Embed Size (px)
Citation preview
SGLT2 Inhibitors in CombinationTherapy: From Mechanisms toClinical Considerations in Type 2Diabetes ManagementDiabetes Care 2018;41:1543–1556 | https://doi.org/10.2337/dc18-0588
The progressive nature of type 2 diabetes (T2D) requires practitioners to periodicallyevaluate patients and intensify glucose-lowering treatment once glycemic targetsare not attained. With guidelines moving away from a one-size-fits-all approachtoward settingpatient-centered goals andallowingflexibility in choosing a second-/third-line drug from the growing number of U.S. Food and Drug Administration–approved glucose-lowering agents, keen personalized management in T2D hasbecome a challenge for health care providers in daily practice. Among the newergeneration of glucose-lowering drug classes, sodium–glucose cotransporter2 inhibitors (SGLT2is), which enhance urinary glucose excretion to lower hyper-glycemia, have made an imposing entrance to the T2D treatment armamentarium.Given their unique insulin-independent mode of action and their favorable efficacy–to–adverse event profile and given their marked benefits on cardiovascular-renaloutcome in moderate-to-high risk T2D patients, which led to updates of guidelinesand product monographs, the role of this drug class in multidrug regimes ispromising. However, despite many speculations based on pharmacokinetic andpharmacodynamic properties, physiological reasoning, and potential synergism,the effects of these agents in terms of glycemic and pleiotropic efficacy whencombined with other glucose-lowering drug classes are largely understudied. Inthis perspective, we review the currently emerging evidence, discuss prevailinghypotheses, and elaborate on necessary future studies to clarify the potential risksand benefits of using an SGLT2i in dual combination with metformin and triplecombination with a glucagon-like peptide 1 receptor agonist, dipeptidyl peptidase4 inhibitor, or other glucose-lowering agent that is recommended by the AmericanDiabetes Association and European Association for the Study of Diabetes (i.e., asulfonylurea, thiazolidinedione, or insulin) to treat patients with T2D.
Over the past decade, type 2 diabetes (T2D) management guidelines have movedforward from a one-size-fits-all recommendation toward a patient-centered approach(1–4). Two observations from landmark diabetes trials have encouraged this treatmentpersonalization that balances the benefits of glycemic control with its potential risksin the context of cardiovascular risk reduction, which includes lifestyle adaptations,blood pressure (BP) control, and lipid management. First, in particular in patients withlong-standing T2D, strict glycemic control may increase the risk of hypoglycemia,resulting in reduced quality of life and possibly increased cardiovascular risk, empha-sizing the importance of drug classeswith lowhypoglycemia risk. Second,while glucoselowering per se reduces or prevents the onset and development of microvascular
Diabetes Center, Department of Internal Medi-cine, VU University Medical Center, Amsterdam,the Netherlands
Corresponding author: Michael J.B. van Baar,[email protected].
Received 12 April 2018 and accepted 12 May2018.
M.J.B.v.B. and C.C.v.R. contributed equally to thiswork.
© 2018 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Michael J.B. van Baar,
Charlotte C. van Ruiten,
Marcel H.A. Muskiet,
Liselotte van Bloemendaal,
Richard G. IJzerman, and
Daniel H. van Raalte
Diabetes Care Volume 41, August 2018 1543
PER
SPECTIV
ESIN
CARE

complications, the impact of glucose con-trol on cardiovascular-renal complicationsis muchmore modest and emerges onlyafter many years, emphasizing the impor-tance of drug classes with cardiovascular-renal benefit. Although this concept ofpersonalization is highly appealing,manyhealth care providers are confrontedwith the predicament of how to pur-sue this approach in clinical practice, inparticular when multiple drugs areindicated.The preferred and most used first-line
pharmacotherapy to manage hypergly-cemia in T2D is indisputably metformin.Yet, six drug classes are currently recom-mended by the American DiabetesAssociation (ADA) and European Asso-ciation for the Study of Diabetes for
combination therapy on top of metformin:sodium–glucose cotransporter 2 inhibitors(SGLT2is), glucagon-like peptide 1 re-ceptor agonists (GLP-1RAs), dipeptidylpeptidase 4 inhibitors (DPP-4is), sulfo-nylureas, thiazolidinediones, and basalinsulin. All of these drug classes possessspecific modes of action, safety profiles,and cardiovascular-renal effects, whichraises the question of which combinationstrategy should be initiated after met-formin monotherapy failure. Ideally, thequantitative or net effect of a combina-tion is additive (i.e., sum of expectedactions of two drugs alone) or super-additive (i.e., greater than the expectedsum), which implies the use of glucose-lowering drug classes that mechanisti-cally address different components of
the prevailing pathophysiological de-fects and/or one drug favorably alteringthe actions of the other. Managementstrategies should exploit these combi-nation effects to maximize treatmentoutcome.
Since SGLT2is and GLP-1RAs exhibit alow hypoglycemia risk and members ofthese drug classes demonstrated signif-icant reductions in major adverse car-diovascular event (MACE) and mortalityoutcomes in recently reported cardio-vascular outcomes trials (CVOTs) forsafety, these drug classes have gainedparticular attention. In this perspective,we focus on SGLT2is in dual combinationwith metformin and triple combinationwith other glucose-lowering drug classesin T2D management.
Figure 1—Pathophysiology and drug targets. T2D is a heterogeneous disorder with a complex pathophysiology, in which genetic and environmentalfactors contribute to dysfunction of various organ systems that control glucose homeostasis (5,6). Insulin resistance of liver, adipose, and skeletalmuscle tissue results in respectively impaired insulin-induced reductionofHGP, lipolysis, and impaired insulin-stimulatedglucoseuptake(5).Hyperglycemiaevolves when pancreatic b-cells are unable to secrete sufficient insulin to overcome insulin resistance (i.e., b-cell failure). In addition, a-celldysfunction, characterized by fasting and postprandial hyperglucagonemia, stimulates HGP, which further augments hyperglycemia. Moreover, theefficacy of gut-derived incretin hormones GLP-1 and GIP to facilitate meal-related insulin release and glucagon suppression is impaired. The kidneyscontribute to hyperglycemia by increasing tubular glucose reabsorption, presumably through upregulation of SGLT2 and increased renalgluconeogenesis (7). Last, in the development of T2D, impaired activation of satiety centers in the brain stimulates excessive food intake, and insulinresistance in the brain may alter central control of metabolic homeostasis (45). Pleiotropic drug effects are illustrated by the frame and color of theboxes. Green indicates body weight loss, blue indicates body weight neutrality, and red indicates body weight gain. A dotted frame indicates bloodpressure reduction, and a solid frame indicates blood pressure neutrality. SU, sulfonylurea; TZD, thiazolidinedione.
1544 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018

PATHOPHYSIOLOGY OFHYPERGLYCEMIA IN T2DThe pathophysiology of T2D involvesvarious organs that control glucosehomeostasis, as reviewed extensivelyelsewhere and summarized in Fig. 1 (5,6).We highlight the increased glucose re-absorption, impaired incretin effect, andimpaired activation of satiety centers inthe brain, as these pathophysiologicaldefects have emerged as either estab-lished or potential therapeutic targets.The renal reabsorption of glucose is
controlled by two symporters that co-transport sodium and glucose. SGLT2 issituated at the first two convoluted seg-ments of the proximal tubule and, un-der physiological conditions, reabsorbs;90% of the filtered glucose, whereasthe remaining 10% is reabsorbed bySGLT1 located in the adjacent straightsegment. In T2D, the maximal reabsorp-tion capacity is raised, which preventsglycosuria and energy loss but adds tothe persistence of hyperglycemia.In response to food intake, gut endo-
crine cells secrete glucose-dependent in-sulinotropic polypeptide (GIP) and GLP-1.Both incretins have glucose-dependentinsulinotropic and glucagon-suppressingeffects (7), which cause oral glucose up-take to result in a 50–70% greater insulinresponse than glucose infused intrave-nously despite equality in plasma glucoselevels, a finding called the incretin effect.Due to rapid degradation by DPP-4 andthe liver, systemic concentrations are lowand insufficient to explain the full capac-ity of the incretin effect, suggesting thatGLP-1 mainly acts via local paracrine orautocrine rather than systemic actions.Although plasma incretin levels are notaffected, the incretin effect is impairedor even absent in T2D, which contributesto the disrupted glycemic control (8).Food intake is the result of complex
interactions between nutrients, hor-mones, neuropeptides, and several dif-ferent brain areas. Important centralnervous system structures that controlenergy balance and adjust food intake(i.e., homeostatic feeding) are the brain-stem and hypothalamus, as they re-ceive, convey, and integrate peripheralsignals of changes in nutrients, hormones,and neuropeptides. Other areas such asthe corticolimbic circuits are involvedin the cognitive, emotional, and reward-ing properties of food intake (i.e., non-homeostatic or hedonic feeding). In T2D,
impaired activation of satiety centersstimulates excessive food intake, andinsulin resistance in the brain may altercentral control of metabolic homeosta-sis (9).
SGLT2is
At present, four oral agents (i.e., canagli-flozin, dapagliflozin, empagliflozin, andertugliflozin) are approved for the treat-ment of T2D by the U.S. Food and DrugAdministration (FDA) and the EuropeanMedicines Agency, either as monother-apy or in combination with other glucose-lowering drug classes.
Glycemic ControlAccording to a 2013 meta-analysis,the glucose-lowering efficacy of SGLT2isin T2D patients without severe renalimpairment and baseline HbA1c of 6.9–9.2% is on average 0.79% when used asmonotherapy and 0.61% when used asadditional therapy (10). Since hypergly-cemia increases the filtered glucose load,the glycemic efficacy of this drug class inparticular is amplified at high baselinelevels. Conversely, since the filtered glu-cose load in patients with impaired renalfunction is reduced, the glucose-loweringefficacy parallels renal function and grad-ually declines to HbA1c reductions of 0.3–0.4% in estimated glomerular filtrationrate (eGFR) range 30–59 mL/min/1.73 m2
and no effect,30 mL/min/1.73 m2 (11).SGLT2is increase plasma glucagon levelsand stimulate hepatic glucose produc-tion (HGP), which restricts their glucose-lowering capacity. Considering that theirmode of action is independent of insulinresistance and b-cell failure, SGLT2is areeffective in all individuals with T2D andpreserved renal function.
Pleiotropic EffectsSGLT2is have several pleiotropic effects.First, SGLT2is induce weight loss of 2–3 kg, which starts with a fast decline of1–2 kg in the first weeks, which may bethe result of acute osmotic diuresis byblockade of the SGLT2 receptor (12).Thereafter, body weight declines moregradually over 20 weeks, which can berelated to reductions in fat mass, andsubsequently reaches a plateau phase(13). Interestingly, this 2- to 3-kg weightloss observed at the plateau phase is lessthan expected based on the calculatedloss of calories excreted in the urine,which would equal a weight reduction of;11 kg. Since SGLT2is do not alter resting
or postprandial energy expenditure (14),the discrepancy between expected andobserved weight loss implies that caloricintake is increased. Second, accordingto a 2017 meta-analysis, SGLT2is causepersistent reductions in systolic BP (SBP)and diastolic BP (DBP) of;5 and 2mmHg,respectively (15). Several mechanismsthat may underlie this antihypertensiveeffect have been suggested: 1) plasmavolume contraction by osmotic diure-sis; 2) weight loss; 3) improvements invascular stiffness by reductions in bodyweight, hyperglycemia-associated oxida-tive stress, and/or endothelial glycocalyxprotection from sodium overload; 4)reduced sympathetic nervous systemactivity; and 5) lower serum uric acidconcentrations (16). Third, SGLT2is mod-estly alter lipid profiles by reductionsin plasma triglycerides and increasesin HDL cholesterol and LDL cholesterol(11). Fourth, although the effects on liverhistology are unknown, SGLT2is attenu-ate several factors associated with non-alcoholic steatohepatitis (NASH) andnonalcoholic fatty liver disease (NAFLD),such as weight gain, elevated alanineaminotransferase, high liver fat index,and visceral fat (17). Fifth, SGLT2is in-duce natriuresis, which might improvewhole-body sodium balance and volumestatus (18), and are associated with im-proved endothelial function and re-duced vascular stiffening, decreasingthe demand placed on cardiac tissuethat causes left ventricular hypertrophy(19). Sixth, a study by Cherney et al.(20) suggested that in type 1 diabetes,SGLT2is reduce intraglomerular pres-sure by enhancing urinary sodium deliveryto the macula densa, thereby activatingtubuloglomerular feedback (TGF) and in-creasing afferent renal arteriolar resis-tance. While such mechanistic data arenot available in T2D, eGFR trajectories inphase 3 trials indicate acute reductions inglomerular hyperfiltration by means of aninitial drop and subsequent stabilizationof renal function over time, halting thenatural decline in eGFR. Last, presumablythrough reductions in intraglomerular pres-sure, SGLT2is attenuate albuminuria by30–40% (18). Interestingly, the effects ofSGLT2i on bodyweight, BP, and albuminuriaappear to be independent of eGFR (21).
Outcomes in CVOTsCardiovascular safety and benefit ofSGLT2is empagliflozin and canagliflozin
care.diabetesjournals.org van Baar and Associates 1545
Table
1—Reportedca
rdiova
scularandrenaloutcometrials
inT2D
(CVOTs)
Nam
eof
clinical
trial
Interven
tion
Population
Follow-up
(years)
Prim
aryoutcome
Keysecondary
outcome
CVdeath
MI¶
Stroke¶
HHF
Unstable
angina
hospitalization
All-cause
mortality
Worsen
ingof
nep
hropathy†
SGLT2is
EMPA
-REG
OUTC
OME
(n5
7,02
0)
Empagliflozin
vs.placebo
T2Dpatients
with
established
CVD
3.1
3-pointMACE
4-po
intMACE
0.62
(0.49–0.77
)0.87
(0.70–1.09
)1.18
(0.89–1.56
)0.65
(0.50–0.85
)0.99
(0.74–1.34)
0.68
(0.57–0.82
)0.61
(0.53–0.70
)
0.86
(0.74–0.99
)0.89
(0.78–1.01
)
CANVAS
Program
(n510,142)
Canagliflozin
vs.placebo
T2Dpatients
with
established
CVDor
$2CVrisk
factors
2.4
3-pointMACE
All-cause
andCV
mortality
0.96
(0.77–1.18
)**
0.89
(0.73–1.09
)#0.87
(0.69–1.09
)#0.67
(0.52–0.87)#
NA
0.87
(0.74–1.01
)**
0.60
(0.47–0.77)#
0.86
(0.75–0.97
)#0.87
(0.72–1.06
)#0.90
(0.76–1.07
)#
GLP-1RAs
ELIXA
(n5
6,06
8)
Lixisenatide
vs.placebo
T2Dpatients
with
arecentacute
coronaryeven
t
(,18
0daysbefore
screen
ing)
2.1
4-pointMACE
Expanded
MACE
0.98
(0.78–1.22
)1.03
(0.87–1.22
)1.12
(0.79–1.58
)0.96
(0.75 –1.23
)1.11
(0.47–2.62)
0.94
(0.78–1.13
)NA
1.02
(0.89–1.17
)1.00
(0.90–1.11
)
LEADER
(n5
9,34
0)
Liraglutidevs.
placebo
T2Dpatients
with
established
CVD,
kidney
disease,or
HFor$1CVrisk
factors
3.8
3-pointMACE
Expanded
MACE
0.78
(0.66–0.93
)0.86
(0.73–1.00
)0.86
(0.71–1.06
)0.87
(0.73–1.05
)0.98
(0.76–1.26)
0.85
(0.74–0.97
)0.78
(0.67–0.92
)
0.87
(0.78–0.97
)0.88
(0.81–0.96
)
SUSTAIN-6*
(n5
3,29
7)
Semaglutide
vs.placebo
T2Dpatients
with
established
CVD,
CKD
,orHFor$1
CVrisk
factors
2.1
3-pointMACE
Expanded
MACE
0.98
(0.65–1.48
)0.74
(0.51–1.08
)0.61
(0.38–0.99
)1.11
(0.77–1.61
)0.82
(0.47–1.44)
1.05
(0.74–1.50
)0.64
(0.46–0.88
)
0.74
(0.58–0.95
)0.74
(0.62–0.89
)
EXSCEL
(n514,752)
Exen
atideQW
vs.placebo
T2Dpatients
with
orwithout
established
CVD
3.2
3-pointMACE
Individual
componen
tsof
MACE
0.88
(0.76–1.02
)0.97
(0.85–1.10
)0.85
(0.70–1.03
)0.94
(0.78–1.13
)1.05
(0.94–1.18)
0.86
(0.77–0.97
)NA
0.91
(0.83–1.00
)
DPP
-4is
SAVOR-TIM
I
53(n
5
16,492
)
Saxagliptinvs.
placebo
T2Dpatients
with
ahistory
ofor
multiple
risk
factors
forCVD
2.1
3-pointMACE
Expanded
MACE
1.03
(0.87–1.22
)0.95
(0.80–1.12
)1.11
(0.88–1.39
)1.27
(1.07–1.51
)1.19
(0.89–1.60)
1.11
(0.96–1.27
)1.08
(0.88–1.32
)
1.00
(0.89–1.12
)1.02
(0.94–1.11
)
EXAMINE
(n5
5,38
0)
Alogliptinvs.
placebo
T2Dpatients
with
recentACS(15–90
daysbefore
randomization)
1.5
3-pointMACE
4-po
intMACE
0.85
(0.66–1.10
)1.08
(0.88–1.33
)0.91
(0.55–1.50
)1.19
(0.90–1.58
)0.90
(0.60–1.37)
0.88
(0.71–1.09
)NA
0.96
(95%
UL
#1.16)
0.95
(95%
UL#1.14
)
TECOS
(n514,671)
Sitagliptinvs.
placebo
T2Dpatients
with
established
CVD
3.0
4-pointMACE
3-po
intMACE
1.03
(0.89–1.19
)0.95
(0.81–1.11
)0.97
(0.79–1.19
)1.00
(0.83–1.20
)0.90
(0.70–1.16)
1.01
(0.90–1.14
)NA
0.98
(0.89–1.08
)0.99
(0.89–1.10
)
Thiazolidined
iones
PROactive
(n5
5,23
8)
Pioglitazone
vs.placebo
T2Dpatients
with
established
CVD
2.8
Expanded
MACE
3-po
intMACE
0.94
(0.74–1.20
)0.83
(0.65–1.06
)0.81
(0.61–1.07
)1.41
(1.10–1.80
0.78
(0.55–1.11)
0.96
(0.78–1.18
)NA
0.90
(0.80–1.02
)0.84
(0.72–0.98
)
TOSCA.IT
(n5
3,02
8)
Pioglitazone
vs.
sulfonylurea
T2Dpatients
withou
trecentCV
even
ts(.
6
months)
orCHF
4.8
Expanded
MACE
Expanded
MACE
2.24
(0.69–7.28
)0.87
(0.48–1.55
)0.79
(0.41–1.53
)1.57
(0.76–3.24
)NA
1.10
(0.75–1.61
)NA
0.96
(0.74–1.26
)0.88
(0.65–1.21
)
Con
tinu
edon
p.15
47
1546 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018

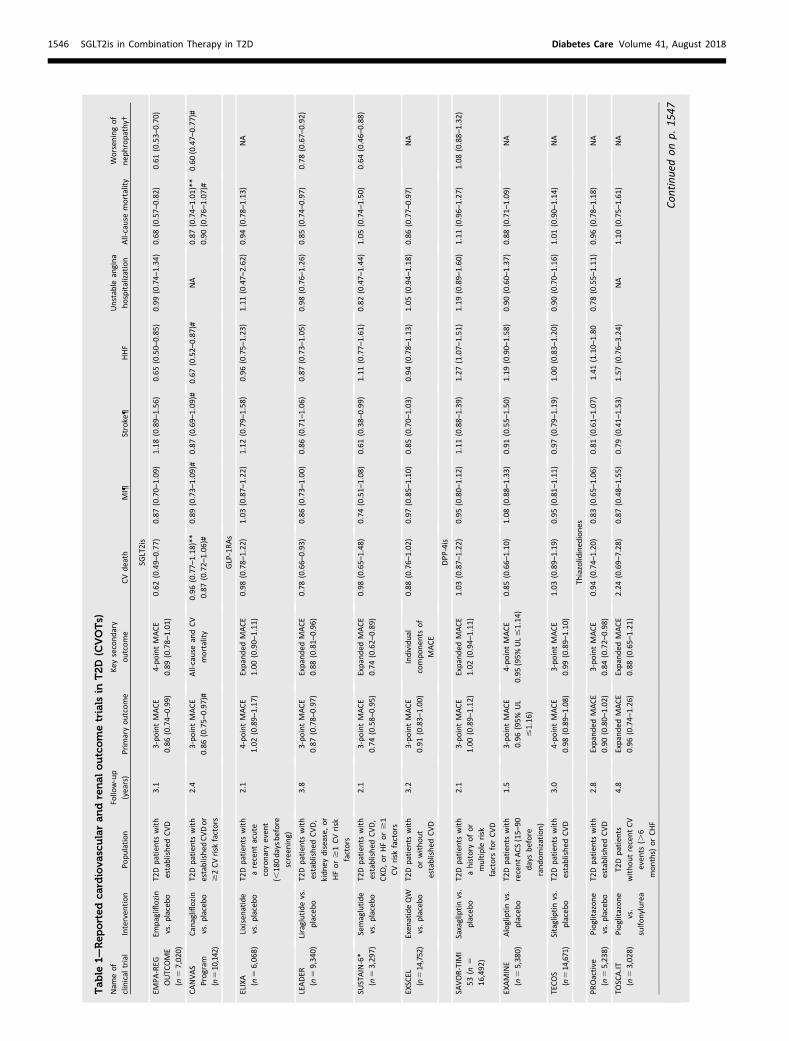
were demonstrated in the BI 10773(Empagliflozin) Cardiovascular OutcomeEvent Trial in Type 2 Diabetes MellitusPatients (EMPA-REG OUTCOME) trial andthe Canagliflozin Cardiovascular Assess-ment Study (CANVAS) Program (i.e., twostudies, CANVAS and CANVAS-Renal[CANVAS-R], jointly reported) (22,23).Importantly, nearly all included patientswere adequately treated with statins andBP-lowering agents, most notably renin-angiotensin-aldosterone system (RAAS)inhibitors (;80%). In EMPA-REG OUT-COME, the incidence of cardiovasculardeath was reduced, whereas in bothEMPA-REG OUTCOME and the CANVASProgram, a reduction in hospitalizationfor heart failure (HHF) and incident orworsening of nephropathy was observed(Table 1) (22–24). Since the subtle im-provements in cardiovascular risk fac-tors are unlikely to contribute to thelarge and early benefit, there has beenmuch speculation about the underlyingmechanisms. In a post hoc analysis ofEMPA-REG OUTCOME, plasma volumecontraction, estimated by hematocrit con-centration, has been put forward (25).Other explanations include alterations ofcardiac substrate metabolism and directeffects on the cardiomyocyte (26,27).
Adverse EffectsSGLT2is are well tolerated and have a lowhypoglycemia risk in patients not usingsulfonylureas or insulin. The main ad-verse effect is a four- to fivefold increasedrisk of genital mycotic infection (11).Rare episodes of diabetic ketoacidosis(DKA), particularly in patients with long-standing T2D, have been reported, whichprompted the FDA to issue a warn-ing about this potential complication.SGLT2is have the propensity to causeDKA due to a reduced availability of car-bohydrates caused by SGLT2i-inducedglycosuria, a shift in substrate utilizationfrom glucose to fat oxidation, and the pro-motion of hyperglucagonemia, stimulat-ing ketogenesis (28). Finally, in theCANVASProgram, canagliflozin was associated witha higher risk of bone fractures and lower-limb amputations (22), which have notbeen reported with other SGLT2is.
SGLT2 INHIBITION INCOMBINATION THERAPY
Since the glucose-lowering mechanismof SGLT2is does not interact with drugsthat improve b-cell function or insulin
Table
1—Continued
Nam
eof
clinical
trial
Interven
tion
Population
Follow-up
(years)
Prim
aryoutcome
Keysecondary
outcome
CVdeath
MI¶
Stroke¶
HHF
Unstable
angina
hospitalization
All-cause
mortality
Worsen
ingof
nep
hropathy†
Insulin
DEV
OTE
(n5
7,63
7)
Insulin
degludec
vs.
insulin
glargine
T2Dpatients
with
established
CVD,
CKD
,orHFor$1
CVrisk
factors
2.0
3-pointMACE
Expanded
MACE
0.96
(0.76–1.21
)0.85
(0.68–1.06
)0.90
(0.65–1.23
)NA
0.95
(0.68–1.31)
0.91
(0.78–1.06
)NA
0.91
(0.78–1.06
)0.92
(0.80–1.05
)
Adaptedfrom
Cefaluet
al.(99).Fourmem
bersoftw
odifferent
drugclassesdem
onstratedcardiovascular(CV)ben
efitin
CVOTs.In
EMPA
-REG
OUTC
OME,
empagliflozindem
onstrateda14
%reductionin
primaryen
dpoint3-pointMACE,
mainly
drivenbya38
%reductionin
cardiovasculardeath.Moreo
ver,a35
%risk
reductionin
HHFem
ergedafterseveralmonths,suggestingacute
effectsonrenal
andsystem
ichem
odynam
icfunctionordirecteffectsonthecardiovascularsystem
.Also,
new
-onsetorworsen
ingnep
hropathywas
reducedby39%.Thesecondaryoutcomes
ofCANVASandCANVAS-Rhavebeenrevisedto
prioritize
cardiovasculardeath,all-causemortality,
andHFandto
improve
theoutcom
esMIandstroke.Instead
ofreportingtheseparated
dose
effects,theresultsofboth
studiesanddoseswerecombined
andreported
astheCANVASProgram.Canagliflozinreducedtheprimaryen
dpoint3-pointMACEby14
%andHHFrisk
by33
%.Thecomposite
renal
outcomewas
reduced
by40
%.In
LEADER
,liraglutide
reducedprimaryen
dpoint3-pointMACEby13
%,withreductionofeq
ual
size
inallthreecomponen
ts.In
SUSTAIN-6,semaglutidereducedtheprimaryen
dpoint3-pointMACEby26
%,withthe
greatest
reductionsin
thestroke
category.In
conclusion,theben
efitofSG
LTisislikelyrelatedto
reductionsin
HF,
whichisdissimilarto
themore
antiatherogenicreductionsseen
withGLP-1RAs.Alloutcomes
areHR(95%
CI),exceptforEXAMINE
secondaryoutcome,
whichgivesa95
%upper
limit.95%
UL,upper
limitof95%
CI;ACS,
acute
coronarysyndrome;
CHF,
congestiveheart
failure;DEV
OTE,ATrialComparingCardiovascularSafety
ofInsulin
Degludec
VersusInsulin
Glarginein
Patien
tsWithType2Diabetes
atHighRiskofCardiovascularEven
ts;NA,notassessed/notreported
.*Powered
torule
outan
HRupper
margin$1.8;
superiority
hypothesisnotprespecified
.#N
ontrun
catedintegrated
data(refersto
pooleddatafrom
CANVAS,
includingbefore
20Novem
ber
2012
plusCANVAS-R).**Truncatedintegrated
dataset(refersto
pooleddatafrom
CANVASafter20
Novembe
r2012
plusCANVAS-R;prespecified
intreatinghierarchyas
theprincipal
datasetforanalysisforsuperiority
ofall-causemortalityandCVdeath
intheCANVASProgram
).¶Rep
orted
forfatalandnonfataleven
tsin
alltrialsexceptEXAMINE,
ELIXA,SU
STAIN-6,PR
Oactive,andTO
SCA.IT,whichreported
fornonfataleven
tsonly.†Worsen
ingnep
hropathywas
defi
ned
asdoublingofcreatininelevel,initiationofdialysis,renal
transplantation,orcreatinine.6.0mg/dL(530
mmol/L)
inSA
VOR-TIM
I53
;as
thenew
onsetofmacroalbuminuria(urineACR.30
0mg/g)
oradoublingoftheserum
creatininelevel
andan
eGFR
of#45
mL/min/1.73m
2,theneedforcontinuou
srenal-rep
lacemen
ttherapy,
ordeath
from
renal
disease
inLEADER
,SU
STAIN-6,andEM
PA-REG
OUTC
OME;
andas
40%
reductionin
eGFR,renal-rep
lacemen
ttherapy,
ordeath
from
renal
causesin
CANVAS.
Worsen
ingnep
hropathywas
aprespecified
exploratory
adjudicated
outcomein
SAVOR-TIM
I53
,LEADER
,SU
STAIN-6,andCANVASbutnotin
EMPA
-REG
OUTC
OME.
care.diabetesjournals.org van Baar and Associates 1547

sensitivity, combination therapy mightresult in additive efficacy (Fig. 2). More-over, the efficacy of SGLT2is may behampered by increased caloric intakeand increased HGP, disadvantages thatcan be mitigated by concomitant treat-ment with another agent. Also, otheragents might have pleiotropic effectsthat modulate cardiovascular-renal riskdifferently. Therefore, combination ther-apy with SGLT2is has potential benefitson both the preservation of glycemiccontrol and cardiovascular-renal com-plications (Table 2) (29–31).
SGLT2is and GLP-1RAs
GLP-1RAsSince exogenous GLP-1, in contrast toGIP, still exerts an insulinotropic effectin T2D patients, GLP-1RAs were de-veloped to mimic the effects of na-tive GLP-1, reducing blood glucose by
stimulating insulin and suppressing glu-cagon secretion in a glucose-dependentmanner (Fig. 1). Seven GLP-1RAs, namelyshort-acting exenatide, liraglutide, andlixisenatide and long-acting exenatide,semaglutide, dulaglutide, and albiglu-tide have been approved by the FDAand the European Medicines Agency forthe treatment of T2D. GLP-1RAs reduceHbA1c levels by ;1%, which varies be-tween agents based on their mode ofaction (32). Short-acting GLP-1RAs areinjected preprandially, causing sup-pressed postprandial glucagon levelsand decreased gastric emptying rates,which prolongs the rate of glucose entryinto the duodenum and blunts theabsorption of meal-derived glucose, col-lectively lowering postprandial hyper-glycemia. Because of the uninterruptedinsulin stimulation, long-acting GLP-1RAshave a more pronounced effect on HbA1c
and fasting plasma glucose (FPG). Thelack of efficacy of long-acting GLP-1RAsin reducing meal-related hyperglycemiamight be explained by rapid tachyphyl-axis of GLP-1RA–induced gastric empty-ing deceleration (33).
GLP-1RAs induce several pleiotropiceffects. The associated weight loss of;3 kg is the result of delayed gastricemptying, peripheral vagal nerve stim-ulation, and central nervous systemactivation, which collectively promotesatiety, decrease hunger sensation,and ultimately lead to a reduction infood intake, involving brain areas as-sociated with both homeostatic andhedonic feeding (9,34). Moreover, GLP-1RAs cause SBP and DBP reductions of;3 and 1 mmHg, respectively (35), andimprovements in lipid profiles by reduc-tions in LDL cholesterol, total cholesterol,and triglycerides (36). In addition, GLP-1RAs activate several anti-inflammatorypathways, including reductions in oxida-tive stress via reactive oxygen species,nuclear factor-kB binding/activation, ex-pression of inflammatory cytokines andC-reactive protein, and increases in adi-ponectin (37). Also, GLP-1RAs seem tohave beneficial effects on NASH andNAFLD by reductions in body weight,de novo hepatic lipogenesis, oxidativestress, inflammatory cytokines, andendoplasmatic reticulum stress and im-provements in hepatic insulin sensitiv-ity, triglyceride handling, and neuralregulation of hepatic metabolism (38,39).In the Liraglutide Efficacy and Action inNon-Alcoholic Steatohepatitis (LEAN)trial, liraglutide reduced liver enzymesand oxidative stress and improved liverhistology in patients NAFLD and T2D(40).
The CVOTs investigating lixisenatide(Evaluation of Lixisenatide in Acute Cor-onary Syndrome [ELIXA]), liraglutide(Liraglutide Effect and Action in Diabe-tes: Evaluation of Cardiovascular OutcomeResults [LEADER]), semaglutide (Trial toEvaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Sub-jects With Type 2 Diabetes [SUSTAIN-6]),and exenatide (Exenatide Study of Car-diovascular Event Lowering [EXSCEL])all reported cardiovascular safety (Table1) (41–44). LEADER and SUSTAIN-6demonstrated cardiovascular benefit,whereas the improved cardiovascularoutcome in EXSCEL just missed statisticalsignificance (hazard ratio [HR] 0.91; 95%
Figure 2—Mechanistic principles for net effects of drugs in combination therapy. The quantitativeor net effect of two or more drugs depends on whether the individual drug effects are in-dependent or interactive. When drug effects are independent, the quantitative effect is eitheradditive or subadditive. When drug effects interact, the quantitative effect can be subadditiveby antagonism or interference, or superadditive by enhancement or synergism. The effect ofthe individual drugs is indicated next to the arrows, and the net effect of the combination isindicated by the number at the right of each pair. Themaximumeffect is 100. A represents drugA, and B represents drug B. The top panel illustrates mechanisms for drugs with independentactions, with additivity occurring if tissue responsiveness permits both drug A and drug B toexert their full effect (left) but with subadditivity occurring if tissue responsiveness is thelimiting factor for the totalmagnitude of response possible (right). The bottompanel illustratesmechanisms for drugs with interactive actions. The left side of the bottom panel illustrates twopossibilities for subadditivity: simple antagonism (top), in which drug B reduces the effect ofdrug A threefold (indicated by the red inhibition line) but has no effect on its own, andinterference (bottom), in which drug B reduces the effect of drug A threefold (indicated by thered inhibition line), preventing it from exerting its full response, but drug B nonetheless hasa beneficial effect on its own. The right side of the bottom panel illustrates two possibilities forsuperadditivity: enhancement, in which drug B increases the effect of drug A twofold (greenarrow) but hasno effect on its own (top), and synergism, inwhichdrugBexerts a useful effect onits own in addition to its twofold enhancement of the effects on drug A (bottom).
1548 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018
CI 0.83–1.00; P = 0.06 for superiority).ELIXA could not demonstrate cardiovascu-lar benefit. The cardiovascular benefit ofliraglutide was driven by reductions inboth all-cause and cardiovascular mortality,whereas semaglutide mainly affected non-fatal stroke. These benefits of GLP-1RAtreatment are likely mediated by antiather-osclerotic mechanisms, which could be theresult of the activated anti-inflammatorypathways. The renal outcome improvedwith both liraglutide and semaglutide,mainly driven by reductions in macro-albuminuria. In all CVOTs, GLP-1RAs re-duced progression of albuminuria overtime ranging from 22 to 46%, yet it re-mains uncertain whether these effectsare truly independent of glucose controlas HbA1c differences between groupswere considerable (45). However, in re-sponse to a comment, the authors ofLEADER showed that adjustment forHbA1c, body weight, and SBP did not alterthe composite renal outcome (46). In thesame study, liraglutide decelerated theeGFR decline by 2% (27.44 vs. 27.82mL/min/m2 in 36 months) from baselinecompared with placebo, most evidentlyin patients with baseline eGFR 30–59 mL/min/1.73 m2. In prepublished results ofthe Study Comparing Dulaglutide WithInsulin Glargine on Glycemic Control inParticipants With Type 2 Diabetes andModerate or Severe Chronic Kidney Dis-ease (AWARD-7) (47), a randomized open-label study comparing once-weekly(QW) dulaglutide (0.75 mg or 1.5 mg)
with insulin glargine plus prandial insulinlispro in 576 T2D subjects with stage 3–4chronic kidney disease (CKD), dulaglu-tide showed greater reductions in al-buminuria (albumin-to-creatinine ratio[ACR] of227.7 and226.7, respectively,vs. 216.4 in the placebo group) andagain decelerated the eGFR declineslightly compared with insulin glargine.The mechanisms responsible for theserenal benefits are not completely un-derstood. Current suggestions involvethe effect of reductions in body weightand BP, anti-inflammatory effects, andalteration of renal hemodynamics eitherby inhibition of vasodilation of the affer-ent renal arteriole by activation of TGF viadownregulation of the sodium-hydrogenexchanger isoform 3 receptor locatedprior to the macula densa or by inhibi-tion of factors that cause constriction ofthe efferent arteriole, such as reactiveoxygen species, RAAS components, andendothelin-1. Moreover, it has beensuggested that GLP-1RAs act on neuralregulation centers of sodium and waterhomeostasis. Paradoxically, GLP-1RAsalso cause direct GLP-1R–mediated andindirect nitric oxide–dependent vasodi-lation of the afferent arteriole, causing anincrease in glomerular pressure. The ef-fect on renal function is thus a complexbalance between direct afferent vasodi-latory actions and inhibition of pathwaysassociated with glomerular hyperfiltration.Since T2D patients have impaired nitricoxide–dependent vasodilatory capacity,
the presence of glomerular hyperfiltra-tion could well be essential for incretintherapies to exert their renoprotectiveeffect (45,48).
Common adverse effects of GLP-1RAsare nausea and occasional vomiting, whichare usually mild to moderate and tran-sient (49). In SUSTAIN-6, increased ratesof retinopathy were observed, more likelycaused by rapid glucose reductions thandrug-specific effects. The putative rela-tionship between GLP-1RAs and pancre-atitis has been extensively debated (50).In a comprehensive 2017 meta-analysis,there was no association between acutepancreatitis and GLP-1RAs (51). This wasconfirmed by the 2017 meta-analysisof all CVOTs of GLP-1RAs by Bethel et al.(52).
Glycemic ControlTwo clinical trials have examined theglucose-lowering efficacy of SGLT2is com-bined with GLP-1RAs in T2D patients.In DURATION-8 (53), 695 metformin-treated participants were allocated todapagliflozin 10 mg, exenatide 2 mg, ordapagliflozin plus exenatide 2/10 mg.Combination therapy reduced HbA1cby 2.0% from baseline 9.3%, whichwas significantly more than exenatideor dapagliflozin alone (Fig. 3) (53).In Study of Dulaglutide (LY2189265)in Participants With Type 2 Diabe-tes Mellitus (AWARD-10) investigating424 patients randomly assigned to24-week dulaglutide 1.5 and 0.75 mgor placebo added to ongoing SGLT2itreatment and metformin, combinationtherapy led to significant greater HbA1creductions of 1.34 and 1.21%, respec-tively, vs. 0.54% with placebo from amean baseline of 8.0% (54). In a post hocsubgroup analysis of CANVAS involving95 patients with baseline HbA1c of 7.9–8.3%, addition of canagliflozin to GLP-1RA treatment reduced HbA1c by 1.00%(95% CI 0.65–1.35) for 100mg and 1.06%(95% CI 0.69–1.43) for 300mg comparedwith placebo (55). The achieved netglycemic efficacy of the combination issubadditive, which could be explainedby the interactive effects on glucagonand HGP, but could also be the result ofa more comprehensive interactive ef-fect. As elegantly explained by Polidoriet al. (56), the glucose-lowering efficacyof all glucose-lowering agents dependson the level of hyperglycemia, whichmeans that subadditivity can be expected
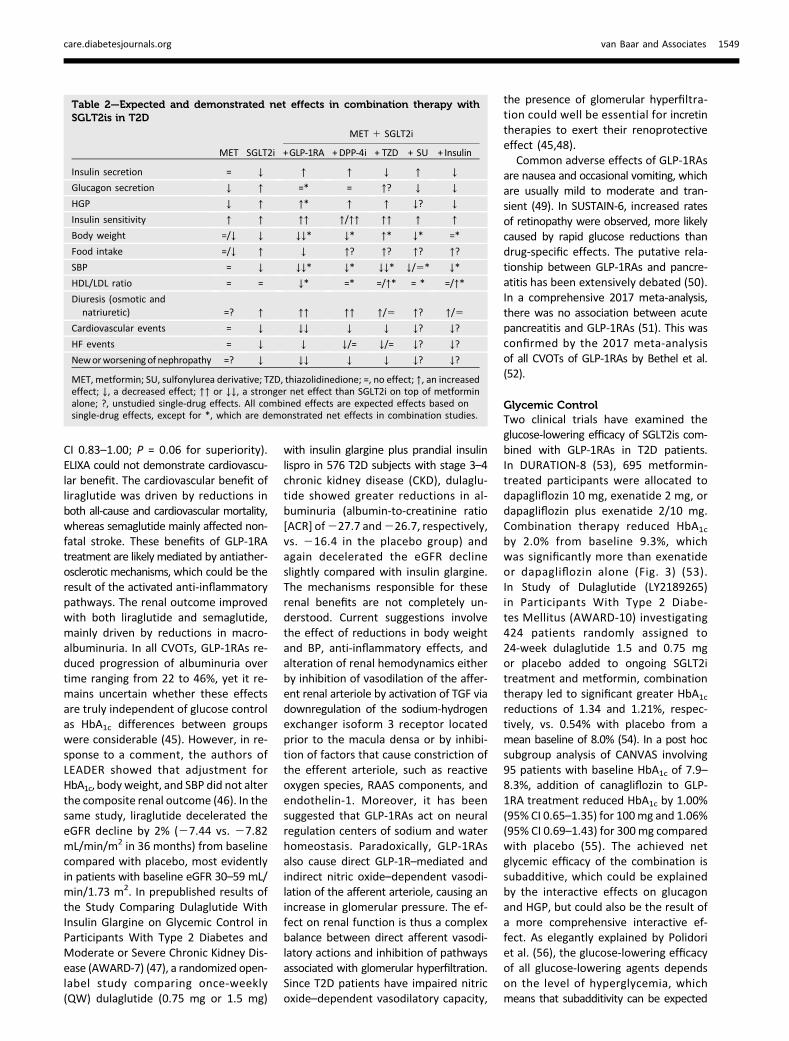
Table 2—Expected and demonstrated net effects in combination therapy withSGLT2is in T2D
MET SGLT2i
MET 1 SGLT2i
+GLP-1RA +DPP-4i + TZD + SU + Insulin
Insulin secretion = ↓ ↑ ↑ ↓ ↑ ↓
Glucagon secretion ↓ ↑ =* = ↑? ↓ ↓
HGP ↓ ↑ ↑* ↑ ↑ ↓? ↓
Insulin sensitivity ↑ ↑ ↑↑ ↑/↑↑ ↑↑ ↑ ↑
Body weight =/↓ ↓ ↓↓* ↓* ↑* ↓* =*
Food intake =/↓ ↑ ↓ ↑? ↑? ↑? ↑?
SBP = ↓ ↓↓* ↓* ↓↓* ↓/5* ↓*
HDL/LDL ratio = = ↓* =* =/↑* = * =/↑*
Diuresis (osmotic andnatriuretic) =? ↑ ↑↑ ↑↑ ↑/5 ↑? ↑/5
Cardiovascular events = ↓ ↓↓ ↓ ↓ ↓? ↓?
HF events = ↓ ↓ ↓/= ↓/= ↓? ↓?
Neworworseningof nephropathy =? ↓ ↓↓ ↓ ↓ ↓? ↓?
MET, metformin; SU, sulfonylurea derivative; TZD, thiazolidinedione; =, no effect; ↑, an increasedeffect; ↓, a decreased effect; ↑↑ or ↓↓, a stronger net effect than SGLT2i on top of metforminalone; ?, unstudied single-drug effects. All combined effects are expected effects based onsingle-drug effects, except for *, which are demonstrated net effects in combination studies.
care.diabetesjournals.org van Baar and Associates 1549

for all possible combinations that do notevoke synergism. Unfortunately, this combi-nation does not result in the glycemic syn-ergy so hoped for but is subadditive as aresult of interference.
Pleiotropic EffectsIn DURATION-8, a nearly additive netbody weight reduction of 3.41 kg (mean
baseline weight 91 kg) in patients re-ceiving combination treatment was ob-served. Moreover, a net SBP reductionof 4.2 mmHg from baseline 131 mmHgsuggested synergy and a possible inter-action between drugs (Fig. 3). No signif-icant differences in lipid levels betweenthe treatment groups were observed.AWARD-10 demonstrated that addition
of dulaglutide to ongoing SGLT2i treat-ment further reduced body weight by3.1 and 2.6 kg and SBP by 4.5 and 3.2mmHg for the 1.5 and 0.75 mg doses, re-spectively. In the context of DURATION-8,it is remarkable that addition of dulaglutidein AWARD-10, in particular in the lowdose, struggles to significantly stand outagainst placebo. This could be explainedby the substantial HbA1c, FPG, body weight,and SBP reductions seen in the placebogroup, which reveal an ongoing SGLT2ieffect. For instance, background SGLT2itreatment was initiated mostly just 3–6months prior to randomization, which isbefore the body weight plateau phase.Although it seems that dulaglutide hasadded benefits even on top of ongoingSGLT2i effects, it is not entirely possibleto separate and quantify the GLP-1RA-and SGLT2i-induced actions given the de-sign of the trial. In the post hoc analysisof CANVAS, placebo-subtracted reduc-tions when canagliflozin 100 or 300 mgwas added to GLP-1RA therapy were 2.7and 3.3 kg in body weight and 7.0 and6.9 mmHg in SBP, respectively. The effecton lipids was again neutral. The com-bined effect on NASH and NAFLD hasnot been studied; however, since bothdrug classes improve related etiologicfactors and reduce visceral fat and GLP-1RAs demonstrated efficacy in liver his-tology, the combination has additivepotency in the treatment of these diseases(40,57).
Both drug classes exert distinct renalbenefits, which combined could leadto additive or synergistic effects on thepreservation of renal function. For in-stance, as glucagon induces glomerularhyperfiltration via TGF-mediated dilata-tion of the afferent arteriole, a reductionof glucagon by incretin therapy could po-tentiate the effects of SGLT2is on TGF.Combination therapy thus has promisingrenalbenefits,whichcall for further study.
Outcomes in CVOTsCardiovascular safety or benefit has notbeen studied for this combination. Asboth agents reduce cardiovascular riskthrough different mechanisms (athero-genic and volume related, respectively),they might produce an additive cardio-vascular benefit, a hypothesis that re-quires further study. Conversely, there isalso the possibility that beneficial effectscan be limited by interference. For in-stance, the substrate shift hypothesis
Figure 3—Additivity in glycemic and pleiotropic effects. Reductions from baseline in combinationtherapy vs. either agent alone. At the moment, four studies have investigated the net effects ofglucose-lowering combination therapy with SGLT2is on top of metformin, one with GLP-1RAs andthree with DPP-4is. Frıas et al. (53) investigated the effect of 28-week exenatide 2 mg QW incombination with dapagliflozin 10 mg once daily (QD) on top of metformin in 695 T2D patients.DeFronzo et al. (96) investigated the effects of 52- and 24-week empagliflozin and linagliptin on topof metformin in 686 T2D patients. Given data derive from 24-week empagliflozin 10 mg QD andlinagliptin 5 mg QD, except for SBP data, which derive from 52-week therapy in the same dose.Pratley et al. (97) assessed the effects of 52- and 26-week ertugliflozin and sitagliptin in 1,233 T2Dpatients on top of metformin. Data derive from 26-week ertugliflozin 5 mg QD and sitagliptin100 mg QD. Rosenstock et al. (98) assessed the effects of 24-week dapagliflozin 10 mg QD andsaxagliptin 5 mg QD in 534 T2D patients on top of metformin.
1550 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018

regarding the benefits of SGLT2i on heartfailure (HF) postulates beneficial effectsof increased ketogenesis on the heart.GLP-1RAs could mitigate this effect bylowering glucagon levels.
Adverse EventsThe combination of GLP-1RAs andSGLT2is is associated with a low hypo-glycemia risk due to their glucose-dependent efficacy. The risk of DKA mightbe offset by the glucagon-suppressingproperties of GLP-1RAs. In both DURATION-8 and AWARD-10, combination therapywas well tolerated and side effects werenot different than those that could beexpected from either agent alone.
Pathophysiological RationaleThe stimulation of insulin and sup-pression of glucagon by GLP-1RAscomplements the insulin-independentpathophysiological defect targeted bySGLT2is and compensates for theSGLT2i-induced increase of HGP. Despitethis elegant rationale, the net glycemicefficacy is subadditive. DeFronzo et al.(58) investigated this result in more de-tail, showing that liraglutide indeed in-hibited canagliflozin-induced incrementsin glucagon levels but failed to antago-nize the rise in HGP, an observation thatneeds additional study. The combinationresults in nearly additive body weightloss, suggesting that deceleration of gas-tric emptying and reduction of foodintake by GLP-1RAs do not limit theweight-reducing efficacy by glycosuriawith SGLT2is. It remains unclear whetherGLP-1RAs suppress SGLT2i-induced hy-perphagia. Last, the net effect on BPwas superadditive, suggesting synergy,which could be a favorable pleiotropiceffect.
SGLT2is AND DPP-4is
DPP-4isAlthough DPP-4is were developed toprevent the rapid degradation of nativeGLP-1, inhibition also leads to augmentedconcentrations of several other DPP-4substrates. As such, the glucose-loweringcapacities of this drug class are probablynot limited to the induced prolongedpostprandial rise in endogenous GLP-1 (Fig. 1) but also involve increasedconcentrations of other glucoregulatorysubstrates (59). DPP-4is are less potentthan GLP-1RAs and lower postprandialglucose by ;3.0 mmol/L, FPG by 1.0–1.5 mmol/L, and HbA1c by 0.77% from
a mean baseline of 8.05% (60,61). Thisis mainly achieved through increasedinsulin and suppressed glucagon secre-tion, which results in reduced HGP. Cur-rently, five DPP-4is are available inEurope and the U.S., namely sitagliptin,vildagliptin, saxagliptin, alogliptin, andlinagliptin.
The drug class alters cardiovascular-renal risk factors to a smaller extent thanGLP-1RAs. DPP-4is are considered weightneutral, lower SBP and DBP by ;3 and1mmHg, respectively (62), andmodestlyimprove total cholesterol and triglycer-ide concentrations (45). In comparisonwith GLP-1RAs, DPP-4is possess distinctglucose-independent anti-inflammatoryand antifibrotic properties, which couldbe mediated indirectly via DPP-4 sub-strates or directly, as DPP-4is affect T-celldevelopment, T-cell activation, and im-mune regulation (45).
The CVOTs of alogliptin (Examina-tion of Cardiovascular Outcomes withAlogliptin versus Standard of Care[EXAMINE]), saxagliptin (SaxagliptinAssessment of Vascular OutcomesRecorded in Patients with DiabetesMellitus–Thrombolysis in MyocardialInfarction 53 [SAVOR-TIMI 53]), andsitagliptin (Trial Evaluating Cardiovascu-lar Outcomes With Sitagliptin [TECOS])all demonstrated cardiovascular safety(Table 1) but indicated no trend to-ward benefit (63–65). Unexpectedly, inSAVOR-TIMI 53 and numerically butnonsignificantly in EXAMINE, DPP-4i usewas associated with an increase in HHFwithout an increase in mortality, whichprompted the FDA to issue a safetywarning for the whole drug class forthis potential complication. Plausiblemechanistic explanations are lacking,and given the absence of any harmfulsignals in TECOS, it seems unlikely thatthese results can be extrapolated toDPP-4is per se.
The effect of DPP-4is on renal diseasein T2D is inconclusive. Combined datafrom 13 placebo-controlled clinical trialsshowed reduced renal disease eventsby ;16% (66). In SAVOR-TIMI 53, sax-agliptin reduced the ACR by 34 mg/gbut did not affect hard renal outcome.In the Efficacy, Safety & Modification ofAlbuminuria in Type 2 Diabetes SubjectsWith Renal Disease With LINAgliptin(MARLINA-T2D) trial investigating 360patients with microalbuminuria despiteRAAS blockade, 24-week linagliptin did
not significantly change eGFR or loweralbuminuria (67). EXAMINE only reportedchange in eGFR from baseline, whichwas not altered by alogliptin, and TECOSreported slight reductions in eGFR(1.34 mL/min/1.73 m2) and ACR (0.18mg/g), of which the clinical implicationis unknown.
The adverse event profile of DPP-4isis mild, with placebo-like event rates.As mentioned earlier, the increased HHFhas resulted in an FDA safety warningon the labels of agents of this drug class.Although the incidence is low, usage isassociated with an increased risk ofpancreatitis (50,68).
Glycemic ControlIn phase 3 trials investigating combina-tion therapy versus either SGLT2is orDPP-4is alone, HbA1c was reduced by;1.2–1.5%, which was significantlymore than either agent alone (Fig. 3).A meta-analysis by Cho et al. (69) sum-marized the effects of 10 SGLT2i/DPP-4icombination studies, mostly on top ofmetformin. Combination therapy versusDPP-4is alone resulted in significantlygreater reductions (0.62%; 95% CI 0.51–0.73; P , 0.001), with slightly larger re-ductions when an SGLT2i was added toa DPP-4i (0.70%; 95% CI 0.54–0.85; P ,0.001) compared with initial combina-tion therapy (0.51%; 95% CI 0.37–0.65).Combination therapy compared withSGLT2is alone resulted in significantlyhigher reductions in HbA1c (0.32%;95% CI 0.22–0.48; P , 0.001). Initialcombination proved to be equally as ef-fective as add-on strategies. After strat-ification by baseline HbA1c levels, theadditional reduction by SGLT2is as esti-mated from combination therapy versusDPP-4is alone showed reductions pro-portional to baseline HbA1c. In contrast,combination therapy versus SGLT2isalone resulted in modest reductions re-gardless of baseline HbA1c. Interestingly,the authors thereafter suggest thatadditional glucose control is significantwhen SGLT2is are combined with oradded to DPP-4is but not vice versa,as was also suggested previously (30).The stimulation of HGP by SGLT2i-induced glycosuria might be so power-ful that it limits the glycemic efficacyof DPP-4is in this combination. Similarto combination with GLP-1RAs, the netglycemic efficacy is not synergistic butsubadditive as a result of interference.
care.diabetesjournals.org van Baar and Associates 1551

Pleiotropic EffectsUnlike combination therapy with GLP-1RAs, phase 3 combination trials versuseither agent alonewith SGLT2is andDPP-4is indicate that the additive BP and bodyweight reductions are not significantlydifferent in comparison with SGLT2ialone (Fig. 3). Cho et al. (69) demonstratethat this applies for both initial combi-nation and the add-on studies. More-over, post hoc data of CANVAS do notindicate significant differences in lipidprofiles of patients also treated withDPP-4is, suggesting that combined usedoes not relevantly affect lipid levels.Interestingly, DPP-4is are associatedwith increased urinary sodium excretion(70,71). Lovshin et al. (70) recently sug-gested, based on a mechanistic studyusing fractional lithium excretion, thatDPP-4is block sodium reabsorption dif-ferently than SGLT2is, at a location down-stream of the macula densa, thereby notaltering TGF and renal hemodynamicfunctions, which explains the mild-to-neutral effects on eGFR trajectoriesand albuminuria. Yet, DPP-4is could stillimprove renal function via GLP-1R–mediated effects or via other DPP-4 sub-strates associated with sodium excretionor anti-inflammatory effects such asSDF-1a, neuropeptide Y, PYY, substanceP, and BNP (45).
Outcomes in CVOTsThe cardiovascular outcomes of SGLT2iscombined with DPP-4is have not beeninvestigated. In the reported CVOTsthat examined DPP-4is, SGLT2is werenot used as background therapy. Viceversa, in EMPA-REG OUTCOME, DPP-4iuse was almost associated with worseoutcome in the subgroup analysis of theprimary outcome, but the small numbers(23 events in 198 patients) are not con-vincing (HR 1.27 [95% CI 0.82–1.98] vs.0.81 [95% CI 0.70–0.95]; P for interac-tion 0.06). The CANVAS Program did notreport such an analysis. Therefore, thecardiovascular-renal outcome of com-bined use is unknown; however, giventhat DPP-4is only modestly alter riskfactors and do not induce cardiovascu-lar-renal benefit, it is unlikely that theseagents will majorly improve SGLT2i-induced benefits.
Adverse EventsSGLT2is have potential adverse effectsthat could be ameliorated when combined
with DPP-4is. For instance, the rate ofgenital infections is lowered by 26%when used in this combination, whichhas been attributed to DPP-4i effects onthe immune system (72). Moreover, al-though speculative, the increased rateof HHF associated to saxagliptin may becounteracted by the cardioprotectiveeffects of SGLT2is. The risk of DKA maybe lower due to an enlarged insulin/glucagon ratio. Other adverse effectswill probably be independent and thusadditive.
Pathophysiological RationaleWhen considering the SGLT2i/DPP-4icombination, baseline HbA1c and drugsequence are important factors that de-termine glycemic efficacy. Although thecombination results in a clinically rele-vant reduction of HbA1c and FPG, additionof a DPP-4i to ongoing SGLT2i therapyreduces glycemic levels modestly, and itseems unlikely that DPP-4is can offsetSGLT2i-induced increments in gluca-gon levels andHGP.However, synergismmight still be possible on pleiotropictargets such as the preservation of renalfunction.
SGLT2is AND OTHER GLUCOSE-LOWERING AGENTS
SGLT2is and SulfonylureasSulfonylureas are frequently used assecond-line therapy due to their well-established efficacy and low costs. Bydepolarizing the b-cell membrane, sul-fonylureas stimulate insulin secretionand, according to a 2010 meta-analysis,thereby lower HbA1c by ;1.0–1.25%when used on top of metformin (73).Their effect on BP and lipids is neutral.Common adverse effects are hypoglyce-mia and weight gain (74). The durabilityof this drug class is weak, which is of-ten related to induced b-cell failure.Although sulfonylureas have been usedfor several decades, the cardiovascular-renal safety of sulfonylureas has notbeen studied properly. Two ongoing stud-ies, Cardiovascular and Renal Microvas-cular Outcome Study With Linagliptinin Patients With Type 2 Diabetes Melli-tus (CARMELINA) (NCT01897532) andCardiovascular Outcome Study of Lina-gliptin Versus Glimepiride in PatientsWith Type 2 Diabetes (CAROLINA)(NCT01243424), which are designed todemonstrate the cardiovascular safetyof linagliptin versus placebo and active
comparator glimepiride, respectively, couldvia an indirect comparison help to fi-nally narrow this long existing gap in ourknowledge.
The effect of combination therapyversus either agent alone has not beeninvestigated, and as a consequence,the quantitative effects are unclear.Phase 3 trials showed that addingSGLT2is to sulfonylurea therapy causesgreater glycemic efficacy than placebo(75,76). In combination, SGLT2is mightreduce the sulfonylurea-induced b-cellstress by lowering the b-cell afterload.Moreover, the addition of SGLT2is tosulfonylureas reduces body weight,lowers BP, and has no effect on lipids(77–79). In EMPA-REG OUTCOME,sulfonylurea usage in 2,014 patientsdid not alter the cardiovascular bene-fit of empagliflozin (HR 0.87; 95% CI0.69–1.11; P for interaction 0.83).
SGLT2is and ThiazolidinedionesThiazolidinediones, agonists of the per-oxisome proliferator–activated receptorg, improve insulin sensitivity by sensitiz-ing muscle, liver, and adipose tissue toinsulin and preserve b-cell function, col-lectively improving glycemic control (80).Since rosiglitazone is associated withsignificant increases in the risk of myo-cardial infarction (MI) (81), pioglitazoneis currently the most preferred agent. Inthe efficacy and tolerability trial of thePioglitazone 027 Study Group, pioglita-zone lowered HbA1c on top ofmetforminby 0.8% compared with placebo (meanbaseline 9.8–9.9%) (82). Pioglitazone in-duces weight gain due to adipogenesisbut lowers BP and improves lipid profiles(80). Pioglitazone has potentially harm-ful side effects, which include increasedfracture risk, edema, and HF (80,83).The underlying mechanism of edemaand HF could be fluid retention andplasma volume expansion, which resultfrom sodium reabsorption in the renalcollecting duct. In the PROspective pio-glitAzone Clinical Trial In macroVascularEvents (PROactive), pioglitazone signifi-cantly reduced the main secondary endpoint 3-point MACE (all-cause mortal-ity, nonfatal MI, stroke) but not theprimary extended MACE due to an in-crease in leg revascularization (84). Also,in subgroup analyses involving patientswith established MI (85) or stroke (86),reoccurrence of these events was signif-icantly reduced, indicating a benefit on
1552 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018

atherosclerotic outcome. This result wasconfirmed by the Insulin ResistanceIntervention After Stroke (IRIS) study(87), which demonstrated that in pa-tients who had insulin resistance alongwith a recent history of ischemic strokeor transient ischemic attack, pioglitazonesignificantly reduces the event rate offatal or nonfatal MI and stroke (HR 0.76;95% CI 0.62–0.93; P = 0.007). However,Thiazolidinediones or Sulfonylureas Car-diovascular Accidents Intervention Trial(TOSCA.IT) showed that the incidence ofcardiovascular events was similar whensulfonylureas (mostly glimepiride andgliclazide) were compared with pioglita-zone, without significant differences inrisk of HF. Probably due to the healthypopulation, the event rates in TOSCA.ITwere so low that the study was termi-nated early on the basis of a futilityanalysis. These results thus have tobe interpreted with caution. The effi-cacy and tolerability of empagliflozinadded to pioglitazone was assessed inthe EMPA-REG PIO studies (88,89). Atweek 24, empagliflozin reducedHbA1c by;0.7% compared with placebo from abaseline of 8.1–8.2% in 498 T2D patients.Body weight decreased by ;1.5 kg withempagliflozin, whereas placebo resultedin an increase of ;0.3 kg. Addition ofcanagliflozin to pioglitazone (90) or ad-dition to pioglitazone without metformin(91) resulted in similar effects. Overall,addition of SGLT2is to pioglitazone ontop of metformin reduces HbA1c and BPand ameliorates but does not halt weightgain and edema (31). The beneficial ef-fects of pioglitazone on atheroscleroticoutcomes stroke andMI could additivelyimprove cardiovascular outcome whencombined with SGLT2is. Since pioglita-zone has shown to improve hepatic fatcontent and liver histology (80), thecombination might be effective in thetreatment of NASH and NAFLD. Theoret-ically, the much-debated pioglitazone-associated adverse effects edema and HFcould be offset by SGLT2is. An additive orsynergistic effect on BP and weight gain,togetherwithSGLT2i-inducedplasmacon-traction, could result in cardioprotection,but this hypothesis needs further research.
SGLT2is and InsulinWhile increasing insulin dosages willcorrect any level of hyperglycemia, treat-ment intensification is hampered by in-creased weight gain and hypoglycemia
risk. Weight gain results in the needfor higher insulin dosages and, as such,creates a vicious circle. Therefore, clinicalpractice strategies pursue lower insulindosages by adding other glucose-loweringagents that increase insulin sensitivityor lower insulin need. In a meta-analysisof seven phase 3 studies in 4,235 in-sulin-treated patients (including basaland basal-bolus regimens), addition ofan SGLT2i caused HbA1c reductions of0.56%, reduced FPG by 0.95 mmol/L, andinduced weight loss of 2.63 kg, andinsulin dose was decreased by 8.79IU from mean of ;65 IU comparedwith placebo (92). Additionally, theSGLT2i-induced reductions in BP aremaintained on an insulin background(93–95). In EMPA-REG OUTCOME, SGLT2ismaintained their cardiovascular ben-efit in patients who were on insulin(2,252 patients, HR 0.93; 95% CI 0.75–1.13; P for interaction 0.28). In the meta-analysis mentioned earlier, an increasedrisk of drug-related adverse events of36% was observed, and urinary tract in-fections and genital infections increasedby 29% and 357%, respectively (92). Last,the propensity of SGLT2is to cause DKAcan be amplified when SGLT2i causes areduction in the dose of concomitant in-sulin therapy.
CONCLUSIONS
Clinical ConsiderationsWhen balancing risks and benefits ofglycemic control and pursuing cardiovas-cular risk reduction, a patient-centeredapproach requires numerous considera-tions, including glycemic efficacy, hypo-glycemia risk, history of cardiovasculardisease (CVD), weight control, adverseeffects, renal effects, delivery method,costs, and patient preferences. The dif-ferences in the current (inter)nationalguidelines illustrate the challenge of sucha holistic approach. The ADA’s Standardsof Medical Care in Diabetesd2018 (1)offers a free choice from the six discusseddrug classes recommended after initiationof metformin, and we support the re-cently added recommendation that T2Dpatients with established CVD shouldbe treated with an agent that reducescardiovascular events and/or mortality.Considering the CVOTs (Table 1), weadvocate the use of GLP-1RAs in patientswith CVD of atherosclerotic origin andSGLT2is in patients with diabetes-related
HF and/or CKD. Although the freedom ofchoice provides opportunities for thoroughpatient- and disease-based individual-ization, it assumes a comprehensiveknowledge of the T2D treatment arma-mentarium (Fig. 1), in particular whencombination therapy is indicated (Table2). The National Institute for Healthand Care Excellence guideline (2) fo-cuses on the use of DPP-4is, pioglita-zone, and sulfonylureas. The use ofSGLT2is is restricted to patients witha significant hypoglycemia risk or tothose in which metformin and sulfonyl-ureas are contraindicated or not toler-ated. Triple therapy with SGLT2is isnot the first recommendation and is ad-vised on top of metformin with pioglita-zone or sulfonylurea. GLP-1RAs can beconsidered as triple therapy in severelyoverweight patients and/or to reduceobesity-associated comorbidities butare not mentioned in combination withSGLT2is. Although this guideline takeshypoglycemia risk into account, it seemsto favor cost-effectiveness over car-diovascular benefit, weight control, andsafety-to-efficacy profile. The currentAmerican Association of Clinical Endo-crinologists and American College of En-docrinology algorithm (3) recommendsa hierarchy of use for all FDA-approvedagents in mono-, dual, and triple ther-apy. On top ofmetformin, the suggestedorder is GLP-1RAs, SGLT2is, DPP-4is,thiazolidinediones, basal insulin, cole-sevelam, bromocriptine, a-glucosidaseinhibitors, and sulfonylureas/glinides.In triple therapy, this order remains,except for DPP-4is, which drop downbelow basal insulin. The hierarchy pro-vides support, but the fixed character isreminiscentofaone-size-fits-all approach.It is clear that guidelines face an insolubledilemma to either offer support in a morestepwise or simplified approach that im-pedes individualization or offer freedomof choice in a holistic patient-centeredapproach, leaving health care providerswithout direction or endorsement.
The five possible combinations withSGLT2is on top of metformin discussedin this perspective all showed greaternet glycemic efficacy than either agentalone and resulted in clinically meaning-ful reductions of HbA1c. Yet, none of themdemonstrated (super)additive glycemicefficacy, which could be explained by theobservation that the glycemic efficacyof all drug classes depends on baseline
care.diabetesjournals.org van Baar and Associates 1553

hyperglycemia, causing interference (Fig.2) (56). Nonetheless, even combinationswith GLP-1RAs or DPP-4is were sub-additive (Fig. 3), which suggests thatthe potent glycosuria-driven action ofSGLT2is on glucagon and HGP cannotsufficiently be counteracted by the in-cretin therapies to evoke synergism. Theglycemic rationale for a specific drugcombination for an individual patientthus lies in the prevailing pathophysi-ological defects rather than a demon-strated superior net glycemic efficacyof one combination over the other.In contrast, the combined net pleio-
tropic effects are various. From anSGLT2i-centered point of view, a combi-nation with GLP-1RAs seems most at-tractive, showing additive effects inbody weight and even synergism in SBPreduction (Fig. 3). Moreover, this com-bination couples the two drug classesthat demonstrated cardiovascular-renalbenefit. Although these benefits haveenthused many and revised T2D man-agement, several questions remain. First,what mechanisms underlie the benefits?Second, are these benefits class effects?Third, are these benefits generalizableto all T2D patients? Fourth, what is thebenefit of one drug class over the other?Ultimately, will these benefits remain incombination therapy?
Future PerspectiveAt present, we do not know the answersto these questions. The increasing num-ber of mechanistic trials and futureCVOTs that investigate cardiovascularand/or renal effects will possibly ans-wer the first two questions but willnot demonstrate generalizability or head-to-head risks and benefits. Unfortu-nately, it is unlikely that these questionswill ever be answered by dedicated ran-domized clinical trials due to the costsand feasibility of such trials, let alone forcombination therapy. Therefore, in orderto maximize the effect of a patient-centered approach and exploit the ben-efits of combination therapy, we call forthe use of well-designed observationalstudies in the real-life setting to clarifythe individual benefits of one agent andone combination over the other.
Duality of Interest. M.H.A.M. consulted for EliLilly & Co. R.G.IJ. is the principal investigatorof studies sponsored by research grants from
AstraZeneca, Eli Lilly & Co., and Novo Nordisk.D.H.v.R. serves on advisory boards of Sanofi andMerck Sharp & Dohme. R.G.IJ. and D.H.v.R.report receiving no personal payments in con-nection to the above-mentioned activities;all payments were directly transferred to theVU University Medical Center/Diabetes Centernonprofit research foundation. The authors havewritten the entire article themselves, withoutany sponsorship or funding of a pharmaceuticalcompany. No other potential conflicts of inter-est relevant to this article were reported.
References1. American Diabetes Association. 8. Pharma-cologic approaches to glycemic treatment:Standards of Medical Care in Diabetesd2018.Diabetes Care 2018;41(Suppl. 1):S73–S852. National Institute for Health and Care Excel-lence. Type 2 diabetes in adults: management.NICE guideline (NG28), December 2015. Avail-able from https://www.nice.org.uk/guidance/ng28. Accessed 17 March 20183. Garber AJ, Abrahamson MJ, Barzilay JI, et al.Consensus statement by the American Associa-tion of Clinical Endocrinologists and AmericanCollege of Endocrinology on the comprehensivetype 2 diabetes management algorithm - 2017executive summary. Endocr Pract 2017;23:207–2384. Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of hyperglycaemia in type 2 diabe-tes, 2015: a patient-centred approach. Updateto a position statement of the American Diabe-tes Association and the European Association forthe Study of Diabetes. Diabetologia 2015;58:429–4425. DeFronzo RA. Banting Lecture. From the tri-umvirate to the ominous octet: a new paradigmfor the treatment of type 2 diabetes mellitus.Diabetes 2009;58:773–7956. Kahn SE, Cooper ME, Del Prato S. Pathophys-iology and treatment of type 2 diabetes: per-spectives on the past, present, and future. Lancet2014;383:1068–10837. Holst JJ, Vilsbøll T, Deacon CF. The incretinsystem and its role in type 2 diabetes mellitus.Mol Cell Endocrinol 2009;297:127–1368. Nauck MA, Meier JJ. The incretin effect inhealthy individuals and those with type 2diabetes: physiology, pathophysiology, and re-sponse to therapeutic interventions. LancetDiabetes Endocrinol 2016;4:525–5369. van Bloemendaal L, Ten Kulve JS, la Fleur SE,Ijzerman RG, DiamantM. Effects of glucagon-likepeptide 1 on appetite and body weight: focus onthe CNS. J Endocrinol 2014;221:T1–T1610. Vasilakou D, Karagiannis T, Athanasiadou E,et al. Sodium-glucose cotransporter 2 inhibitorsfor type 2 diabetes: a systematic review andmeta-analysis. Ann Intern Med 2013;159:262–27411. van Bommel EJ, Muskiet MH, Tonneijck L,KramerMH,NieuwdorpM, van RaalteDH. SGLT2inhibition in the diabetic kidney-from mecha-nisms to clinical outcome. Clin J Am Soc Nephrol2017;12:700–71012. Sha S, Polidori D, Heise T, et al. Effect of thesodium glucose co-transporter 2 inhibitor can-agliflozin on plasma volume in patients withtype 2 diabetes mellitus. Diabetes Obes Metab2014;16:1087–1095
13. FerranniniG,HachT,CroweS, SanghviA,HallKD, Ferrannini E. Energy balance after sodium–glucose cotransporter 2 inhibition. DiabetesCare 2015;38:1730–173514. Ferrannini E, Muscelli E, Frascerra S, et al.Metabolic response to sodium-glucose cotrans-porter 2 inhibition in type 2 diabetic patients. JClin Invest 2014;124:499–50815. Baker WL, Buckley LF, Kelly MS, et al. Effectsof sodium-glucose cotransporter 2 inhibitors on24-hour ambulatory blood pressure: a systema-tic review and meta-analysis. J Am Heart Assoc2017;6:e00568616. Muskiet MHA, van Bommel EJM, van RaalteDH. Antihypertensive effects of SGLT2 inhibitorsin type 2 diabetes. Lancet Diabetes Endocrinol2016;4:188–18917. Sumida Y, Yoneda M. Current and futurepharmacological therapies for NAFLD/NASH. JGastroenterol 2018;53:362–37618. Heerspink HJ, Perkins BA, Fitchett DH,Husain M, Cherney DZ. Sodium glucose cotrans-porter 2 inhibitors in the treatment of diabetesmellitus: cardiovascular and kidney effects, po-tential mechanisms, and clinical applications.Circulation 2016;134:752–77219. Lytvyn Y, Bjornstad P, Udell JA, Lovshin JA,Cherney DZI. Sodium glucose cotransporter-2inhibition in heart failure: potential mechanisms,clinical applications, and summary of clinicaltrials. Circulation 2017;136:1643–165820. Cherney DZ, Perkins BA, Soleymanlou N,et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patientswith type 1 diabetes mellitus. Circulation 2014;129:587–59721. Dekkers CCJ, Wheeler DC, Sjostrom CD,Stefansson BV, Cain V, Heerspink HJL. Effectsof the sodium-glucose co-transporter 2 inhibitordapagliflozin in patients with type 2 diabetesand Stages 3b–4 chronic kidney disease. NephrolDial Transplant. 23 January 2018 [Epub aheadof print]. DOI: 10.1093/ndt/gfx35022. Neal B, Perkovic V, Mahaffey KW, et al.Canagliflozin and cardiovascular and renal eventsin type 2 diabetes. N Engl J Med 2017;377:644–65723. ZinmanB,WannerC, Lachin JM,et al.; EMPA-REG OUTCOME Investigators. Empagliflozin, car-diovascular outcomes, and mortality in type2 diabetes. N Engl J Med 2015;373:2117–212824. Wanner C, Inzucchi SE, Lachin JM, et al.;EMPA-REG OUTCOME Investigators. Empagliflo-zin and progression of kidney disease in type 2diabetes. N Engl J Med 2016;375:323–33425. Inzucchi SE, Zinman B, Fitchett D, et al. Howdoes empagliflozin reduce cardiovascular mor-tality? Insights from a mediation analysis of theEMPA-REG OUTCOME trial. Diabetes Care 2018;41:356–36326. Ferrannini E, Mark M, Mayoux E. CV Pro-tection in the EMPA-REG OUTCOME trial: a“thrifty substrate” hypothesis. Diabetes Care2016;39:1108–111427. Uthman L, Baartscheer A, Bleijlevens B, et al.Class effects of SGLT2 inhibitors in mouse car-diomyocytes and hearts: inhibition of Na+/H+
exchanger, lowering of cytosolic Na+ and vaso-dilation. Diabetologia 2018;61:722–72628. Rosenstock J, Ferrannini E. Euglycemic di-abetic ketoacidosis: a predictable, detectable,
1554 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018

and preventable safety concern with SGLT2inhibitors. Diabetes Care 2015;38:1638–164229. DeFronzo RA. Combination therapy withGLP-1 receptor agonist and SGLT2 inhibitor.Diabetes Obes Metab 2017;19:1353–136230. Scheen AJ. DPP-4 inhibitor plus SGLT-2 in-hibitor as combination therapy for type 2 di-abetes: from rationale to clinical aspects. ExpertOpin Drug Metab Toxicol 2016;12:1407–141731. DeFronzo RA, Chilton R, Norton L, Clarke G,Ryder RE, Abdul-Ghani M. Revitalization of pio-glitazone: the optimum agent to be combinedwith a sodium-glucose co-transporter-2 inhibi-tor. Diabetes Obes Metab 2016;18:454–46232. Shyangdan DS, Royle P, Clar C, Sharma P,Waugh N, Snaith A. Glucagon-like peptide ana-logues for type 2 diabetes mellitus. CochraneDatabase Syst Rev 2011;Oct 5:CD00642333. Nauck MA, Kemmeries G, Holst JJ, Meier JJ.Rapid tachyphylaxis of the glucagon-like peptide1-induced deceleration of gastric emptying inhumans. Diabetes 2011;60:1561–156534. Sun F, Chai S, Li L, et al. Effects of glucagon-like peptide-1 receptor agonists on weight lossin patients with type 2 diabetes: a systematicreview and network meta-analysis. J DiabetesRes 2015;2015:157201.35. Sun F, Wu S, Guo S, et al. Impact of GLP-1receptor agonists on blood pressure, heart rateand hypertension among patients with type 2diabetes: a systematic review and network meta-analysis. Diabetes Res Clin Pract 2015;110:26–3736. Sun F,WuS,Wang J, et al. Effect of glucagon-like peptide-1 receptor agonists on lipid profilesamong type 2 diabetes: a systematic review andnetworkmeta-analysis.ClinTher2015;37:225-241.e837. Nauck MA, Meier JJ, Cavender MA, Abd ElAziz M, Drucker DJ. Cardiovascular actions andclinical outcomes with glucagon-like peptide-1receptor agonists and dipeptidyl peptidase-4inhibitors. Circulation 2017;136:849–87038. Dutour A, Abdesselam I, Ancel P, et al. Ex-enatide decreases liver fat content and epicardialadipose tissue in patients with obesity and type 2diabetes: a prospective randomized clinical trialusing magnetic resonance imaging and spectros-copy. Diabetes Obes Metab 2016;18:882–89139. Smits MM, van Raalte DH, Tonneijck L,MuskietMH, KramerMH, CahenDL. GLP-1 basedtherapies: clinical implications for gastroenter-ologists. Gut 2016;65:702–71140. Armstrong MJ, Gaunt P, Aithal GP, et al.;LEAN trial team. Liraglutide safety and efficacyin patients with non-alcoholic steatohepatitis(LEAN):amulticentre, double-blind, randomised,placebo-controlled phase 2 study. Lancet 2016;387:679–69041. Pfeffer MA, Claggett B, Diaz R, et al.; ELIXAInvestigators. Lixisenatide in patients with type2 diabetes and acute coronary syndrome. N EnglJ Med 2015;373:2247–225742. Marso SP, Daniels GH, Brown-Frandsen K,et al.; LEADER Steering Committee; LEADER TrialInvestigators. Liraglutide and cardiovascularoutcomes in type 2 diabetes. N Engl J Med 2016;375:311–32243. Marso SP, Bain SC, Consoli A, et al.; SUSTAIN-6 Investigators. Semaglutide and cardiovascu-lar outcomes in patients with type 2 diabetes.N Engl J Med 2016;375:1834–184444. Holman RR, Bethel MA, Mentz RJ, et al.;EXSCEL Study Group. Effects of once-weekly
exenatide on cardiovascular outcomes in type2 diabetes. N Engl J Med 2017;377:1228–123945. Muskiet MHA, Tonneijck L, Smits MM, et al.GLP-1 and the kidney: from physiology to phar-macology and outcomes in diabetes. Nat RevNephrol 2017;13:605–62846. Mann JFE, Ørsted DD, Buse JB. Liraglutideand renal outcomes in type 2 diabetes. N Engl JMed 2017;377:2197–219847. Tuttle KR, Lakshmanan MC, Gross JL, et al.Comparable glycaemic control with once weeklydulaglutide versus insulin glargine, both com-bined with lispro, in type 2 diabetes and chronickidney disease (AWARD-7) (Abstract). Diabeto-logia 2017;60:S348. Tonneijck L, Muskiet MH, Smits MM, et al.Glomerular hyperfiltration in diabetes: mecha-nisms, clinical significance, and treatment. J AmSoc Nephrol 2017;28:1023–103949. Meier JJ. GLP-1 receptor agonists for in-dividualized treatment of type 2 diabetes melli-tus. Nat Rev Endocrinol 2012;8:728–74250. Egan AG, Blind E, Dunder K, et al. Pancreaticsafety of incretin-based drugs–FDA and EMAassessment. N Engl J Med 2014;370:794–79751. StorgaardH,Cold F,GluudLL,Vilsbøll T, KnopFK. Glucagon-like peptide-1 receptor agonistsand risk of acute pancreatitis in patients withtype 2 diabetes. Diabetes Obes Metab 2017;19:906–90852. Bethel MA, Patel RA, Merrill P, et al. Car-diovascular outcomes with glucagon-like pep-tide-1 receptor agonists in patients with type 2diabetes: a meta-analysis. Lancet Diabetes En-docrinol 2017;6:105–11353. Frıas JP, Guja C, Hardy E, et al. Exenatide onceweekly plus dapagliflozin once daily versus ex-enatide or dapagliflozin alone in patients withtype 2 diabetes inadequately controlled withmetformin monotherapy (DURATION-8): a 28week, multicentre, double-blind, phase 3, rand-omised controlled trial. Lancet Diabetes End-ocrinol 2016;4:1004–101654. Ludvik B, Frıas JP, Tinahones FJ, et al. Du-laglutide as add-on therapy to SGLT2 inhibitorsin patients with inadequately controlled type 2diabetes (AWARD-10): a 24-week, randomised,double-blind, placebo-controlled trial. Lancet Di-abetes Endocrinol 2018;6:370–38155. Fulcher G, Matthews DR, Perkovic V, et al.;CANVAS trial collaborative group. Efficacy andsafety of canagliflozin when used in conjunctionwith incretin-mimetic therapy in patients withtype 2 diabetes. Diabetes Obes Metab 2016;18:82–9156. Polidori D, Capuano G, Qiu R. Apparentsubadditivity of the efficacy of initial combina-tion treatments for type 2 diabetes is largelyexplained by the impact of baseline HbA1c onefficacy. Diabetes ObesMetab 2016;18:348–35457. Carbone LJ, Angus PW, YeomansND. Incretin-based therapies for the treatment of non-alcoholic fatty liver disease: a systematic reviewand meta-analysis. J Gastroenterol Hepatol 2016;31:23–3158. DeFronzoRA,MartinezR,Al-JaboriH, AdamsJ, Triplitt C, Cersosimo E. Liraglutide fails to off-set the rise in hepatic glucose production (HGP)seen with SGLT2i treatment (Abstract). Diabetes2017;66(Suppl. 1):A28359. Andersen ES, Deacon CF, Holst JJ. Do weknowthe truemechanismof actionof theDPP-4
inhibitors? Diabetes Obes Metab 2018;20:34–4160. Esposito K, Chiodini P, Maiorino MI, et al. Anomogram to estimate the HbA1c responseto different DPP-4 inhibitors in type 2 diabetes:a systematic review and meta-analysis of 98trials with 24 163 patients. BMJ Open 2015;5:e00589261. Tahrani AA, Barnett AH, Bailey CJ. Pharma-cology and therapeutic implications of currentdrugs for type 2 diabetes mellitus. Nat RevEndocrinol 2016;12:566–59262. Zhang X, Zhao Q. Effects of dipeptidyl pep-tidase-4 inhibitors on blood pressure in patientswith type 2 diabetes: a systematic review andmeta-analysis. J Hypertens 2016;34:167–17563. White WB, Cannon CP, Heller SR, et al.;EXAMINE Investigators. Alogliptin after acutecoronary syndrome in patients with type 2diabetes. N Engl J Med 2013;369:1327–133564. Green JB, Bethel MA, Armstrong PW, et al.;TECOS Study Group. Effect of sitagliptin oncardiovascular outcomes in type 2 diabetes. NEngl J Med 2015;373:232–24265. Scirica BM, Bhatt DL, Braunwald E, et al.;SAVOR-TIMI 53 Steering Committee and In-vestigators. Saxagliptin and cardiovascularoutcomes in patients with type 2 diabetesmellitus. N Engl J Med 2013;369:1317–132666. Cooper ME, Perkovic V, McGill JB, et al.Kidney disease end points in a pooled analysisof individual patient-level data from a largeclinical trials program of the dipeptidyl pepti-dase 4 inhibitor linagliptin in type 2 diabetes.Am J Kidney Dis 2015;66:441–44967. Groop PH, Cooper ME, Perkovic V, et al.Linagliptin and its effects on hyperglycaemiaand albuminuria in patients with type 2diabetes and renal dysfunction: the randomizedMARLINA-T2D trial. Diabetes Obes Metab2017;19:1610–161968. Meier JJ. GLP-1 receptor agonists for in-dividualized treatment of type 2 diabetes melli-tus. Nat Rev Endocrinol 2012;8:728–74269. Cho YK, Kang YM, Lee SE, et al. Efficacy andsafety of combination therapy with SGLT2 andDPP4 inhibitors in the treatment of type 2 di-abetes: a systematic review and meta-analysis.Diabetes Metab. 3 February 2018 [Epub aheadof print]. DOI: 10.1016/j.diabet.2018.01.01170. Lovshin JA, Rajasekeran H, Lytvyn Y, et al.Dipeptidyl peptidase 4 inhibition stimulates dis-tal tubular natriuresis and increases in circulat-ing SDF-1a1-67 in patients with type 2 diabetes[published corrections appears in Diabetes Care2017;40:1420–1421]. Diabetes Care 2017;40:1073–108171. Tonneijck L, Smits MM, Muskiet MH, et al.Renal effects of DPP-4 inhibitor sitagliptin orGLP-1 receptor agonist liraglutide in overweightpatients with type 2 diabetes: a 12-week,randomized, double-blind, placebo-controlledtrial. Diabetes Care 2016;39:2042–205072. Fadini GP, Bonora BM, Mayur S, Rigato M,Avogaro A. Dipeptidyl peptidase-4 inhibitorsmoderate the risk of genitourinary tract infec-tions associated with sodium-glucose co-transporter-2 inhibitors. Diabetes Obes Metab2018;20:740–74473. Sherifali D, Nerenberg K, Pullenayegum E,Cheng JE, Gerstein HC. The effect of oral anti-diabetic agents on A1C levels: a systematic
care.diabetesjournals.org van Baar and Associates 1555

review and meta-analysis. Diabetes Care 2010;33:1859–186474. Zhang F, Xiang H, Fan Y, et al. The effects ofsulfonylureas plus metformin on lipids, bloodpressure, and adverse events in type 2 diabetes:a meta-analysis of randomized controlled trials.Endocrine 2013;44:648–65875. Strojek K, Yoon KH, Hruba V, Elze M,Langkilde AM, Parikh S. Effect of dapagliflozinin patients with type 2 diabetes who have in-adequate glycaemic control with glimepiride:a randomized, 24-week, double-blind, placebo-controlled trial. Diabetes Obes Metab 2011;13:928–93876. Fulcher G, Matthews DR, Perkovic V, et al.Efficacy and safety of canagliflozin used in con-junction with sulfonylurea in patients with type2 diabetes mellitus: a randomized, controlledtrial. Diabetes Ther 2015;6:289–30277. Haring HU, Merker L, Seewaldt-Becker E,et al.; EMPA-REG METSU Trial Investigators.Empagliflozin as add-on to metformin plus sul-fonylurea in patients with type 2 diabetes:a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care 2013;36:3396–340478. Wilding JP, Charpentier G, Hollander P, et al.Efficacy and safety of canagliflozin in patientswithtype 2 diabetes mellitus inadequately controlledwithmetformin and sulphonylurea: a randomisedtrial. Int J Clin Pract 2013;67:1267–128279. Matthaei S, Bowering K, Rohwedder K, GrohlA, Parikh S, Study G; Study 05 Group. Dapagli-flozin improves glycemic control and reducesbody weight as add-on therapy to metformin plussulfonylurea:a24-weekrandomized,double-blindclinical trial. Diabetes Care 2015;38:365–37280. Yki-Jarvinen H. Thiazolidinediones. N Engl JMed 2004;351:1106–111881. Nissen SE, Wolski K. Rosiglitazone revisited:an updated meta-analysis of risk for myocardialinfarction and cardiovascular mortality. ArchIntern Med 2010;170:1191–120182. Einhorn D, Rendell M, Rosenzweig J, EganJW, Mathisen AL, Schneider RL. Pioglitazonehydrochloride in combination with metforminin the treatment of type 2 diabetes mellitus:a randomized, placebo-controlled study. The Pio-glitazone 027 Study Group. Clin Ther 2000;22:1395–140983. Wilcox R, Kupfer S, Erdmann E; PROactiveStudy investigators. Effects of pioglitazone on
major adverse cardiovascular events in high-risk patients with type 2 diabetes: results fromPROspective pioglitAzone Clinical Trial In macroVascular Events (PROactive 10). Am Heart J 2008;155:712–71784. Dormandy JA, Charbonnel B, Eckland DJ, et al.;PROactive Investigators. Secondary preventionof macrovascular events in patients with type 2diabetes in the PROactive Study (PROspectivepioglitAzone Clinical Trial In macroVascularEvents): a randomised controlled trial. Lancet2005;366:1279–128985. Erdmann E, Dormandy JA, Charbonnel B,Massi-Benedetti M, Moules IK, Skene AM; PRO-active Investigators. The effect of pioglitazoneon recurrent myocardial infarction in 2,445patients with type 2 diabetes and previousmyocardial infarction: results from the PRO-active (PROactive 05) Study. J Am Coll Cardiol2007;49:1772–178086. Wilcox R, Bousser MG, Betteridge DJ, et al.;PROactive Investigators. Effects of pioglitazonein patients with type 2 diabetes with or with-out previous stroke: results from PROactive(PROspective pioglitAzone Clinical Trial In macro-Vascular Events 04). Stroke 2007;38:865–87387. Kernan W, Viscoli C, Furie K, et al. Pioglita-zone after ischemic stroke or transient ischemicattack. N Engl J Med 2016;374:1321–133188. Kovacs CS, Seshiah V, Swallow R, et al.;EMPA-REG PIO� trial investigators. Empagli-flozin improves glycaemic and weight controlas add-on therapy to pioglitazone or pioglita-zone plus metformin in patients with type 2diabetes: a 24-week, randomized, placebo-controlled trial. Diabetes Obes Metab 2014;16:147–15889. Kovacs CS, Seshiah V,Merker L, et al.; EMPA-REG EXTENDTM PIO investigators. Empagliflozinas add-on therapy to pioglitazone with or with-out metformin in patients with type 2 diabetesmellitus. Clin Ther 2015;37:1773–1788.e190. Forst T, Guthrie R, Goldenberg R, et al.Efficacy and safety of canagliflozin over 52 weeksin patients with type 2 diabetes on backgroundmetformin and pioglitazone. Diabetes ObesMetab 2014;16:467–47791. Rosenstock J, VicoM,Wei L, Salsali A, List JF.Effects of dapagliflozin, an SGLT2 inhibitor, onHbA(1c), body weight, and hypoglycemia riskin patients with type 2 diabetes inadequately
controlled on pioglitazone monotherapy. Dia-betes Care 2012;35:1473–147892. Tang H, Cui W, Li D, et al. Sodium-glucoseco-transporter 2 inhibitors in addition to insu-lin therapy for management of type 2 diabe-tes mellitus: a meta-analysis of randomizedcontrolled trials. Diabetes Obes Metab 2017;19:142–14793. Rosenstock J, Jelaska A, Frappin G, et al.;EMPA-REG MDI Trial Investigators. Improvedglucose control with weight loss, lower insulindoses, and no increased hypoglycemia withempagliflozin added to titrated multiple dailyinjections of insulin in obese inadequately con-trolled type 2 diabetes. Diabetes Care 2014;37:1815–182394. Neal B, Perkovic V, de Zeeuw D, et al.;CANVAS Trial Collaborative Group. Efficacy andsafety of canagliflozin, an inhibitor of sodium-glucose cotransporter 2, when used in conjunctionwith insulin therapy in patients with type 2 di-abetes. Diabetes Care 2015;38:403–41195. Wilding JP, Norwood P, T’joen C, Bastien A,List JF, Fiedorek FT. A study of dapagliflozin inpatients with type 2 diabetes receiving highdoses of insulin plus insulin sensitizers: applica-bility of a novel insulin-independent treatment.Diabetes Care 2009;32:1656–166296. DeFronzo RA, Lewin A, Patel S, et al. Com-bination of empagliflozin and linagliptin as sec-ond-line therapy in subjects with type 2 diabetesinadequately controlled on metformin. DiabetesCare 2015;38:384–39397. Pratley RE, Eldor R, Raji A, et al. Ertugliflozinplus sitagliptin versus either individual agent over52 weeks in patients with type 2 diabetes melli-tus inadequately controlled with metformin:the VERTIS FACTORIAL randomized trial. Dia-betes Obes Metab 2018;20:1111–112098. Rosenstock J, Hansen L, Zee P, et al. Dualadd-on therapy in type 2 diabetes poorly con-trolled with metformin monotherapy: a ran-domized double-blind trial of saxagliptin plusdapagliflozin addition versus single addition ofsaxagliptin or dapagliflozin to metformin. Dia-betes Care 2015;38:376–38399. Cefalu WT, Kaul S, Gerstein HC, et al. Car-diovascular outcomes trials in type 2 diabetes:where do we go from here? Reflections from aDiabetes Care Editors’ Expert Forum. DiabetesCare 2018;41:14–31
1556 SGLT2is in Combination Therapy in T2D Diabetes Care Volume 41, August 2018





























