Embed Size (px)
Citation preview

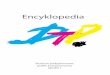
Fig. 1. A full-thickness biopsy of the terminal ileum showsfeatures of granulomatous inflammation at the base of the ulcer.
Anatomical diagnosis. M. tuberculosis infection of thesmall bowel.
REFERENCES
1. Spechler SJ. Schimmel EM. Gastrointestinal tract bleeding 01 unknown origin. ArchIntern Med 1982: 142: 236-240.
2. Thompson IN, saJem AA. Hemingway AP. et al. Specialist Investigation of obscuregastrointestinal bleeding. Gut 1987; 28: 47-51.
3. Glassock FU. Brenner BM. The major gJomerulopathies. In: Wilson JO. Braunwald E.Isselbacher KJ. et aJ.. eds. Harrison's Principles of Internal Medicine. 12th 00. NewYor1c McGraw-Hill, 1991: 117Q-11SQ.
4. Bllller HA. Grand RJ. Lactose intolerance. Am Rev Med 1990; 14: 141.5. Mathews JB, Silerl W. Operations for peptic ulCef" disease and earty postoperative
complications. In: Sleiseng8l" MH, Fontuan JS, eds. Gasuoinrestina/ Disease.ParhophysK)iogy. Diagnosis, Management. 5th ed. Philadelphia; WB Saunders, 1993:713-730.
6. Aosenblan SG, Drake S, Fadem S, W6ch A, l.ifschitz MD. Gasuointestinal blood lossitl patients wfth chronic renal failure. Am J Kidney Di$ 1982; 1: 232-236.
7. Bemersen B. .Johnsen A, Straume B. BorhoI PG. Jenssen TO, Stakkevold PATowards a true prevaleoce of peptic ulcer; the Soneisa gastI'OitttestinaJ disordersD.ldy. Gut 1990; 31: 989-992_
8. Musola R. Franzin G, Monl A. Manfrini C. Prevaience of gasuointestinaJ lesions inurerric pa!ients undergoing dialysis and after renal transplantation.. GaszroinresrEndcsc 1904: 30; 343-346_
9. Zuckennan GR, Cornene GL. CIouse RG, Hanel" HA. Uppet" gastn:Jintestinal bleedingitt patients with chronic renal fallure. Ann Intern Med 1985: 102: 588-592-
10. MatCuard SP, Weinstock.N. Gasuointestinalang~in renal failure. J CIinGastroenterol1988; 10: 482-434.
11. Nawab F. MasU!'S P, SlJbtamani R, Ortego TJ, Thompson CH. Angiodysp/asia inpatients with renal insufficiency. Am J Gastmetlterol 1989; 84: 1297-1301.
12. Steger AC, GaUand AB, Hemingway A, er al. Gastrointestinal haemonhage from asecond C3USl! itt patients with colonic angiodysplasia Br J $urg 1987; 74: 726-727.
13. Riners B, Grabensee 8. Heering P. Malignancy under immunosuppressive therapyincluding cyclospolitte. TfIIlsplant Proc 1994: 26: 2656-2657.
14. VilardeU J. Oppenheimer F, TeJbot-Wright R. er al. Increased risk of malignant turnersin renal transplant recipients receiving cyclospo<ine. Transplant Proc 1992; 24: 1948.
15. Suzuki S, Tanaka K, Ohsaka Y. et al. Development of de IWI'O malignancies followingrenal transplantatiott: a single centre srudy. Transpianr Proc 1994: 26: 938-940.
16. McCabe RE. Diagnosis of pulmonary infections in immunocompromised patients.Med Clin North Am 1988: 72; 1067-10~.
17. KoseIj M. ButIJtl)vW: J, Malovrh M. Tuberculosis in renaJ eJlogtaft recipients.Transplant Proc 1992; 24: 1909-1910.
18. Hall CM, Willalll PA, SWanepoel CA. Mycobacterial ittfectiOtt in renaJ transplalltrecipients. Presentatiott at the Annual Research Day. Department of Medicine.Urtiversity of Cape Towtt. 17 Sep 1992.
19. Novis BH, Bank S, Marils IN_ GastrointesMal and peritoneal luben;ulosls: a study 01cases at the Groote Schuur Hospital. 1962-1971. S AIr Med J 1973: 47: 385--372-
20. GiIinsky NH, Marb IN, Kottlel'RE. Price SK. Abdominal tuberculosis: a IQ-yearreYiew. S Air MedJ 198:3; 64: 849-857.
21. Homan WP, Grate WR, Oitteett P. A «-year experience WIth tubercub.ts entenx:oli1is.World J SuTg 19n; 1: 245-250.
22. I<Iirnadi OE. Qrmerod LP. Gastrointestinal tuberculosis: a retrospective review of 109cases itI a district geoeraI hospital. 0 J Med 1985; 56; 569-578.
23.. Bhansali SK. Abdominal lUbefeuIc:lsls: experience with 300 cases. Am J Gastroenrerof19n; 61: 324.-337.
24. Weissman 0, Gumaste W, Dave PS, Keh W. Bleeding from a tubereulous gastriculcer. Am J Gasrroenteml1990; 85: 742-744.
25. Rais N, Plumber ST. Undre AA,B~SO. Masslve lower ga5tn:ointestittalhaett'lOlThage as a complicatiott 01 intestinal tuberculosis. J Assoc Physicians India1987; 35: 647--648.
26. Waghrnare 6G, Holay MO. Cas RN, Kher A. Massive rectal bleeding due to colonictuberculosis. J Assoc Ptlysicjans India. 1988: 36(6): 392·393.
27. Pozniak AL. Dalton-Clark HJ, Ralphs ON. Colonic tuberculosis presenting as massiverectal bleeding. Tut:JercJe 19a5; 66: 295-299.
28. Wainsztein N, Roe! J, Morales JC. [Intestinal h8fT1OrrtJage due to tuberculosis in apatient with a kidney U"&nsplant] [Spanish]. MedidruJ (8 Aires) 1985; 45(6): 663-666.
Accepted 1 May 1996.
SHORT REPORT
An analysis of DTPassociated reactions bymanufacturer, batch,vaccinator, series numberand infant weightJ.G.Benade
Objectives. To detennine whether two commonly usedDTP batches manufactured by Rh6ne-Poulenc Rorer weremore reactogenic than two commonly used batches
manufactured by the South African Institute of MedicalResearch.
Design. Prospective study.Setting. Six community clinics.
Patients. Infants routinely scheduled for their first threeDTP immunisations.
Main outcome measures. Local and systemic adverse
reactions following immunisation with DTP.Results. Local reactions were significantly more
common with both Rh6ne--Poulenc Rarer products.
Conclusion. AJI adverse reaction rates comparedfavourably with those reported by the Centers for DiseaseControl.
S Atr Med J 1996; 86: 1288-1290.
Because of inadequate surveillance systems in many localauthorities, it is impossible to substantiate a growingperception that the diphtheria-tetanus-pertussis vaccine,DTP-Merieux, manufactured by Rh6ne-Poulenc Rorer, ismore reactogenic than DTP manufactured by the SouthAfrican Institute for Medical Research (SAIMR). Since thisclimate of uncertainty can eventually undermine theExpanded Programme on Immunisation, the validity of theseperceptions was investigated by a stUdy of the reactionprofiles of four commonly used vaccine batches, suspectedof unacceptable reactogenicity by some local authorities.
LiteratureIt is well known that whole-cell pertussis--containing vaccineis more reactogenic than most of the vaccines routinetyused for immunisations.U The reported incidence oftenderness, erythema, swelling or induration at the injectionsite varies from 300 - 700/1 000 DTP doses, USUally occurswithin 48 hours of vaccination and is mostly setf-limited.l
-6 Anodule may occasionally be palpable at the injection site for
Department of Community Health, University of Stellenbosch,Tygerberg, W. Cape
J. G. Benade. M.a OlB.• M.MEO. (C.H.)
Volume 86 No, 10 Ocrobu 1996 SAMJ

SAMJARTICLES
several weeks, but sterile abscesses have been reportedoccasionally (6 - 10 x 1ca doses of DTP). Injection siteabscess rates depend mainly on the sterility of vaccinationpractices. Rates of adverse events following immunisation(AEFI) are lowest when the vaccine is administered in thebuttocks,6 while subcutaneous administration at any site isparticularly prone to cause local AEFI.
A variety of mild-to-moderate systemic effects frequentlyoccur within 3 - 6 hours of DTP administration and canpersist for 1 - 2 days l..3.3-7 but appear to be without sequelae.s
Fever of ~ 40.5°C is rare and hypotonic hyporesponsiveepisodes even more so. The role of DTP in exceedingly rareneurological illnesses, e.g. prolonged convulsions,encephalopathy or sudden infant death syndrome, remainsunclear.' The frequencies of local reactions and fever areknown to increase with an increasing number of OTP doses,while mild-to-moderate systemic reactions decrease with anincreasing number of doses. 5
.6.9 Substitution of diphtheria
tetanus (01) vaccine is advisable in cases of moderate-tosevere AEFI with DTP.
Subjects and methodsThree high-turnover clinics at both the Western CapeRegional Services Council (WCRSC) and KraaifonteinMunicipality were selected. Infants aged 3, 41/2 and 6months, routinely scheduled for their first three DTPimmunisations (DTP1, DTP2, DTP3), were prospectivelyenrolled from 1 June 1994 to 30 January 1995. All vaccinewas provided by the Department of National Health (WesternCape). All vaccinations were administered intramuscularly inthe deltoid area (23-gauge needle) and vials were stored andhandled according to World Health Organisation guidelines.7
Informed consent was obtained and contraindications asdefined by the vaccine package inserts were adhered to.
At WCRSC clinics, infants randomly received either DTPMeri;,ux batch K5315 or SAIMR batch G03509 and, atKraaifontein clinics, DTP-Merieux J5497 or SAIMR F08609.Methods of randomisation varied slightly between the two
clinic groups in order to minimise clinic disruption. DTP dosenumbers and batches were recorded on clinic cards toensure vaccination with the same batch at consecutivevisits. Each sister kept standardised personal immunisationrecords. Parents were requested to notify anyone of theAEFI described to any sister at the clinic where vaccinationwas performed. Notifications were evaluated by clinic sistersaccording to a standard questionnaire and by directobservation. The Epi Info 6 statistical programme was usedto analyse data.
ResultsTable I summarises adverse events that followed within48 - 72 hours of immunisation with the four batches, incomparison with AEFI rates reported by an authoritativesource.! Redness in the 10 - 24 mm range was most prevalent(> 75% of cases) and the majority of cases had swelling in the10 - 39 mm range (> 75% of cases). The majority ot palpablemasses were 10 - 24 mm in diameter (> 75% of cases).
In total, significantly more infants experienced local (2.08< RR =4.16 < 8.34) and systemic (2.38 < RR =6.84 < 19.67)reactions with batch J5497 than with F08609. Vaccinationwith DTP-Merieux K5315 resulted in significantly more localreactions (1.47 < RR = 5.15 < 18.65) than vaccination withSAIMR G03509. DTP-Merieux K5315 was no morereact0genic than SAIMR G03509 at any specific WCRSCclinic. Merieux J5497 only caused significantly more totalreactions than SAIMR F08609 at the largest Kraaifonteinclinic (2.51 < RR = 5.07 < 10.26).
In total, AEFI cases and controls did not differ in terms ofweight at birth, at DTP1 or at OTP2. In an inception cohortat the Kraaifontein clinics, the incidence of AEFI declinedsignificantly with subsequent dose numbers of MerieuxJ5497 (P < 0.001). The RR for a local AEFI with J5497 (N =222), compared with F08609 (N = 183), was 4.12 at DTP1(95% Cl = 1.43; 11.84), 3.10 at DTP2 (95% Cl = 1.04; 9.25)and 0.93 at DTP3 (95% Cl = 0.13; 6.54).
The incidence 9f fever was excluded from all calculations,since thermometers were not used uniformly.
Table I. Rate (per 1 000 doses) of adverse events occurring within 48 - 72 hours of DTP vaccination, regardless of dose number
2.9 013.4:1: 3.2'3.2 2.4
5.31 ot0 01.4 0.80 00 0
0 00 0
J5497 K5315MMWW (N = 629) (N = 1 059)
LocalRedness 330 6.3 1.9Swelling 400 55.6; 5.7'Subcutaneous nodule 12.7 4.7Pain 500
SystemicFever> 38°C 500 14.31 01Drowsiness 330 3.2 0Fretfulness 500 17.6 1.9Vomiting 66 3 0Persistent, inconsolable crying> 3 hrs 10 3.2 0Collapse 1.3Convulsions 0.57 1.6 0Sterile abscesses 6 x 10' 0 0Fever> 4O.5°C 3
• Adapted from reference 1.t Subjectively judged by parent.:l: Sum of nodules, lnduration and masses.
Merieux SAIMR
F08609 G03509(N = 748) (N = 1 259)
SAMJ Volume 86 No. 10 October 1996 1289

DiscussionThe local and systemic rates of AEFI with all the batchesused in this study compared very favourably with thosereported by the Immunisation Practices Advisory Committeeof the Centers for Disease Control' (as indicated in Table I)and the International Children's Center in Paris. 11 Even themost reactogenic batch, DTP-Merieux J5497, was clearlywithin acceptable levels and the majority of local reactionswere relatively minor. At the Kraaifontein clinics, AEFI ratesseemed to depend on the broad socio-economic level of thecommunity served. The Kraaifontein clinic where twovaccinators were less prone to AEFI than their colleagues,suggests differences in vaccine administration techniqueamong vaccinators. Contrary to international experience, theincidence of local AEFI for DTP-Merieux J5497 decreasedwith increasing dose number, thus indicating that the morereactogenic individuals were at greatest risk of an AEFI atDTP1.
ConclusionsOur results prove that perceptions of 'unacceptable levels ofAEFI' for the batches used are unfounded and in danger ofcompromising the goals of the Expanded Programme onImmunisation. ll Improved surveillance at all levels to provideaccurate data for rational decision-making, combined withincreased levels of knowledge about what kind of AEFI are'acceptable', could contribute substantially towardsattainment of high DTP coverage.
The risk of an AEFI with DTP in this study was determinedby the choice of vaccine manufacturer and batch,vaccinator, dose series number and the broad socioeconomic group of the patient. More comprehensive studiesare required to determine whether a link exists between AEFIand vaccine efficacy.
I acknowledge the contributions of the Department ofCommunity Health, University of Stellenbosch, the formerWestern Cape Regional Services Council, the Municipality ofKraaifontein and the Department of Health.
REFERENCES
1 RecommffldallOflS 01 the ImmunIsation PractIces AdVIsory CommIttee {ACIPJ.Oiphthena. Tetanus ano P",rtUSSIS: Recommel1aatlOI1S lar VaCCine Use and OtherPreventive Measures MMWR 1991; 40: 1-23
2 Bernst~n 01. SmIth VE Schif GM. et al. ComparIson of acellular pertussIsvaccJne IVlth ",hole cell vaCCine as a boost., In Children 15 to 18 months and <:106 years of age Pedtatrlnfect Dis J 1993; 12: 131-135
3 Canad,an PharmaceutIcal Assoclatton - O'phlhena ana letanus lo_old anapertUSMl vaccIne absorbed. In: Krogh CME. lK! CompendIum of PhiJrmaceutlcalSpeclalr:es. Toronto; CK Productions, 199: 3s-:.
<:. Dukes MNA, Aronson JK. 8lac\o;;.... ell 8. et al, ea! Merler's Side E""ects of Drugs.An Encyc/opec,a of Adverse Reac!Jons and fntefllctwns AmsletCam: E1sl!V'er.1988: 680·681
5 CDdy CL. 8ara"f W. Cherry JD, el al The nature ard rales of ao\e-t'Se r;:'iJct,onsassociateo w,Ul OPT and OT lITU'I1unlsat,on lfl mfants and chdoren Ped,amcs1981: 68: 650·660
6. 8araff U. Cooy CL. Cherry JO DTP-assQClaled reactIons. An anafys S byIn/l!Crlon slle. manufacturar prior reaClJons and dose Ped,atncs 19a..;: 73: 31·36
7. The Cald Cn/lIl'l (~artment of NatIonal Health C,rcular No 28 '901_ Pretona:Government Printer. 1990
8. Hirtz OG. Nelson K6. ElIenburg JH. Seizures folloWII'!g ch,lahood ImmumsalJon.J Pediau 1983; 102: 1<:-18.
9 Long SS. DeForest A. Penrtdge Pe<!lamc AssQClates. SlTllth DG. et at.Lon91tudinal study 01 adverse reactIons follOWIng oiphrheria-telanus-pertusslsvaccIne In infancy. Pedtamcs 1990: 85: 29-1·302
10. Fillastre C. Guena N. Ajlar N, et al. Twenty years' experience wIth tnple ant,genvaccine (DIphtheria-Pertussis'Tetanus). Pea,arne 1988, 43, 73·79.
11. Wor/(snop for DIstnCI Level Srafl on Prioflty CommUnicable D'sease SurveJllance'Facllilator"s gUIde BrazzaviJle: WHO RegIonal Office for Africa. 1995
Accepted 7 Mar 1996.
HISTORY OF MEDICINE
Was Isaac diabetic?Azila Talit Reisenberger
Isaac was the second of the three biblical patriarchs ofwhom Abraham and Jacob are the first and third. Hisposition in the middle of this lineage may be responsible forhis mediocre image in the eyes of some readers of the Bible,an image that is reinforced by the sense of his having beenof a somewhat lethargic personality and not noted for thebursts of actiVity or feats of physical achievementassociated with other famous biblical figures. This, togetherwith the rest of the biblical account of his life, affords atantalising opportunity to speculate on his medicalcondition, specifically the possibility that lsaac might havebeen diabetic.
Signs and symptomsDiabetes mellitus and its complications encompass amultiplicity of signs, symptoms and secondary conditions,which include a constant need for water, increased appetite,lethargy and chronic fatigue, visual deficit due to cataractsor retinopathy, and sexual dysfunction including impotence.This paper asserts that a sufficient number of theseconditions can be discerned in lsaac to make him aprobable diabetic.
At the age of 40, lsaac married Rebekah (Genesis 25:20).Thereafter, the couple evidently experienced a long period ofinvoluntary infertility, for Rebekah did not become pregnantuntil 20 years later when she was delivered of her twin sons,Esau and Jacob. Isaac was now 60 years old (Genesis 25:26) - or was he? At this point. it may be appropriate to takea closer look at the question of Isaac's age. The Bible saysthat when he was 100 years old. and when 'his eyes weretoo dim to see', he called his eldest son Esau to give him hisblessing, for 'behold, I am grown old, I know not the day ofmy death' (Genesis 27: 1·2). Given that such a blessing wasnormally bestowed when the giver was on his death-bed,Isaac must have felt very sick indeed, and it seemsreasonable that, having reached a century, Isaac should beconcerned about his mortality and should begin to thinkabout bestowing his assets. But Isaac went on to liveanother 80 biblical years after this event! The Bible says:'And the days of Isaac were 180 years. And Isaac departedthis life, and died, and was gathered unto his people old andfull of days; and Esau and Jacob his sons buried him'(Genesis 35: 28-29).
During the period after the blessing, Isaac'S sons gotmarried, had many children, and established themselves aspatriarchs in their own right. Isaac even survived familytragedies such as the rape of his grand-daughter and araging neighbourhood dispute that culminated in massmurder. Despite his own feelings, Isaac was evidently not
Department of Hebrew and Jewish Studies, University of Cape Town
Azila Taln: Reisenberger MA. >'H.C
I1290 \-afume 86 /\·0. 10 Oaober 1996 SAMJ