Embed Size (px)
Citation preview

Short- and Long-Term Outcomes ofWiktor Stent Implantation at Low Versus
High PressuresPaul Yang, MD, Mariann Gyongyosi, MD, PhD, Ali Hassan, MD, Gunter Heyer, MD,Werner Klein, MD, Olev Luha, MD, Edwin Maurer, MD, Volker Muhlberger, MD,
Othmar Pachinger, MD, Heinz Sochor, MD, Josef Sykora, MD, Heinrich Weber, MD,Franz Weidinger, MD, and Dietmar Glogar, MD,
on behalf of the Austrian Wiktor Stent Study Group
A prospective, randomized, multicenter trial was con-ducted to evaluate whether high-pressure postdilation ofthe Wiktor stent provides short- and long-term benefitscompared with the conventional low-pressure implanta-tion technique. From June 1995 through May 1996, 181patients were randomly assigned to either low-pressure(6 to 12 atm, group A, n 5 94) Wiktor stent placementor to high-pressure postdilation (>13 atm, group B, n 587) after stent deployment. All patients were followed upclinically for 7 6 3 months, with an angiographic follow-upin 154 patients (85%). After stent implantation, neitherminimal lumen diameter (MLD) nor percent diameter ste-nosis (%DS) differed significantly between the 2 groups(MLD, 2.8 6 0.5 vs 2.9 6 0.5 mm; %DS, 17 6 8% vs 16 69% for groups A and B, respectively). However, a trendtoward a larger mean lumen diameter within the stent wasobserved in group B (3.3 6 0.6 vs 3.5 6 0.5 mm for
groups A and B, respectively; difference between means0.14 mm, 95% confidence interval 20.01 to 0.29, p 50.08). Angiographic follow-up revealed similar MLD and%DS in both treatment groups (MLD, 2.1 6 0.7 vs 2.2 60.8 mm; %DS, 31 6 17% vs 30 6 24% for groups A andB, respectively, p 5 NS). Acute stent thrombosis occurred in2 patients (1%) (1 patient in each group), and subacutethrombosis in 1 patient (0.6%) in group A. There was 1death in group A, and target lesion restenosis (>50% DS)was observed in 15% of patients with no differences be-tween the groups. In conclusion, this study demonstratedfavorable short- and long-term results of Wiktor stent im-plantation. Despite a trend toward additional initial lumengain by high-pressure postdilation, this did not translateinto a measurable improvement in long-term outcome.Q1999 by Excerpta Medica, Inc.
(Am J Cardiol 1999;84:644–649)
In contrast to numerous stainless steel stents of tu-bular or mesh design,1–6 there are insufficient data
regarding adjunctive high-pressure balloon dilation incoil stents, such as Wiktor stents. The Wiktor stent, asingle-wire tantalum coil stent, has not undergoneprofound prospective investigations with respect tosafety and efficacy of high-pressure stenting. It isconceivable that the coil configuration (in conjunctionwith other factors, such as different stent compositionother than stainless steel) may allow optimal stentdeployment without the need for adjunctive high-pressure balloon dilation. Furthermore, whether ag-gressive balloon dilation increases the amount of re-active intimal proliferation and thus leads to evenmore late lumen loss and higher restenosis needs to beclarified.7–9This prospective, randomized, multicenter
trial (the Austrian Wiktor Stent Trial) was thereforedesigned to evaluate whether high-pressure postdila-tion of the Wiktor stent provides short- and long-termbenefits compared with the conventional low-pressureapproach.
METHODSStudy population and protocol: From June 1995
through May 1996, a total of 202 patients were en-rolled prospectively in the trial, which was conductedin 7 Austrian centers. All patients had objective evi-dence of myocardial ischemia and angiographic evi-dence of a target lesion suitable for stent implantation.Indications for stent implantation included elective(primary) stenting,$50% stenosis after balloon an-gioplasty, and threatening or acute vessel closure afterballoon dilatation. Exclusion criteria included a refer-ence diameter,2.5 mm by visual estimation, vesselswith poor or compromised runoff distal to the targetlesion, heavily calcified lesions that would precludeadequate predilatation, and evidence of intracoronarythrombus. Patients with contraindications or intoler-ance to therapy with aspirin or ticlopidine were alsoexcluded.
Patients were randomly assigned by means of cardsin sealed envelopes to either low-pressure Wiktorstent placement at low pressures (6 to 12 atm, groupA) or to high-pressure postdilation ($13 atm, groupB) after stent deployment at low pressures. A cross-
From the Department of Cardiology, University Clinic of Internal Med-icine II, Vienna; Second Department of Internal Medicine, Landeskran-kenanstalten Salzburg, Salzburg; Department of Internal Medicine,Karl-Franzens-University, Graz; Department of Cardiology, MedicalHospital Wels, Wels; Department of Internal Medicine, UniversityHospital of Innsbruck, Innsbruck; Second Medical Department, Land-eskrankenhaus Klagenfurt, Klagenfurt; and Fifth Department of InternalMedicine, Kaiser-Franz-Josef-Hospital, Vienna, Austria. This study wassupported by an educational grant from Medtronic Austria, Vienna,Austria. Manuscript received November 16, 1998; revised manu-script received and accepted May 5, 1999.
Address for reprints: Dietmar Glogar, MD, Department of Cardiol-ogy, University Clinic of Internal Medicine II, Waehringer Guertel 18-20,A-1090 Vienna, Austria. E-mail: [email protected].
644 ©1999 by Excerpta Medica, Inc. All rights reserved. 0002-9149/99/$–see front matterThe American Journal of Cardiology Vol. 84 September 15, 1999 PII S0002-9149(99)00409-9

over between randomization groups was possible atthe operator’s discretion when this was deemed nec-essary.
The investigational protocol was approved by thelocal ethical committees of each participating centerand written informed consent was obtained from allpatients.
Stent implantation procedure: Coronary angiogra-phy and stent implantation procedures were performedaccording to standard clinical practice in each partic-ipating center, by a femoral approach using a 7Fr or8Fr guiding catheter. All patients were pretreated withaspirin ($100 mg/day). Pretreatment with ticlopidine($250 mg/day) was started on the day of the proce-dure. In patients scheduled for elective stent implan-tation, ticlopidine was given beginning 1 or 2 daysbefore the scheduled procedure. During coronary in-tervention, patients received an intravenous bolus of10,000 to 15,000 IU of heparin to maintain an acti-vated clotting time of.300 seconds.
The Wiktor stent (Medtronic, Kerkrade, The Neth-erlands) used during this trial is a balloon-expandablestent of helical coil design composed of a single strandof tantalum wire 0.005 inches in diameter and shapedin a sinusoidal wave pattern. The stent is premountedon a semicompliant polyethylene balloon catheter.Two different stent delivery systems were used at theoperator’s discretion: a “Gold-X” single-operator-ex-change delivery system with a 16-mm Wiktor stentpremounted (used in 88% of patients), or a “Prime”over-the-wire system with a 15-mm Wiktor stent(used in 12%). Nominal, low pressures of 6 to 8 atmwere used to expand the stent. In group A, investiga-tors were permitted to use further balloon inflations atlow pressures (,12 atm) after stent insertion whennecessary. In patients assigned to group B, however, afurther high-pressure balloon inflation ($13 atm) wasrequired after stent deployment regardless of the ini-tial stent result.
Postprocedure medical regimen: There was no strictpostprocedure medication protocol to be used duringthe trial. However, a recommendation was given be-fore the trial: aspirin$100 mg/day for 6 months andticlodipine $250 mg/day for 4 weeks. There wereonly minor differences in the dose of the antiplateletregimen used in the participating institutions: Aspirin100 mg once daily and ticlopidine 250 mg twice dailywere given in 4 of the 7 participating centers (60% ofthe study patients); aspirin 250 mg once daily andticlopidine 250 mg twice daily in 2 centers (20%); andaspirin and ticlopidine both 250 mg once daily weregiven in 1 center (20%).
Data collection: All demographic, clinical, and pro-cedural data were recorded prospectively on standard-ized patient case report forms and forwarded to thecore laboratory at the Vienna University Hospital Car-diac Catheterization Laboratories. Each investigatinginstitution was visited by study monitors at regularintervals for data collection and to ensure the qualityof clinical and angiographic follow-up data. Evidenceof target lesion calcifications or dissections and lesiontypes (classified according to a simplified American
College of Cardiology/American Heart Associationscore)10 were determined by each operator and indi-cated on the case report forms.
Quantitative angiographic analysis: Quantitativecoronary angiographic (QCA) analysis of all proce-dural and follow-up cineangiograms were performedat the core laboratory with the use of a validatededge-detection program (Cardiovascular Measure-ment System Version 2.3D, Medis Medical ImagingSystems, Nuenen, The Netherlands), which has under-gone extensive validation studies and has been de-scribed in detail elsewhere.11,12Minimal lumen diam-eter (MLD), reference diameter (by interpolation),percent diameter stenosis, and mean lumen diameterwere measured. In stented vessel segments, MLD wasrepositioned manually within the stent, when it wasinitially detected outside the stented segment. Calibra-tion was performed in each analyzed cineangiographicframe on contrast-filled catheters as a scaling device todetermine the absolute value (in mm) of MLD.
All QCA measurements were obtained in identicalviews at baseline, after stent implantation, and atfollow-up, after maximal vasodilation with 0.1 to 0.3 ofmg of intracoronary nitroglycerin. End-diastolic frameswere selected for analysis from multiple, preferably or-thogonal, views that best showed the target lesion withno significant foreshortening and overlapping structures.Mean values were calculated from multiple matchedviews for all quantitative angiographic variables. Steno-ses present at follow-up and located at the proximal ordistal outflow of the stent were not measured by meansof QCA, but classified as “peri-stent restenosis” andindicated as such on patient case report forms by eachoperator when a$50% diameter stenosis was evident byvisual inspection. Acute lumen gain was defined as thenet difference between the pre- and postinterventionMLD, and late lumen loss was defined as the net differ-ence in MLD between the postintervention result and thefollow-up angiogram. The ratio of late loss to acute gainwas reported as the loss index.
Intravascular ultrasonic analysis: Intravascular ul-trasound (IVUS) imaging was performed as an op-tional part of the study protocol in a subset of thepatient cohort (n5 31) after diagnostic coronaryangiography and stent implantation. IVUS imageswere obtained with either mechanical (2.9 or 3.2 F,CVIS, Sunnyvale, California) or phased-array elec-tronic IVUS catheters (3.0 F, EndoSonics, RanchoCordova, California) after intracoronary administra-tion of 0.1 to 0.2 mg of nitroglycerin and stored ons-VHS videotapes for subsequent off-line analysis.
Minimal lumen cross-sectional areas were mea-sured in the narrowest segment within the lesion orstent. Lumen cross-sectional areas from segmentsproximal and distal to the target lesion or stent wereaveraged and used as reference values. Absolute val-ues of minimal lesion or stent cross-sectional areaswere also expressed as percentages of the referencecross-sectional area.
Study end points and statistics: The primary studyend point was the angiographic MLD at follow-up.The sample size of 74 patients in each group with
CORONARY ARTERY DISEASE/LOW– VS HIGH–PRESSURE WIKTOR STENT IMPLANTATION 645

angiographic follow-up was determined at the outsetof the study to detect a 0.3-mm difference in MLDbetween the 2 randomized groups, with an assumedstandard deviation of 0.65 mm, ana error of 0.05, and80% power. Secondary study end points were: (1)angiographic target lesion restenosis ($50% diameterstenosis in the stented segment by core laboratoryQCA analysis at follow-up); and (2) occurrence of any1 of the following major adverse cardiac events: death(considered to be cardiac in absence of clear evidenceof noncardiac origin), nonfatal myocardial infarction(serum creatine phosphokinase levels twice the upperlimit of normal with MB fraction$6%, and/or devel-opment of new pathologic Q waves on the electrocar-diogram), lesion-related coronary artery bypass sur-gery, and target lesion reintervention. For patientsexperiencing.1 event, the first event reached wasconsidered.
All statistical analyses were performed on a per-treatment (as-treated) basis according to the final treat-ment in order to take into account crossovers from theinitial randomization. Continuous variables are ex-pressed as mean6 SD and were analyzed by 2-tailedt tests. To avoid possible errors produced by unequalvariances of the means in the 2 groups, the Welchmodified t test was applied when necessary, whichyielded similar results. The means of QCA and IVUSmeasurements after stent implantation and at fol-low-up were compared by the pairedt test. This testwas also used to compare the means before and afterhigh-pressure postdilation within the patients in groupB. The 95% confidence intervals (CI) were calculat-ed.13,14 The Kolmogorov-Smirnov test was applied tocompare the 2 groups for distribution of MLD atbaseline, after stent implantation, and at follow-up.Categoric variables are reported as percentages andwere analyzed by the chi-square test or by Fisher exacttests when necessary. A statistical probability,0.05was considered to indicate significance. All statisticalanalyses were performed using a commercially avail-able software package (S-Plus release 3.4, MathSoft,Cambridge, Massachusetts).
RESULTSBaseline characteristcs: From 202 patients initially
enrolled in the trial, a total of 181 patients were finallyincluded in the trial and eligible for analysis. Seven-teen patients were excluded from final analysis; due toprotocol violation in 9, withdrawal of the informedconsent in 8, and stent delivery failure in 4. Baselineclinical and angiographic characteristics of the studypatients are summarized in Tables I and II. Of the 181patients, 94 (52%) were randomly assigned to group Aand 87 (48%) to group B. There were no statisticaldifferences between groups A and B for all baselineclinical and angiographic variables analyzed.
Immediate results: A total of 200 stents were placedin 181 patients (1.1 stent/patient). The balloon:arteryratio (ratio of maximal balloon diameter and referencevessel diameter as determined by QCA analysis) wassimilar in both groups (1.16 0.2 in group A and 1.160.2 in group B; p5 NS). Mean maximal balloon
inflation pressures were 8.96 2.7 atm in group A and14.66 1.4 atm in group B (p,0.001).
A crossover between treatment groups occurred in7 patients in group A and in 6 patients in group B.Reasons for the crossover from group A to B wereinsufficient stent results despite postdilations with lowpressures requiring further balloon inflations at highpressures. In 6 patients initally randomized to groupB, high-pressure postdilation was not performed be-cause of a potential procedural risk of recrossing thestented lesion with a further balloon for high-pressurepostdilation. In 2 patients in group B, the balloon burstafter Wiktor stent implantation at high pressure, whichwas not observed in patients in group A. The early(acute and subacute) clinical outcome is shown inTable III. Acute stent thrombosis occurred in 1 patientin group A and in 1 patient in group B. These patientshad a nonfatal Q-wave myocardial infarction and un-derwent repeat angioplasty. One patient in group A
TABLE I Baseline Clinical Characteristics of Study Patients
Group A(n 5 94)
Group B(n 5 87)
All Patients(n 5 181)
No. of randomized 94 87 181Age (yr) 61 6 10 59 6 11 60 6 11Male gender 69 (73%) 70 (80%) 139 (77%)Ejection fraction (%) 60 6 14 60 6 14 60 6 14Diabetes mellitus 20 (21%) 14 (16%) 34 (19%)Hypertension 47 (50%) 39 (45%) 86 (48%)Hypercholesterolemia 47 (50%) 50 (57%) 97 (54%)Smoking 35 (37%) 42 (48%) 77 (43%)Recent myocardial infarction 16 (17%) 11 (13%) 27 (15%)Stable angina 54 (57%) 45 (52%) 99 (55%)Unstable angina 40 (43%) 42 (48%) 82 (45%)1-vessel disease 44 (47%) 53 (61%) 97 (54%)2-vessel disease 39 (41%) 28 (32%) 67 (37%)3-vessel disease 11 (12%) 6 (7%) 17 (9%)Indications for stent
Elective 30 (32%) 30 (34%) 60 (33%)Suboptimal angioplasty result 57 (61%) 55 (63%) 112 (62%)Bailout 7 (7%) 2 (3%) 9 (5%)
TABLE II Baseline Angiographic Characteristics of StudyPatients
Group A(n 5 94)
Group B(n 5 87)
All Lesions(n 5 181)
Coronary artery size (mm) 3.0 6 0.6 3.1 6 0.6 3.1 6 0.6Minimal lumen diameter 1.1 6 0.5 1.2 6 0.5 1.1 6 0.5
before procedure (mm)Diameter stenosis (%) 62 6 15 64 6 16 63 6 16Coronary artery stented
Left anterior descending 34 (36%) 23 (26%) 57 (31%)Left circumflex 16 (17%) 18 (21%) 34 (19%)Right 44 (47%) 43 (50%) 87 (48%)Saphenous vein graft 0 3 (3%) 3 (2%)
Target lesionDe novo 73 (78%) 69 (77%) 142 (78%)Restenotic 21 (22%) 18 (23%) 39 (22%)
Calcium 33 (25%) 32 (37%) 65 (36%)Dissection 48 (51%) 27 (31%) 75 (41%)Lesion type
A 32 (34%) 30 (34%) 62 (34%)B 51 (54%) 40 (46%) 91 (50%)C 11 (12%) 17 (20%) 28 (15%)
646 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 SEPTEMBER 15, 1999

experienced a nonfatal Q-wave myocardial infarctiondue to subacute stent thrombosis and was subse-quently referred to coronary artery bypass surgery.
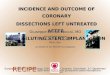
The QCA results are summarized in Table IV. Nosignificant differences were found between groups Aand B for all final QCA measurements after the pro-cedure. A trend toward a larger mean lumen diameterwithin the stent was found for group B (p5 0.08). Ingroup B, the MLD increased from 1.26 0.5 mm atbaseline to 2.76 0.6 mm immediately after stentinsertion at low pressures (p,0.01), which wasslightly but not significantly lower than the MLD ingroup A. After high-pressure postdilatation there wasa further increase in MLD to 2.96 0.5 mm (differencebetween means, 0.24 mm, 95% CI 0.16 to 0.32, p,0.05). The cumulative frequency distributions ofMLD for groups A and B are depicted in Figure 1. Thedistribution curves were essentially identical for bothgroups at baseline. After stent implantation, however,a significant larger MLD was found in group B fordistribution ranges below the 30% quartile. (p50.0116).
In 31 patients (17% of total study cohort; 14 and 17patients in groups A and B, respectively), IVUS ex-amination was performed after diagnostic coronaryangiography and stent implantation. There were nodifferences in baseline lumen cross-sectional areasbetween groups A and B (4.66 1.9 and 4.36 1.4mm2 for groups A and B, respectively; differencebetween means, 0.36 mm2, 95% CI 21.56 to 0.84).After stent implantation, the final lumen cross-sec-tional area, expressed both as an absolute value and asa percentage of the reference cross-sectional area, wasslightly larger in group B. These differences, however,were not significant: 6.76 1.4 mm2 (70 6 24%) ingroup A versus 7.46 1.5 mm2 (79 6 11%) in groupB, difference between means 0.72 mm2 (9.4%), 95%CI 20.34 to 1.78 mm2 (23.9% to 22.7%). Similar tothe findings from the QCA analysis, comparison of thecross-sectional areas before and after high-pressurepostdilation within group B revealed a significantlarger lumen cross-sectional area after high-pressurepostdilation. The lumen cross-sectional area had in-creased from 6.16 1.2 mm2 before to 7.46 1.5 mm2
after high-pressure postdilation (difference betweenmeans 1.28 mm2, 95% CI 1.09 to 1.47, p5 0.048),
and when expressed as a percentage of the reference,from 68 6 8% to 79 6 11% (difference betweenmeans 11%, 95% CI 9.2 to 12.8, p5 0.019).
Long-term results: Long-term clinical follow-up wasachieved in all eligible patients, and follow-up angiog-raphy was performed in 154 patients (85%; 76 and 78patients in groups A and B, respectively) at an intervalof 7 6 3 months after Wiktor stent implantation forboth groups.
Angiographic and clinical follow-up results arelisted in Tables IV and V. The follow-up QCA anal-ysis revealed an MLD of 2.16 0.8 mm and a percentdiameter stenosis of 316 21% for the total studypopulation, with no significant differences betweenthe 2 groups. In addition, the cumulative distributioncurves of MLD, which was shifted to the right ingroup B immediately after stent implantation, renar-rowed at follow-up, thus revealing no between-groupdifference (Figure 1). Late lumen loss, loss index, andnet lumen gain were not significantly different be-tween groups A and B. Target lesion restenosis, aspreviously described, was present in a total of 28patients (14 patients in each group, 15%).
There was 1 sudden death in group A at 1 monthafter stent implantation. No coronary bypass surgeryand no acute myocardial infarctions were recorded ineither group during the follow-up period. Repeat an-gioplasty of the stented vessel segment was performedin 13 and 12 patients (both 14%) in groups A and B,respectively, driven by clinical signs of ischemiaand/or angiographic evidence of restenosis as assessedvisually by each operator-investigator. The overallincidence of major adverse cardiac events at follow-upwas 14%, with no difference between the 2 groups(Table V).
DISCUSSIONThe present study is the first to investigate in a
prospective, randomized fashion the short- and long-term benefit of high-pressure implantation of a single-wire coil stent compared with the conventional low-pressure approach. Our results demonstrate favorableclinical and angiographic outcomes with the Wiktorstent, revealing a low incidence of adverse events andtarget lesion restenosis, with no differrences betweenthe low- and high-pressure randomized groups.
Immediate clinical and angiographic results: The in-cidence of acute or subacute stent thrombosis (2%),with no difference between groups, in the present trialwas comparable to results from other tubular or coilstents15,16 and remarkably lower than those observedin previous published studies of the Wiktor stent forbailout procedures or restenotic lesions.17,18This maybe attributed to refinements and improvements overthe past few years in poststent medical treatment, andprocedural technique and equipment in addition toother factors such as multiple stenting, different stentindications, or patient profile.
Recent observations suggest that a more completestent expansion with the use of high-pressure balloonsshould lead to improved strut/vessel contact evenwithout IVUS guidance.2,3 This technique seems to
TABLE III Early Clinical Outcome
Group A(n 5 94)
Group B(n 5 87)
All Patients(n 5 181)
Acute stent thrombosis 1 (1%) 1 (1%) 2 (1%)Subacute stent thrombosis 1 (1%) 0 1 (1%)Major adverse cardiac events 2 (2%) 1 (1%) 3 (2%)
Death 0 0 0Acute myocardial infarction 2 (2%) 1 (1%) 3 (2%)Coronary bypass surgery 0 0 0Repeat coronary angioplasty 0 0 0
CORONARY ARTERY DISEASE/LOW– VS HIGH–PRESSURE WIKTOR STENT IMPLANTATION 647

confer a greatly reduced rate of stent thrombosis, whichmay eliminate the need for systemic anticoagulation andits complications. We have found that the final lumendimensions as measured by both QCA and IVUS did notdiffer significantly between the high- and low-pressuregroups immediately after stent implantation. Although atrend toward a greater lumen gain could be observed forfinal MLD and mean lumen diameter in the high-pres-sure group than in the low-pressure group, neitherreached the level of statistical significance. However, a
certain benefit of high-pressure postdilata-tion on immediateoutcome can be dem-onstrated by analysis of the frequencydistribution functions for MLD (Figure1), which illustrates an improvement inthe immediate angiographic result byhigh-pressure application in patientswith a relatively small postinterventionMLD (,2.7 mm). Furthermore, MLDsand areas, as measured by QCA andIVUS, respectively, were slightlysmaller in the high-pressure group im-mediately after stent insertion at lowpressures, but improved significantlyafter high-pressure postdilatation.
Long-term outcome: Several investiga-tors have highlighted a potential draw-back of high-pressure stenting based onconcerns that high-pressure balloon infla-tion may increase vessel wall injury andreactive neointimal formation, eventuallyleading to a higher late lumen loss.7–9,19
A recently published unicenter retrospec-tive analysis comparing “aggressive”stent deployment techniques using over-sized balloons (.1.15 balloon/artery ra-tio) or high-inflation pressures ($12 atm)with “nonaggressive” stent implantation
strategies has revealed no increase in late lumen lossor restenosis after aggressive stent implantation.20
Consistent with this finding, our results show no sig-nificant differences in late outcome between the 2randomized groups. No statistical differences in fol-low-up MLD could be detected between the low- andhigh-pressure groups at follow-up, not only with re-spect to absolute diameters or percent diameter steno-sis, but also with regard to the frequency distributionof the follow-up MLD (Figure 1). The overall target
FIGURE 1. Cumulative frequency distribution of MLD at baseline (Pre), after stentimplantation (Post), and at follow-up (Fup) for groups A and B. There was nodifference in baseline distribution between the 2 groups, but after stent implan-tation, the curve for group B is shifted to the right, particularly in ranges belowthe 30% quartile (p 5 0.0116). At 6-month follow-up, the difference nar-rowed below the significance level.
TABLE IV Quantitative Angiographic Results
Group A(n 5 94)
Group B(n 5 87)
Difference BetweenGroups (mean [95% CI])
All Lesions(n 5 181)
Minimal lumen diameter (mm)Baseline 1.1 6 0.5 1.2 6 0.5 0.01 [20.14 to 0.16] 1.1 6 0.5After stent implantation 2.8 6 0.5 2.9 6 0.5 0.11 [20.03 to 0.25] 2.9 6 0.5Follow-up* 2.1 6 0.7 2.2 6 0.8 0.05 [20.18 to 0.28] 2.1 6 0.8
Mean lumen diameter (mm)Baseline 1.9 6 0.5 2.02 6 0.5 0.10 [20.05 to 0.25] 2.0 6 0.5After stent implantation 3.3 6 0.6 3.5 6 0.5 0.14 [20.01 to 0.29] 3.4 6 0.5Follow-up 2.7 6 0.7 2.8 6 0.7 0.03 [20.17 to 0.23] 2.8 6 0.7
Reference diameter (mm)Baseline 3.0 6 0.6 3.1 6 0.6 0.06 [20.11 to 0.23] 3.1 6 0.6After stent implantation 3.4 6 0.6 3.5 6 0.5 0.10 [20.06 to 0.26] 3.4 6 0.5Follow-up 3.0 6 0.7 3.1 6 0.6 0.04 [20.16 to 0.24] 3.1 6 0.7
Percent diameter stenosis (%)Baseline 62 6 15 63 6 16 0.7 [23.9 to 5.3] 63 6 16After stent implantation 17 6 8 16 6 9 20.8 [23.3 to 1.7] 17 6 8Follow-up 31 6 17 30 6 24 20.7 [26.8 to 5.4] 31 6 21
Acute lumen gain (mm) 1.7 6 0.6 1.8 6 0.5 0.10 [20.07 to 0.27] 1.7 6 0.6Late lumen loss (mm) 0.7 6 0.6 0.8 6 0.8 0.07 [20.14 to 0.28] 0.7 6 0.7Net lumen gain (mm) 1.0 6 0.7 1.0 6 0.8 0.05 [20.18 to 0.28] 1.0 6 0.7Loss index 0.4 6 0.4 0.4 6 0.4 0.02 [20.10 to 0.14] 0.4 6 0.5
*Number of patients with angiographic follow-up was 76 (81%) in group A, 78 (90%) in group B, and 154 (85%) in total.
648 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 SEPTEMBER 15, 1999

lesion restenosis and reintervention rates (15% and14%, respectively) in our study compare favorablywith those reported in previous follow-up studies ofWiktor stents.17,18,21 A similar restenosis rate wasfound in a recently published multicenter study of theWiktor stent in chronic total coronary occlusions,when patients with multiple stents (45% of total studypopulation) were disregarded.22 This finding, in con-junction with the encouraging follow-up results of thepresent trial, may testify to the long-term effectivenessof Wiktor stent implantation even in non–“Benestent-like” lesions.
Acknowledgment: We are grateful to Klaus Felsen-stein, PhD, Institute of Statistics, Technical Universityof Vienna, Austria, for statistical advise and criticalreview of the manuscript.
1. Colombo A, Hall P, Nakamura S, Almagor Y, Maiello L, Martini G, GanglioneA, Goldberg SL, Tobis JM. Intracoronary stenting without anticoagulation ac-complished with intravascular ultrasound guidance.Circulation 1995;91:1676–1688.2. Sankardas MA, McEniery PT, Aroney CA, Bett JHN. Elective implantation ofintracoronary stents without intravascular ultrasound guidance or subsequentwarfarin.Cathet Cardiovasc Diagn1996;37:355–359.3. Nakamura S, Hall P, Gaglione A, Tiecco F, Di Maggio M, Maiello L, MartiniG, Colombo A. High pressure assissted coronary stent implantation accomplishedwithout intravascular ultrasound guidance and subsequent anticoagulation. J AmColl Cardiol 1997;29:21–27.
4. Von Birgelen C, Gil R, Ruygrok P, Prati F, Di Mario C, Van der Giessen WJ,De Feyter PJ, Serruys PW. Optimized expansion of the Wallstent compared withthe Palmaz-Schatz stent: on-line observations with two- and three-dimensionalintracoronary ultrasound after angiographic guidance.Am Heart J 1996;131:1067–1075.5. Gorge G, Haude M, Ge J, Voegele E, Gerber T, Rupprecht HJ, Meyer J, ErbelR. Intravascular ultrasound after low and high inflation pressure coronary arterystent implantation.J Am Coll Cardiol1995 26:725–730.6. Goods CM, Al-Shaibi KF, Yadav SS, Liu MW, Negus BH, Iyer SS, Dean LS,Jain SP, Baxley WA, Parks JM, Sutor RJ, Roubin GS. Utilization of the coronaryballoon-expandable coil stent without anticoagulation or intravascular ultrasound.Circulation 1996;92:1803–1808.7. Savage MP, Fishman DL, Douglas JS Jr, Pepine CJ, Werner JA, Bailey SR,Rake R, Goldberg S. The dark side of high pressure stent deployment (abstr).J Am Coll Cardiol1997;29(suppl A):368A.8. Fernandez-Aviles F, Alonso JJ, Duran JM, Gimeno F, Garcia-Moran E,Paniagua J, Garcimartin I, Mun˜oz JC. High pressure increases late loss aftercoronary stenting (abstr).J Am Coll Cardiol1997;29(suppl A):369A.9. Hoffmann R, Mintz GS, Mehran R, Kent KM, Pichard AD, Satler LF, PopmaJJ, Bucher TA, Leon MB. Late tissue proliferation both within and surroundingPalmaz-Schatz stent is associated with procedural vessel wall injury (abstr).J AmColl Cardiol 1997;29(suppl A):397A.10. Ellis SG, Vandermael MG, Cowley MJ, Di Sciascio G, Deligonul U, TopolEJ, Bulle TM. Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease: implications forpatient selection.Circulation 1990;82:1193–1202.11. Reiber JHC, van der Zwet PMJ, von Land CD, Koning G, van Meurs B, BuisB, van Voorthuisen AE. An overview of coronary quantification techniques as of1989. In: Reiber JHC, Serruys PW, eds. Quantitative Coronary Arteriography.Dortrecht: Kluwer Academic, 1991:55–132.12. Reiber JHC, van der Zwet PMJ, von Land CD, Koning G, van Meurs B, BuisB, van Voorthuisen AE. Quantitative coronary arteriography: equipment andtechnical requirements. In: Reiber JHC, Serruys PW, eds. Advances in Quanti-tative Coronary Arteriography. Dortrecht: Kluwer Academic, 1992:75–111.13. Gardner MJ, Altman DG. Confidence intervals rather than P values: estima-tion rather than hypothesis testing.Br Med J1986;292:746–750.14. Bulpitt CJ. Confidence intervals.Lancet1987;1:494–497.15. Moussa I, Di Mario C, Di Francesco L, Reimers B, Blengio S, Colombo A.Subacute stent thrombosis and the anticoagulation controversy: changes in drugtherapy, operator technique, and the impact of intravascular ultrasound.Am JCardiol 1996;78:13–17.16. Kimura T, Yokoi H, Nakagawa Y, Tamura T, Kaburagi S, Sawada Y, SatoY, Yokoi H, Hamasaki N, Nosaka H, Nobuyoshi M. Three-year follow-up afterimplantation of metallic coronary-artery stents.N Engl J Med1996;334:561–566.17. Vrolix M, Piessens J. Usefulness of the Wiktor stent for treatment ofthreatened or acute closure complicating coronary angioplasty. The EuropeanWiktor Stent Study Group.Am J Cardiol1994;73:737–741.18. De Jaegere PP, Serruys PW, Bertrand M, Wiegand V, Kober G, Marquis JF,Valeix B, Uebis R, Piessens J. Wiktor stent implantation in patients with reste-nosis following balloon angioplasty of a native coronary artery.Am J Cardiol1992;69:598–602.19. Mintz GS, Hoffmann R, Mehran R, Pichard AD, Kent KM, Satler LF, PopmaJJ, Leon MB. In-stent restenosis: the Washington Hospital Center Experience.Am J Cardiol1998;81(7A):7E–13E.20. Goldberg SL, Di Mario C, Hall P, Colombo A. Comparison of aggressiveversus nonaggressive balloon dilatation for stent deployment on late loss andrestenosis in native coronary arteries.Am J Cardiol1998;81:708–712.21. Eeckhout E, Goy JJ, Stauffer JC, Vogt P, Kappenberger L. Comparison of theWallstent, Palmaz-Schatz stent and Wiktor stent late after intracoronary stenting.Am J Cardiol1994;74:609–612.22. Anzuni A, Rosanio S, Legrand V, Tocchi M, Coppi R, Bonnier H, SheibanI, Kulbertus HE, Chierchia SL. Wiktor stent for treatment of chronic totalcoronary artery occlusions: short- and long-term clinical and angiographic resultsfrom a large multicenter experience.J Am Coll Cardiol1998;31:281–288.
TABLE V Occurrence of Adverse Cardiac Events andAngiographic Restenosis
Group A(n 5 94)
Group B(n 5 87)
AllPatients
(n 5 181)
Follow-up (mo afterprocedure)*
7 6 3 7 6 3 7 6 3
Target lesion restenosis 14 (15%) 14 (16%) 28 (15%)In-stent restenosis 11 (12%) 9 (10%) 20 (11%)Peristent restenosis 3 (3%) 5 (6%) 8 (4%)
Major adverse cardiacevents
14 (15%) 12 (14%) 26 (14%)
Death 1 (1%) 0 1 (0.6%)Acute myocardialinfarction
0 0 0
Target lesionrevascularization
13 (14%) 12 (14%) 25 (14%)
*Clinical follow-up was achieved in 100% of eligible patients and angio-graphic follow-up was available in 76 patients (81%) in group A, 78 (90%) ingroup B, and 154 (85%) in total.
CORONARY ARTERY DISEASE/LOW– VS HIGH–PRESSURE WIKTOR STENT IMPLANTATION 649