Embed Size (px)
Citation preview

Physiology & Behavior 104 (2011) 180–186
Contents lists available at ScienceDirect
Physiology & Behavior
j ourna l homepage: www.e lsev ie r.com/ locate /phb
Sex differences in physiological and affective responses to stress inremitted depressioni
Sara L. Bagley, Terri L. Weaver, Tony W. Buchanan ⁎Department of Psychology, Saint Louis University, 221 N. Grand Blvd., Saint Louis, MO, USA
i Young Investigator Travel Awardee.⁎ Corresponding author at: Department of Psychology
Grand Blvd., St. Louis, MO 63103, USA. Tel.: +1 314 977E-mail address: [email protected] (T.W. Buchanan)
0031-9384/$ – see front matter © 2011 Elsevier Inc. Aldoi:10.1016/j.physbeh.2011.03.004
a b s t r a c t
a r t i c l e i n f oArticle history:Received 1 October 2010Received in revised form 2 March 2011Accepted 3 March 2011
Keywords:StressRemitted depressionTSSTCortisolSalivaryAlpha-amylaseSex differences
Major depressive disorder (MDD) is associated with alterations in stress physiology. Severe melancholicdepression is characterizedbyhypercortisolism, but community dwellingmildly depressed individuals and thosewith remittedMDDhave shown reducedor normal reactivity to stress. There are also pronounced sex differencesboth in the incidence ofMDD and in stress reactivity. To explore the relationships among depression history, sexdifferences, and stress, we examined stress reactivity in people with and without a history of MDD. Twenty-twoparticipants with remitted MDD (12 men and 10 women) and 36 never depressed comparison participants (22men and 14 women) participated in the study. Cortisol and alpha-amylase (sAA) were sampled from salivabefore, 10 min after, and 30 min after the Trier Social Stress Test (TSST). Participants filled out the Positive AffectNegative Affect Schedule (PANAS) before and after they underwent the TSST. Women with remitted MDDshowed reduced cortisol response to the TSST comparedwith the never MDDwomen, while menwith remittedMDD showed comparable cortisol reactivity to the never depressed men. The groups did not differ on sAAreactivity to stress. The remittedMDDgroup (overall andmen andwomen separately) reported greater negativeaffect both before and after stress compared to the never depressed group. Women from both groups reportedgreater post-stress negative affect than men. In contrast, men from both groups reported higher positive affectbefore and after stress than women. Given that the sex difference findings were not dependent on depressionhistory, self-reported affectivedifferences in response to stressmaypredate depressive symptoms and contributeto sex differences in depression incidence.
, Saint Louis University, 221 N.2271; fax: +1 314 977 1014.
.
l rights reserved.
© 2011 Elsevier Inc. All rights reserved.
1. Introduction
Major depressive disorder (MDD) is highly prevalent in the UnitedStates [1] and one of the leading causes of disability throughout theworld [2]. Life stressors are known to precipitate the onset of depressiveepisodes [3]. In a review of community samples examining stress anddepression, Mazure showed that 82% of depressed individuals experi-enced a severe adverse life event prior to the onset of depression [4]. Bycontrast, only 32% of non-depressed individuals reported such an eventwithin the same time frame. Many of these stressful life events wereindependent fromthe individual—events that the subject couldnot havecontributed to, such as natural disasters—supporting the idea that stresscan play an important causal role in the development of depression [5].
Depression has a high rate of recurrence; a longitudinal study thatexamined patients up to 15 years after an initial episode found arecurrence rate of 87% [6]. Stress may exert different effects on thosewith a history of MDD compared to never depressed individuals. For
example, major stressful life events are more likely to precede earlier,rather than later depressive episodes [7], suggesting that once anindividual has experienced one MDD episode, less stress may berequired to elicit the next episode. These findings support the so-called kindling/sensitization hypothesis: that stress sensitizes thebrain to the development of further episodes of depression [8].
The two primary stress-reactive physiological systems, the HPA axisand sympathetic nervous system (SNS) are under separate, butoverlapping neural control [9]; studies that have examined stressphysiology inMDDgroupshavedemonstrateddysregulation inboth theHPA and SNS [10]. Severe melancholic depression has been character-ized by hypercortisolism [11,12], while mildly depressed individualsand those with remitted MDD show reduced or normal cortisolreactivity to stress [13–15]. Patients with melancholic depression alsodisplay increased SNS activity, in the form of elevated plasmacatecholamines andheart rate,while atypicaldepressedpatientsdisplaysuppressed SNS activity [10,16,17]. Considerable researchhas examinedthe effects of chronic and acute stress on salivary alpha-amylase (sAA),an enzymatic index of the SNS [18]. sAA has not, however, been studiedin relation to MDD, either in an active or remitted state.
Alterations in HPA physiology and brain structure persist afterremission. Ahrens et al. found lower cortisol levels in the morning, atbaseline, and in response to the Groningen Acute Stress Test in women

181S.L. Bagley et al. / Physiology & Behavior 104 (2011) 180–186
remitted from recurrent MDD compared with never depressed women[13]. Notably, they did not find a difference between groups in SNSresponse to the stressor (measured by heart rate, heart rate variability,epinephrine, and norepinephrine). Investigations into brain structurefound that remitted depressives have significantly smaller hippocampalvolumes [19,20]. This finding has been documented several times inindividuals with active depressive episodes [21,22]. Sheline et al.suggest that since the smaller volume of the hippocampus wascorrelated with the number of days depressed, the alteration inhypothalamic–pituitary–adrenal (HPA) axis functioning may haveaffected the hippocampus via glucocorticoid neurotoxicity [23].
There are pronounced sex differences both in the incidence of MDDas well as in physiological and psychological stress reactivity. MDDaffectswomen one-and-a-half to three timesmore commonly thanmen[24]. Compared to men, women are more likely to have a dysregulatedHPA axis, either in the form of hyporeactivity or altered response topharmacological challenge [25,26]. Men tend to show higher cortisoland SNS responses to acute stressors when compared to age-matchedwomen [27–29]. Recent work has demonstrated that men show highersAA in response to stress [30]. In addition to sex differences in stressphysiology, women also report more negative self-concepts and tend toruminate about stressful events, which may make them moresusceptible to depressive symptomatology [31]. Men on the otherhand are more likely to view stressors as a challenge and either ignorethe stressor or try to take direct action to circumvent the stressor, whichmay leadmen to other outcomes in response to stress such as antisocialbehavior and substance abuse [32,33].
In this study, we examined the relationships among stressphysiology, affective reports, and sex in individuals with and withouta history of MDD. Measures of the HPA axis, SNS, and affective reportswere taken before and after participants underwent a psychosocialstressor. The first objective of this study was to examine thephysiological response to stress in those with remitted depression andnever depressed comparison participants. Based on previouswork [13],we predicted that those with remitted MDD would show reduced HPAand SNS stress reactivity compared to never depressed comparisonparticipants. Our secondobjectivewas to examine self-reportedpositiveand negative affects before and after stress in men and women withremitted depression and never depressed comparison participants. Wepredicted that bothmen andwomenwith remittedMDDwould show agreater negative affective response to stress compared to those withouta history of MDD. However, we made no specific predictions regardingpositive affect or sex differences in affective responses to stress.
Table 1Participant characteristics and demographics. Values are mean±standard error of the meanfrom the night before testing reported by each participant subgroup.
Remitted MDD group
Female Male Total MDD(n=10) (n=12) (n=22)
Age (years) 31.1±2.6 36.8±2.2 34.2±1.7Hours of sleep 7.2±0.5 7.1±0.4 7.2±0.3Age 1st MDD episode (years) 26.6±2.5 24.5±2.1 25.5±1.6Number of MDD episodes 1.6±0.4 2.0±0.5 1.8±0.3
Severity (n=10) (n=10⁎) (n=20⁎)
Mild 6 4 10Moderate 3 3 6Severe 1 3 4
Phase of menstrual cycle (n=10) (n=10)
Follicular 6 NA 6Luteal 4 NA 4Irregular 0 NA 0
⁎ One participant was classified as dysthymic and one participant's SCID did not have a sevsex difference among any of the variables (psN0.1). None of the between-group analyses dcomparison group (psN0.1).
2. Methods
2.1. Participants
Participants with and without a history of major depressive disorder(MDD) were recruited from the community by ads posted online and innewspapers. Inclusion into the study was assessed during an initial visit,during which each participant was assessed using the Structured ClinicalInterview for DSM-IV Axis I Disorders (SCID) for current and past mooddisorder. Exclusion criteria for both the remitted MDD and neverdepressed groupswere: current or past episodes of schizophrenia, bipolardisorder, post traumatic stress disorder, diabetes, chronic illness andcurrent episodes of substance abuse or dependence, panic disorder, socialphobia, obsessive compulsive disorder, and generalized anxiety disorder.Exclusion criteria for the never depressed group also included current orpast episodes of MDD. Participants taking psychiatric, neurological, bloodpressure, hormone-based contraceptive or corticosteroid-based medica-tions were excluded, while participants taking cholesterol, allergy, andantidepressant medications were included. Three males with remittedMDD were currently on antidepressant medications (trazadone, velafax-ine [Effexor], andbupropion [Wellbutrin]). None of these participantsmetcriteria for current MDD, and their data were in the range of the otherremitted MDD participants for sAA, cortisol, and self-reported affect.Results of analyses conducted with these participants' data excludedshowed the same pattern as results reported for the complete sample.
One hundred thirty-six participants were initially interviewed and58 participants, 22 participants with a history of MDD (12 men and 10women) and 36 never depressed comparison participants (22men and14women), completed the study. Current phase ofmenstrual cycle wascollected for female participants and exploratory analyses did not showsignificant differences in the distribution of menstrual cycle phasebetween the remitted MDD and comparison women (see Table 1 forparticipant characteristics). All participants gave written informedconsent before study inclusion following procedures approved by theInstitutional Review Board at Saint Louis University.
2.2. Study protocol
2.2.1. Screening dayAfter arrival in the laboratory, the participant read and signed the
informed consent document. A master's level clinical psychologygraduate traineewith formal training in the administration of diagnosticinterviews then conducted the SCID. All diagnostic interviews were
. MDD=major depressive disorder; Hours of Sleep indicates the average hours of sleep
Comparison group Overall
Female Male Total comparison(n=14) (n=22) (n=36) (n=58)
30.8±1.8 32.4±1.7 31.8±1.2 32.7±1.07.5±0.2 6.8±0.3 7.1±0.2 7.1±0.2NA NA NA 25.5±1.6NA NA NA 1.8±0.3
(n=20⁎)
NA NA NA 10NA NA NA 6NA NA NA 4
(n=14) (n=14) (n=24)
7 NA 7 134 NA 4 83 NA 3 3
erity rating. None of the within-group, between sex analyses demonstrated a significantemonstrated a significant difference in demographics between the remitted MDD and

182 S.L. Bagley et al. / Physiology & Behavior 104 (2011) 180–186
supervised and reviewed by the second author and differences indiagnostic decisions were resolved by consensus. Participants whoqualified as either remittedMDDor never depressedwere scheduled fortesting. All further testingoccurredbetween1 day and2 weeks after theSCID. Participants that did not fit the inclusion criteria were debriefedand thanked for their participation. Each screening day session tookapproximately 60 min to complete.
2.2.2. Testing dayFor the testing day, participants were asked to abstain from food or
drink (other than water) for 2 h before arrival at the laboratory.Participants were also asked to get between 6 and 8 h of sleep the nightbefore the test day (mean=7.1, S.E.=0.2) and to refrain from physicalexercise, alcohol, and caffeinated beverages from the evening beforetesting until reporting to the laboratory on the testing day. Participantswere tested between the hours of 1200 and 1600 to control for thediurnal cycles of sAA and cortisol.
Upon arrival, each participant was connected to electrodes formeasure of physiological parameters (to be reported elsewhere),completed a set of demographic questionnaires, and sat in a chair for10 min. The time from participant arrival until the initial saliva sampleranged from 15 to 20 min. At the end of the 10 min the initial salivasample (S1) for the measure of sAA and cortisol was collected and theparticipant filled out the first Positive Affect Negative Affect Schedule(PANAS; Watson, Clark, and Tellegen, 1988). Then the participant wasgiven instructions for the speech portion of the Trier Social Stress Test(TSST; [34]) and was given 5 min to prepare for the speech. In thismodified version of the TSST, participants were told that they had beenaccused of shoplifting and that they were to defend themselves in frontof two store managers (adapted from [35]). During the five-minutepreparation period, the participant could make notes using paper andpencil that were provided; however, they were not allowed to use anynotes during the actual speech. After the preparation period, theparticipant moved to a novel room where the two judges were waitingto view the 10-minute TSST. The participant was videotaped while he/she gave the five-minute speech and did the five-minute verbal mentalarithmetic task (serial subtraction of 13 from1022).When the TSSTwascompleted the participant returned to the original room and filled outthe PANAS for the second time. Ten minutes post-TSST, the participantprovided another saliva sample (S2) for the peak measurement of sAAand cortisol. Thirty minutes after the end of the TSST, the final salivasample (S3)was taken tomeasure the recovery of sAA and cortisol. Theparticipantwas then debriefed and thanked for their participation. Eachtesting day took approximately 60 min to complete.
2.3. Affective response to the TSST
State subjective responses to the TSST were collected using thePositive Affect/Negative Affect Schedule (PANAS; [36]). The scale iscomposed of 20 items; 10 represent the subscale of Positive Affect (PA)and the other 10 represent the subscale of NegativeAffect (NA). PositiveAffect ranges from low (sadness and lethargy) to high (energy,concentration, and engagement) while Negative Affect ranges fromlow (calmness and serenity) to high (distress and unpleasurableengagement). Participants were asked to rate the items to the degreethat they felt them at the present moment on a 5-point Likert scalewhere 1 represented Very Slightly or Not at All and 5 representedExtremely. The PANAS has high internal consistency (PA: Cronbach'salpha=0.89, NA: Cronbach's alpha=0.85; [36]) and both PA and NAare highly correlated with their regression-based factor scores, withconvergent validity correlations ranging from 0.89 to 0.95.
2.4. Saliva assessment of alpha-amylase and cortisol
Saliva was collected using Salivette collection tubes (Sarstedt,Rommelsdorf, Germany). Participants were instructed to chew on a
cotton roll for approximately 2 min and return the saturated cotton rollto the Salivette collection tube when the time was up. Samples werestored at −20 °C until assayed. sAA is an index of SNS activity [37,38]and was measured by the quantitative enzyme kinetic method [37,38].Cortisol, an index of HPA axis activity [39] was measured with acommercial immunoassay kitwith chemiluminescence detection (CLIA;IBL Hamburg, Germany). Intraassay and interassay coefficients ofvariation were less than 10%. The lower sensitivity for cortisol is0.5 nmol/l and 1.5 U/ml for alpha-amylase.
2.5. Data management and analysis
Two participants' sAA data and one participant's cortisol data aremissing due to insufficient volume of saliva in the sample. Allparticipants' data were used in the PANAS analyses. Demographicmeasures were compared between groups and between males andfemales within groups using independent-samples t-tests and Chi-square analyses. None of the demographic measures were differentbetween groups or between sexes (see Table 1). Measures of effect sizeare reported using partial eta-squared (η2).
3. Results
3.1. Physiological results
To determine the efficacy of the stress manipulation and toexamine group and sex differences in reactivity, repeated measuresmultivariate analyses of variance (MANOVAs) were conductedindependently for cortisol and for sAA; the analyses used a 2 Group(remittedMDD and never depressed)×2 Sex×3 Time (S1, S2, and S3)design. Cortisol and sAA increased in response to stress for the wholesample (main effect of Time for cortisol: F(2, 50)=4.4, pb0.05, partialeta-squared=0.15; and main effect of Time for sAA: F(2,51)=5.4,pb0.01, partial eta-squared=0.17).
Addressingobjective 1outlined in Section1, the results demonstratedthat for cortisol, there was a pronounced difference in the way thatparticipantswith remittedMDDrespond to stress and this differencewasmoderated by participant sex. Specifically, women with remitted MDDshowed a reduced cortisol response to stress compared to neverdepressed women, while men with remitted MDD showed an increasedcortisol response compared toneverdepressedmen (Group×Sex×Timeinteraction: F(2, 52)=3.96, pb0.05, partial eta-squared=0.13; seeFig. 1). There was not, however, a Group×Time interaction: F(2, 52)b1,pN0.6, partial eta-squared=0.01. The Group×Sex×Time interactionremained significant when male participants currently takingantidepressant medications were excluded from the analysis (F (2,49)=3.93, pb0.05, partial eta-squared=0.14). Planned contrastscomparing cortisol values at each time point within each sexdemonstrated that remitted MDD women showed lower values thannever depressed women during stress (i.e., 10 minute sample) andpost-stress (i.e., 30 minute sample), p=0.055 and p=0.03, respective-ly. The same comparisons in men showed that cortisol levels in thosewith remitted MDD were not significantly different from their neverdepressed counterparts (psN0.2). There was, however, a main effect ofSex: men from both groups showed higher cortisol levels both beforeand after stress compared to women, F(1,53)=13.2, pb0.01, partialeta-squared=0.2, and a Sex×Time interaction: F(2,50)=3.8, pb0.05,partial eta-squared=0.13. The main effect of Sex remained when themale participants taking antidepressant medications were excludedfrom the analysis (F (1, 50)=12.24, pb0.01, partial eta-squared=0.2).
In contrast to cortisol reactivity, sAA reactivity did not differ basedonMDD history or sex (nomain effects or interactions of sex or group:psN0.2; see Fig. 2).
To control for potential sex differences in depression severity,clinician rated severity (mild, moderate, and severe) was entered as acovariate in a separate set of analyses (MANCOVAs). Theprimary results
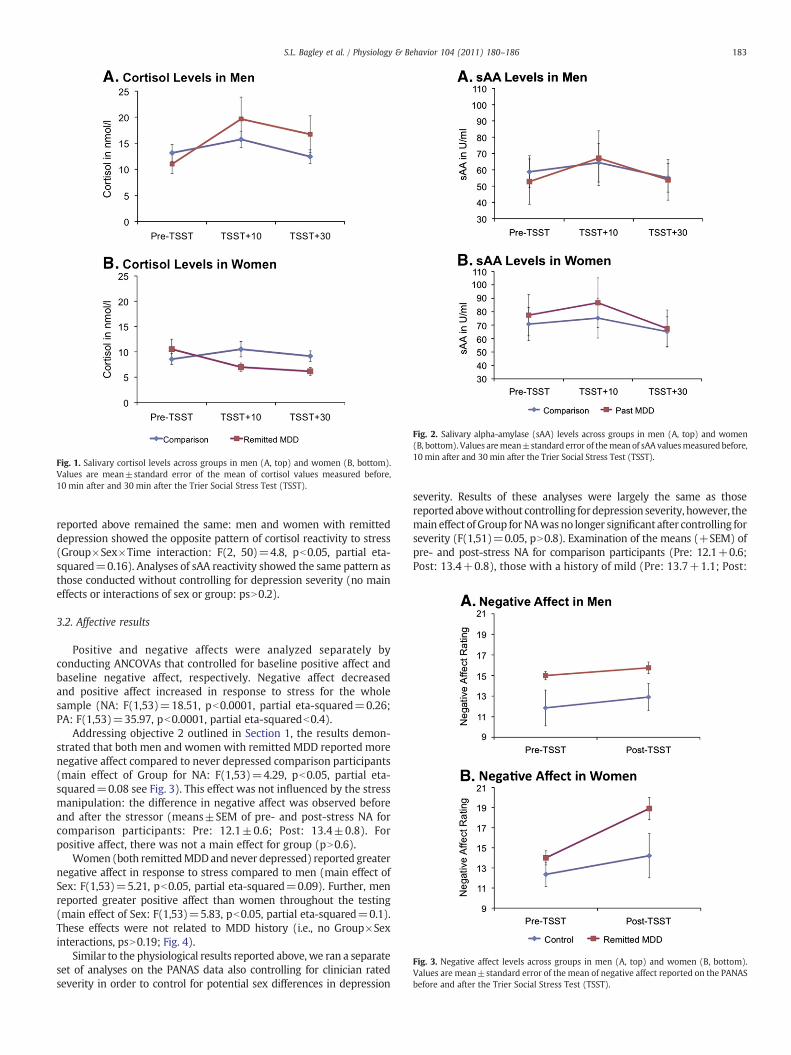
Fig. 1. Salivary cortisol levels across groups in men (A, top) and women (B, bottom).Values are mean±standard error of the mean of cortisol values measured before,10 min after and 30 min after the Trier Social Stress Test (TSST).
Fig. 2. Salivary alpha-amylase (sAA) levels across groups in men (A, top) and women(B, bottom). Values aremean±standard error of themean of sAA valuesmeasuredbefore,10 min after and 30 min after the Trier Social Stress Test (TSST).
Fig. 3. Negative affect levels across groups in men (A, top) and women (B, bottom).Values are mean±standard error of the mean of negative affect reported on the PANASbefore and after the Trier Social Stress Test (TSST).
183S.L. Bagley et al. / Physiology & Behavior 104 (2011) 180–186
reported above remained the same: men and women with remitteddepression showed the opposite pattern of cortisol reactivity to stress(Group×Sex×Time interaction: F(2, 50)=4.8, pb0.05, partial eta-squared=0.16). Analyses of sAA reactivity showed the same pattern asthose conducted without controlling for depression severity (no maineffects or interactions of sex or group: psN0.2).
3.2. Affective results
Positive and negative affects were analyzed separately byconducting ANCOVAs that controlled for baseline positive affect andbaseline negative affect, respectively. Negative affect decreasedand positive affect increased in response to stress for the wholesample (NA: F(1,53)=18.51, pb0.0001, partial eta-squared=0.26;PA: F(1,53)=35.97, pb0.0001, partial eta-squaredb0.4).
Addressing objective 2 outlined in Section 1, the results demon-strated that both men and women with remitted MDD reported morenegative affect compared to never depressed comparison participants(main effect of Group for NA: F(1,53)=4.29, pb0.05, partial eta-squared=0.08 see Fig. 3). This effect was not influenced by the stressmanipulation: the difference in negative affect was observed beforeand after the stressor (means±SEM of pre- and post-stress NA forcomparison participants: Pre: 12.1±0.6; Post: 13.4±0.8). Forpositive affect, there was not a main effect for group (pN0.6).
Women (both remittedMDDand never depressed) reported greaternegative affect in response to stress compared to men (main effect ofSex: F(1,53)=5.21, pb0.05, partial eta-squared=0.09). Further, menreported greater positive affect than women throughout the testing(main effect of Sex: F(1,53)=5.83, pb0.05, partial eta-squared=0.1).These effects were not related to MDD history (i.e., no Group×Sexinteractions, psN0.19; Fig. 4).
Similar to the physiological results reported above, we ran a separateset of analyses on the PANAS data also controlling for clinician ratedseverity in order to control for potential sex differences in depression
severity. Results of these analyses were largely the same as thosereported abovewithout controlling fordepression severity, however, themain effect of Group forNAwasno longer significant after controlling forseverity (F(1,51)=0.05, pN0.8). Examination of the means (+SEM) ofpre- and post-stress NA for comparison participants (Pre: 12.1+0.6;Post: 13.4+0.8), those with a history of mild (Pre: 13.7+1.1; Post:
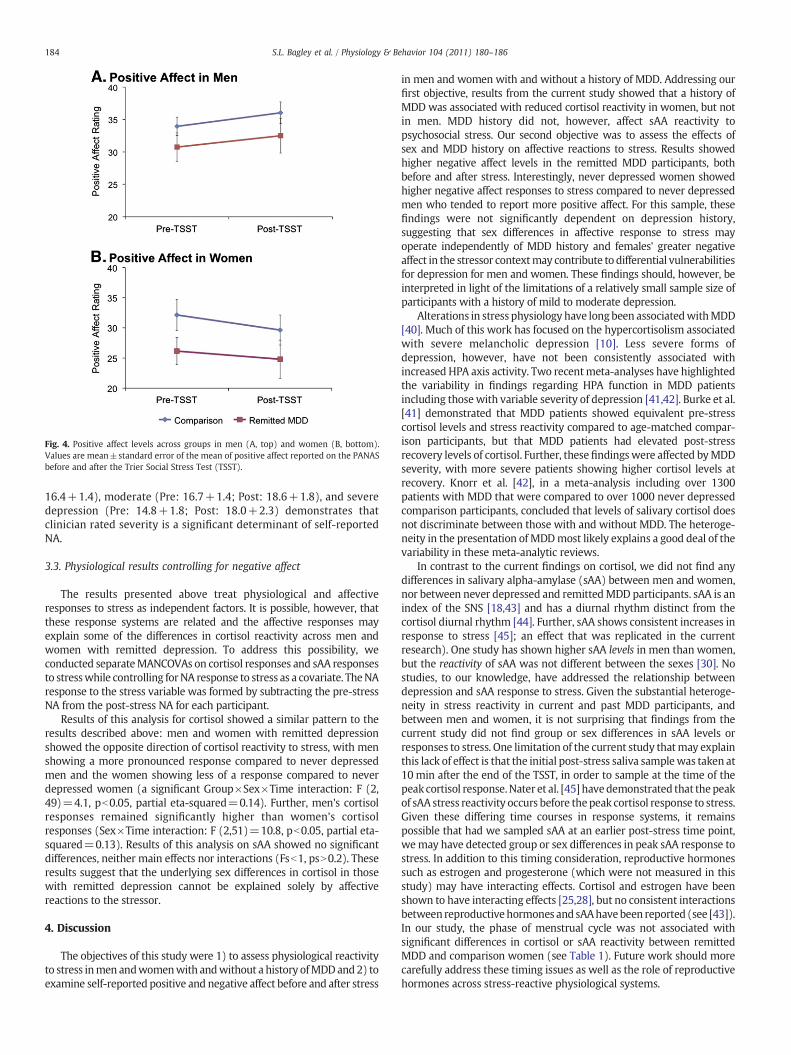
Fig. 4. Positive affect levels across groups in men (A, top) and women (B, bottom).Values are mean±standard error of the mean of positive affect reported on the PANASbefore and after the Trier Social Stress Test (TSST).
184 S.L. Bagley et al. / Physiology & Behavior 104 (2011) 180–186
16.4+1.4), moderate (Pre: 16.7+1.4; Post: 18.6+1.8), and severedepression (Pre: 14.8+1.8; Post: 18.0+2.3) demonstrates thatclinician rated severity is a significant determinant of self-reportedNA.
3.3. Physiological results controlling for negative affect
The results presented above treat physiological and affectiveresponses to stress as independent factors. It is possible, however, thatthese response systems are related and the affective responses mayexplain some of the differences in cortisol reactivity across men andwomen with remitted depression. To address this possibility, weconducted separateMANCOVAs on cortisol responses and sAA responsesto stresswhile controlling forNA response to stress as a covariate. TheNAresponse to the stress variable was formed by subtracting the pre-stressNA from the post-stress NA for each participant.
Results of this analysis for cortisol showed a similar pattern to theresults described above: men and women with remitted depressionshowed the opposite direction of cortisol reactivity to stress, with menshowing a more pronounced response compared to never depressedmen and the women showing less of a response compared to neverdepressed women (a significant Group×Sex×Time interaction: F (2,49)=4.1, pb0.05, partial eta-squared=0.14). Further, men's cortisolresponses remained significantly higher than women's cortisolresponses (Sex×Time interaction: F (2,51)=10.8, pb0.05, partial eta-squared=0.13). Results of this analysis on sAA showed no significantdifferences, neither main effects nor interactions (Fsb1, psN0.2). Theseresults suggest that the underlying sex differences in cortisol in thosewith remitted depression cannot be explained solely by affectivereactions to the stressor.
4. Discussion
The objectives of this study were 1) to assess physiological reactivityto stress inmen andwomenwith andwithout a history ofMDDand2) toexamine self-reported positive and negative affect before and after stress
in men and women with and without a history of MDD. Addressing ourfirst objective, results from the current study showed that a history ofMDD was associated with reduced cortisol reactivity in women, but notin men. MDD history did not, however, affect sAA reactivity topsychosocial stress. Our second objective was to assess the effects ofsex and MDD history on affective reactions to stress. Results showedhigher negative affect levels in the remitted MDD participants, bothbefore and after stress. Interestingly, never depressed women showedhigher negative affect responses to stress compared to never depressedmen who tended to report more positive affect. For this sample, thesefindings were not significantly dependent on depression history,suggesting that sex differences in affective response to stress mayoperate independently of MDD history and females' greater negativeaffect in the stressor contextmay contribute to differential vulnerabilitiesfor depression for men and women. These findings should, however, beinterpreted in light of the limitations of a relatively small sample size ofparticipants with a history of mild to moderate depression.
Alterations in stress physiology have longbeen associatedwithMDD[40]. Much of this work has focused on the hypercortisolism associatedwith severe melancholic depression [10]. Less severe forms ofdepression, however, have not been consistently associated withincreased HPA axis activity. Two recentmeta-analyses have highlightedthe variability in findings regarding HPA function in MDD patientsincluding thosewith variable severity of depression [41,42]. Burke et al.[41] demonstrated that MDD patients showed equivalent pre-stresscortisol levels and stress reactivity compared to age-matched compar-ison participants, but that MDD patients had elevated post-stressrecovery levels of cortisol. Further, thesefindingswere affected byMDDseverity, with more severe patients showing higher cortisol levels atrecovery. Knorr et al. [42], in a meta-analysis including over 1300patients with MDD that were compared to over 1000 never depressedcomparison participants, concluded that levels of salivary cortisol doesnot discriminate between those with and without MDD. The heteroge-neity in the presentation of MDDmost likely explains a good deal of thevariability in these meta-analytic reviews.
In contrast to the current findings on cortisol, we did not find anydifferences in salivary alpha-amylase (sAA) between men and women,nor between never depressed and remittedMDD participants. sAA is anindex of the SNS [18,43] and has a diurnal rhythm distinct from thecortisol diurnal rhythm [44]. Further, sAA shows consistent increases inresponse to stress [45]; an effect that was replicated in the currentresearch). One study has shown higher sAA levels in men than women,but the reactivity of sAA was not different between the sexes [30]. Nostudies, to our knowledge, have addressed the relationship betweendepression and sAA response to stress. Given the substantial heteroge-neity in stress reactivity in current and past MDD participants, andbetween men and women, it is not surprising that findings from thecurrent study did not find group or sex differences in sAA levels orresponses to stress. One limitation of the current study thatmay explainthis lack of effect is that the initial post-stress saliva samplewas taken at10 min after the end of the TSST, in order to sample at the time of thepeak cortisol response.Nater et al. [45] havedemonstrated that thepeakof sAA stress reactivity occurs before thepeak cortisol response to stress.Given these differing time courses in response systems, it remainspossible that had we sampled sAA at an earlier post-stress time point,wemay have detected group or sex differences in peak sAA response tostress. In addition to this timing consideration, reproductive hormonessuch as estrogen and progesterone (which were not measured in thisstudy) may have interacting effects. Cortisol and estrogen have beenshown to have interacting effects [25,28], but no consistent interactionsbetween reproductivehormones and sAAhavebeen reported (see [43]).In our study, the phase of menstrual cycle was not associated withsignificant differences in cortisol or sAA reactivity between remittedMDD and comparison women (see Table 1). Future work should morecarefully address these timing issues as well as the role of reproductivehormones across stress-reactive physiological systems.

185S.L. Bagley et al. / Physiology & Behavior 104 (2011) 180–186
The current study used the remitted depression paradigm [46],which is based on the assumption that differences between those withremittedMDDcompared tonever depressed individuals reflects either apredisposition for, or some lingering effect of, the MDD episode in theremitted MDD individual. To our knowledge, only one other study hasexamined stress reactivity using the remitted depression paradigm.Ahrens et al. [13] addressed basal and stress-reactive ACTH, cortisol,norepinephrine, and several cardiovascular parameters in a group ofwomen remitted fromMDD. Results showed thatwomenwith remittedMDD had lower morning cortisol levels as well as a blunted ACTH andcortisol response to stress. These authors did not find significantdifferences in SNS measures between the remitted MDD group andcomparison participants. Results from the women in the current studyreplicate these findings from Ahrens et al. [13]: the women withremittedMDDshowed ablunted cortisol response to stress compared tonever depressed comparison participants, but no differences in SNSreactivity were found.
Men with a history of depression, by contrast, did not show thisblunted cortisol reactivity; their responsewas not significantly differentfrom the never depressedmen. Ahrens et al. [13] did not includemen intheir study and their participants had experienced more severedepression than the participants included in the current study. Thesepatients had an average of more than nine episodes of MDD and had allbeen hospitalized for their depression. By contrast, the average numberof depressive episodes in our sample was less than two and only four ofour participants had been classified as having severe depression.Further, the participants from the Ahrens et al. studywere considerablyolder than those included in our study (average age 51 years versus anaverage of 34 years in our sample). Considering the demographic anddiagnostic severity differences between the participants in the currentstudy and the sample used by Ahrens et al., the consistent findings withregard to cortisol reactivity is noteworthy.
These findings support previous work with participants in an activedepressed episode, which has demonstrated significant variability instress reactivity. Some of this work reports heightened HPA reactivity,while others showed hyporeactivity or no difference from comparisonparticipants [41,42]. The currentwork extendsfindings onHPA reactivityand current MDD, suggesting that dysregulation of HPA reactivity tostress may continue after a depressive episode remits. The findings arenot mirrored for men with remitted depression. With the limitations oflow sample size in this study, and the challenges with the remitteddepression paradigm [46], there is still a need to examine whether thissex-related dysregulation of HPA reactivity can be detected prior to theonset of a depressive episode orwhether the dysregulation is a reflectionof alteredphysiology in response to the depressive episode (or episodes).
Although considerable research has documented increased stressreactivity in men compared to women, our results show that men hadelevated cortisol levels compared to women even before the stressor.This differencewas noted formen from the remittedMDDgroup aswellas theneverdepressedmen.The causeof this pre-stress sexdifference incortisol is unclear. There were no sex differences in age, time of testing,or other demographic variables that are typically associatedwith alteredHPA output. One possibility is that the experimenters for the studywerefemale, which may have led to an elevated cortisol level in the menduring the initial phases of the testing, which included the experi-menters affixingelectrodes on theparticipants' hands and torsos. Futureresearch should address potential interactions between sex of experi-menters and participants in order to address this potential confound.Another limitation to the study was the lack of a priori control overtiming of testing during different phases of the menstrual cycle in thefemale participants.We did document the current phase in each femaleparticipant (see Table 1); the remitted MDD and never depressedwomen did not differ with regard to the distribution of the number ofwomen in eachmenstrual phase. Futurework should better address thepotential interactive effects of depression history and menstrual phaseon stress reactivity.
The second objective of this work was to address the role of self-reported positive and negative affects in the context of depressionhistory and sex differences. Men and women with a history of MDDreported higher negative affect compared to never depressed compar-ison participants. These differences were observed before and after thestress manipulation. There has been considerable research on therelative roles of positive and negative affects as predictors of mood andanxiety disorders [47–49]. A consistent pattern is that depression isassociated with a general reduction in positive affect while anxietydisorders aremore associatedwith increases in negative affect [36]. Thispattern of reduced positive affect is consistent with the notion of a lackof pleasurable experiences and positive mood states in individuals withMDD [50]. Our finding demonstrated that the increased negative affectdoes not remit with the remission of the MDD episode. The remittedMDD participants also reported lower positive affect than thecomparison participants, although this difference was not statisticallysignificant. These findings are consistent with other research using theremitted depression design, which has shown that negative cognitivestyles and attitudes persist after remission of MDD [51]. An importantcaveat to consider, however, is that this study employed the stateversion of the PANAS, not the trait version.
Two of the primary risk factors in predicting the onset of an episodeof MDD include exposure to a stressful life event and being a woman.Among the never depressed comparison participants, women reportedgreater negative affect in response to stress and lower positive affectbefore and after stress compared to men. These findings are somewhatsurprising, given that previous research with the PANAS has notrevealed consistent sex differences, either at baseline [52] or in responseto laboratory stress [53,54]. Anecdotal evidence and scientific reportsendorse the notion that women are “more emotional” than men [55].Evidence for this assertion is sparse, but there are some indications of anemotional advantage in women compared to men for certain domains.These domains include facial emotion processing [56], recall ofemotional autobiographical memories [57], and emotional awareness[58]. The current findings, however, do not conform to thesedocumented emotional advantages in women. Our data, by contrast,demonstrate greater reported positive affect in men. The items thatconstitute the positive affect scale of the PANAS include excited, strong,enthusiastic, proud, and active, among others. These adjectives havebeen associated with extraversion [47] and may reflect our maleparticipants' notions of masculinity. Future work should address therelationship between positive affect and resilience to depression inmenand women.
5. Conclusions
Findings from this study replicate and extend previous work onstress reactivity in remitted depression [13]. Further, this workdemonstrates sex differences, both in physiological and psychologicalreactivity to stress. This work calls into question the assumption thatdepression and depression history is always associated with hyper-cortisolism and suggests that one potential mechanism of thepredominance of depression among women, as opposed to men,may be differences in the relative balance of positive versus negativeaffect.
Acknowledgements
We thank Dana Hamann and Meghan von Linden for theirassistance with conducting clinical interviews and scheduling andthe laboratory of Dr. Clemens Kirschbaum for conducting thebiochemical assays. This work was funded by a Young InvestigatorAward from the National Alliance for Research on Schizophrenia andDepression awarded to T.W.B.
186 S.L. Bagley et al. / Physiology & Behavior 104 (2011) 180–186
References
[1] Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States. Results from the NationalComorbidity Survey. Arch Gen Psychiatry Jan 1994;51(1):8–19.
[2] Murray CJ, Lopez AD. Evidence-based health policy—lessons from the GlobalBurden of Disease Study. Science Nov 1 1996;274(5288):740–3.
[3] Hammen C. Stress and depression. Annu Rev Clin Psychol 2005;1:293–319.[4] Mazure CM. Life stressors as risk factors in depression. Clin Psychol Sci Pract
1998;5:291–313.[5] Kendler KS, Karkowski LM, Prescott CA. Causal relationship between stressful life
events and the onset of major depression. Am J Psychiatry Jun 1999;156(6):837–41.[6] Keller MB, Boland RJ. Implications of failing to achieve successful long-term
maintenance treatment of recurrent unipolar major depression. Biol PsychiatrySep 1 1998;44(5):348–60.
[7] Kendler KS, Thornton LM, Gardner CO. Stressful life events and previous episodesin the etiology of major depression in women: an evaluation of the “kindling”hypothesis. Am J Psychiatry Aug 2000;157(8):1243–51.
[8] Post RM. Transduction of psychosocial stress into the neurobiology of recurrentaffective disorder. Am J Psychiatry Aug 1992;149(8):999–1010.
[9] Lovallo WR. Stress and health: biological and psychological interactions. 2nd ed.Thousand Oaks, CA: Sage; 2005.
[10] Gold PW, Wong ML, Chrousos GP, Licinio J. Stress system abnormalities inmelancholic and atypical depression: molecular, pathophysiological, and thera-peutic implications. Mol Psychiatry Sep 1996;1(4):257–64.
[11] Holsboer F, Barden N. Antidepressants and hypothalamic–pituitary–adrenocorti-cal regulation. Endocr Rev 1996;17(2):187–205.
[12] Wong ML, Kling MA, Munson PJ, et al. Pronounced and sustained centralhypernoradrenergic function in major depression with melancholic features:relation to hypercortisolism and corticotropin-releasing hormone. Proc Natl AcadSci USA 2000;97:325–30.
[13] Ahrens T, Deuschle M, Krumm B, van der Pompe G, den Boer JA, Lederbogen F.Pituitary–adrenal and sympathetic nervous system responses to stress in womenremitted from recurrent major depression. Psychosom Med May 2008;70(4):461–7.
[14] Peeters F, Nicolson NA, Berkhof J. Levels and variability of daily life cortisolsecretion in major depression. Psychiatry Res Apr 15 2004;126(1):1–13.
[15] Strickland PL, Deakin JF, Percival C, Dixon J, Gater RA, Goldberg DP. Bio-socialorigins of depression in the community. Interactions between social adversity,cortisol and serotonin neurotransmission. Br J Psychiatry Feb 2002;180:168–73.
[16] Carney RM, Freedland KE, Veith RC. Depression, the autonomic nervous system,and coronary heart disease. Psychosom Med May–Jun, 2005;67(Suppl 1):S29–33.
[17] Veith RC, Lewis N, Linares OA, et al. Sympathetic nervous system activity in majordepression. Basal and desipramine-induced alterations in plasma norepinephrinekinetics. Arch Gen Psychiatry May 1994;51(5):411–22.
[18] Nater UM, La Marca R, Florin L, et al. Stress-induced changes in human salivaryalpha-amylase activity—associations with adrenergic activity. Psychoneuroendo-crinology Jan 2006;31(1):49–58.
[19] Neumeister A, Wood S, Bonne O, et al. Reduced hippocampal volume inunmedicated, remitted patients with major depression versus control subjects.Biol Psychiatry Apr 15 2005;57(8):935–7.
[20] Sheline YI. Hippocampal atrophy in major depression: a result of depression-induced neurotoxicity? Mol Psychiatry Sep 1996;1(4):298–9.
[21] Bremner JD, NarayanM, Anderson ER, Staib LH, Miller HL, Charney DS. Hippocampalvolume reduction in major depression. Am J Psychiatry 2000;157:115–8.
[22] Sheline YI. 3D MRI studies of neuroanatomic changes in unipolar majordepression: the role of stress and medical comorbidity. Biol Psychiatry Oct 152000;48(8):791–800.
[23] Sapolsky RM, Krey LC, McEwen BS. The neuroendocrinology of stress and aging:the glucocorticoid cascade hypothesis. Endocr Rev 1986;7(3):284–301.
[24] Weissman MM, Bland RC, Canino GJ, et al. Cross-national epidemiology of majordepression and bipolar disorder. JAMA Jul 24–31, 1996;276(4):293–9.
[25] Kudielka BM, Kirschbaum C. Sex differences in HPA axis responses to stress: areview. Biol Psychol 2005;69:113–32.
[26] Young E, Korszun A. Women, stress, and depression: sex differences in hypotha-lamic–pituitary–adrenal axis regulation. In: LeibenluftE, editor.Genderdifferences inmood and anxiety disorders: from bench to bedside. Washington, D.C.: AmericanPsychiatric Press; 1999. p. 31–52.
[27] Frankenhaeuser M, Dunne E, Lundberg U. Sex differences in sympathetic–adrenalmedullary reactions induced by different stressors. Psychopharmacology (Berl)May 5 1976;47(1):1–5.
[28] Kirschbaum C, Wust S, Hellhammer D. Consistent sex differences in cortisolresponses to psychological stress. Psychosom Med Nov–Dec, 1992;54(6):648–57.
[29] Lundberg U, de Chateau P, Winberg J, Frankenhaeuser M. Catecholamine andcortisol excretion patterns in three-year-old children and their parents. J HumStress Sep 1981;7(3):3–11.
[30] van Stegeren AH, Wolf OT, Kindt M. Salivary alpha amylase and cortisol responsesto different stress tasks: impact of sex. Int J Psychophysiol Jul 2008;69(1):33–40.
[31] Nolen-Hoeksema S. Gender differences in depression. Curr Dir Psychol Sci2001;10:173–6.
[32] Eckenrode J, editor. The social context of coping. New York: Plenum Press; 1991.[33] Stroud LR, Salovey P, Epel ES. Sex differences in stress responses: social rejection
versus achievement stress. Biol Psychiatry Aug 15 2002;52(4):318–27.[34] Kirschbaum C, Pirke K-M, Hellhammer DH. The ‘Trier Social Stress Test’—a tool for
investigating psychobiological stress responses in a laboratory setting. Neurop-sychobiology 1993;28:76–81.
[35] al'Absi M, Bongard S, Buchanan TW, Pincomb GA, Licinio J, Lovallo WR.Cardiovascular and neuroendocrine adjustment to public speaking and mentalarithmetic stressors. Psychophysiology 1997;34(3):266–75.
[36] Watson D, Clark LA, Carey G. Positive and negative affectivity and their relation toanxiety and depressive disorders. J Abnorm Psychol Aug 1988;97(3):346–53.
[37] Granger DA, Kivlighan KT, el-Sheikh M, Gordis EB, Stroud LR. Salivary alpha-amylase in biobehavioral research: recent developments and applications. Ann NY Acad Sci Mar 2007;1098:122–44.
[38] Rohleder N, Nater UM. Determinants of salivary alpha-amylase in humans andmethodological considerations. Psychoneuroendocrinology May 2009;34(4):469–85.
[39] Kirschbaum C, Hellhammer DH. Salivary cortisol in psychobiological research: anoverview. Neuropsychobiology 1989;22:150–69.
[40] Carpenter Jr WT, Bunney Jr WE. Adrenal cortical activity in depressive illness. Am JPsychiatry Jul 1971;128(1):31–40.
[41] Burke HM, Davis MC, Otte C, Mohr DC. Depression and cortisol responses topsychological stress: a meta-analysis. Psychoneuroendocrinology Oct 2005;30(9):846–56.
[42] Knorr U, Vinberg M, Kessing LV, Wetterslev J. Salivary cortisol in depressedpatients versus control persons: a systematic review and meta-analysis.Psychoneuroendocrinology Oct 2010;35(9):1275–86.
[43] Nater UM, Rohleder N. Salivary alpha-amylase as a non-invasive biomarker for thesympathetic nervous system: current state of research. Psychoneuroendocrinol-ogy May 2009;34(4):486–96.
[44] Nater UM, Rohleder N, Schlotz W, Ehlert U, Kirschbaum C. Determinants of thediurnal course of salivary alpha-amylase. Psychoneuroendocrinology May2007;32(4):392–401.
[45] Nater UM, Rohleder N, Gaab J, et al. Human salivary alpha-amylase reactivity in apsychosocial stress paradigm. Int J Psychophysiol Mar 2005;55(3):333–42.
[46] Just N, Abramson LY, Alloy LB. Remitted depression studies as tests of the cognitivevulnerability hypotheses of depression onset: a critique and conceptual analysis.Clin Psychol Rev Feb 2001;21(1):63–83.
[47] Clark LA, Watson D. Tripartite model of anxiety and depression: psychometricevidence and taxonomic implications. J Abnorm Psychol Aug 1991;100(3):316–36.
[48] Watson D, Clark LA, Weber K, Assenheimer JS, Strauss ME, McCormick RA. Testinga tripartite model: II. Exploring the symptom structure of anxiety and depressionin student, adult, and patient samples. J Abnorm Psychol Feb 1995;104(1):15–25.
[49] Watson D, Weber K, Assenheimer JS, Clark LA, Strauss ME, McCormick RA. Testinga tripartite model: I. Evaluating the convergent and discriminant validity ofanxiety and depression symptom scales. J Abnorm Psychol Feb 1995;104(1):3–14.
[50] Gotlib I, Hammen C, editors. Handbook of depression. 2nd ed. New York: GuilfordPress; 2009.
[51] Haeffel GJ, Abramson LY, Voelz ZR, et al. Negative cognitive styles, dysfunctionalattitudes, and the remitted depression paradigm: a search for the elusive cognitivevulnerability to depression factor among remitted depressives. Emotion 2005;5:343–8.
[52] Watson D, Clark LA, Tellegen A. Development and validation of brief measures ofpositive and negative affect: the PANAS scales. J Pers Soc Psychol 1988;54:1063–70.
[53] Buchanan TW, Driscoll D, Mowrer SM, et al. Medial prefrontal cortex damageaffects physiological and psychological stress responses differently in men andwomen. Psychoneuroendocrinology Jan 2010;35(1):56–66.
[54] Buchanan TW, Tranel D. Stress and emotional memory retrieval: effects of sex andcortisol response. Neurobiol Learn Mem Feb 2008;89(2):134–41.
[55] Barrett LF, Robin L, Pietromonaco PR, Eyssell KM. Are women the “moreemotional” sex? Evidence from emotional experiences in social context. CognEmotion 1998;12:555–78.
[56] McClure EB. A meta-analytic review of sex differences in facial expressionprocessing and their development in infants, children, and adolescents. PsycholBull 2000;126:424–53.
[57] Davis PJ. Gender differences in autobiographical memory for childhood emotionalexperience. J Pers Soc Psychol 1999;76:498–510.
[58] Barrett LF, Lane RD, Sechrest L, Schwartz GE. Sex differences in emotionalawareness. Pers Soc Psychol Bull 2000;26:1027–35.











![Analysing user physiological responses for affective video ... · Analysing user physiological responses for affective video ... [52] summarise music videos automatically by using](https://img.pdfslide.net/doc/110x75/603579fb21ea6862b9609541/analysing-user-physiological-responses-for-affective-video-analysing-user-physiological.jpg)