Embed Size (px)
Citation preview
SHOCK & RESUSITASI CAIRAN
DEFINITION
• Shock is a multifactorial syndrome leading to systemic and localized tissue hypoperfusion and resulting in cellular hypoxia and multiple organ dysfunction
DESCRIPTION
• Perfusion may be decreased systemacally with obvious signs such as hypotension
• Perfusion may be decreased because of maldistribution as in septic shock where systemic perfusion may appear elevated
DESCRIPTION
Prognosis is determined by• degree of shock, • duration of shock, • number of organ affected,• previous organ dysfunction and• possibly some genetic predispositition
CLASSIFICATION OF SHOCK
1. Hypovolemic shock2. Obstructive shock3. Cardiogenic shock4. Distributive shock
HYPOVOLEMIC SHOCK
• Loss of circulating intravascular volume and decrease in cardiac preload
• May be from hemorrhage : trauma, gastrointestinal bleeding, nontraumatic internal bleeding (aneurysm, ectopic rupture), vaginal bleeding
HYPOVOLEMIC SHOCK
• May be from nonhemorrhagic fluid loss from;• gastrointestinal tract (vomiting, diarrhea,
fistula),• urinary loss (hyperglycemia with
glucosuria), • evaporative loss (fever, hyperthermia)• intestinal fluid shifts (third spacing as with a
bowel obstruction)
HYPOVOLEMIC SHOCK
Clinical sign
• Depend on volume lost
• Symptoms include: tachycardia, hypotension, decreased urine output, mental status changes, tachypnea
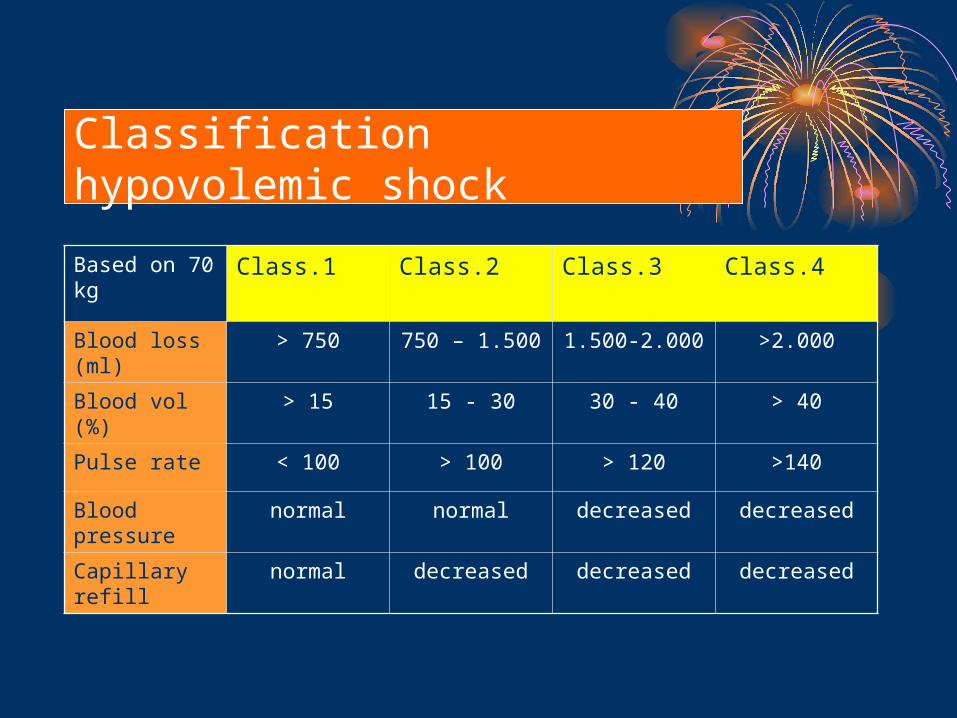
Classification hypovolemic shock
Based on 70 kg
Class.1 Class.2 Class.3 Class.4
Blood loss (ml)
> 750 750 – 1.500 1.500-2.000 >2.000
Blood vol (%) > 15 15 - 30 30 - 40 > 40
Pulse rate < 100 > 100 > 120 >140
Blood pressure
normal normal decreased decreased
Capillary refill
normal decreased decreased decreased
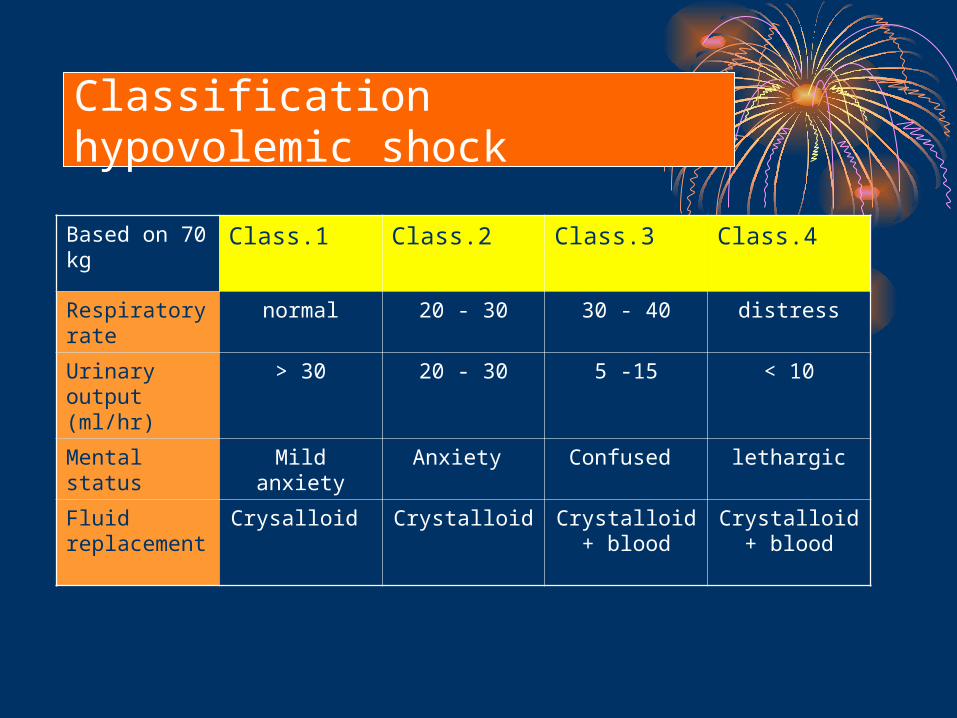
Classification hypovolemic shock
Based on 70 kg
Class.1 Class.2 Class.3 Class.4
Respiratory rate
normal 20 - 30 30 - 40 distress
Urinary output (ml/hr)
> 30 20 - 30 5 -15 < 10
Mental status
Mild anxiety Anxiety Confused lethargic
Fluid replacement
Crysalloid Crystalloid Crystalloid + blood
Crystalloid + blood
DIAGNOSIS
• VITAL SIGN.• Heart rate• Blood pressure• TemSperature• Urine output• Pulse oxymetri
• Patient with normal or near normal signs, 50-85% are still in shock
HEART RATE (HR)
• TACHYCARDIA is an early sign of significantvolume loss in shock.
• The heart rate of young patient or those on β blockers may be not increase
• Bradycardia after prolonged hypotension precludes cardiovascular collapse
BLOOD PRESSURE (BP)
• HYPOTENSION and narrowing pulse pressure are a sign of severe volume loss and shock.
• Mean arterial pressure (MAP) is a better guide to therapy than systolic BP
TEMPERATURE
• Hyperthermia, normothermia, hypothermia may be present in shock.
• Hypothermia is a sign of severe hypovolemic and septic shock
URINE OUTPUT
• Early guide of hypovolemia and end organ response (renal) to shock.
• This is a delayed vital sign because 1 to 2 hours are needed to obtain an acurate measure
PULSE OXIMETRY
• Continuously measured and early indicator of hypoxemia but may be invalid in hypothermic patients
INVASIVE HEMODYNAMIC MONITORING
1. Arterial catheters2. Central venous catheters
(CVc)3. Pulmonary arterial catheters
(PAc)
INVASIVE HEMODYNAMIC MONITORING
•Arterial catheters; give continuous blood pressure measurement.
•Central venous catheters (CVc); gives continuous central venous pressure (CVP) measurement.
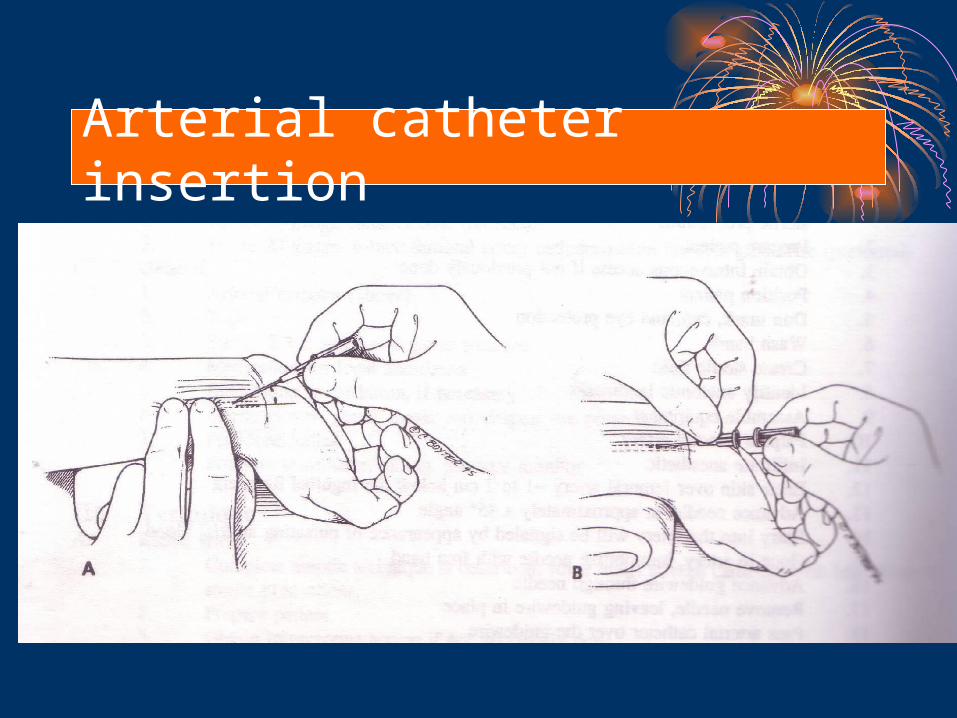
Arterial catheter insertion
INVASIVE HEMODYNAMIC MONITORING
• Pulmonary arterial catheters (PAc) can measure CVP, right arterial (RA) pressure, pulmonary artery pressure (PAp), pulmonary arterial occlusion pressure (PAOp / wedge pressure), cardiac output (CO).
• PAc will help guide aggresive resuscitation in patient with severe shock
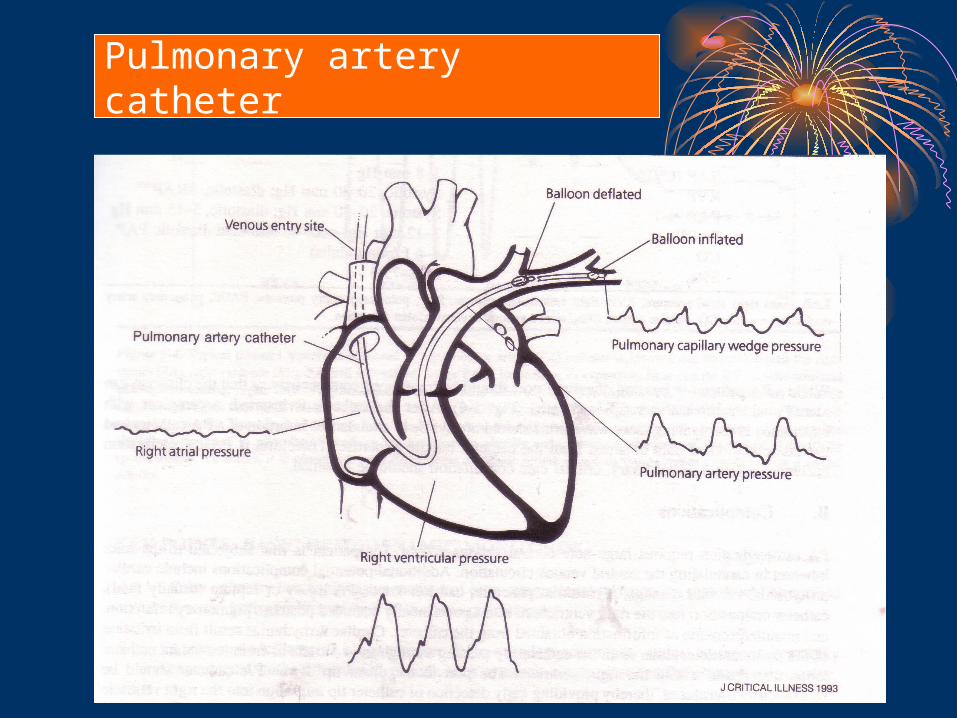
Pulmonary artery catheter
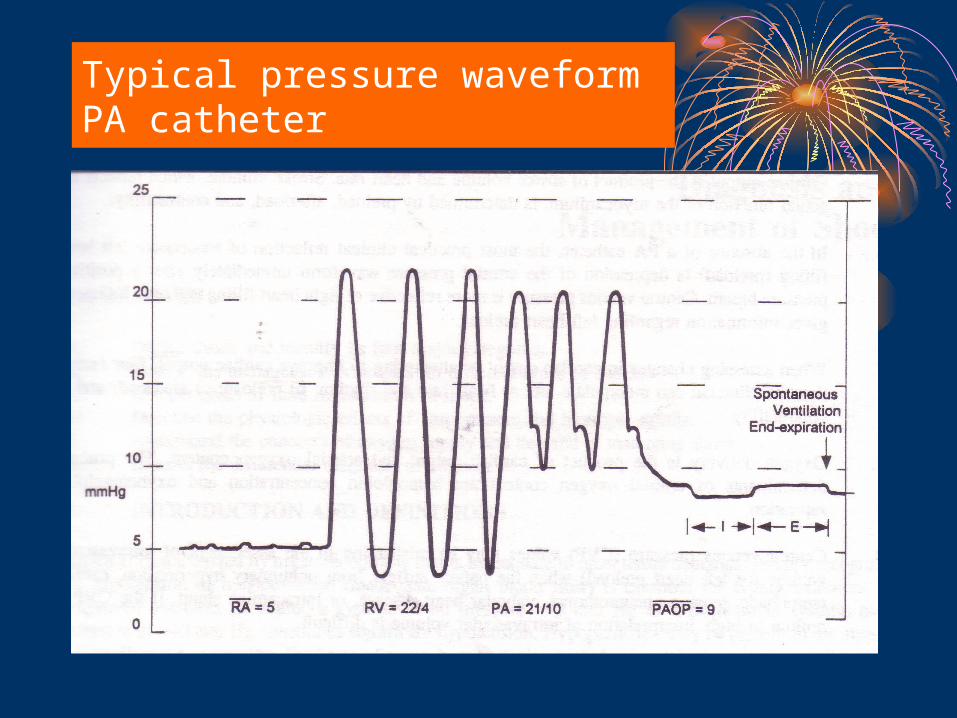
Typical pressure waveform PA catheter
CARDIAC OUTPUT – CARDIAC INDEX
• Cardiac output (CO) or Cardiac index (CI) reflect cardiac function and can be directly measured by a PAC.
• Optimizing CI can be increased by increasing preload , increasing contractility or decreasing afterload
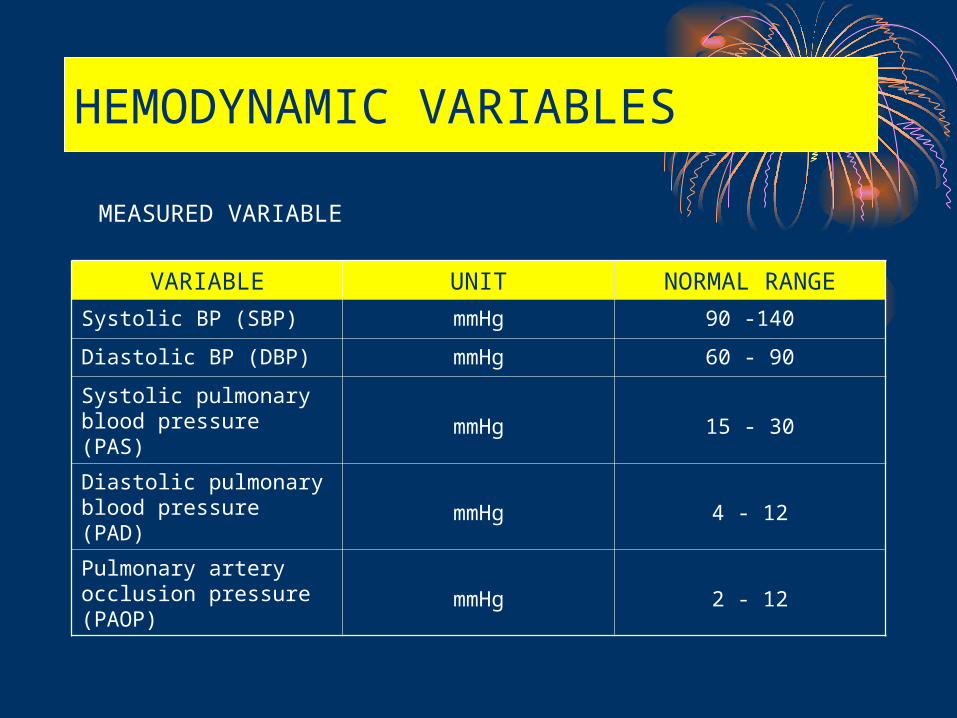
HEMODYNAMIC VARIABLES
VARIABLE UNIT NORMAL RANGE
Systolic BP (SBP) mmHg 90 -140
Diastolic BP (DBP) mmHg 60 - 90
Systolic pulmonary blood pressure (PAS) mmHg 15 - 30
Diastolic pulmonary blood pressure (PAD) mmHg 4 - 12
Pulmonary artery occlusion pressure (PAOP)
mmHg 2 - 12
MEASURED VARIABLE
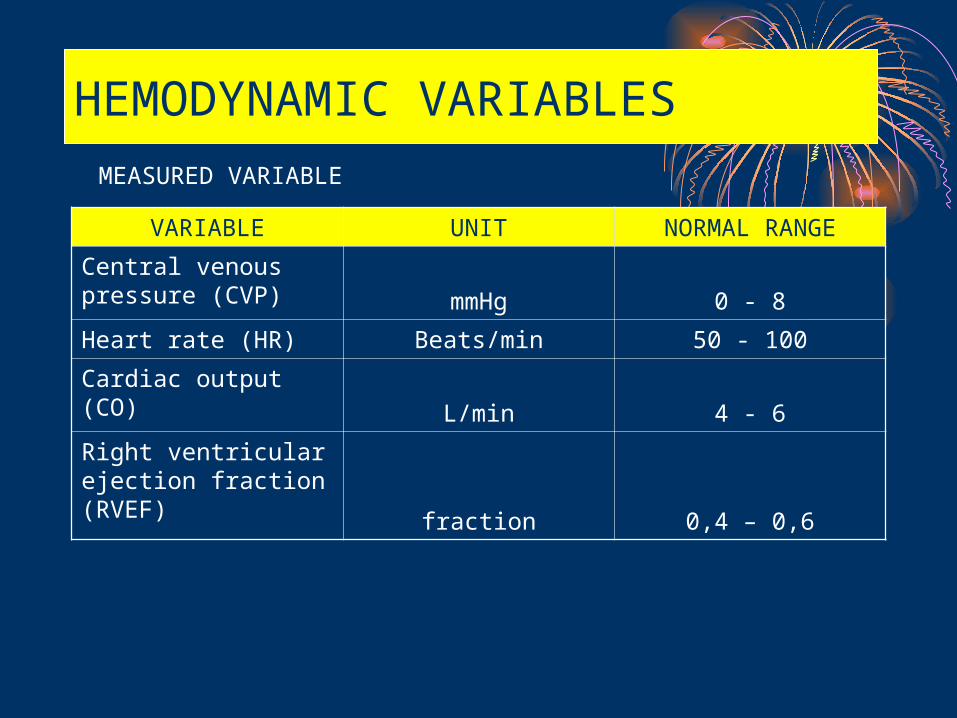
HEMODYNAMIC VARIABLES
VARIABLE UNIT NORMAL RANGE
Central venous pressure (CVP) mmHg 0 - 8
Heart rate (HR) Beats/min 50 - 100
Cardiac output (CO)L/min 4 - 6
Right ventricular ejection fraction (RVEF) fraction 0,4 – 0,6
MEASURED VARIABLE
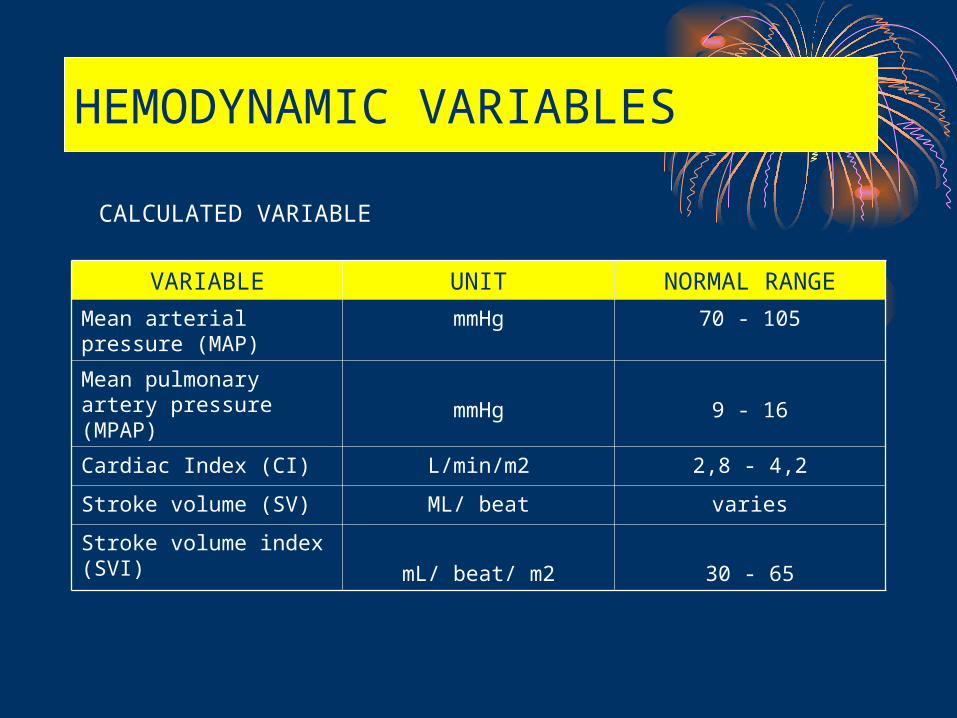
HEMODYNAMIC VARIABLES
VARIABLE UNIT NORMAL RANGE
Mean arterial pressure (MAP)
mmHg 70 - 105
Mean pulmonary artery pressure (MPAP) mmHg 9 - 16
Cardiac Index (CI) L/min/m2 2,8 - 4,2
Stroke volume (SV) ML/ beat varies
Stroke volume index (SVI) mL/ beat/ m2 30 - 65
CALCULATED VARIABLE
TREATMENT
• Rapid recognition and restoration of perfusion is the key to preventing multiple organ dysfunction and death.
• In all forms of shock, rapid restoration of preload with infusion of fluids is the first treatment
TREATMENT
• Crystalloid is first infused and then blood is infused if shock is secondary to hemorrhage.
• Early diagnosis of the etiology is essential and further treatment of the shock depends on its etiology.
TREATMENTHypovolemic shock
• Rapid infusion of crystalloid, large-bore venous acces is needed and central access may be necessary .
• Blood tranfused after 2-3 liter crystalloid, if the cause is hemorrhage. The source of bleeding needs to be controlled
Basic management
• The initial therapy of choice: replacement of intravascular volume.
• Physical examination may provide valuable information about the intravascular volume status (clear lung field and flat neck vein suggest a need for additional fluid resuscitation in the hypotensive patient).