Embed Size (px)
Citation preview

SGA 2003-W-6701-SS Slide 1Downloaded from – www.singulair.ae
Dual Pathways of Asthmatic Inflammation
CApacidad de SIngulair Oral en la Prevencion de Exacerbaciones Asmaticas
Montelukast with Inhaled Corticosteroids

SGA 2003-W-6701-SS Slide 2Downloaded from – www.singulair.ae
Adapted from National Institutes of Health Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention: A Pocket Guide for Physicians and Nurses. Publication No. 95-3659B. Bethesda, MD: National Institutes of Health, 1998; Bjermer L Respir Med 2001;95:703-719.
Importance of Inflammation in Asthma
• Asthma is fundamentally a disease of inflammation
• Inflammation causes bronchoconstriction and airway hyperresponsiveness, resulting in symptoms
• Treating inflammation first in patients with mild to moderate persistent asthma is an appropriate treatment approach

SGA 2003-W-6701-SS Slide 3Downloaded from – www.singulair.ae
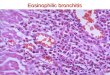
Airway Inflammation Persisted Despite Corticosteroid Use
ICS=inhaled corticosteroids; OCS ± ICS=received oral corticosteroids with or without ICS
Adapted from Louis R et al Am J Respir Crit Care Med 2000;161:9-16.
20,00010,000
1,000
100
10
1
Eosinophil 103/gsputum
Controlgroup
Mild to moderate
ICSlow-dose(n=10)
ICShigh-dose
(n=15)
OCS(n=10)
OCS ± ICS(n=7)
Severe asthma
p<0.01
p<0.001
p<0.001
p<0.01
In a clinical study of 74 patients

SGA 2003-W-6701-SS Slide 4Downloaded from – www.singulair.ae
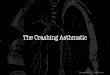
Leukotrienes
Other inflammatory mediators
This slide is an artistic rendition.
Adapted from Holgate ST, Peters-Golden M J Allergy Clin Immunol 2003;111(1 suppl):S1-S4; Holgate ST et al J Allergy Clin Immunol 2003;111(1 suppl):S18-S36; Henderson WR Jr et al Am J Respir Crit Care Med 2002;165:108-116; Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(1 suppl):S37-S42; Varner AE, Lemanske RF Jr. In Asthma and Rhinitis. Oxford, UK: Blackwell Science, 2000:1172-1185.
No Inflammation InflammationAsthma
Leukotrienes: Important in Early Asthma and Throughout the Disease

SGA 2003-W-6701-SS Slide 5Downloaded from – www.singulair.ae
• Suppression of a number of inflammatory mediators– Cytokines– Adhesion molecules– Inducible enzymes
• Variable effects on inflammatory processes
Adapted from Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(suppl 1):S37-S48.
Dual Pathways of Inflammation Actions of Corticosteroids

SGA 2003-W-6701-SS Slide 6Downloaded from – www.singulair.ae
Dual Pathways of Inflammation Effects of the CysLT1 Receptor on Inflammatory Cells
EosinophilsLung Macrophage
Smooth- musclecell
PBMC
CysLT=cysteinyl leukotriene; PBMC=peripheral blood mononuclear cells
Adapted from Figueroa DJ et al Am J Respir Crit Care Med 2001;163:226-233.
Monocytes

SGA 2003-W-6701-SS Slide 7Downloaded from – www.singulair.ae
Dual Pathways of Inflammation Expression of the CysLT1 Receptor
Neutrophil
Monocyte
Macrophage
Basophil
Pluripotent hemopoieticstem cell
T CellsEosinophil
B Lymphocyte
CCR3
CD4+CD8+
CD19
M-CSF, GM-CSF, IL-3
LTC4, LTD4, LTE4
LN5
Mast Cell
LTC4
LTD4
LTE4
M-CSFGM-CSF
IL-5IL-3
GM-CSFLTC4
LTD4
LTE4
CD14
IL5Rβ
Represents the CysLT1 receptor
Adapted from Figueroa DJ et al Am J Respir Crit Care Med 2001;163:226-233; Mellor et al Proc Natl Acad Sci USA 2001;98:7964-7969
CysLT1R
CD34+

SGA 2003-W-6701-SS Slide 8Downloaded from – www.singulair.ae
Adapted from Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(suppl 1):S37-S48.
Dual Pathways of Inflammation Leukotrienes Are Powerful Inflammatory Mediators
Mediatorreceptor
Othermediators
CysLTreceptor CysLT

SGA 2003-W-6701-SS Slide 9Downloaded from – www.singulair.ae
• Suppress many inflammatory mediators
• Suppress inflammatory processes– Via the leukotriene pathway– Via the steroid-sensitive pathway
LTRAs = leukotriene receptor antagonists
Adapted from Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(suppl 1):S37-S48.
Dual Pathways of Inflammation Actions of LTRAs
Leukotrienes are highly specific but catalyze a massive inflammatory cascade

SGA 2003-W-6701-SS Slide 10Downloaded from – www.singulair.ae
Dual Pathways of Inflammation Central Role of CysLTs in Asthma
Adapted from Hay DWP et al Trends Pharmacol Sci 1995;16:304-309.
Inflammatory Cells (mast cells, eosinophils)
Sensory Nerves
(C fibers)
CysLTsEdema
BloodVessel
Decreased Mucus Transport
EosinophilInflux
Cationic Protein Release,Epithelial-Cell Damage
Contraction and Proliferation
Airway Smooth Muscle
Increased Mucus
Secretion
Airway Epithelium

SGA 2003-W-6701-SS Slide 11Downloaded from – www.singulair.ae
p = NS between groups
Adapted from O’Shaughnessy KM et al Am Rev Respir Dis 1993;147:1472-1476.
18.720
16
12
8
4
0
Urinary LTE4
excretion(ng/mmol
creatinine)
18.4
PlaceboFluticasone propionate
Effect of Inhaled Fluticasone Propionate on Urinary LTE4 Excretion

SGA 2003-W-6701-SS Slide 12Downloaded from – www.singulair.ae
*
*p<0.05 vs. baseline
Adapted from Dworski R et al Am J Respir Crit Care Med 1994;149:953-959.
0.3
0.2
0.1
0
Urinary LTE4
(ng/mgcreatinine)
Post-allergen challenge
Baseline
ControlPrednisone
*
Effect of Oral Prednisone on Urinary LTE4 Excretion

SGA 2003-W-6701-SS Slide 13Downloaded from – www.singulair.ae
n=14
Adapted from Dworski R et al Am J Respir Crit Care Med 1994;149:953-959.
Oral Prednisone Did Not Suppress CysLT Levels Recovered from BAL Fluid
BAL = bronchoalveolar lavage
Adapted from Dworski R et al Am J Respir Crit Care Med 1994;149:953-959.
80
70
60
50
40
30
20
10
0
BALlevels(pg/ml)
LTE4LTC4
Before prednisoneAfter prednisone
Eicosanoids in Asthmatics

SGA 2003-W-6701-SS Slide 14Downloaded from – www.singulair.ae
*p<0.02 vs. normal individuals; **p<0.05 vs. normal individuals
Adapted from Pavord ID et al Am J Respir Crit Care Med 1999;160:1905-1909.
14
12
10
8
6
4
2
0
SputumCysLT levels(ng/ml)
Controls(n=10)
6.4
All patients with asthma
(n=26)
9.4*
Patients with persistent
asthma(n=10)
11.4**
Patients with acute attacks
(n=12)
13*
Effect of ICS on Sputum Leukotriene Levels

SGA 2003-W-6701-SS Slide 15Downloaded from – www.singulair.ae
LABA = long-acting beta2 agonist
Adapted from Currie GP et al Am J Respir Crit Care Med (in press).
Dual Pathways of Inflammation Long-Acting Beta2 Agonists Did Not Have Anti-inflammatory Effects
0
–100
–200
Change ineosinophils
( 106/L)from run-in
ICS + LABA + Montelukast
ICS +LABA ICS
ICS +Montelukast
p<0.05
p<0.05
LTRA montelukast further reduced inflammation when added to ICS

SGA 2003-W-6701-SS Slide 16Downloaded from – www.singulair.ae
*p<0.05 compared with beclomethasone
Adapted from LaViolette M et al Am J Respir Crit Care Med 1999;160:1862-1868.
0.12
0.10
0.08
0.06
0.04
0.02
0
Eosinophilcounts(change
from baseline 103/µl)
Placebo Beclomethasone Montelukast+
beclomethasone
Montelukast
*
<1*
Treatment group
Dual Pathways of Inflammation LTRA Montelukast Further Reduced Asthmatic Inflammation
Complementary therapy that targets dual pathways of inflammation provided better control of inflammation

SGA 2003-W-6701-SS Slide 17Downloaded from – www.singulair.ae
block steroid-sensitivemediators
blocks the effects of CysLTs
Inhaled steroidsMontelukast
Dual Pathways of Inflammation Montelukast Combined with a Steroid Affects the Dual Pathways of Inflammation
The slide represents an artistic rendition.
Adapted from Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(1 suppl):S37-S42; Bisgaard H Allergy 2001;56(suppl 66):7-11.
Steroid-sensitive mediators
play a key role in asthmatic inflammation
CysLTsplay a key role in asthmatic inflammation
Steroids do NOT inhibit CysLT formation in the airways of asthmatic patients
DUAL PATHWAY

SGA 2003-W-6701-SS Slide 18Downloaded from – www.singulair.ae
Dual Pathways of Inflammation Airway Inflammation Correlated with Lung Function and Clinical Control
FEV1 = forced expiratory volume in one second; PEFR = peak expiratory flow rate; rS = Spearman’s rank coefficient of correlation; ECP = eosinophilic cationic protein
Adapted from Louis R et al Am J Respir Crit Care Med 2000;161:9-16.
0
–0.2
–0.4
–0.6
rS
FEV1
Daily symptomscore
PEFRvariability
–0.51
Absolute eosinophil countsECP concentrations
–0.36
–0.49 –0.51
–0.43
–0.52

SGA 2003-W-6701-SS Slide 19Downloaded from – www.singulair.ae
• CysLTs and steroid-sensitive mediators are two important pathways of inflammation in asthma
• Corticosteroids do not block the leukotriene-mediated pathway of inflammation
• Treating dual pathways of inflammation in the airway of asthmatic patients may provide better control of inflammation and effective asthma control
Adapted from Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(1 suppl):S37-S42; Bisgaard H Allergy 2001;56(suppl 66):7-11.
Summary Targeting Dual Pathways of Inflammation Improves Asthma Control

SGA 2003-W-6701-SS Slide 20Downloaded from – www.singulair.ae
Capacity of Oral SINGULAIR to Prevent Asthma Exacerbations
CApacidad de SIngulair™ Oral en la Prevencion de
Exacerbaciones Asmaticas
SINGULAIR (montelukast sodium) is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA.

SGA 2003-W-6701-SS Slide 21Downloaded from – www.singulair.ae
Adapted from National Institutes of Health Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention: A Pocket Guide for Physicians and Nurses. Publication No. 95-3659B. Bethesda, MD: National Institutes of Health, 1998; Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(1 suppl):S37-S42; discussion S43-S48; LaViolette M et al Am J Respir Crit Care Med 1999;160:1862-1868; Bisgaard H Allergy 2001;56(suppl 66):7-11.
• Rationale– Leukotrienes are powerful inflammatory mediators
that are not blocked by steroids in the airways of asthmatic patients
– LTRAs can further reduce inflammation and improve symptoms when added to ICS therapy
• Additive effects on peripheral blood eosinophils, a marker of inflammation, shown in clinical studiesof LTRAs + ICS
– Effects of ICS + leukotriene-modifying treatment on reducing asthma exacerbations, a prominent goal of asthma therapy, must be evaluated
• Objective – To evaluate the addition of oral montelukast to
patients’ usual dose of inhaled budesonide in the treatment of adults with mild to moderate asthma
Rationale and Objective

SGA 2003-W-6701-SS Slide 22Downloaded from – www.singulair.ae
PEFR = peak expiratory flow rate
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
CASIOPEA Study
Primary Endpoint
% of Asthma Exacerbation Days
Defined as a day when any of the following occurred
• Awake all night (awake all night or recurrent episodes of awakening)
• Increase from baseline in symptom score of >50%
• Increase from baseline in beta-agonist use of >70% (minimum increase 2 puffs/day)
• Decrease from baseline of >20% in morning PEFR
• Morning PEFR <180 l/min
• Asthma attack (unscheduled medical care for asthma)

SGA 2003-W-6701-SS Slide 23Downloaded from – www.singulair.ae
Budesonide Turbuhaler 400–1600 µg qd
+ montelukast (n=326)
Budesonide Turbuhaler 400–1600 µg qd
+ placebo
(n=313)
qd = once daily
Inhaled short-acting beta2 agonists were permitted as needed.
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
CASIOPEA Study
Design
Period I
Weeks
Period II
Budesonide Turbuhaler
400–1600 µg/day
V1–2
V20
V24
V28
V516

SGA 2003-W-6701-SS Slide 24Downloaded from – www.singulair.ae
FEV1 = forced expiratory volume in one second
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
• Non-smoking asthmatic patients 18–70 years of age
• Prior treatment with a clinically stable dose of ICS equivalent to budesonide 400–1600 µg/day
• FEV1 55% of predicted
• Reversible airway obstruction (12% increase from baseline)
• Minimum total daytime asthma symptom score of 64 (of possible 336)
1 puff/day of beta2 agonist
CASIOPEA Study
Inclusion Criteria

SGA 2003-W-6701-SS Slide 25Downloaded from – www.singulair.ae
*Mean ± SD **Mean of scores to four questions, each rated on a scale of 0 (best) to 6 (worst)***44 (14%) and 35 (11%) patients on placebo and montelukast, respectively, received 400 µg/day
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
Montelukast Budesonide + Budesonide
(n=313) (n=326) Age, yr (range)* 44 ± 16 (18–79) 42 ± 15 (18–76)Gender, no.
Female 121 (39%) 124 (38%) Male 192 (61%) 202 (62%)
Duration of asthma, year* 13.8 ± 11.7 13.8 ± 11.4% of predicted FEV1* 81 ± 21 81 ± 19
Morning PEFR (L/min) 365 ± 108 373 ± 105Evening PEFR (L/min) 375 ± 108 382 ± 107Daytime asthma symptom score*,** 2.3 ± 0.8 2.2 ± 0.8Beta2-agonist use (puffs/day)* 3.3 ± 2.3 3.2 ± 2.5
Budesonide dose (µg/day), no.*** I. 400–800 202 (66%) 219 (69%) II. 801–1200 15 (5%) 18 (6%) III. 1201–1600 91 (30%) 80 (25%)
CASIOPEA Study
Baseline Characteristics of Patients

SGA 2003-W-6701-SS Slide 26Downloaded from – www.singulair.ae
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
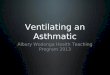
CASIOPEA Study
Montelukast + Budesonide Significantly Reduced Asthma-Exacerbation Days
4.8
3.1
Budesonide + placebo (n=308)
Montelukast + budesonide
(n=317)
Medianpercentageof asthma-
exacerbation days
5
4
3
2
1
0
35%p=0.03

SGA 2003-W-6701-SS Slide 27Downloaded from – www.singulair.ae
p=0.67 (ns) across strata
Adapted from additional analysis of CASIOPEA study: asthma exacerbation days per budesonide dose strata and onset of action for beta agonist use
Regardless of ICS dose
CASIOPEA Study
Montelukast + Budesonide Reduced Asthma-Exacerbation Days
10
8
6
4
2
0
No. ofasthma
exacerbationdays
I (n=421)
Budesonide + placeboMontelukast + budesonide
II (n=33)
III (n=171)
Strata of ICS dose

SGA 2003-W-6701-SS Slide 28Downloaded from – www.singulair.ae
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
CASIOPEA Study
Montelukast + Budesonide Significantly Increased Asthma-Free Days
42.3
66.1
Budesonide + placebo (n=308)
Montelukast + budesonide
(n=317)
Medianpercentageof asthma-free days
70
60
50
40
30
56%p=0.001

SGA 2003-W-6701-SS Slide 29Downloaded from – www.singulair.ae
*The percentage of patients who awoke during the night because of asthma
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
CASIOPEA Study
Montelukast + Budesonide Significantly Reduced Nocturnal Awakenings
25.6
Least square mean % of
patientswith nocturnalawakenings*
35
30
25
20
32.2
20%p=0.01
Budesonide + placebo (n=308)
Montelukast + budesonide
(n=317)

SGA 2003-W-6701-SS Slide 30Downloaded from – www.singulair.ae
*p = 0.05 vs. budesonide alone
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
CASIOPEA Study
Montelukast + Budesonide Significantly Reduced Beta2-Agonist Use*
% changefrom
baseline inbeta2-agonist
use
30
20
10
0
–10
–20
–30
–40
First 7 days in active treatment
Budesonide + placebo (n=313)Montelukast + budesonide (n=326)
Basal 1 2 3 4 5 6 7
A more rapid onset of action than budesonide + placebo

SGA 2003-W-6701-SS Slide 31Downloaded from – www.singulair.ae
CASIOPEA Study
Montelukast + Budesonide Significantly Increased AM PEFR*
Tertiary endpoint: Morning PEFR
Mean adjusted by center and stratum
*p = 0.05 vs. budesonide alone
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-21.
11.3
16.86
Budesonide + placebo (n=308)
Montelukast + budesonide
(n=317)
20
15
10
5
0
49%p=0.05
Least square mean change
in morningPEFR
(L/min)

SGA 2003-W-6701-SS Slide 32Downloaded from – www.singulair.ae
% of Patients Most Common Budesonide + Montelukast + Adverse Events placebo (n=313) budesonide (n=326) Influenza 11 12Headache 9 11Upper respiratory infection 7 5Worsening asthma 5 7Epigastric pain/pyrosis 2 3Urinary tract infection 2 2Rhinitis 2 2Pharyngitis 1 2Bronchitis 1 2Total 41 44
No significant differences between groups
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
Montelukast + Budesonide Was Well Tolerated
Incidence of adverse events comparable to budesonide + placebo

SGA 2003-W-6701-SS Slide 33Downloaded from – www.singulair.ae
Adapted from Vaquerizo MJ et al Thorax 2003;58:204-211.
• Montelukast added to patients’ usual dose of budesonide significantly improved asthma control (p0.05)– Effective control regardless of patients’
budesonide dose
• Faster onset of action than budesonide + placebo, evident from day 1
• Montelukast + budesonide was well tolerated, with a tolerability profile comparable to budesonide + placebo
CASIOPEA Study
Summary
Montelukast provided effective asthma control

SGA 2003-W-6701-SS Slide 34Downloaded from – www.singulair.ae
Adapted from Peters-Golden M, Sampson AP J Allergy Clin Immunol 2003;111(1 suppl):S37-S42; Currie GP et al Am J Respir Crit Care Med (in press); LaViolette M et al Am J Respir Crit Care Med 1999;160:1862-1868; Bisgaard H Allergy 2001;56(suppl 66):7-11; Vaquerizo MJ et al Thorax 2003;58:204-211.
Conclusions
• CysLTs and steroid-sensitive mediators comprise dual pathways of inflammation in asthma
• Corticosteroids at any dose do not block leukotrienes in the airways of asthmatic patients
• In clinical studies, complementary therapy with the LTRA montelukast and ICS effectively reduced inflammation and improved symptom control in patients with mild to moderate persistent asthma

SGA 2003-W-6701-SS Slide 35Downloaded from – www.singulair.ae
References
Please see notes page.

SGA 2003-W-6701-SS Slide 36Downloaded from – www.singulair.ae
Montelukast with Inhaled Corticosteroids
Targeting Dual Pathways of Asthmatic Inflammation
Before prescribing, please consult the manufacturers’ prescribing information.
Merck does not recommend the use of any product in any different manner than as described
in the prescribing information.
Copyright © 2003 Merck & Co., Inc., Whitehouse Station, NJ, USA.
All rights reserved. 4-05 SGA 2003-W-6701-SS Printed in USA
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com