S, Swanson MS, Trevathan GE. Persistence of sleep disturbances in
preschool children. Journal of Pediatrics 1987;110(4):642-646.
68. Kerr S. Preventing sleep problems in infants: a randomized controlled trial. J Adr
Nurs 1999; 24:938-942.
69. Kerr S, Jowett S. Sleep problems in pre-school children: a review of the literature.
Child: Care, Health and Development 1994;20:379-391.
70. Klackenberg G. Sleep behaviour studied longitudinally: data from 4-16 years on
duration, night-awakening and bedsharing. Acta Paediatrica Scandinavica
1982;71:501-506.
7l. Klackenberg G. The development of children in a Swedish urban community. A
prospective longitudinal study. VI. The sleep behaviour of children up to three
years of age. Acta Paediatrica Scandinavica Suppl. 187. 1968;105-121.
72. Landgren M, Pettersson R, Kjellman B, Gillberg C. ADHD, DAMP and other
neurodevelopmental/psychiatric disorders in 6-year-old children: epidemiology and
comorbidity. Developmental Medicine and Child Neurology 1996; 38:891-906.

72
73. Leeson R, Barbour J, Romaniuk D, Warr R. Management of infant sleep problems
in a residential unit. Child: Care, Health and Development 1994;20(2):89-100.
74. Loyd BH, Abidin. Revision of the Partenting Stress Index. Journal of Pediatric
Psychology 1985; 10:169-177.
75. Lozoff B, Wolf AW, Davis NS. Cosleeping in urban families with young children
in the United States. Pediatrics 1984; 74:171-182.
76. Lozoff B, Wolf AW, Davis NS. Sleep problems seen in pediatric practice.
Pediatrics 1985;75:477-483
77. Madansky D, Edelbrock C. Cosleeping in a community sample of 2- and 3-year-old
children. Pediatrics 1990; 86:197-203.
78. Marcotte AC, Thacher P, Buttens M, Bortz J, Acebo C, Carskadon M. Parental
report of sleep problems in children with attentional and learning disorders. Journal
of Developmental and Behavioural Pediatrics 1998; 19(3):178-186.
79. Messer DJ, Lauder L, Humphrey S. The effectiveness of group therapy in treating
children´s sleeping problems. Child: care, health and development 1994; 20:267-
277.
80. Mick E, Biederman J, Jetton J, Faraone S. Sleep disturbances associated with
attention deficit hyperactivity disorder: The impact of psychiatric comorbidity and
pharmacotheraphy. Journal of Chile and Adolescent Psychopharmacology 2000;
10(3):223-231.
81. Minde K, Faucon A, Falkners S. Sleep Problems in Toddlers: Effect of treatment
on their daytime behaviour. Journal of American Child Adolescent Psychiatry
1994; 33(8):1113-1121.
82. Minde K, Popiel K, et al. The evaluation and treatment of sleep disturbances in
young children. Journal of Child Psychology and Psychiatry 1993;34(4):521-533.

73
83. Mindell JA. Sleep disorders in children. Health Psychology 1993;12(2):151-162.
84. Mindell JA, Owens JA, Carskadon MA. Developmental features of sleep. Child
Adolesc Psychiatr Clin North Am 1999;8:695-725.
85. Moore T, Ucko LE. Night waking in early infancy. Archives of Disease in
Childhood 1957;32:333-342.
86. Osterholm P, Lindeke LL, Amidon D. Sleep disturbance in infants ages 6 to 12
months. Pediatr Nurs 1983; 9:269-271.
87. Owens-Stively J et al. Child temperament, parenting discipline style, and daytime
behaviour in childhood sleep disorders. J Dev Behav Pediatrics 1997; 18(5):314-
321.
88. Palm L, Persson E, Bjerre I, Elmqvist D, Blennow G. Sleep and wakefulness in
preadolescent children with deficits in attention, motor control and perception. Acta
Paediatrica 1992; 81:618-624.
89. Paret I. Night waking and its relation to mother – infant interaction in nine-month-
old infants. In Call JD, Galenson E, Tysom RL (eds). Frontiers of Infant Psychiatry
1983;171-177. New York Basic Books.
90. Picchietti DL, England SJ, Walters AS, Willis K, Verrico T. Periodic limb
movement disorder and restless legs syndrome in children with attention-deficit
hyperactivity disorder. J Child Neurol 1998; 13:588-594.
91. Picchietti DL, Underwood DJ, Farris WA, Walters AS, Shah MM, Dahl RE,
Trubnick LJ, Bertocci MA, Wagner M, Hening WA. Further studies on periodic
limb movement disorder and restless legs syndrome in children with attention-
deficit hyperactivity disorder. Movement Disorders 1999; 14(6):1000-1007.
92. Pollock J. Night-waking at five years of age: predictors and prognosis. Journal of
Child Psychology and Psychiatry 1994;35(4):699-708.

74
93. Prince JB, Wilens TE, Biederman J, Spencer TJ, Wozniak JR. Clonidine for sleep
disturbances associated with attention-deficit hyperactivity disorder: A systematic
chart review of 62 cases. J Am Acad Child Adolesc Psychiatry 1996; 35(5):599-
605.
94. Ragins N, Schachter J. A study of sleep behaviour in two-year-old children. Journal
of Child Psychology and Psychiatry 1971;10:464-480.
95. Rasmussen P, Gillberg C. Perceptual, motor and attentional deficits in seven-year-
old children. Paediatric aspects. Acta Paediatrica Scandinavica 1983; 72:125-130.
96. Rasmussen P, Gillberg C. Perceptual, motor and attentional deficits in sex-year-old
children. Screening procedure in pre-school. Acta Paediatrica Scandinavica 1982;
71:121-129.
97. Richert V, Johnson C. Reducing nocturnal awakening and crying episodes in
infants and young children: A comparison between scheduled awakenings and
systematic ignoring. Pediatrics 1988; 81: 203-212.
98. Richman N. A community survey of characteristics of one to two year-olds with
sleep disruptions. Journal of the American Academy of Child Psychiatry
1981;20:281-291.
99. Richman N. Sleep problems in young children. Archives of Disease in Childhood
1981; 56:491-493.
100. Richman N. Surveys of sleep disorders in children in a general population. In
Guilleminault C (eds). Sleep and its disorders in children. New York, Raven Press
1987.
101. Richman N, Douglas J, Hunt H, Lansdown R, Levere R. Behavioural methods in
the treatment of sleep disorder – a pilot study. Journal of Child Psychology and
Psychiatry 1985;26: 581-590.
75
102. Richman N, Stevenson JE, Graham PJ. Behaviour problems in three-year-old
children: An epidemiological study in a London borough. Journal of Child
Psychology and Psychiatry 1975;12:5-33.
103. Richman N, Stevenson J, Graham P. Preschool to school: a behavioural study.
London: Academic Press, 1982.
104. Ring A, Stein D, Barak Y, Teicher A, Hadjez J, Elizur A, Weizman A. Sleep
disturbances in children with attention-deficit/hyperactivity disorder: A
comparative study with healthy siblings. Journal of Learning Disabilities 1998;
31(6): 572-578.
105. Roffwarg HP, Muzio JN, Dement WC. Ontogenetic development of the human
sleepdream cycle. Science 1966;156:604-619.
106. Rona R, Li L, Gulliford M, Chinn S. Disturbed sleep: effects of sociocultural
factors and illness. Arch Dis Child 1998; 78(1):20-25.
107. Rosen CL. Sleep disorders in infancy, childhood and adolescence. Curr Opin Pulm
Med 1997; 3(6):449-455.
108. Sadeh A. Assessment of intervention for infant night waking: parental reports and
activity-based home monitoring. J Consult Clin Psychol 1994; 62:63-68.
109. Sadeh A. Evaluating night wakings in sleep-disturbed infants: a methodological
study of parental reports and actigraphy. Sleep 1996;19(10):757-762.
110. Sadeh A, Anders TF. Infant sleep problems: origin, assessment, interventions.
Infant Mental Health Journal 1993; 14(1):17-34.
111. Sadeh A, Lavie P, Sher A, Tirosh E, Epstein R. Actigraphic home-monitoring
sleep-disturbed and control infants and young children: a new method for pediatric
assessment of sleep-wake patterns. Pediatrics 1991;87:494-499.

76
112. Sadeh A, Sharkey KM, Carskadon MA. Activity-based sleep-wake identification:
an empirical test of methodological issues. Sleep 1994;17:201-207.
113. SAS. SAS introductory guide for personal computers. Version 6. Edition ed: Cary,
NC: SAR Institute Inc, 1985.
114. Schachter FF, Fuchs ML, Bijur PE, Stone RK. Cosleeping and sleep problems in
Hispanic-American urban young children. Pediatrics 1989; 84:522-530.
115. Scher A. A longitudinal study of night waking in the first year. Child Care Health
Dev 1991;7(5):295-302.
116. Scott G, Richards MPM. Night waking in one-year-old children in England. Child
Care Health Dev 1990; 16: 283-302.
117. Sears W. Night time parenting 1985. Collins Dove, Melbourne.
118. Seymour F, Broch P, During M, Poole G. Reducing sleep disruptions in young
children: Evaluation of therapist guided and written information approaches: A
brief report. Journal of Child Psychology and Psychiatry 1989; 30:913-918.
119. Smedje H. Nighttime sleep and daytime behaviour in children. Studies based on
parents’ perceptions of five to eight year old children. Academic disseratation.
Uppsala University 2000.
120. Stein MA. Unravelling sleep problems in treated and untreated children with
ADHD. Journal of Child and Adolescent Psychopharmacology 1999; 9(3):157-168.
121. Stores G. Practitioner review: assessment and treatment of sleep disorders in
children and adolescents. J Child Psychol Psychiatry 1996;37:907-925.
122. Tannock R. Attention Deficit Hyperactivity Disorder. Advances in cognitive,
neurobiological, and genetic research. Journal of Child Psychology and Psychiatry
1998; 39:65-99.

77
123. Tirosh E, et al. Sleep characteristics of asthmatics in the first four years of life: a
comparative study. Archives of Disease in Childhood 1993;68(4):481-483.
124. Trommer BL, Hoeppner JB, Rosenberg RS, Armstrong KJ, Rothstein JA. Sleep
disturbance in children with attention deficit disorder. Annals of Neurology 1988;
24:322.
125. Van Tassel E. The relative influence of child and environmental characteristics on
sleep disturbances in the first and second years of life. Journal of Developmental
and Behavioural Pediatrics 1985;6(2):81-86.
126. Walters J. Sleep management – the hidden agenda. Child: care, health and
development 1993; 19:197-208.
127. Wilens T, Biederman J, Spencer T. Clonidine for sleep disturbances associated with
attention-deficit hyperactivity disorder. J Am Child Adolesc Psychiatry 1994;
33(3):424-426.
128. Wolfson A, Lacks P, Futterman A. Effects of parent training on infant sleeping
patterns, parents´ stress, and perceived parental competence. Journal of Consulting
and Clinical Psychology 1992; 60:41-48.
129. Zuckerman B, Stevenson J, Bailey V. Sleep problems in early childhood:
continuities, predictive factors, and behavioural correlates. Pediatrics 1987;80:664-
671.
130. Östberg M, Hagekull B, Wettergren S. A measure of parental stress in mothers with
small children: dimensionality, stability and validity. Scandinavian Journal of
Psychology 1997; 38:199-208.





























![[Product Monograph Template - Standard] - Roche … and Packaging section of the product monograph Severe respiratory insufficiency ... Sleep apnea syndrome Myasthenia gravis](https://img.pdfslide.net/doc/110x75/5ae5e3e07f8b9acc268c9f1c/product-monograph-template-standard-roche-and-packaging-section-of-the.jpg)