Embed Size (px)
DESCRIPTION
Obstacles to Adding Measures to EHRs and Ways to Overcome these for the Patient, Provider, System, and Society: General Principles and Real-World Experience Presented to the IOM Committee on Recommended Social and Behavioral Domains and Measures for Electronic Health Records April 8, 2014. - PowerPoint PPT Presentation
Citation preview

Obstacles to Adding Measures to EHRs and Ways to Overcome these for the Patient, Provider, System, and Society: General Principles and Real-World ExperiencePresented to the IOM Committee on Recommended
Social and Behavioral Domains and Measures for Electronic Health Records
April 8, 2014
Shaun J. Grannis, MD MS FAAFP FACMIThe Regenstrief Institute
Indiana University School of Medicine

Adding EHR data and functionality is costly
• Potential for increased data gathering burden– Additional time– Altered workflow
• Necessary Design/Development costs– Systems must be re-configured to accommodate
new data/functionality• Who absorbs these costs?

“Why, What, How, and By Whom”• Why:
– Well-articulated Problem/Need/Goal ... to which additional information/functionality are a clear solution
• What:– Identify information needed to accomplish the goal
• How:– Define process. Re-use existing resources before
asking for more: Identify and leverage potential pre-existing measures that address the need.

“Why, What, How, and By Whom”• Who:
– Contemplate who may be optimally positioned to gather/supply new information• Physician• Nurse• Registration Clerk• Patient• Other?

Examples

Rwanda: Maternal Child Health


Clinic
Community
Hospital
?

Clinic
Community
Hospital

Define Metrics to Assess Progress Toward Goal

Integrating Community level and Geospatial data

“Why”: Integrating Community level geospatial data
• Socio-behavioral factors are important, often unrecognized determinants of health outcomes
• US healthcare system is oriented to acute, hospital based, disease treatment.
• Responding to the health needs of both non-hospitalized and hospitalized patients with chronic diseases is proving difficult.
• Improving population level health problems like healthcare disparities is also challenging, in part because of the complex interplay of socio-behavioral, community and biologic factors within the context of the current healthcare system.
• Just as IT enabled advances in sub-molecular medicine, behavioral and population sciences are on the verge of an IT based revolution.

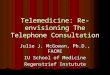
Patient Address Change
ADT Processor
Update person_address table with new address information
person_address table
Address Update Detector
In real-time, Address Update Detector detects and writes address changes to the post_processing table
post_processing table
Geo-Coding Application
Geo-Coding app reads the post_processing table
5
Call Polis Center web service which returns geo-coded addresses
Polis Web Service
3
4
6
1
2
Frederickson K, Grannis SJ, Dixon B, Bodenhamer DJ, Wiehe S. Incorporating geospatial capacity within clinical data systems to address social determinants of health. Public Health Reports. 2011 126. Suppl 3: 54.

Population-Level Analytics: Surveillance, Patient trends,
Predictive Modeling

GI Event

Hospital
Interface
Engine(Routing)
Information Flow: Clinical
Network ConnectionHL7 ADT
message
Hospital ED
Registration
Hospital Firewall(Encryption)
Firewall(Decryption)
Message Listene
rMessage Processor
Imported into
Clinical Reposito
ryClinical Repositor
y

Hospital
Interface
Engine(Routing)
Information Flow: PH Surveillance
Network ConnectionHL7 ADT
message
Hospital ED
Registration
Hospital Firewall(Encryption)
Firewall(Decryption)
Message Listene
rMessage Processor
Batched, delivered to ISDH
every 3 hours
Public Health

Multi-stream Surveillance

Flu CC
Pneumonia ICD9
Pneumonia CC
ILI ICD9
ILI CC
All Flu Tests
Positive Flu Tests
Positive Rate
Flu ICD9
H1N
1, A
pril
2009
H1N
1,O
ct
2009

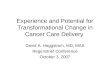
Population Trends

A network diagram illustrating the connectedness among Indiana EDs that participate in PHESS. Circular nodes represent EDs; node size indicates the visit volume; node color indicates the centrality of the ED. The gray edges connecting nodes indicate where patient crossover occurs. EDs that share proportionally larger number of patients are clustered together. While general clusters of "medical trading areas" emerge, the myriad gray edges clearly illustrate how interconnected all EDs are to one another.

84% PPV for predicting which patients who will use ED > 16 times in two years.
Wu J, Xu H, Finnell JT, Grannis SJ. A Practical Method for Predicting Frequent Use of Emergency Department Care Using Routinely Available Electronic Registration Data. AMIA Annu Symp Proc. 2013:1524.
Predicting Frequent ED Users

Thank You!