Embed Size (px)
Citation preview

Journal of Sleep Medicine & Disorders
Cite this article: Matsumura Y, Ueda H, Concepción C, Koh M, Tanimoto K (2015) Effect of a Simplified Two-Piece Mandibular Advancement Appliance for Obstructive Sleep Apnea. J Sleep Med Disord 2(3): 1025.
Central
*Corresponding authorHiroshi Ueda, Orthodontic Clinic, Hiroshima University Hospital, 1-2-3 Kasumi, Minami-ku, Hiroshima 734-8553, Japan, Tel: 81-082-257-5686; Fax: 81-082-257-5687; Email:
Submitted: 06 April 2015
Accepted: 20 April 2015
Published: 12 June 2015
Copyright© 2015 Ueda et al.
OPEN ACCESS
Keywords•Obstructive sleep apnea•Oral appliance•Apnea-hypopnea index•Jaw movement•Temporomandibular joint•Masticatory discomfort
Short Communication
Effect of a Simplified Two-Piece Mandibular Advancement Appliance for Obstructive Sleep ApneaYu Matsumura1, Hiroshi Ueda2*, Cynthia Concepción1, Myongsun Koh2 and Kotaro Tanimoto1
1Department of Orthodontics and Craniofacial Developmental Biology, Hiroshima University, Hiroshima, Japan2Orthodontic Clinic, Hiroshima University Hospital, Japan
Abstract
Oral appliances (OAs) are available and distributed widely in the field of dentistry to treat mild-to-moderate obstructive apnea. However, several studies found that OAs induced temporomandibular joint (TMJ) discomfort and masticatory muscle stiffness. We developed a new appliance that significant improved the apnea-hypopnea index (AHI) and horizontal jaw movement, which may diminish TMJ and masticatory side effects.
ABBREVIATIONSOA: Oral Appliance; TMJ: Temporomandibular Joint; AHI:
Apnea-Hypopnea Index; PSG: Polysomnography
INTRODUCTIONOral appliance (OA) therapy aims to enlarge the upper airway
by forward mandibular repositioning to treat mild-to-moderate obstructive sleep apnea (OSA). Long-term use of OAs can cause temporomandibular joint (TMJ) discomfort and masticatory side effects, which have been described in several studies [1-3]. We developed a new appliance that allows significant jaw movement, thereby diminishing TMJ and masticatory side effects. The aim of this study was to evaluate the improvement of mild-to-moderate OSA using a simplified two-piece mandibular advancement appliance.
MATERIALS AND METHODSPatients and methods
Nineteen consecutive patients (14 males and 5 females; mean age: 53.3±14.3 years) referred to the Dental Clinic of Hiroshima University Hospital from the sleep laboratory in 2012 and 2013 for moderate OSA were selected for this study. All patients were requested to complete a written informed consent form for participating in the study. The institutional ethics committee approved the study design, which adhered to the tenets of the amended Declaration of Helsinki.
A full-night diagnostic polysomnography (PSG) was conducted for every patient. The mean apnea-hypopnea index (AHI) was 14.4±2.6. Cephalometric analysis was used to determine the mandibular advancement. A follow-up PSG was done for every patient, and questionnaires were used to obtain information on TMJ side effects and dentition after training the patients to use the OA (mean: 4.4±2.4 months).
Appliance design
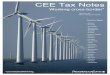
The appliance consisted of two occlusal splints held together by an orthodontic wire (Figures 1a,b,c). The splints were constructed using a 0.75mm thick acrylic resin that provides full occlusal coverage of the teeth. A 0.0215” multi-stranded, twisted wire was attached on the buccal sides of the lower splint. Patients could easily connect the lower splint with the hook attached on the front portion of the upper splint. The initial mandibular advancement was defined as the edge to edge bite position with a
Figure 1a Mandibular position shifted to the right with OA.

Ueda et al. (2015)Email:
J Sleep Med Disord 2(3): 1025 (2015) 2/2
Central
3-4 mm vertical opening at the anterior of the teeth. This appliance permitted patients to freely move their jaws horizontally (approximately 10 mm laterally), while simultaneously preventing downward movement of the mandible within 2 mm in the supine position by means of an opt electric jaw-tracking system with six degrees of freedom (Gnathohexagraph system II, Onosokki Co., Yokohama, Japan) (Table 1).
The mandibular position could also be titrated forward from
its initial position by adjusting the wire length on the appliance.]
RESULTS AND DISCUSSIONThe mean body mass index (BMI) was 21.3±2.2 in OSA
patients. AHI was significantly improved in most patients (mean: 6.1±2.4, P<0.05). The mean amount of mandibular advancement was 3.4±2.7 mm (Table 2). Temporary TMJ and masticatory muscle side effects were not observed.
The AHI was significantly improved using the new appliance, although the mean AHI was greater than 5.0. No complaints of TMJ pain or myofascial discomfort were observed. We speculated that the lower degree of mandibular advancement could make these side effects negligible [4-7].
CONCLUSIONThe developed appliance is efficient, inexpensive, hard
to break, and gentle on intra- and extra-oral tissues. The materials used for the appliance are easy to obtain, and the fabrication is extremely simple. This appliance permits lateral, but not backward, mandible movement. Thus, undesirable side effects, such as TMJ disorders and masticatory dysfunction, are decreased.
ACKNOWLEDGEMENTSThis study was supported in part by a Grant-in-Aid for
Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan (245930940).
REFERENCES1. Pantin CC, Hillman DR, Tennant M. Dental side effects of an oral device
to treat snoring and obstructive sleep apnea. Sleep. 1999; 22: 237-240.
2. Bloch KE, Iseli A, Zhang JN, Xie X, Kaplan V, Stoeckli PW, et al. A randomized, controlled crossover trial of two oral appliances for sleep apnea treatment. Am J Respir Crit Care Med. 2000; 162: 246-251.
3. Fritsch KM, Iseli A, Russi EW, Bloch KE. Side effects of mandibular advancement devices for sleep apnea treatment. Am J Respir Crit Care Med. 2001; 164: 813-818.
4. Lowe AA, Fleetham JA, Adachi S, Ryan CF. Cephalometric and computed tomographic predictors of obstructive sleep apnea severity. Am J Orthod Dentofacial Orthop. 1995; 107: 589-595.
5. Robertson C, Herbison P, Harkness M. Dental and occlusal changes during mandibular advancement splint therapy in sleep disordered patients. Eur J Orthod. 2003; 25: 371-376.
6. Fransson AM, Tegelberg A, Johansson A, Wenneberg B. Influence on the masticatory system in treatment of obstructive sleep apnea and snoring with a mandibular protruding device: a 2-year follow-up. Am J Orthod Dentofacial Orthop. 2004; 126: 687-693.
7. Otsuka R, Almeida FR, Lowe AA. The effects of oral appliance therapy on occlusal function in patients with obstructive sleep apnea: a short-term prospective study. Am J Orthod Dentofacial Orthop. 2007; 131: 176-183.
Matsumura Y, Ueda H, Concepción C, Koh M, Tanimoto K (2015) Effect of a Simplified Two-Piece Mandibular Advancement Appliance for Obstructive Sleep Apnea. J Sleep Med Disord 2(3): 1025.
Cite this article
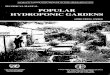
Figure 1b Mandibular rest position with OA.
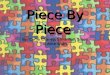
Figure 1c Mandibular position shifted to the left with OA.
Table 1: The distance of mandibular movement with OA during maximum voluntary effort.
Jaw movement mm
right-left direction shift to the rightshift to the left
11.9±1.9911.4±1.82
antero-posterior direction
maximum jaw openinglateral jaw movement
1.63±0.950.770.25
(N = 5)
Table 2: Demographic data of patients.
Mean ±SD
Mean age (years) 53.3±14.3
Mean BMI 21.3±2.2
Baseline AHI 14.4±2.6
AHI after OA therapy 6.1±2.4
Mandibular advancement (mm) 3.4±2.7