Embed Size (px)
Citation preview

Central Annals of Otolaryngology and Rhinology
Cite this article: Gill KS, Rabinowitz M, Hsu D, Evans J, Farrell C, et al. (2016) Strategies to Protect the Cranial Base in Endoscopic Skull Base Surgery. Ann Otolaryngol Rhinol 3(11): 1140.
*Corresponding author
Marc Rosen, Department of Otolaryngology-Head & Neck Surgery, Thomas Jefferson University, 925 Chestnut St 6th floor, Philadelphia, PA, USA, Tel: 2159556760, Fax: 215503-3736 Email:
Submitted: 09 September 2016
Accepted: 10 October 2016
Published: 12 October 2016
ISSN: 2379-948X
Copyright© 2016 Rosen et al.
OPEN ACCESS
Keywords• Cranial base• Skull base• Nasogastric• Endoscopic• Inadvertent• Cranial base protection
Short Communication
Strategies to Protect the Cranial Base in Endoscopic Skull Base SurgeryKurren S Gill1, Mindy Rabinowitz1, David Hsu1, James Evans1,2, Christopher Farrell2, Gurston Nyquist1,2, and Marc Rosen1,2*1Department of Otolaryngology-Head & Neck Surgery, Thomas Jefferson University, USA2Department of Neurologic Surgery, Thomas Jefferson University, USA
Abstract
Introduction: Large cranial base defects after transsphenoidal surgery exposes the brain to iatrogenic injury via insertion of endonasal tubes. It has been reported in the literature that nasogastric tubes have inadvertently been placed into the brainstem or spinal cord postoperatively. This can have devastating ramifications including neurologic sequelae or fatality. For these reasons, it is prudent to implement surgical techniques to help protect the cranial base against iatrogenic injury after endoscopic, endonasal skull base surgery.
Methods: We performed a Pub Med literature review of cases of inadvertent intracranial placement of a NGT. We categorized the causes as traumatic, non-traumatic, and surgical, and identified trends to assess potential risk factors. Articles not in English were excluded from our review.
Results: We identified 37 articles describing 41 instances of a misguided NGT intracranially. Twenty-seven cases (65.8%) were in the setting of trauma, 7 (17%) in non-traumatic settings, and 7 (17%) after surgery. Sixteen of forty-one (39%) died of various causes and 5 (31.3%) were directly attributable to intracranial insertion of the NGT.
Discussion: We describe several techniques to protect the cranial base including middle turbinate preservation and medialization, limited posterior nasal septectomy and trans-septal approaches. In addition, we provide a video illustrating the how the cranial base is protected using these methods.
Conclusion: Operative techniques in endoscopic transsphenoidal skull base surgery that facilitate closure of the sphenoid sinus likely decrease the risk of postoperative iatrogenic injury via inadvertent placement of endonasal tubes.
ABBREVIATIONSNGT: Naso Gastric Tube
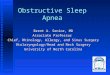
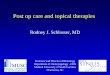
INTRODUCTIONAlthough relatively uncommon, inadvertent instrumentation
of nasogastric tubes into the brain stem (Figure 1) or spinal cord (Figure 2) is a recognized post-operative complication of endonasal skull base surgery or acute head trauma. This can lead to devastating consequences such as hemiplegia, meningitis, and intracranial hemorrhage (ICH) [1]. According to Fletcher et al., this misplacement is lethal in 64% of cases [2]. Sites of entry of a NGT into the cranial vault include: a comminuted fracture of the
basilar skull or floor of the anterior cranial fossa providing entry from the nasopharynx, and disruption or fracture of the cribriform plate or an unusually thin cribriform plate, which is especially at risk when a transversely oriented rigid NGT is improperly advanced [3,4]. For this reason, relative contraindications to NGT insertion include CSF rhinorrhea in association with head or maxillofacial trauma and failure of an NGT to pass freely and easily [4]. To avoid these potential complications, it is prudent to confirm the placement of a NGT by anteroposterior and lateral radiographs of the skull rather than by aspiration of gastric contents or auscultation of air injected through the tube [4,5]. Alternatively, confirmation via water-soluble contrast is another option in adults. It is recommended that patients with craniofacial

Central
Rosen et al. (2016)Email:
Ann Otolaryngol Rhinol 3(11): 1140 (2016) 2/4
injury should instead undergo placement via the oral route with direct visualization [3].
Endoscopic skull base surgery, in particular, creates a potential direct pathway to to the intracranial compartment from the nostrils. This increases the likelihood of intracranial NGT placement. The majority of the literature reporting these instances is in the form of individual case reports. There have been 3 instances reported in the literature of this complication occurring after endoscopic transsphenoidal surgery and 1 case after endoscopic transnasal resection of a clival chordoma [6]. Three of these patients died [6-9] and one survived with severe thalamic and cortical injuries [10].
METHODS We performed a Pub Med literature review of cases of
inadvertent intracranial placement of a NGT. We categorized the causes as traumatic, non-traumatic, and surgical, and identified trends to assess potential risk factors. Articles not in English were excluded from our review.
RESULTS We identified 37 articles describing 41 instances of a
misguided NGT intracranially. Twenty-seven cases (65.8%) were in the setting of trauma, 7 (17%) in non-traumatic settings, and 7 (17%) after surgery (Table 1). Surgeries included endoscopic transsphenoidal resection of pituitary tumors (3), endoscopic transnasal transclival resection of a clival chordoma
(1), craniotomy for pituitary adenoma (1), craniotomy for intracranial hemorrhage (1), and repair of choanal atresia (1). Non-traumatic cases included: a patient with thin cribriform plate, status epilepticus and congenital defect (possibly nasal glioma), treacher-collins syndrome, routine nasal intubation of premature infant, premature infant with ARDS, Goldenhar syndrome with cribriform plate agenesis, and healthy patient who volunteered for a study on bile secretions.
Sixteen of forty-one (39%) died of various causes including intracranial hemorrhage, bronchopneumonia, or head injuries they presented with upon admission. Five of these deaths (31.3%) were directly attributable to intracranial insertion of the NGT. The most common insertion point was via the cribriform plate (19 cases, 46%), with the second most common being the sphenoid sinus (6 cases, 14.6%).
DISCUSSION
Operative techniques to protect the cranial base
Herein we describe operative techniques that serve to protect the cranial base after transsphenoidal surgery. In all instances, a wide bony sphenoidotomy is created, and just the mucosa on one or both sides may be limited. One method to protect the cranial base is by creating conservative sphenoidotomies (1.5 approaches, (Figure 3). For example, a right-sided wide sphenoidotomy is performed along with a small contralateral sphenoidotomy. A limited posterior septectomy of <2 cm is created. Once healed, the opening to the sphenoid sinus is very narrow. In our experience, not only does a smaller posterior septectomy serve to protect the cranial base, but it also has the additional advantage of decreasing post-operative sinonasal morbidity [11]. This protective feature of a limited posterior septectomy should not outweigh the need for exposure, especially in larger tumors or based on patient’s anatomy. Adequate exposure should always be maintained even if it results in a larger posterior septectomy.
A septoplasty with a sub mucosal “tunnel” approach can be utilized to correct septal deviations. On the side of the spur or deviation, a hemi-transfixion incision is made and the surgeon works inside the submucosal septal tunnel to create a sphenoidotomy (in a submucosal fashion) and access the
Figure 1 CT scan showing inadvertent instrumentation of a nasogastric tube into the intracranial cavity.
Figure 2 MRI showing a nasogastric tube tracking down the spine.
Figure 3 1.5 approach: a right sided wide sphenoidotomy is performed along with a small contralateral sphenoidotomy.

Central
Rosen et al. (2016)Email:
Ann Otolaryngol Rhinol 3(11): 1140 (2016) 3/4
Figure 4 A septoplasty with a submucosal “tunnel” approach.
Figure 5 Medical alert bracelet indicating previous skullbase surgery and current cranial base defect.
Table 1: List of cases of inadvertent intracranial nasogastric tube insertion in a PUBMED literature reviewReference Setting Outcome/ComplicationsAdler Trauma DeathArslantas Trauma Discharged in good healthPsarras Trauma Full recoveryGalloway Trauma DeathVeeravagu Trauma Good neurologic recoveryGenu Trauma Discharged with right hemiplegiaFerreras Trauma No complications
Hande Post-Op (trans-sphenoidal) Died of bronchopnuemonia
Glasser Non-trauma Not stated (patient unresponsive upon removal of NGT)
Hanna Post-Op Death due to NGTPandey Trauma Died of head injuriesMetheny Post-Op Thalamic and cortical injuriesNathoo Post-Op SurvivedRahimi-Moghavar Trauma Death
Guerra Post-Op (trans-sphenoidal) Death
Castiglione Trauma Death due to NGTFremstad Trauma Death due to NGTSacks Trauma Not StatedWyler Trauma DeathSeebacher Trauma Death
Cornett Trauma Discharged with L hemiparesis, cognitive/linguistic impairment
Borovich (2 pts) Trauma One death; one full recoveryGustavsson Trauma Survived with visual field defectFletcher (2 pts) Trauma Acceptable recoveryGregory Trauma Survived
Freij Non-Trauma Death due to meningitis and bronchopneumonia
Paul Post-Op (trans-sphenoidal) Died from ICH due to NGT
Muzumdar Non-Trauma Good neurologic recoveryCameron Non-Trauma SurvivedPawar Trauma DeathAraimo Post-Op No complicationsKoch Trauma Not statedMoustoukas Trauma Died of head injuriesvan den Anker Non-Trauma No complicationsAllen Non-Trauma Not statedYoung Non-Trauma CSF rhinorrhea surgically correctedKatz Trauma Death due to NGTAbbreviations: NGT: Nasogastric Tube; ICH: Intracranial Hemorrhage; CSF: Cerebrospinal Fluid
skull base. Thus, the sphenoid sinus ostium on the side of the hemi-transfixion incision is not widened and the skull base is not exposed (Figure 4). This helps to protect the skull base because the majority of the mucosa overlying the sphenoid face is preserved, thereby closing off the large bony sphenoidotomy.
Another method involves preserving the middle turbinates. Complete ethmoidectomies are not performed but rather limited posterior ethmoidectomies are utilized when needed for access. The middle turbinates are medialized at the end of the procedure (Video 1). This serves to protect access to the sphenoid by a NGT because it closes off the sphenoidotomy, allowing the NGT to preferentially pass into the nasopharynx. While some may advocate for routine middle turbinate sacrifice in endoscopic sinus surgery, preserving the middle turbinate, as we do here, also decreases risk of cerebrospinal fluid leak, maintains the basal lamella as a surgical landmark for further endonasal navigation, and decreases scarring, among other advantages [12]. A prospective observational study by Nyquist et al. found that middle turbinate preservation in endoscopic endonasal transsphenoidal surgery can still provide adequate exposure for successful tumor resection and skull base reconstruction while preserving postoperative sinonasal function [13]. Additionally, a recent retrospective cohort study by Sowerby et al. compared
patients who underwent middle turbinate sacrifice and middle turbinate sparing endonasal approaches to the sella and found no effect on postoperative radiographic frontal sinusitis [14]. These studies advocate routine middle turbinate preservation and suggest no advantages to routine middle turbinate sacrifice in endoscopic endonasal transsphenoidal surgery.
In contrast to routinely removing bone over the carotid artery and optic nerves, we maintain these protective bony structures.

Central
Rosen et al. (2016)Email:
Ann Otolaryngol Rhinol 3(11): 1140 (2016) 4/4
Gill KS, Rabinowitz M, Hsu D, Evans J, Farrell C, et al. (2016) Strategies to Protect the Cranial Base in Endoscopic Skull Base Surgery. Ann Otolaryngol Rhinol 3(11): 1140.
Cite this article
Routine bony removal exposing critical structures along the cranial base is avoided and exposure is based on the access required for each individual case. These surgical techniques also allow for preservation of bilateral nasal septal flaps, which is also an advantage of these techniques.
Additionally, we ensure patients are adequately informed of their risk for a cranial base defect after their surgery, and some have found wearing medical alert bracelets (Figure 5) detailing their special circumstances to be extremely helpful in relaying this potentially life-saving information to other medical providers in emergency settings.
CONCLUSIONInadvertent intracranial placement of NGTs after endoscopic
skull surgery is a recognized and potentially lethal complication. Intra-operative techniques can be employed to prevent incorrect NGT instrumentation and ensuing life-threatening neurologic sequelae. We describe techniques including middle turbinate preservation and medialization, a limited posterior nasal septectomy, and transseptal approaches to help fortify the cranial base after transsphenoidal surgery.
REFERENCES1. Genú PR, de Oliveira DM, Vasconcellos RJ, Nogueira RV, Vasconcelos
BC. Inadvertent intracranial placement of a nasogastric tube in a patient with severe craniofacial trauma: a case report. J Oral Maxillofac Surg. 2004; 62: 1435-1438.
2. Fletcher SA, Henderson LT, Miner ME, Jones JM. The successful surgical removal of intracranial nasogastric tubes. J Trauma. 1987; 27: 948-952.
3. Katz MI, Faibel M. Inadvertent intracranial placement of a nasogastric tube. AJR Am J Roentgenol. 1994; 163: 222.
4. Koch KJ, Becker GJ, Edwards MK, Hoover RL. Intracranial placement of
a nasogastric tube. AJNR Am J Neuroradiol. 1989; 10: 443-444.
5. Fremstad JD, Martin SH. Lethal complication from insertion of nasogastric tube after severe basilar skull fracture. J Trauma. 1978; 18: 820-822.
6. Hanna AS, Grindle CR, Patel AA, Rosen MR, Evans JJ. Inadvertent insertion of nasogastric tube into the brain stem and spinal cord after endoscopic skull base surgery. Am J Otolaryngol. 2012; 33: 178-180.
7. Hande A, Nagpal R. Intracranial malposition of nasogastric tube following transnasal transsphenoidal operation. Br J Neurosurg. 1991; 5: 205-207.
8. Guerra B, Slade TL, Kelly PJ. Intracranial introduction of a nasogastric tube in a patient with a pituitary tumor. Surg Neurol. 1979; 12: 135-136.
9. Patel SG, Singh B, Polluri A, Bridger PG, Cantu G, Cheesman AD, et al. Craniofacial surgery for malignant skull base tumors: report of an international collaborative study. Cancer. 2003; 98: 1179-1187.
10. Metheny NA. Inadvertent intracranial nasogastric tube placement. Am J Nurs. 2002; 102: 25-27.
11. Garcia HG, Marc Otten, Marc Pyfer, Saurabh J, Singhal, Alfred Marc Iloreta, et al. Minimizing septectomy for endoscopic transsphenoidal approaches to the sellar and suprasellar regions: a cadaveric morphometric study. J Neurol Surg B. 2016; 77: 193-278.
12. Figueroa RE. Imaging Anatomy in Revision Sinus Surgery. Revision Sinus Surgery. 2008; 1-11.
13. Nyquist GG, Anand VK, Brown S, Singh A, Tabaee A, Schwartz HT, et al. Middle turbinate preservation in endoscopic transsphenoidal surgery of the anterior sull base. Skull Base. 2010; 20: 343-347.
14. Sowerby LJ, Mann S, Starreveld Y, Kotylak T, Mechor B, Wright ED. A comparison of radiographic evidence of frontal sinusitis in middle-turbinate sacrificing versus middle-turbinate sparing approaches to the sella. Am J Rhinol Allergy. 2016; 30: 306-309.