Embed Size (px)
Citation preview

Short- and Long-term Effects of OutpatientRehabilitation in Patients with Chronic
Obstructive Pulmonary Disease:A Randomized Trial
Thierry Troosters, PhD, Rik Gosselink, PhD, Marc Decramer, PhD
PURPOSE: Pulmonary rehabilitation programs are effective inpatients with severe chronic obstructive pulmonary disease(COPD) in the short term, but their long-term effects are notknown. We investigated the short- and long-term effects of a6-month outpatient rehabilitation program in patients with se-vere COPD.SUBJECTS AND METHODS: One hundred patients wererandomly assigned to receive either an exercise training pro-gram that included cycling, walking, and strength training (n 550) or usual medical care (n 5 50). Thirty-four patients in thetraining group were evaluated after 6 months (end of training),and 26 were evaluated after 18 months of follow-up. In thecontrol group, 28 patients were evaluated at 6 months and 23after 18 months. We measured pulmonary function, 6-minutewalking distance, maximal exercise capacity, peripheral and re-spiratory muscle strength, and quality of life (on a 20 to 140 –point scale), and estimated the cost-effectiveness of the pro-gram.RESULTS: At 6 months, the training group showed improve-
ment in 6-minute walking distance [mean difference (train-ing 2 control) of 52 m; 95% confidence interval (CI), 15 to89 m], maximal work load (12 W; 95% CI, 6 to 19 W), maximaloxygen uptake (0.26 liters/min; 95% CI, 0.07 to 0.45 liters/min),quadriceps force (18 Nm; 95% CI, 7 to 29 Nm), inspiratorymuscle force (11 cm H2O; 95% CI, 3 to 20 cm H2O), and qualityof life (14 points; 95% CI, 6 to 21 points; all P ,0.05). At 18months all these differences persisted (P ,0.05), except for in-spiratory muscle strength. For 6-minute walking distance andquality of life, the differences between the training group andcontrols at 18 months exceeded the minimal clinically-impor-tant difference.CONCLUSION: Among patients who completed the 6-monthprogram, outpatient training resulted in significant and clini-cally relevant changes in 6-minute walking distance, maximalexercise performance, peripheral and respiratory musclestrength, and quality of life. Most of these effects persisted 18months after starting the program. Am J Med. 2000;109:207–212. q2000 by Excerpta Medica, Inc.
Pulmonary rehabilitation programs improve func-tional exercise capacity and quality of life in pa-tients with severe chronic obstructive pulmonary
disease (COPD) (1). However, the effects of outpatienttraining programs have not been studied comprehen-sively in a randomized controlled trial. Well-conductedstudies have previously used only limited outcome mea-sures that focused on functional exercise performance orquality of life (2,3). In addition, the long-term mainte-nance of these benefits was not addressed in most of therandomized trials (4 –7). In two trials that had long-termfollow-up (3,8), there were no clear effects 18 monthsafter starting the program. This may have been because of
the short duration of the interventions in those studies(9).
We performed a randomized trial to investigate theshort- and long-term effects of a 6-month outpatienttraining program as compared with usual care. The effec-tiveness of the program was assessed in terms of pulmo-nary function, functional and maximal exercise capacity,peripheral and respiratory muscle strength, and quality oflife. In addition, we estimated the cost-effectiveness of thetraining program.
MATERIAL AND METHODS
Patients were sampled from consecutive patients referredto our outpatient clinic between 1995 and 1997. Theywere randomly assigned to the training or control groupusing sealed envelopes that had been prepared before thestart of the study. Patients were eligible for inclusion ifthey were younger than 75 years of age, had a forced ex-piratory volume in 1 second (FEV1) that was less than65% of the predicted value, and if their clinical conditionwas stable at inclusion, with no infection or COPD exac-erbation in the previous 4 weeks. We excluded patients
From the Respiratory Rehabilitation and Respiratory Division, Univer-sity Hospitals Katholieke Universiteit Leuven, Leuven, Belgium, andFaculty of Physical Education and Physiotherapy, Katholieke Univer-siteit Leuven, Leuven, Belgium.
Supported by the Fonds voor Wetenschappelijk Onderzoek-Vlaan-deren (G0189.97 and G0175.99), Levenslijn Grant 7.0002.94, andOnderzoeksfonds KU Leuven, Grant 27/98.
Requests for reprints should be addressed to Rik Gosselink, PhD, PT,Division of Respiratory Rehabilitation, University Hospital Gasthuis-berg, Herestraat 49, 3000 Leuven, Belgium.
Manuscript submitted June 14, 1999, and accepted in revised formMay 10, 2000.
q2000 by Excerpta Medica, Inc. 0002-9343/00/$–see front matter 207All rights reserved. PII S0002-9343(00)00472-1

with other severe medical problems, such as heart failure,myocardial infarction, cerebrovascular disease, cancer, ororthopedic disorders. The study was approved by the lo-cal ethics committee.
Measurements were made at enrollment, and at 6months and 18 months after the start of the study. At allvisits, patients underwent spirometry and whole bodyplethysmography (Body Box 1085, Medical Graphics,Inc., St. Paul, Minnesota). FEV1 and forced vital capacitywere measured according to the European RespiratorySociety guidelines for pulmonary function testing (10).In addition, the diffusing capacity for carbon monoxidewas measured by the single breath method (Sensor Med-ics 6200, Bilthoven, The Netherlands) at the initial visit.Results were expressed as a percentage of the predictednormal values (10).
Isometric quadriceps strength was measured using aCybex II dynamometer (Lumex, Bay Shore, New York).Peak extension torque was evaluated at 60 degrees of kneeflexion. Reference values for quadriceps force were devel-oped in our laboratory (11). Tests were performed at leastthree times, and the best of two reproducible tests wasused for further analysis.
Inspiratory and expiratory muscle strength was mea-sured using standard techniques (12). At least five at-tempts were made to measure expiratory muscle strengthfrom total lung capacity and to measure inspiratory mus-cle strength from residual volume. Both were determinedas the pressure that could be sustained for at least 1 sec-ond. Tests were repeated until the variability among thethree best attempts was less then 5%. The highest valuewas expressed as a percent of the predicted value (13).
Functional exercise performance was measured by a6-minute corridor-walking test. Encouragement wasstandardized (14). A 54-m improvement was consideredclinically important (15). To avoid learning effects, thebest of two tests was used and expressed as percent of thepredicted value (16).
Maximal exercise capacity was assessed by maximal cy-cle ergometry (Partn’air 5400; Medisoft, Dinant, Bel-gium). Patients cycled at an incremental workload (110W per minute) until exhaustion. Oxygen consumption,carbon dioxide output, and ventilation were measuredbreath by breath. Heart rate was monitored constantly.Maximal oxygen consumption was compared with nor-mal values (17). At 6 months, data obtained from a max-imal exercise test were analyzed at 60% of the initialworkload.
The Chronic Respiratory Disease Questionnaire (18)was used to assess health-related quality of life. This 20-item questionnaire, which scores quality of life into fourdomains (dyspnea, mastery, emotional functioning, andfatigue) has been validated in the Dutch language (19).
InterventionPatients assigned to the training program were invited toattend the outpatient sessions three times a week in thefirst 3 months; during the subsequent 3 months, trainingfrequency was reduced to twice weekly. Each session hada duration of 1.5 hours. Training items were cycling,treadmill walking, stair climbing, and peripheral muscletraining. Patients started the program at 60% of the initialmaximal workload on the cycle ergometer and at 60% oftheir maximal walking speed during the 6-minute walk-ing test. During the first 3 months, this workload wasincreased up to 80% of the maximal workload and max-imal walking speed. In each session, patients also per-formed arm cranking and stair climbing in 2-minuteblocks (1 to 3 repetitions). Peripheral muscle strengthtraining on a multi-gym device was performed in threeseries of 10 repetitions at 60% of the one repetition max-imum for each muscle group (triceps, latissimus dorsi,pectoralis, and quadriceps muscle). Physiotherapists en-sured close supervision and continuous encouragementof the patients. Oxygen saturation and heart rate weremeasured during the training sessions. Supplemental ox-ygen was given to maintain oxygen saturation above 90%.
Cost-effectivenessThe program had a cost of $57 per session per patient,based on the charges as reimbursed by the NationalHealth Insurance, which covers the salary for 1.5 hours oftreatment from a physical therapist. The total cost of theprogram per patient was determined by multiplying thiscost by the number of sessions.
Statistical AnalysisBaseline characteristics of the two groups were comparedusing unpaired t tests. The effects of treatment (trainingor control) were analyzed with a repeated measures anal-ysis of variance. Unpaired t tests were used to evaluate theeffects of treatment at the end of training (6 months) andfollow-up (18 months). Statistical significance was set atP ,0.05. All tests were performed with the StatisticalAnalysis System (SAS Institute, Cary, North Carolina).
RESULTS
One hundred consecutive eligible patients fulfilled inclu-sion criteria and were randomly assigned to either thetraining group (n 5 50) or the control group (n 5 50).Three patients (1 in the training group and 2 in the con-trol group) refused initial testing, leaving 97 patients whounderwent initial tests. Of these, 12 patients refused toparticipate in the training sessions, and 15 patients in thecontrol group refused further follow-up. Except that theywere older [mean (6 SD) age of 66 6 7 years vs 61 6 9years, P ,0.004], these patients did not differ from thepatients with follow-up. In addition, 3 of the remaining
Effects of Outpatient Rehabilitation in Chronic Obstructive Pulmonary Disease/Troosters et al
208 August 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109

37 patients in the training group (2 of whom died) and 5of the remaining patients in the control group (3 of whomdied) were not able to comply with short-term follow-up(6 months). Long-term (18-month) follow-up could notbe performed in 11 of the 37 patients in the traininggroup (9 of whom died) and in 10 of the 33 patients (7 ofwhom died) in the control group. There were no differ-ences in 18-month mortality between the two groups(P 5 0.79).
All patients had severe COPD with moderate periph-eral and respiratory muscle weakness and with impairedfunctional and maximal exercise capacity. There were nosignificant differences in the characteristics of the 70 pa-tients who participated in the training and control groups(Table 1). Patients who died during the trial (n 5 16) hada significantly lower FEV1 (32% 6 12% vs 45% 6 13% ofpredicted, P ,0.001), diffusing capacity for carbon mon-oxide (41% 6 19% vs 64% 6 25% of predicted, P,0.001), walking distance (357 6 117 vs 429 6 124 m, P
,0.05), and maximal exercise capacity (58 6 30 vs 79 634 W, P ,0.02) than those who survived.
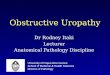
Rehabilitation ProgramPatients in the training group participated in a mean of46 6 11 sessions (attendance rate 77% 6 19%). Trainingintensity for walking and cycling reached a plateau, onaverage, after 3 months (Figure 1). Heart rate during thetraining session averaged 92% 6 9% of the maximalachieved heart rate during the incremental maximal ex-ercise test and remained relatively constant throughoutthe 6 months of training.
Effects of TrainingCompared with usual care, there were no significant ef-fects of the training program on measures of pulmonaryfunction. The training program did, however, improve6-minute walking distance, maximal work load, maximaloxygen uptake, quadriceps force, and quality-of-life score
Figure 1. Upper panel: training intensity (mean 6 SD) fortreadmill walking (open circles) and cycle exercise (closed cir-cles). Workload during cycle exercise (in watts) is expressedrelative to the maximal workload achieved during the maximalincremental exercise test. Workload during treadmill walking isexpressed as percent of the speed achieved during the initial6-minute walking test. Lower panel: total training time(mean 6 SD) during training sessions, by week of training.
Table 1. Characteristics of Subjects in the Control and TrainingGroups*
Characteristic
ControlGroup
(n 5 33)
TrainingGroup
(n 5 37)
Mean 6 SD or Number(Percent)
Age (years) 63 6 7 60 6 9Male sex 30 (90) 31 (81)Body mass index (kg/m2) 25 6 5 24 6 4Forced expiratory volume in
1 second (percentpredicted)
43 6 12 41 6 16
Forced vital capacity(percent predicted)
84 6 18 81 6 19
Diffusing capacity forcarbon dioxide (percentpredicted)
64 6 25 60 6 28
Maximal inspiratorypressure (percentpredicted)
66 6 23 72 6 24
Maximal expiratory pressure(percent predicted)
74 6 29 75 6 27
Quadriceps force (percentpredicted)
80 6 24 79 6 25
6-minute walking distance(percent predicted)
61 6 18 60 6 19
Maximal work load (watts) 86 6 40 76 6 36Maximal oxygen uptake
(percent predicted)72 6 39 74 6 35
Disease-specific quality oflife (points)†
84 6 22 77 6 17
* Only patients who participated in the training sessions or follow-upare included.† As assessed using the Chronic Respiratory Disease Questionnaire(range, 20 to 140).
Effects of Outpatient Rehabilitation in Chronic Obstructive Pulmonary Disease/Troosters et al
August 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109 209

(Table 2, Figure 2). After 6 months, ventilation at iso-workload (60% of the initial maximal work load) de-creased significantly (22.3 6 4.9 liters) compared withcontrol (11.2 6 4.5 liters, P ,0.05), while oxygen uptakewas similar in the two groups. Changes in carbon dioxideproduction were not significantly different between thetraining and the control group. Mean change in heart ratewas somewhat greater in the training group comparedwith the control group (28 6 11 vs 21 6 13, P 5 0.06) atthis submaximal workload.
After 18 months, the improvements in 6-minute walk-ing distance (difference between mean change from base-line in the treatment group 2 mean change from baselinein the control group of 90 m; 95% confidence interval[CI], 41 to 149 m; P ,0.01), maximal work load (13 W;95% CI, 4 to 22 W; P ,0.05), maximal oxygen uptake(0.27 liters/min; 95% CI, 0.02 to 0.52 liters/min; P,0.05), quadriceps strength (15 Nm; 95% CI, 1 to 30Nm; P ,0.05), and quality of life (17 points; 95% CI, 8 to26 points; P ,0.001) were maintained in the traininggroup compared with the control group.
The improvements in quadriceps strength were corre-lated with the improvements in walking distance at both 6months (r 5 0.38, P ,0.05) and 18 months (r 5 0.47, P,0.05).
The mean cost of the program per patient was$2,615 6 $625
DISCUSSION
We found that a 6-month outpatient rehabilitation pro-gram that involved moderate-to-high training intensity
did not alter pulmonary function, but did improve func-tional and maximal exercise performance, peripheral andrespiratory muscle strength, and quality of life whencompared with usual care in patients with severe COPD.Improvements in functional and maximal exercise per-formance and quality of life were clinically relevant (15)and were maintained 18 months after the onset of train-ing. However, 31% of patients dropped out of the studyby 6 months, and 36% by 18 months. Goldstein et al (2)reported similar dropout and refusal rates. In our study,the main reasons for dropping out were unwillingness toparticipate in the rehabilitation sessions, refusal to partic-ipate in further assessments, or death. Patients who diedduring the trial had severe disease, as manifested by lowvalues for FEV1 and diffusing capacity for carbon mon-oxide, and a low exercise capacity (20 –22). As reportedby others, the pulmonary rehabilitation program did notprevent short-term mortality (3).
The training regimen that we used differed somewhatfrom other trials. Patients trained at a slightly greater in-tensity than reported by Maltais et al (23), but the train-ing time for each session was substantially shorter in ourstudy. The mean attendance rate in our study (77% 619%) was similar to that in the study of Bendstrup et al(6), although less than that reported by others (23).
The magnitude of the training effect (approximately20% improvement) in this study is similar to other trials,as measured by improvement in functional exercise ca-pacity (5,24 –26) and maximal exercise capacity(8,24,27,28). Although some trials have not demon-strated improvements in maximal oxygen uptake(4,24,28,29), the increase (12% 6 29%) that we achieved
Table 2. Effects of a Pulmonary Rehabilitation Training Program at 6 Months, Compared withControl*
Measurement
Absolute Values Difference betweenGroups in Change
from Baseline(95% Confidence
Interval)P
Value†
ControlGroup
(n 5 28)
TrainingGroup
(n 5 34)
Forced expiratory volume in 1second (L)
1.3 6 0.4 1.2 6 0.5 0.04 (20.09–0.12) 0.89
Quadriceps force (Nm) 121 6 52 144 6 45 18 (7–30) 0.004Maximal inspiratory pressure
(cm H2O)68 6 23 83 6 28 11 (3–20) 0.04
6-minute walking distance (m) 438 6 104 468 6 125 52 (15–89) 0.01Maximal work load (watts) 85 6 37 88 6 36 12 (6–19) 0.003Maximal oxygen uptake
(L/min)1.54 6 0.63 1.63 6 0.64 0.256 (0.07–0.45) 0.02
Disease-specific quality of life(points)
82 6 25 90 6 18 14 (6–21) 0.002
* Results are presented both as absolute values at 6 months and as the difference (change in treatment group2change in control group) from baseline.† For the comparison of difference in change from baseline.
Effects of Outpatient Rehabilitation in Chronic Obstructive Pulmonary Disease/Troosters et al
210 August 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109

resembles that reported in studies that used strenuous,individually-tailored cycle exercise (3,23,30,31). The im-provements that we observed in all four dimensions ofquality of life were similar to those reported in a recentmeta-analysis (1).
Most of the benefits of training in this study persistedfor 12 months after the training program had been com-pleted. Swerts et al (9) reported that the improvementsseen after an 8-week program declined gradually during 1year of follow-up, whereas patients who continued thetraining program for 20 weeks (60 sessions) maintainedimprovements in walking distance. Two other studiesthat had shorter training periods were unable to showlong-term benefits (3,8). Whether this apparent discrep-ancy is the result of the duration of the training programis not clear. In our study, the maintained improvement at18 months not only reached statistical significance, butalso the difference with controls exceeded the minimal
clinically-important difference for improvements inquality of life and functional exercise capacity. For thelatter test, it was estimated to be 54 m (19). In our study,after the rehabilitation period had been completed, theaverage improvement—which was approximately 90 min walking distance—persisted in those subjects who re-turned for the 1-year follow-up. Similar and persistentimprovements in quality of life were also seen, whereasthere was a significant and clinically-important deterio-ration of mean quality of life in the control group.
Our outpatient-based program had a mean cost perpatient of approximately $2,600 to achieve a mean im-provement of 52 m in 6-minute walking distance at 6months. A previous study reported that a hospital-basedprogram cost approximately $7,800 per patient and re-sulted in a 37m improvement in 6-minute walking dis-tance (2). Thus, outpatient rehabilitation appears to bemore cost-effective than an inpatient program. Com-pared with home rehabilitation, which was reported tocost approximately $660 per patient and resulted in ap-proximately a 39m improvement in 6-minute walkingdistance (8), the costs of our rehabilitation program weregreat. However, the patients in our study had more severedisease than those in the study of the home-care programand might need more careful monitoring during training.Indeed, prudent training strategies in a home setting werenot effective in one study that enrolled patients with se-vere COPD (7).
We conclude that a 6-month outpatient rehabilitationprogram with high-intensity training resulted in clinical-ly-relevant improvements in functional and maximal ex-ercise capacity, peripheral and respiratory musclestrength, and quality of life in patients with severe COPDwho were willing to participate in the program. Most ofthe effects were maintained among patients who com-pleted the 18-month follow-up.
ACKNOWLEDGMENTThe authors thank Edgard Kellens, Anne Cattaert, HildeWitvrouwen, Katleen Schrever, staff members involved in thetraining sessions. We also acknowledge the excellent statisticalaid of Renild Schepers.
REFERENCES1. Lacasse Y, Wong E, Guyatt GH, et al. Meta-analysis of respiratory
rehabilitation in chronic obstructive pulmonary disease. Lancet.1996;348:1115–1119.
2. Goldstein RS, Gort EH, Stubbing D, et al. Randomised controlledtrial of respiratory rehabilitation. Lancet. 1994;344:1394 –1397.
3. Ries AL, Kaplan RM, Limberg TM, Prewitt LM. Effects of pulmo-nary rehabilitation on physiologic and psychosocial outcomes inpatients with chronic obstructive pulmonary disease. Ann InternMed. 1995;122:823– 832.
4. Reardon J, Awad E, Normandin E, et al. The effect of comprehen-
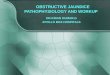
Figure 2. Training effect for 6-minute walking distance (up-per), expressed as mean (6 SD) percent change compared withbaseline. Mean 6 SD training effect for the change in the dys-pnea dimension of the quality-of-life questionnaire (lower) isexpressed as change (in points) compared with baseline. Thedashed line represents the minimal clinically-important differ-ence. *P ,0.05, **P ,0.01 compared with controls.
Effects of Outpatient Rehabilitation in Chronic Obstructive Pulmonary Disease/Troosters et al
August 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109 211

sive outpatient pulmonary rehabilitation on dyspnea. Chest. 1994;105:1046 –1052.
5. Weiner P, Azgad Y, Ganam R. Inspiratory muscle training com-bined with general exercise reconditioning in patients with COPD.Chest. 1992;102:1351–1356.
6. Bendstrup J, Ingemann Jensen J, Holm S, Bengtsson B. Out-patientrehabilitation improves activities of daily living, quality of life andexercise tolerance in chronic obstructive pulmonary disease. EurRespir J. 1998;10:2801–2806.
7. Wedzicha JA, Bestall JC, Garrod R, et al. Randomized controlledtrial of pulmonary rehabilitation in severe chronic obstructive pul-monary disease patients, stratified with the MRC dyspnea scale. EurRespir J. 1998;12:363–369.
8. Strijbos JH, Postma DS, Van Altena R, et al. A comparison betweenoutpatient hospital-based pulmonary rehabilitation program and ahome-care pulmonary rehabilitation program in patients withCOPD. A follow-up of 18 months. Chest. 1996;109:366 –372.
9. Swerts PMJ, Kretzers LMJ, Terpstra-Lindeman E, et al. Exercisereconditioning in the rehabilitation of patients with chronic ob-structive pulmonary disease: a short- and long-term analysis. ArchPhys Med Rehabil. 1990;71:550 –573.
10. Quanjer PH, Tammeling GJ, Pedersen OF, et al. Lung volumes andforced expiratory flows. Eur Respir J. 1993;6(suppl 16):5– 40.
11. Decramer M, Lacquet LM, Fagard R, Rogiers P. Corticosteroidscontribute to muscle weakness in chronic airflow obstruction. Am JRespir Crit Care Med. 1994;150:11–16.
12. Black LF, Hyatt RE. Maximal respiratory pressures: normal valuesand relationship to age and sex. Am Rev Respir Dis. 1969;99:696 –702.
13. Rochester D, Arora NS. Respiratory muscle failure. Med Clin NorthAm. 1983;67:573–598.
14. Guyatt GH, Pugsley SO, Sullivan MJ, et al. Effect of encouragementon walking test performance. Thorax. 1984;39:818 – 822.
15. Redelmeier DA, Bayoumi AM, Goldstein R, Guyatt G. Interpretingsmall differences in functional status: the six minute walk test inchronic lung disease patients. Am J Respir Crit Care Med. 1997;155:1278 –1282.
16. Troosters T, Gosselink R, Decramer M. Six minute walking distancein healthy elderly subjects. Eur Resp J. 1999;14:270 –274.
17. Jones NL, Makrides L, Hitchcock C, et al. Normal standards for anincremental progressive cycle ergometer test. Am Rev Respir Dis.1985;131:700 –708.
18. Guyatt GH, Berman LB, Townsend M, et al. A measure of quality oflife for clinical trials in chronic lung disease. Thorax. 1987;42:773–778.
19. Gosselink HAAM, Wagenaar RC, Keimpema VA, Chadwick-Straver RVM. The effects of a rehabilitation program in patientswith COPD and asthma. Ned Tijdschr Fysioth. 1990;100:193–199.
20. Dubois P, Machiels J, Smeets F, et al. CO transfer capacity as adetermining factor of survival for severe hypoxemic patients underlong-term oxygen therapy. Eur Respir J. 1990;3:1042–1047.
21. Ebi-Kryston KL. Predicting 15 year chronic bronchitis mortality inthe Whitehall study. J Epidemiol Community Health. 1989;43:168 –172.
22. Gerardi DA, Lovett L, Benoit-Connors ML, ZuWallack RL. Vari-ables related to increased mortality following outpatient pulmo-nary rehabilitation. Eur Respir J. 1996;9:431– 435.
23. Maltais F, Leblanc P, Jobin J, et al. Intensity of training and physi-ologic adaptation in patients with chronic obstructive pulmonarydisease. Am J Respir Crit Care Med. 1997;155:555–561.
24. O’Donnell DE, McGuire MA, Samis L, Webb KA. The impact ofexercise reconditioning on breathlessness in severe chronic airflowlimitation. Am J Respir Crit Care Med. 1995;152:2005–2013.
25. ZuWallack RL, Patel K, Reardon JZ, et al. Predictors of improve-ment in the 12-minute walking distance following a six-week out-patient pulmonary rehabilitation program. Chest. 1991;99:805–808.
26. White RJ, Rudkin ST, Ashley J, et al. Outpatient pulmonary reha-bilitation in severe chronic obstructive pulmonary disease. J RoyColl Phys London. 1997;31:541–545.
27. Wanke T, Formanek D, Lahrmann H, et al. The effects of com-bined inspiratory muscle and cycle ergometer training on exer-cise performance in patients with COPD. Eur Respir J. 1994;7:2205–2211.
28. Casaburi R, Porszasz J, Burns MR, et al. Physiologic benefits ofexercise training in rehabilitation of patients with severe chronicobstructive pulmonary disease. Am J Respir Crit Care Med. 1997;155:1541–1551.
29. Clark CJ, Cochrane JE, Mackay E. Low intensity peripheral muscleconditioning improves exercise tolerance and breathlessness inCOPD. Eur Respir J. 1996;9:2590 –2596.
30. Vallet G, Ahmaidi S, Serres I, et al. Comparison of two trainingprogrammes in chronic airway limitation patients: standardizedversus individualized protocols. Eur Respir J. 1997;10:114 –122.
31. Wijkstra PJ, Van der Mark TW, Kraan J, et al. Effects of homerehabilitation on physical performance in patients with chronicobstructive pulmonary disease (COPD). Eur Respir J. 1996;9:104 –110.
Effects of Outpatient Rehabilitation in Chronic Obstructive Pulmonary Disease/Troosters et al
212 August 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109